
Transcatheter Aortic Valve Replacement vs. Surgical Aortic Valve Replacement for Long-Term Mortality Due to Stroke and Myocardial Infarction: A Meta-Analysis during the COVID-19 Pandemic

 , ,
, ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Translations
2.2. Study Selection
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
- (a)
- Any study that was not a trial.
- (b)
- Studies over five years old.
- (c)
- Studies that did not contain any control or experimental data.
- (d)
- Studies that did not report a neurological or cardiogenic cause of mortality.
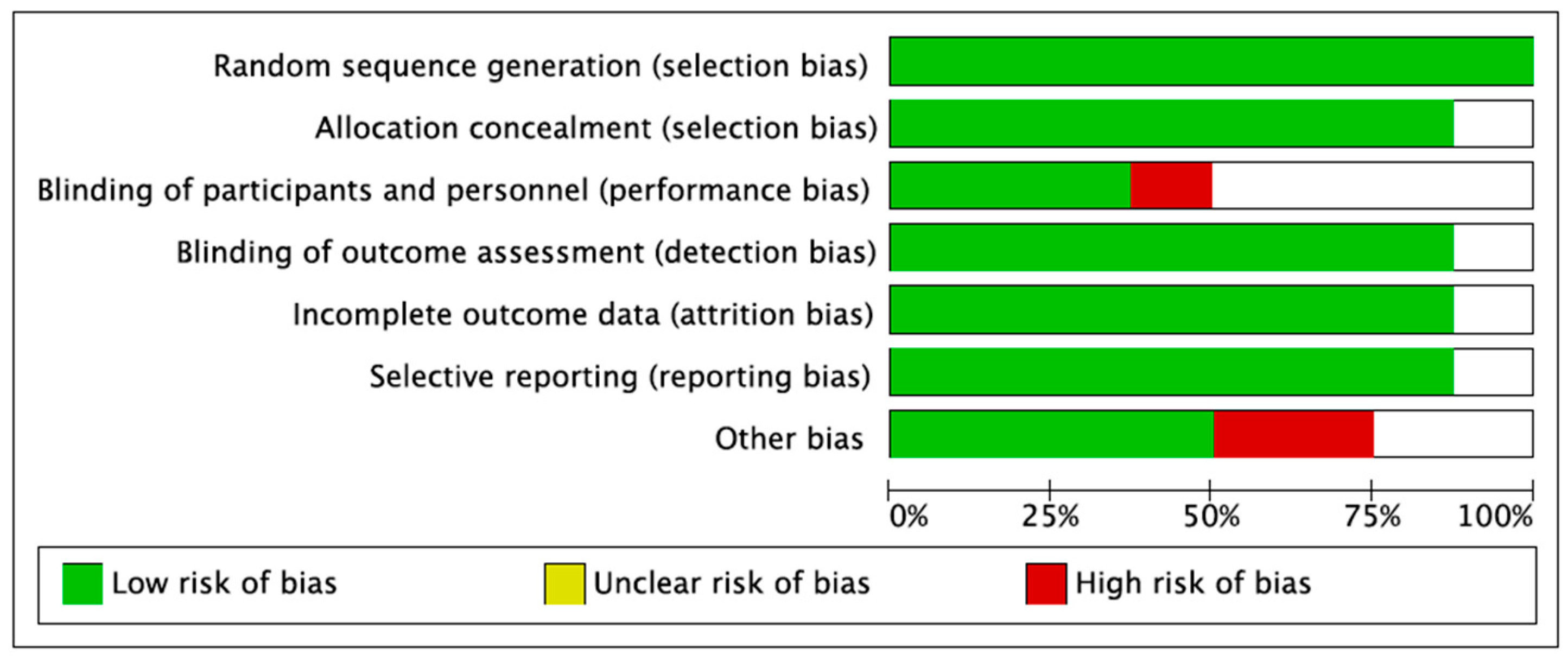
2.2.3. Data Extraction and Quality Assessment
2.2.4. Statistical Analysis
3. Results
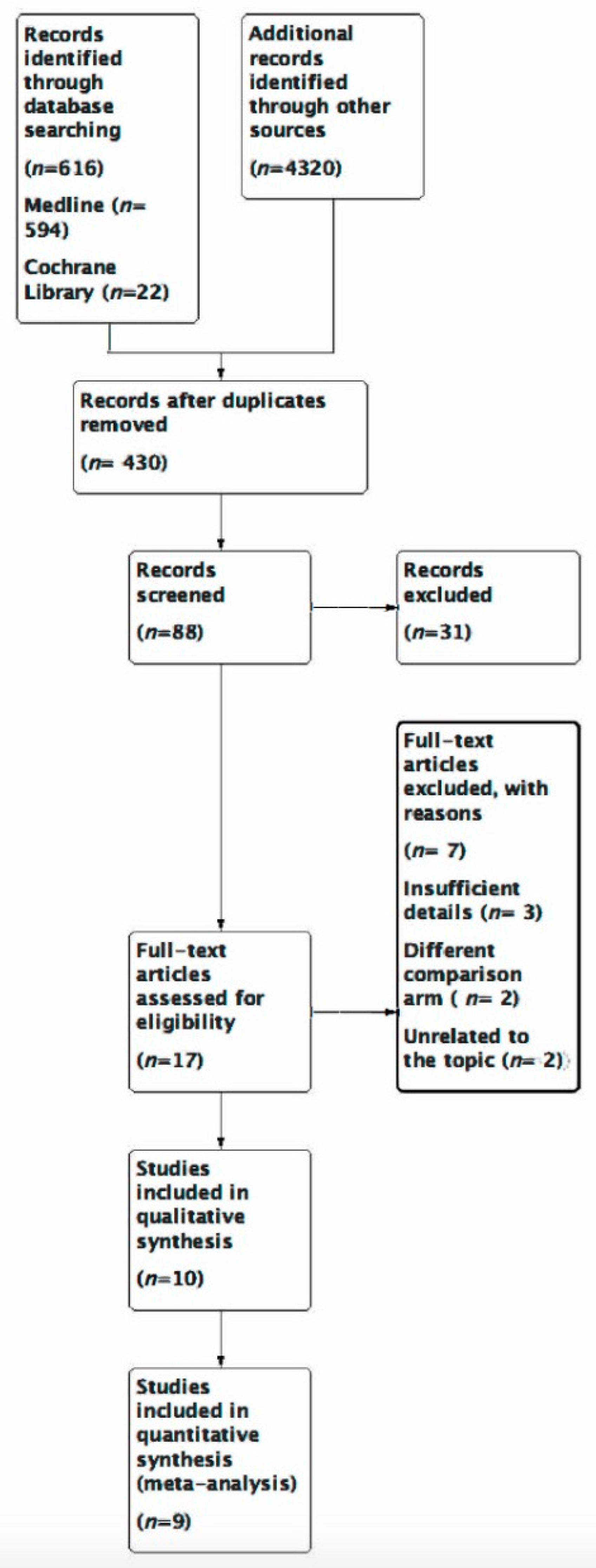
3.1. Results of Literature Search
3.2. Study Characteristics
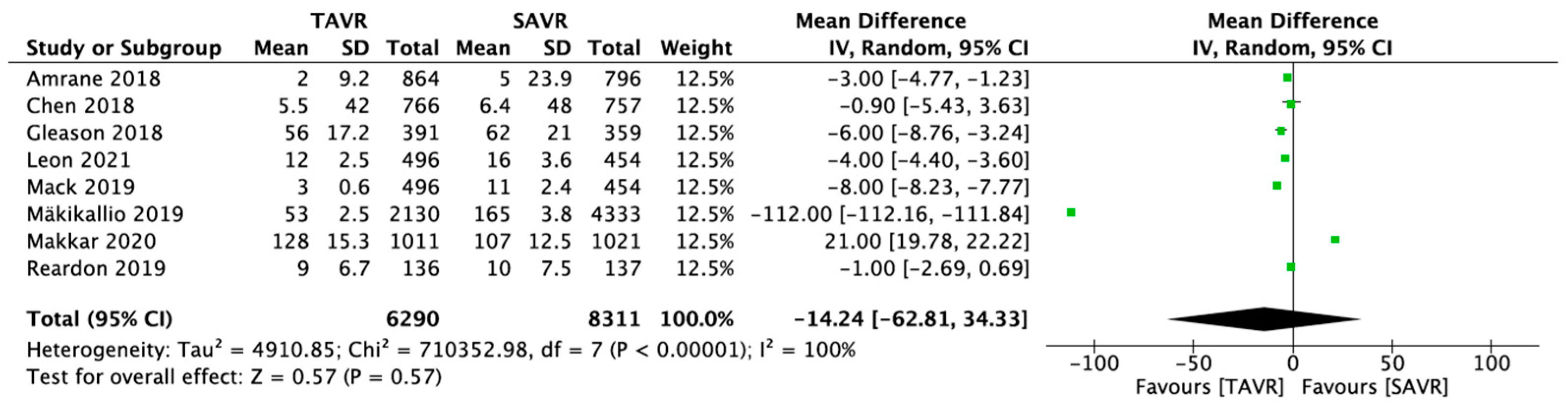
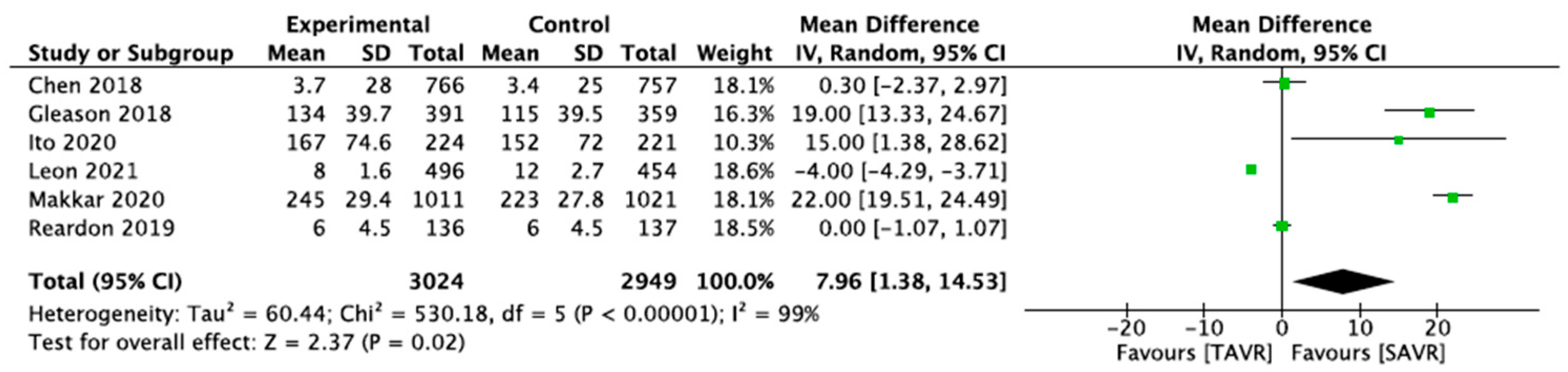
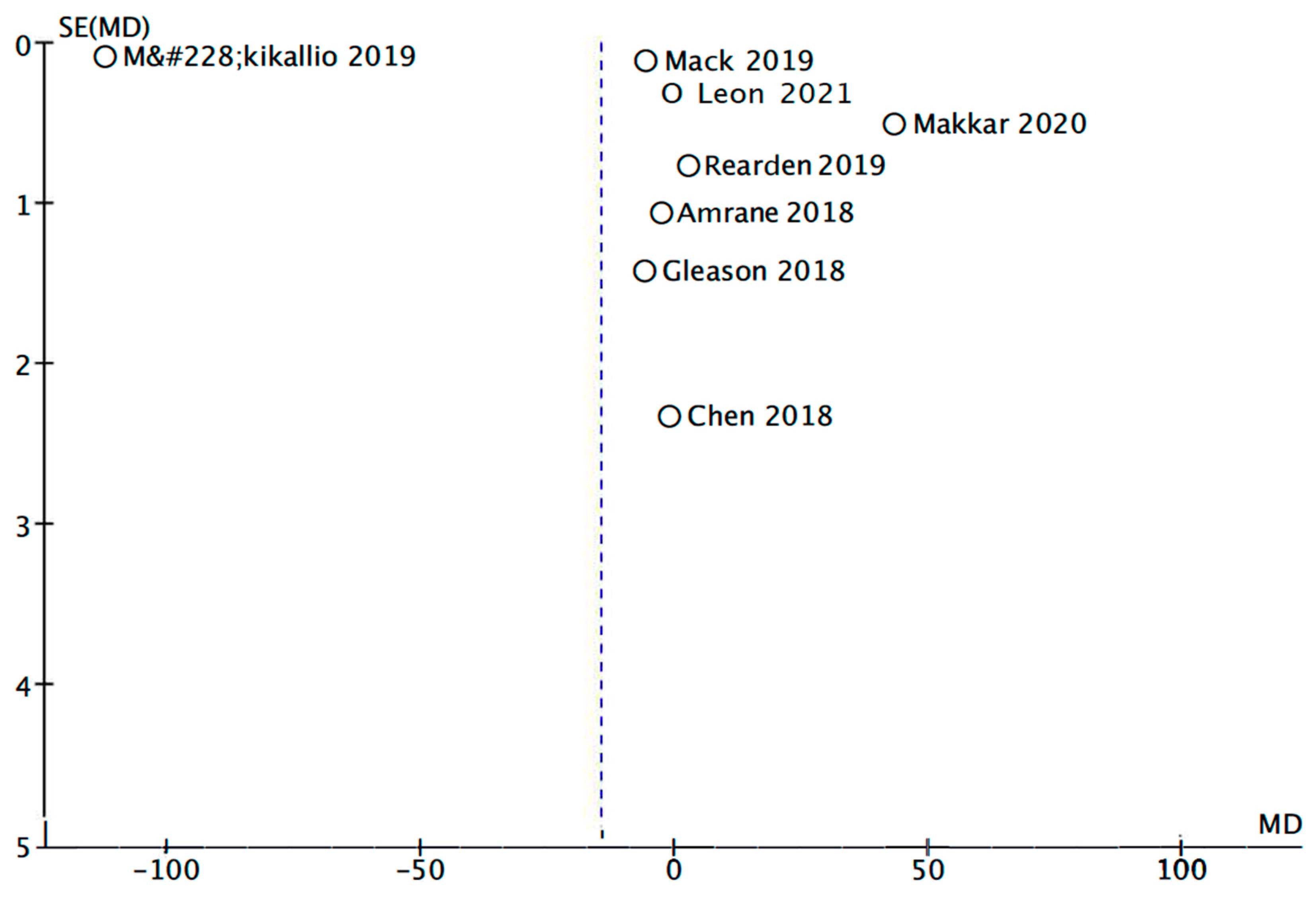
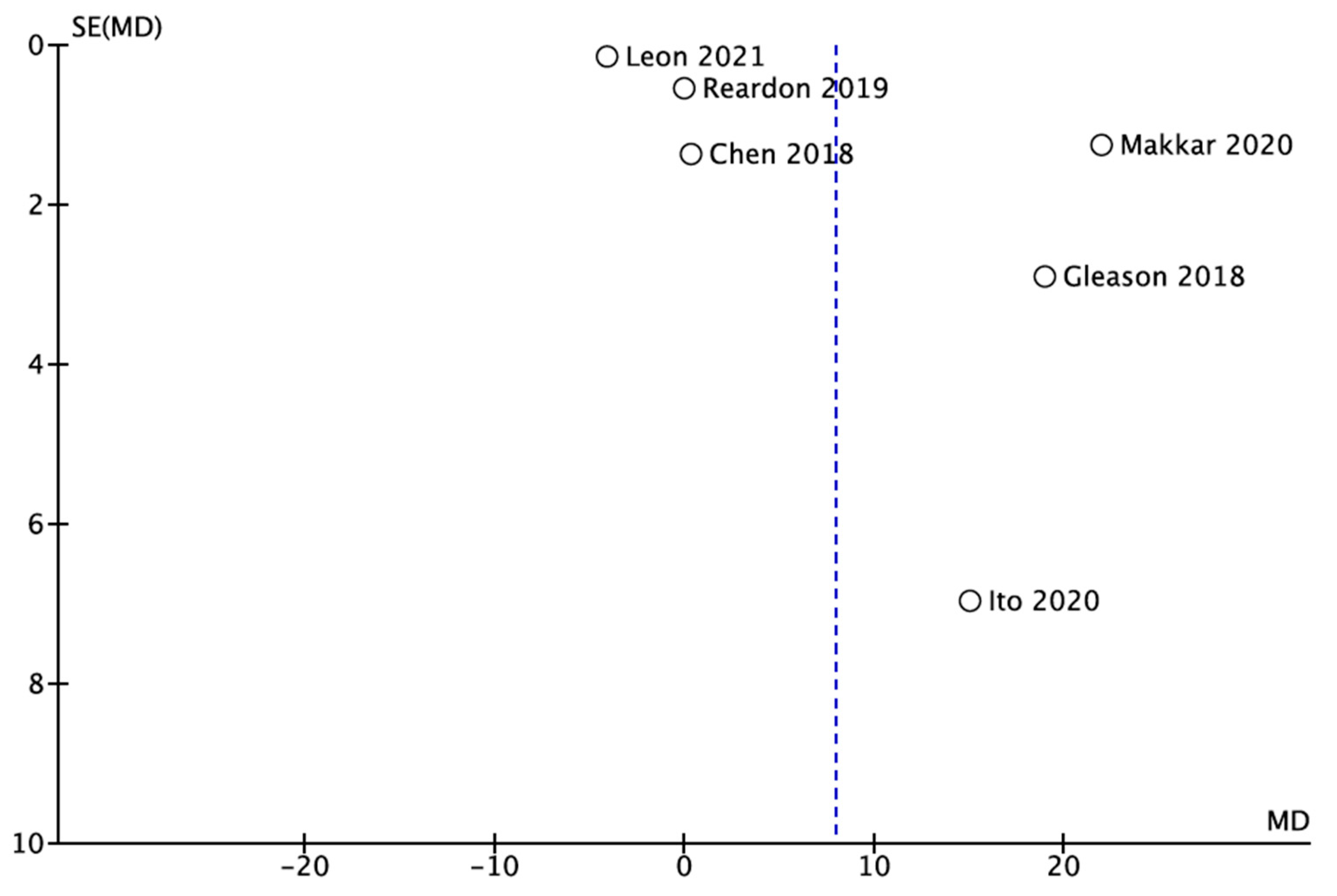
3.3. Results of Meta-Analysis
4. Discussion
5. Limitations
6. Future Implications
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ding, Q.; Liu, S.; Yao, Y.; Liu, H.; Cai, T.; Han, L. Global, Regional, and National Burden of Ischemic Stroke, 1990–2019. Neurology 2022, 98, e279. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. (2022, October 14) Heart Disease Facts. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/heartdisease/facts.htm (accessed on 11 December 2022).
