
Impact of Pulmonary Hypertension on Mortality after Surgery for Aortic Stenosis



Abstract
1. Introduction
2. Materials and Methods
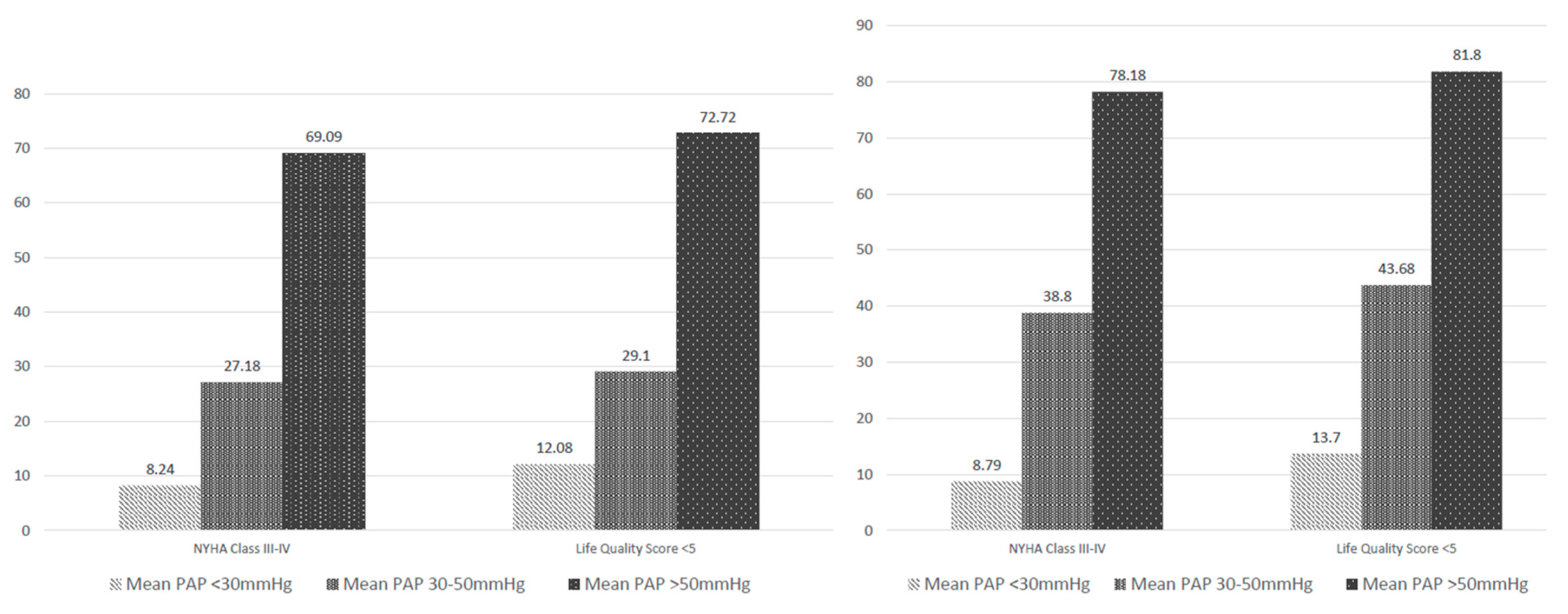
- Group A—182 patients with normal PAP.
- Group B—103 patients with mean PAP between 30 and 50 mmHg.
- Group C—55 patients with mean PAP more than 50 mmHg [9].
