


Cocaine Abuse as an Immunological Trigger in a Case Diagnosed with Eales Disease

 , , ,
, , , {kind=link}
{kind=link}
Abstract
1. Introduction
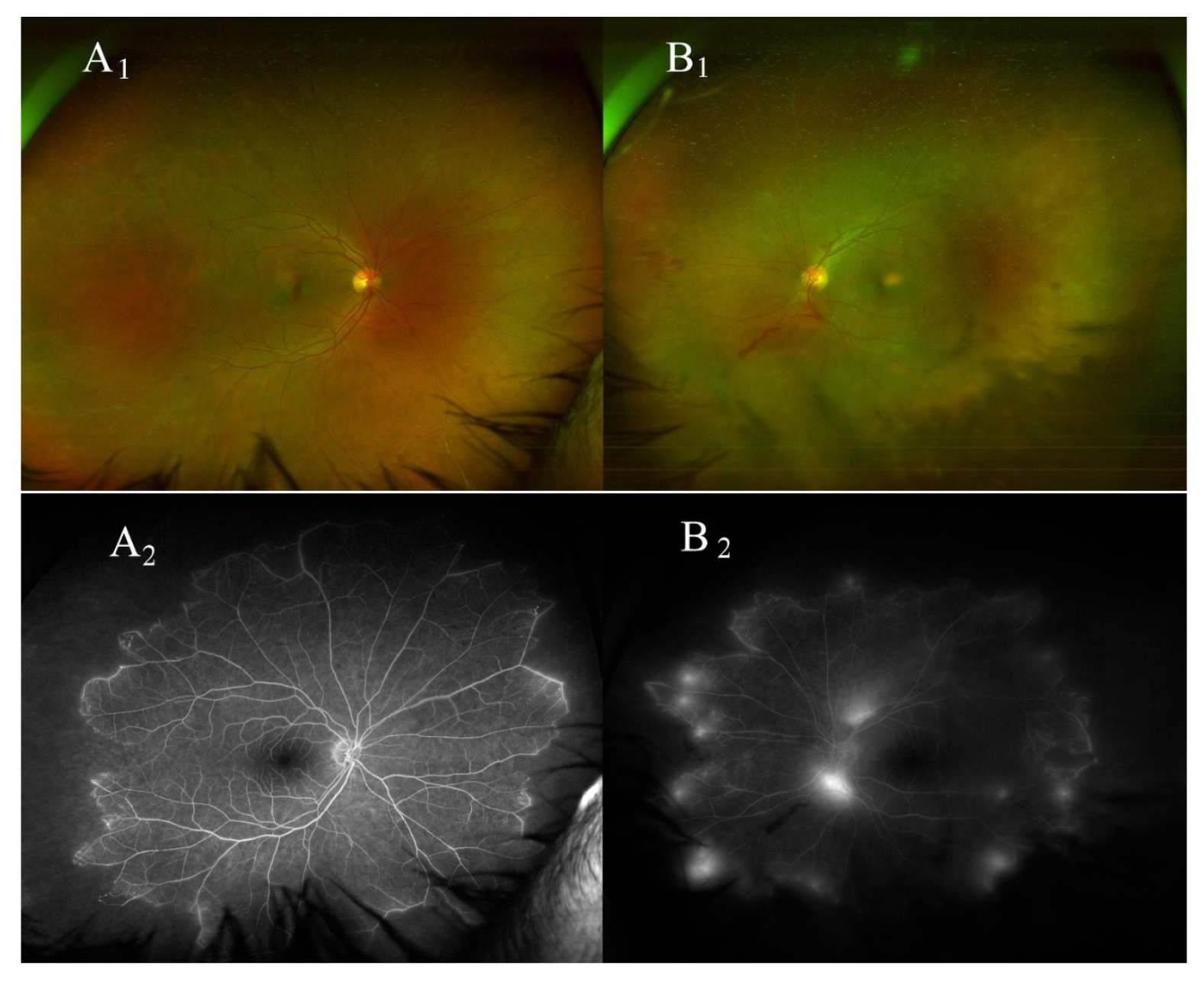
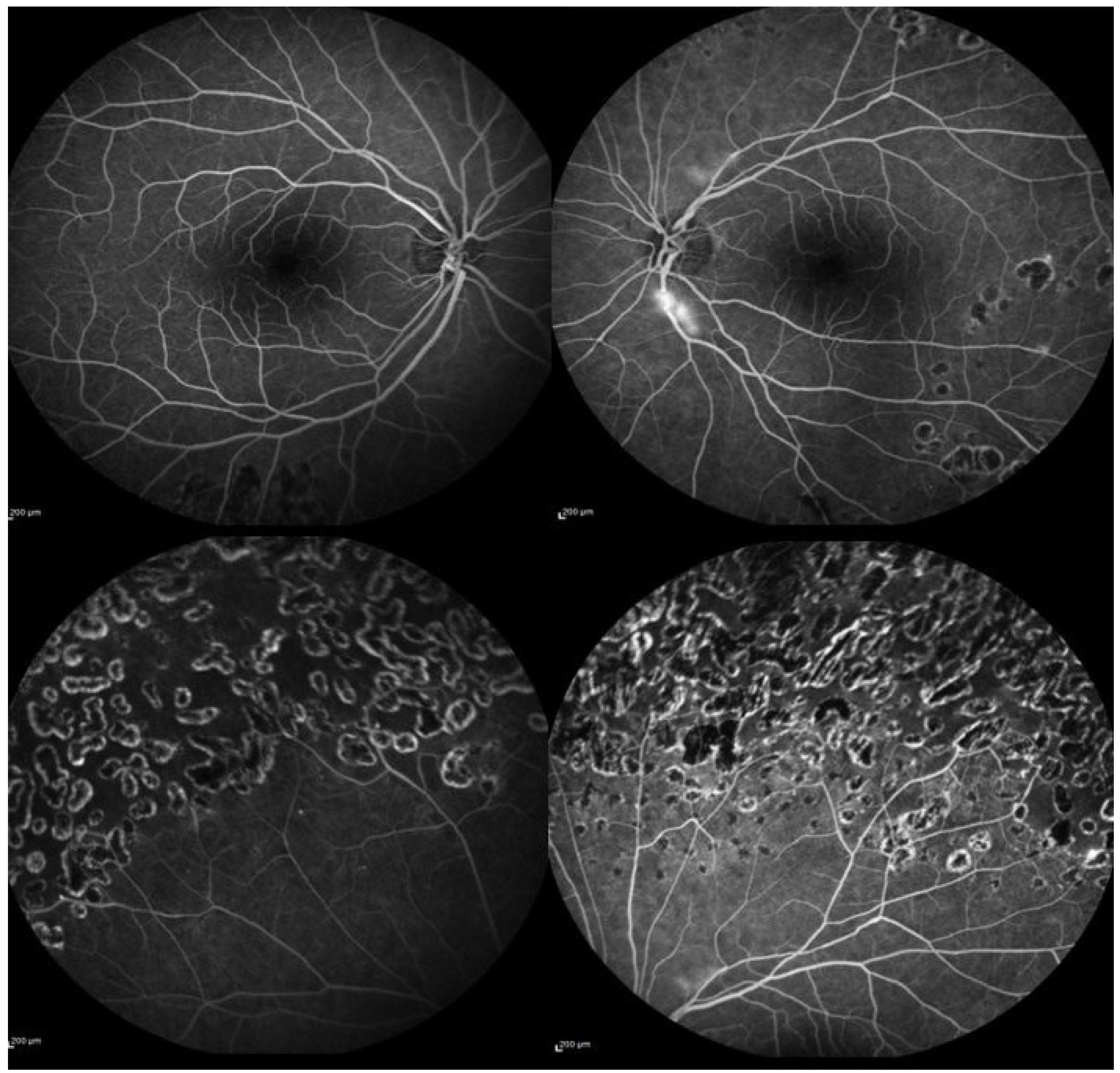
2. Case Presentation
3. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LE | left eye |
| RE | right eye |
| BE | both eyes |
| FFA | fundus fluorescein angiography |
References
- Raizada, K.; Tripathy, K. Eales Disease. In StatPearls. Edn. Treasure Island (FL): StatPearls Publishing Copyright © 2022; StatPearls Publishing LLC: Tampa, FL, USA, 2022. [Google Scholar]
- Biswas, J.; Sharma, T.; Gopal, L.; Madhavan, H.N.; Sulochana, K.N.; Ramakrishnan, S. Eales disease—An update. Surv. Ophthalmol. 2002, 47, 197–214. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Biswas, J. Further evidence of the association of latent Mycobacterium tuberculosis in Eales’ disease. Int. Ophthalmol. 2021, 41, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Kolar, P. Risk factors for central and branch retinal vein occlusion: A meta-analysis of published clinical data. J. Ophthalmol. 2014, 2014, 724780. [Google Scholar] [CrossRef] [PubMed]
- Eller, A.W.; Bontempo, F.A.; Faruki, H.; Hassett, A.C. Peripheral retinal neovascularization (Eales disease) associated with the factor V Leiden mutation. Am. J. Ophthalmol. 