- Andreasen, C.; Gislason, G.H.; Køber, L.; Abdulla, J.; Martinsson, A.; Smith, J.G.; Torp-Pedersen, C.; Andersson, C. Incidence of Ischemic Stroke in Individuals with and Without Aortic Valve Stenosis: A Danish Retrospective Cohort Study. Stroke 2020, 51, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Jaakkola, J.; Jaakkola, S.; Airaksinen, K.E.J.; Husso, A.; Juvonen, T.; Laine, M.; Virtanen, M.; Maaranen, P.; Niemelä, M.; Mäkikallio, T.; et al. Subtype of atrial fibrillation and the outcome of transcatheter aortic valve replacement: The FinnValve Study. PLoS ONE 2020, 11, e0238953. [Google Scholar] [CrossRef] [PubMed]
- Greve, A.M.; Dalsgaard, M.; Bang, C.N.; Egstrup, K.; Ray, S.; Boman, K.; Rossebø, A.B.; Gohlke-Baerwolf, C.; Devereux, R.B.; Køber, L.; et al. Stroke in Patients with Aortic Stenosis. The Simvastatin and Ezetimibe in Aortic Stenosis Study. Stroke 2014, 45, 1939–1946. [Google Scholar] [CrossRef] [PubMed]
- Paradis, J.-M.; Fried, J.; Nazif, T.; Kirtane, A.; Harjai, K.; Khalique, O.; Grubb, K.; George, I.; Hahn, R.; Williams, M.; et al. Aortic stenosis and coronary artery disease: What do we know? What don’t we know? A comprehensive review of the literature with proposed treatment algorithms. Eur. Heart J. 2014, 35, 2069–2082. [Google Scholar] [CrossRef]
- Adler, Y.; Vaturi, M.; Herz, I.; Iakobishvili, Z.; Toaf, J.; Fink, N.; Battler, A.; Sagie, A. Nonobstructive aortic valve calcification: A window to significant coronary artery disease. Atherosclerosis 2002, 161, 193–197. [Google Scholar] [CrossRef]
- Kvidal, P.; Bergström, R.; Hörte, L.G.; Ståhle, E. Observed and relative survival after aortic valve replacement. J. Am. Coll. Cardiol. 2000, 35, 747–756. [Google Scholar] [CrossRef]
- Garcia, D.; Camici, P.G.; Durand, L.-G.; Rajappan, K.; Gaillard, E.; Rimoldi, O.E.; Pibarot, P. Impairment of coronary flow reserve in aortic stenosis. J. Appl. Physiol. 2009, 106, 113–121. [Google Scholar] [CrossRef]