3. Results
- -
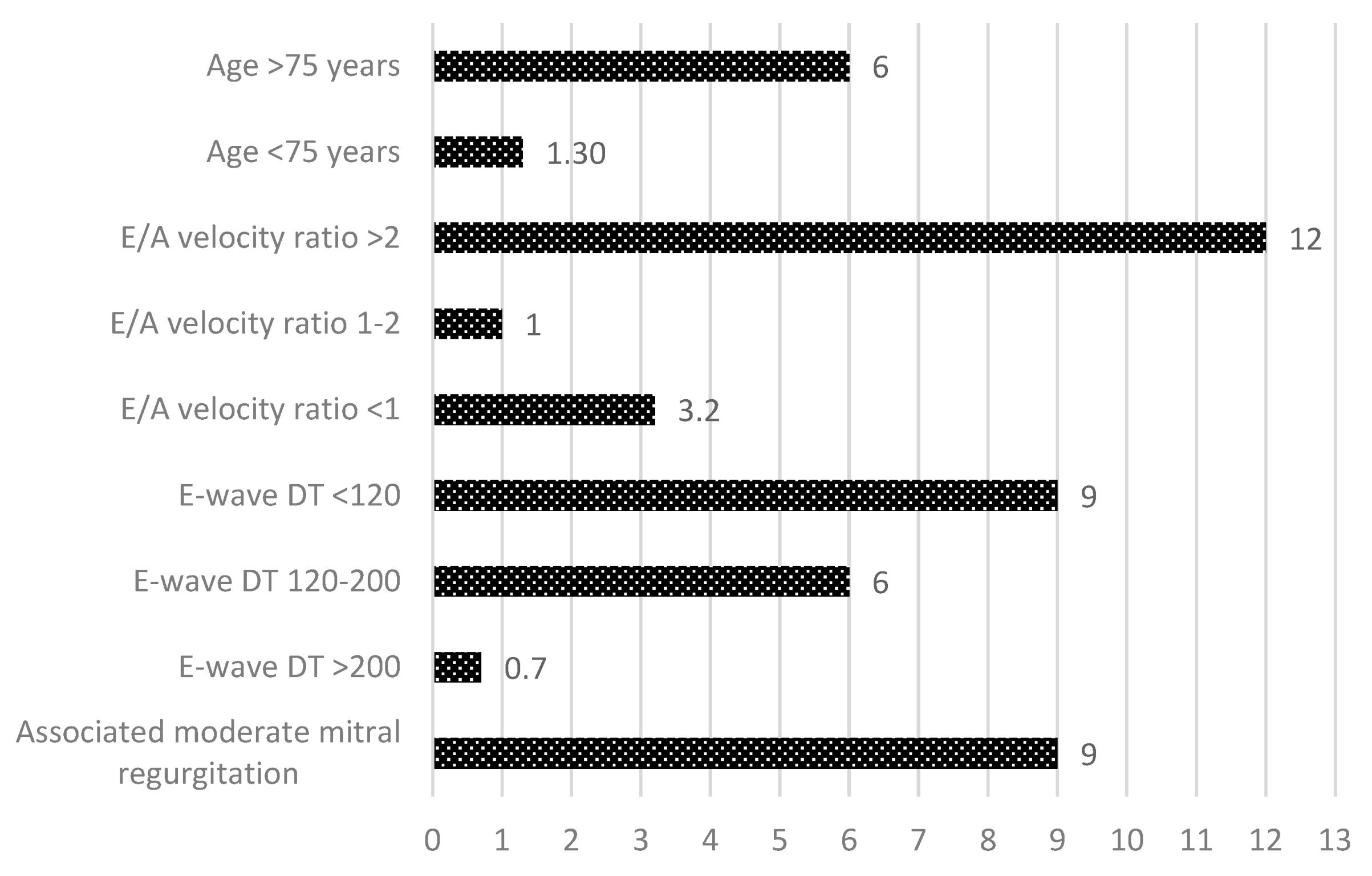
- Age >75 years (RR = 6), p < 0.001;
- -
- Restrictive LV diastolic filling pattern (RR = 9), p < 0.001;
- -
- Associated moderate mitral regurgitation (RR = 9), p < 0.0001.