1998, 126, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Havakuk, O.; Rezkalla, S.H.; Kloner, R.A. The Cardiovascular Effects of Cocaine. J. Am. Coll Cardiol. 2017, 70, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Carroll, W.J.; Maganti, N.; Gill, M.K. Hypoperfusion of the deep capillary plexus associated with acute on chronic cocaine use. Am. J. Ophthalmol. Case Rep. 2020, 18, 100684. [Google Scholar] [CrossRef] [PubMed]
- Fortenbach, C.R.; Modjtahedi, B.S. Bilateral Enlargement of the Foveal Avascular Zone on Optical Coherence Tomography Angiography Associated With Cocaine Use. JAMA Ophthalmol. 2020, 138, 708–710. [Google Scholar] [CrossRef] [PubMed]
- Rahman, W.; Thomas, S.; Wiselka, M.; Bibby, K. Cocaine-induced chorioretinal infarction. Br. J. Ophthalmol. 2008, 92, 150–151. [Google Scholar] [CrossRef] [PubMed]
- Roohipourmoallai, R.; Davoudi, S.; Hosseinian Benvidi, S.M.; Iyer, S.S.R. Peripheral Retinal Neovascularization in a Patient with Sarcoidosis and Cocaine-Associated Autoimmunity. Case Rep. Ophthalmol. Med. 2021, 2021, 9923260. [Google Scholar] [CrossRef] [PubMed]
- Pontieri, F.E.; Tanda, G.; Orzi, F.; Di Chiara, G. Effects of nicotine on the nucleus accumbens and similarity to those of addictive drugs. Nature 1996, 382, 255–257. [Google Scholar] [CrossRef] [PubMed]
- Biswas, J.K.R.R.; Pal, B.; Gondhale, H.P.; Kharel Sitaula, R. Long-Term Outcomes of a Large Cohort of Patients with Eales’ Disease. Ocul. Immunol. Inflamm. 2018, 26, 870–876. [Google Scholar] [CrossRef] [PubMed]