- Rajappan, K.; Rimoldi, O.E.; Dutka, D.P.; Ariff, B.; Pennell, D.J.; Sheridan, D.J.; Camici, P.G. Mechanisms of coronary microcirculatory dysfunction in patients with aortic stenosis and angiographically normal coronary arteries. Circulation 2002, 105, 470–476. [Google Scholar] [CrossRef]
- Bjursten, H.; Norrving, B.; Ragnarsson, S. Late stroke after transcatheter aortic valve replacement: A nationwide study. Sci. Rep. 2021, 11, 9593. [Google Scholar] [CrossRef]
- Van Mieghem, N.M.; El Faquir, N.; Rahhab, Z.; Rodríguez-Olivares, R.; Wilschut, J.; Ouhlous, M.; Galema, T.W.; Geleijnse, M.L.; Kappetein, A.P.; Schipper, M.E.I. Incidence and predictors of debris embolizing to the brain during transcatheter aortic valve implantation. JACC Cardiovasc. Interv. 2015, 8, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Sender, S.J.; Kohli, P.; Sharma, G.; Blumenthal, R.S. COVID-19’s Impact on Heart Disease and Stroke Mortality; Expert Analysis; American College of Cardiology: Washington, DC, USA, 2022. [Google Scholar]
- Sidney, S.; Lee, C.; Liu, J.; Khan, S.S.; Lloyd-Jones, D.M.; Rana, J.S. Age-adjusted mortality rates and age and risk–associated contributions to change in heart disease and stroke mortality, 2011–2019 and 2019–2020. JAMA Netw. Open 2022, 5, e223872. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontata, G.P.; Makkar, J.J.; et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus Surgical Aortic-Valve Replacement in High-Risk Patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef]