- -
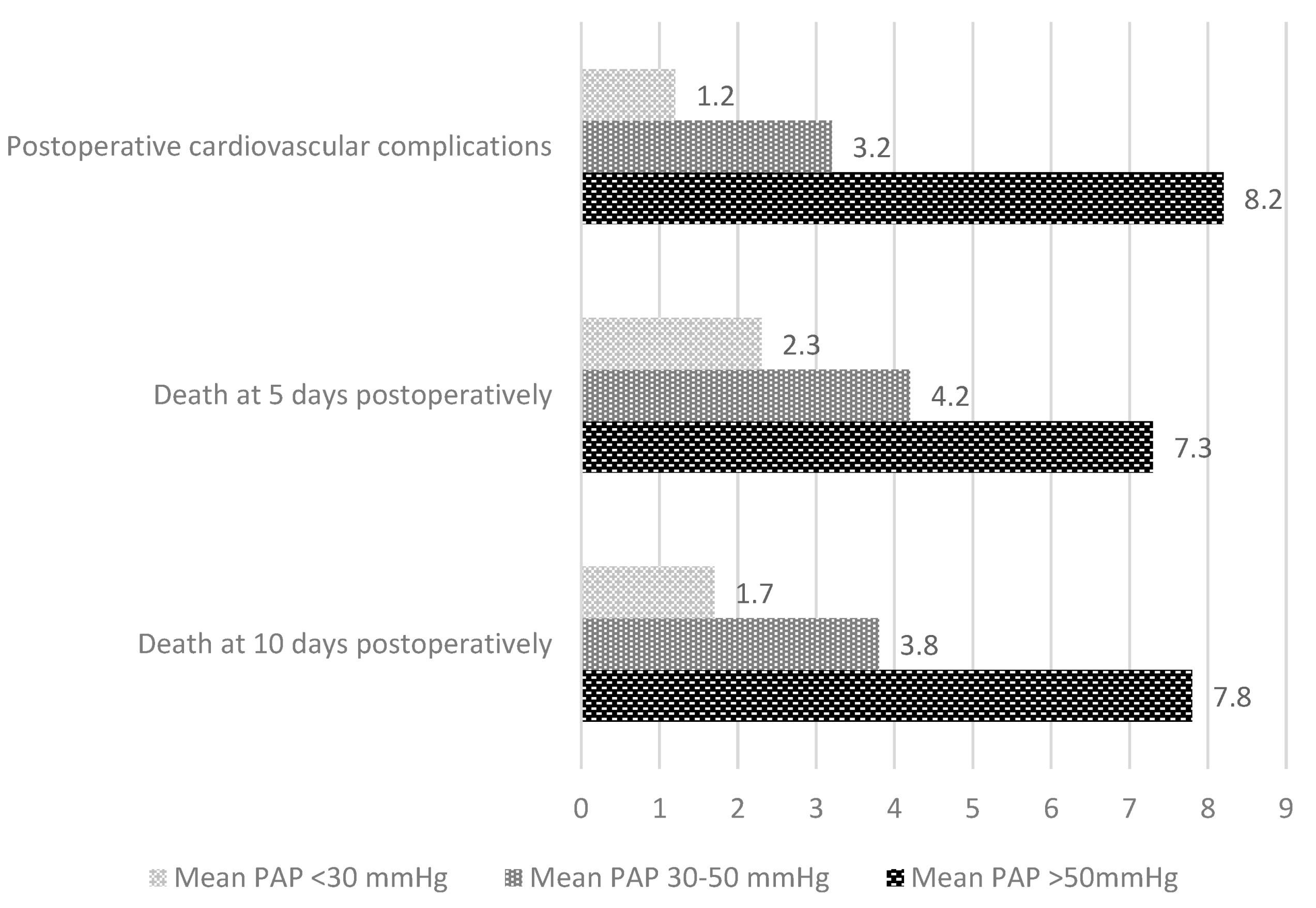
- Mean PAP > 50 mmHg (RR = 9), p < 0.001;
- -
- Restrictive LV diastolic filling pattern (RR = 9), p < 0.001;
- -
- Age >75 years (RR = 6), p < 0.001;
- -
- Interventricular septum thickness >18 mm;
- -
- The presence of comorbidities (diabetes mellitus and chronic kidney disease) (RR = 9), p < 0.0001.