- El-Asrar, A.M.; Al-Kharashi, S.A. Full panretinal photocoagulation and early vitrectomy improve prognosis of retinal vasculitis associated with tuberculoprotein hypersensitivity (Eales’ disease). Br. J. Ophthalmol. 2002, 86, 1248–1251. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iannetti, L.; Scarinci, F.; Alisi, L.; Beccia, A.; Cacciamani, A.; Saturno, M.C.; Gharbiya, M. Cocaine Abuse as an Immunological Trigger in a Case Diagnosed with Eales Disease. Medicina 2023, 59, 169. https://doi.org/10.3390/medicina59010169
Iannetti L, Scarinci F, Alisi L, Beccia A, Cacciamani A, Saturno MC, Gharbiya M. Cocaine Abuse as an Immunological Trigger in a Case Diagnosed with Eales Disease. Medicina. 2023; 59(1):169. https://doi.org/10.3390/medicina59010169
Chicago/Turabian StyleIannetti, Ludovico, Fabio Scarinci, Ludovico Alisi, Alessandro Beccia, Andrea Cacciamani, Maria Carmela Saturno, and Magda Gharbiya. 2023. "Cocaine Abuse as an Immunological Trigger in a Case Diagnosed with Eales Disease" Medicina 59, no. 1: 169. https://doi.org/10.3390/medicina59010169
APA StyleIannetti, L., Scarinci, F., Alisi, L., Beccia, A., Cacciamani, A., Saturno, M. C., & Gharbiya, M. (2023). Cocaine Abuse as an Immunological Trigger in a Case Diagnosed with Eales Disease. Medicina, 59(1), 169. https://doi.org/10.3390/medicina59010169