- Adams, D.H.; Popma, J.J.; Reardon, M.J.; Yakubov, S.J.; Coselli, J.S.; Deeb, G.M.; Gleason, T.G.; Buchbinder, M.; Hermiller, J., Jr.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Prosthesis. N. Engl. J. Med. 2014, 370, 1790–1798. [Google Scholar] [CrossRef] [PubMed]
- Gleason, T.G.; Reardon, M.J.; Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Lee, J.S.; Kleiman, N.S.; Chetcuti, S.; Hermiller, J.B.; Heiser, J.; et al. 5-Year Outcomes of Self-Expanding Transcatheter Versus Surgical Aortic Valve Replacement in High-Risk Patients. J. Am. Coll. Cardiol. 2018, 72, 2687–2696. [Google Scholar] [CrossRef]
- Mäkikallio, T.; Jalava, M.P.; Husso, A.; Virtanen, M.; Laakso, T.; Ahvenvaara, T.; Tauriainen, T.; Maaranen, P.; Kinnunen, E.-M.; Dahlbacka, S.; et al. Ten-year experience with transcatheter and surgical aortic valve replacement in Finland. Ann. Med. 2019, 51, 270–279. [Google Scholar] [CrossRef]
- Makkar, R.R.; Thourani, V.H.; Mack, M.J.; Kodali, S.K.; Kapadia, S.; Webb, J.G.; Yoon, S.-H.; Trento, A.; Svensson, L.G.; Herrmann, H.C.; et al. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N. Engl. J. Med. 2020, 382, 799–809. [Google Scholar] [CrossRef]
- Martin, G.P.; Curzen, N.; Goodwin, A.T.; Nolan, J.; Balacumaraswami, L.; Ludman, P.F.; Kontopantelis, E.; Wu, J.; Gale, C.P.; de Belder, M.A.; et al. Indirect Impact of the COVID-19 Pandemic on Activity and Outcomes of Transcatheter and Surgical Treatment of Aortic Stenosis in England. Circ. Cardiovasc. Interv. 2021, 14, e010413. [Google Scholar] [CrossRef]