4. Discussion
5. Conclusions
- The relevant independent predictors for PHT occurrence in surgical AS were: age > 75 years, restrictive LVDFP and the presence of moderate MR.
- The presence of a severe PHT in patients with AS undergoing surgical AVR was associated with an early postoperative increased mortality rate. The mean PAP is a more reliable parameter for prognosis appreciation than the LV systolic function.
- The independent predictors for increased early postoperative mortality rate in patients with surgical AS were:
- -
- Mean PAP > 50 mmHg;
- -
- The presence of a restrictive LVDFP;
- -
- Age > 75 years;
- -
- Interventricular septum thickness >18 mm;
- -
- Comorbidities (diabetes mellitus and pulmonary diseases).
- PHT regression at 2 years postoperatively was only correlated with preoperative left ventricular dimensions and systolic and diastolic function and could not be predicted by other clinical or ultrasound parameters.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MOBILITY | 0 | Unable to control or use arms and legs. |
| 1 | Requires help of another person or mechanical equipment (such as canes, crutches, braces, or wheelchair) to walk or get around independently. | |
| 2 | Able to walk, bend, lift, jump, and run normally for age | |
| EMOTION | 0 | Almost always fretful, angry, irritable, anxious, or depressed. |
| 1 | Occasionally or often fretful, angry, irritable, anxious, depressed, or suffering “night terrors”. | |
| 2 | Generally happy and free from worry. | |
| SENSATION | 0 | Not able to see, hear, and speak normally for age. |
| 1 | Sees, hears, or speaks with limitations or with equipment. | |
| 2 | Able to see, hear, and speak normally for age. | |
| SELF-CARE | 0 | Requires the help of another person to eat, bathe, dress, or use the toilet. |
| 1 | Requires help to eat, bathe, dress, or use the toilet independently. | |
| PAIN | 0 | Frequent or severe pain; frequent disruption of normal activities. Discomfort requires prescription narcotics for relief |
| 1 | Occasional pain. Discomfort relieved by non-prescription drugs or self-control activity without disruption of normal activities. | |
| 2 | Free or occasional pain and discomfort. |
References
- Micha, T.; Maeder, L.W.; Rickli, H. Pulmonary hypertension in aortic valve stenosis. Trends Cardiovasc. Med. 2022, 32, 73–81. [Google Scholar]
- Maeder, M.T.; Weber, L.; Buser, M.; Gerhard, M.; Haager, P.K.; Maisano, F.; Rickli, H. Pulmonary hypertension in aortic and mitral valve disease. Front. Cardiovasc. Med. 2018, 5, 40. [Google Scholar] [CrossRef] [PubMed]
- Levy, F.; Bohbot, Y.; Sanhadji, K.; Rusinaru, D.; Ringle, A.; Delpierre, Q.; Smaali, S.; Gun, M.; Marechaux, S.; Tribouilloy, C. Impact of pulmonary hypertension on long-term outcome in patients with severe aortic stenosis. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 553–561. [Google Scholar] [CrossRef]