- Grant, S.W.; Hickey, G.L.; Ludman, P.; Moat, N.; Cunningham, D.; de Belder, M.; Blackman, D.J.; Hildick-Smith, D.; Uppal, R.; Kendall, S.; et al. Activity and outcomes for aortic valve implantations performed in England and Wales since the introduction of transcatheter aortic valve implantation. Eur. J. Cardiothorac. Surg. 2015, 49, 1164–1173. [Google Scholar] [CrossRef]
- Lauck, S.; Forman, J.; Borregaard, B.; Sathananthan, J.; Achtem, L.; McCalmont, G.; Muir, D.; Hawkey, M.C.; Smith, A.; Kirk, B.H.; et al. Facilitating transcatheter aortic valve implantation in the era of COVID-19: Recommendations for programmes. Eur. J. Cardiovasc. Nurs. 2020, 19, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Elbaz-Greener, G.; Yarranton, B.; Qiu, F.; Wood, D.A.; Webb, J.G.; Fremes, S.E.; Radhakrishnan, S.; Wijeysundera, H.C. Association Between Wait Time for Transcatheter Aortic Valve Replacement and Early Postprocedural Outcomes. J. Am. Heart Assoc. 2019, 8, e010407. [Google Scholar] [CrossRef] [PubMed]
- Stickels, C.P.; Nadarajah, R.; Gale, C.P.; Jiang, H.; Sharkey, K.J.; Gibbison, B.; Holliman, N.; Lombardo, S.; Schewe, L.; Sommacal, M.; et al. Aortic stenosis post-COVID-19: A mathematical model on waiting lists and mortality. BMJ Open 2022, 12, e059309. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- Amrane, H.; Deeb, G.M.; Popma, J.J.; Yakubov, S.J.; Gleason, T.G.; Van Mieghem, N.M.; Reardon, M.J.; Williams, M.R.; Mumtaz, M.; Kappetein, A.P.; et al. Causes of death in intermediate-risk patients: The Randomized Surgical Replacement and Transcatheter Aortic Valve Implantation Trial. J. Thorac. Cardiovasc. Surg. 2019, 158, 718–728.e3. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Redfors, B.; Ben-Yehuda, O.; Crowley, A.; Greason, K.L.; Alu, M.C.; Finn, M.T.; Vahl, T.P.; Nazif, T.; Thourani, V.H.; et al. Transcatheter Versus Surgical Aortic Valve Replacement in Patients with Prior Cardiac Surgery in the Randomized PARTNER 2A Trial. JACC Cardiovasc. Interv. 2018, 11, 2207–2216. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Leon, M.B.; Mack, M.J.; Hahn, R.T.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Alu, M.C.; Madhavan, M.V.; Chau, K.H.; Russo, M.; et al. Outcomes 2 Years After Transcatheter Aortic Valve Replacement in Patients at Low Surgical Risk. J. Am. Coll. Cardiol. 2021, 77, 1149–1161. [Google Scholar] [CrossRef]
- Kapadia, S.R.; Leon, M.B.; Makkar, R.R.; Tuzcu, E.M.; Svensson, L.G.; Kodali, S.; Webb, J.G.; Mack, M.J.; Douglas, P.S.; Thourani, V.H.; et al. 5-year outcomes of transcatheter aortic valve replacement compared with standard treatment for patients with inoperable aortic stenosis (PARTNER 1): A randomised controlled trial. Lancet 2015, 385, 2485–2491. [Google Scholar] [CrossRef]
- Thyregod, H.G.H.; Ihlemann, N.; Jørgensen, T.H.; Nissen, H.; Kjeldsen, B.J.; Petursson, P.; Chang, Y.; Franzen, O.W.; Engstrøm, T.; Clemmensen, P.; et al. Five-Year Clinical and Echocardiographic Outcomes from the Nordic Aortic Valve Intervention (NOTION) Randomized Clinical Trial in Lower Surgical Risk Patients. Circulation 2019, 139, 2714–2723. [Google Scholar] [CrossRef]
- Kolte, D.; Vlahakes, G.J.; Palacios, I.F.; Sakhuja, R.; Passeri, J.J.; Inglessis, I.; Elmariah, S. Transcatheter Versus Surgical Aortic Valve Replacement in Low-Risk Patients. J. Am. Coll. Cardiol. 2019, 74, 1532–1540. [Google Scholar] [CrossRef] [PubMed]
- Lou, Y.; Gao, Y.; Yu, Y.; Li, Y.; Xi, Z.; Swe, K.N.C.; Zhou, Y.; Nie, X.; Liu, W. Efficacy and Safety of Transcatheter vs. Surgical Aortic Valve Replacement in Low-to-Intermediate-Risk Patients: A Meta-Analysis. Front. Cardiovasc. Med. 2020, 7, 590975. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, T.H.; Thyregod, H.G.H.; Ihlemann, N.; Nissen, H.; Petursson, P.; Kjeldsen, B.J.; Steinbrüchel, D.A.; Olsen, P.S.; Søndergaard, L. Eight-year outcomes for patients with aortic valve stenosis at low surgical risk randomized to transcatheter vs. surgical aortic valve replacement. Eur. Heart J. 2021, 42, 2912–2919. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, V.; Khan, N.; Jaiswal, A.; Dagar, M.; Joshi, A.; Huang, H.; Naz, H.; Attia, A.M.; Ghanim, M.; Baburaj, A.; et al. Early surgery vs. conservative management among asymptomatic aortic stenosis: A systematic review and meta-analysis. Int. J. Cardiol. Heart Vasc. 2022, 43, 101125. [Google Scholar] [CrossRef]
- Kundu, A.; Sardar, P.; Malhotra, R.; Qureshi, W.T.; Kakouros, N. Cardiovascular Outcomes with Transcatheter vs. Surgical Aortic Valve Replacement in Low-Risk Patients: An Updated Meta-Analysis of Randomized Controlled Trials. Cardiovasc. Revasc. Med. 2020, 21, 453–460. [Google Scholar] [CrossRef]
- Harky, A.; Seyedzenouzi, G.; Sanghavi, R.; Premkumar, G.; Badran, A. COVID-19 and its implications on patient selection for TAVI and SAVR: Are we heading into a new era? J. Card. Surg. 2021, 36, 265–267. [Google Scholar] [CrossRef]
- Khalil, K.N.; Forcillo, J. SAVR contemporary outcomes in TAVI era: Still a valid option for the future. J. Card. Surg. 2021, 36, 1477–1478. [Google Scholar] [CrossRef]