- Magne, J.; Pibarot, P.; Sengupta, P.P.; Donal, E.; Rosenhek, R.; Lancellotti, P. Pulmonary hypertension in valvular disease: A comprehensive review on pathophysiology to therapy from the HAVEC group. JACC Cardiovasc Imaging 2015, 8, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Cam, A.; Goel, S.S.; Agarwal, S.; Menon, V.; Svensson, L.G.; Tuzcu, E.M.; Kapadia, S.R. Prognostic implications of pulmonary hypertension in patients with severe aortic stenosis. J. Thorac. Cardiovasc. Surg. 2011, 142, 800–808. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zlotnick, D.M.; Ouellette, M.L.; Malenka, D.J.; DeSimone, J.P.; Leavitt, B.J.; Helm, R.E.; Elaine, M.; Olmstead, E.M.; Costa, S.P.; DiScipio, A.W.; et al. Northern New England Cardiovascular Disease Study Group. Effect of preoperative pulmonary hypertension on outcomes in patients with severe aortic tenosis following surgical aortic valve replacement. Am. J. Cardiol. 2013, 112, 1635–1640. [Google Scholar] [CrossRef]
- Alushi, B.; Beckhoff, F.; Leistner, D.; Franz, M.; Reinthaler, M.; Barbara, E.; Stähli, B.E.; Morguet, A.; Figulla, H.R.; Doenst, T.; et al. Pulmonary Hypertension in Patients With Severe Aortic Stenosis: Prognostic Impact After Transcatheter Aortic Valve Replacement: Pulmonary Hypertension in Patients Undergoing TAVR. JACC Cardiovasc. Imaging 2019, 12, 591–601. [Google Scholar] [CrossRef]
- Al-Khadra, Y.; Darmoch, F.; Pacha, H.M.; Soud, M.; Kajy, M.; Ando, T.; Rab, T.; Grines, C.L.; Kaki, A.; Kwok, C.S.; et al. The Outcomes of Pulmonary Hypertension Patients With Severe Aortic Stenosis Who Underwent Surgical Aortic Valve Replacement or Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2019, 124, 586–593. [Google Scholar] [CrossRef]
- Faqih, S.A.; Noto-Kadou-Kaza, B.; Abouamrane, L.M.; Mtiou, N.; El Khayat, S.; Zamd, M.; Medkouri, G.; Benghanem, M.G.; Ramdani, B. Pulmonary hypertension: Prevalence and risk factors. Int. J. Cardiol. Heart Vasc. 2016, 11, 87–89. [Google Scholar] [CrossRef]
- Maeder, M.T.; Weber, L.; Weilenmann, D.; Chronis, J.; Joerg, L.; Pohle, S.; Haager, P.K.; Brutsche, M.; Neumann, T.; Schoch, O.D.; et al. Impact of the new pulmonary hypertension definition on long-term mortality in patients with severe aortic stenosis undergoing valve replacement. Clin. Cardiol. 2021, 44, 1276–1285. [Google Scholar] [CrossRef]
- Olasińska-Wiśniewska, A.; Grodecki, K.; Urbanowicz, T.; Perek, B.; Grygier, M.; Misterski, M.; Stefaniak, S.; Mularek-Kubzdel, T.; Lesiak, M.; Jemielity, M. Pulmonary artery systolic pressure at 1-month predicts one-year survival after transcatheter aortic valve implantation. Kardiol. Pol. 2022, epub ahead of print. [Google Scholar] [CrossRef]
- Iliuta, L.; Rac-Albu, M. Predictors and late incidence of persistent or recurrent heart failure after aortic valve replacement for aortic stenosis compared with aortic regurgitation. Eur. Heart J. 2014, 35, 58. [Google Scholar]
- Iliuta, L. Impact of Severe Pulmonary Hypertension on Outcomes Late After Aortic Valve Replacement for Aortic Stenosis Compared with Aortic Regurgitation. Cardiology 2014, 128, 177. [Google Scholar]
- Johnson, L.W.; Hapanowicz, M.B.; Buonanno, C.; Bowser, M.A.; Marvasti, M.A.; Parker, F.B. Pulmonary hypertension in isolated aortic stenosis. Hemodynamic correlations and follow-up. J. Thorac. Cardiovasc. Surg. 1988, 95, 603–607. [Google Scholar] [CrossRef]
- Kapoor, N.; Varadarajan, P.; Pai, R.G. Echocardiographic predictors of pulmonary hypertension in patients with severe aortic stenosis. Eur. J. Echocardiogr. 2008, 9, 31–33. [Google Scholar] [CrossRef]