- Cristian, I.A.; Șerbanoiu, L.I.; Busnatu, Ș.Ș.; Chinocel, V.; Andrei, C.L. The Impact of Antithrombotic Therapy in Patients with Decompensated Heart Failure and Iron. Balneo PRM Res. J. 2022, 13, 512. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ion, A.C.; Serbanoiu, L.I.; Plesu, E.; Busnatu, S.S.; Andrei, C.L. Transcatheter Aortic Valve Replacement vs. Surgical Aortic Valve Replacement for Long-Term Mortality Due to Stroke and Myocardial Infarction: A Meta-Analysis during the COVID-19 Pandemic. Medicina 2023, 59, 12. https://doi.org/10.3390/medicina59010012
Ion AC, Serbanoiu LI, Plesu E, Busnatu SS, Andrei CL. Transcatheter Aortic Valve Replacement vs. Surgical Aortic Valve Replacement for Long-Term Mortality Due to Stroke and Myocardial Infarction: A Meta-Analysis during the COVID-19 Pandemic. Medicina. 2023; 59(1):12. https://doi.org/10.3390/medicina59010012
Chicago/Turabian StyleIon, Alexandru Cristian, Liviu Ionut Serbanoiu, Elena Plesu, Stefan Sebastian Busnatu, and Catalina Liliana Andrei. 2023. "Transcatheter Aortic Valve Replacement vs. Surgical Aortic Valve Replacement for Long-Term Mortality Due to Stroke and Myocardial Infarction: A Meta-Analysis during the COVID-19 Pandemic" Medicina 59, no. 1: 12. https://doi.org/10.3390/medicina59010012
APA StyleIon, A. C., Serbanoiu, L. I., Plesu, E., Busnatu, S. S., & Andrei, C. L. (2023). Transcatheter Aortic Valve Replacement vs. Surgical Aortic Valve Replacement for Long-Term Mortality Due to Stroke and Myocardial Infarction: A Meta-Analysis during the COVID-19 Pandemic. Medicina, 59(1), 12. https://doi.org/10.3390/medicina59010012