- Chen, F.; Yang, M.; Wan, C.; Liu, L.; Chen, L. Efficacy and safety of statin therapy in pulmonary hypertension: A systematic review and meta-analysis. Ann. Transl. Med. 2019, 7, 786. [Google Scholar] [CrossRef]
- Crismaru, I.; Stoian, A.P.; Bratu, O.G.; Gaman, M.A.; Stanescu, A.M.A.; Bacalbasa, N.; Diaconu, C.C. Low-density lipoprotein cholesterol lowering treatment: The current approach. Lipids Health Dis. 2020, 19, 1, 85. [Google Scholar] [CrossRef]
- Pai, R.G.; Varadarajan, P.; Kapoor, N.; Bansal, R.C. Aortic valve replacement improves survival in severe aortic stenosis associated with severe pulmonary hypertension. Ann. Thorac. Surg. 2007, 84, 80–85. [Google Scholar] [CrossRef]
- Malouf, J.F.; Enriquez-Sarano, M.; Pellikka, P.A.; Oh, J.K.; Bailey, K.R.; Chandrasekaran, K.; Mullany, C.J.; Tajik, A.J. Severe pulmonary hypertension in patients with severe aortic valve stenosis: Clinical profile and prognostic implications. J. Am. Coll. Cardiol. 2002, 40, 789–795. [Google Scholar] [CrossRef]
- Iliuta, L.; Savulescu, C.; Candea, V. Diastolic versus systolic left ventricular dysfunction as independent predictors for unfavourable postoperative evolution in patients with aortic stenosis undergoing aortic valve replacement. Eur. Heart J. 2005, 26, 193. [Google Scholar]
- Magne, J.; Mohty, D.; Piccardo, A.; Boulogne, C.; Deltreuil, M.; Petitalot, V.; Echahidi, N.; Darodes, N.; Virot, P.; Damy, T.; et al. Impact of Pulmonary Hypertension on Outcome in Patients with Severe Aortic Stenosis and Preserved Left Ventricular Ejection Fraction. Clin. Res. Cardiol. 2017, 106, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Iliuta, L. Predictors of persistent severe diastolic dysfunction after aortic valve replacement in aortic stenosis compared with aortic regurgitation. Eur. Heart J. 2012, 33, 667–668. [Google Scholar]
- El-Korashy, R.I.M.; Amin, Y.M.; Eissa, A.I.; Thabet, T.S. Echocardiography versus right heart catheterization in class I pulmonary hypertension. Egypt. J. Chest Dis. Tuberc. 2014, 63, 419–422. [Google Scholar] [CrossRef]
- Zolty, R.; Vittorio, T.; Lowes, B.; Shakar, S.; Brieke, A.; Cannon, A.; Cleveland, J.; D’Alessandro, D.; Goldstein, D.; Maybaum, S. Normalization of Fixed Pulmonary Hypertension in Severe Heart Failure Patients with Placement of Left Ventricular Assist Device. J. Heart Lung Transplant. 2008, 28, S265. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iliuta, L.; Rac-Albu, M.; Rac-Albu, M.-E.; Andronesi, A. Impact of Pulmonary Hypertension on Mortality after Surgery for Aortic Stenosis. Medicina 2022, 58, 1231. https://doi.org/10.3390/medicina58091231
Iliuta L, Rac-Albu M, Rac-Albu M-E, Andronesi A. Impact of Pulmonary Hypertension on Mortality after Surgery for Aortic Stenosis. Medicina. 2022; 58(9):1231. https://doi.org/10.3390/medicina58091231
Chicago/Turabian StyleIliuta, Luminita, Marius Rac-Albu, Madalina-Elena Rac-Albu, and Andreea Andronesi. 2022. "Impact of Pulmonary Hypertension on Mortality after Surgery for Aortic Stenosis" Medicina 58, no. 9: 1231. https://doi.org/10.3390/medicina58091231
APA StyleIliuta, L., Rac-Albu, M., Rac-Albu, M.-E., & Andronesi, A. (2022). Impact of Pulmonary Hypertension on Mortality after Surgery for Aortic Stenosis. Medicina, 58(9), 1231. https://doi.org/10.3390/medicina58091231