
Does Endoscopic Transnasal Optic Nerve Decompression Followed by Radiosurgery Improve Outcomes in the Treatment of Parasellar Meningiomas?

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Methods
2.2. Patient Characteristics
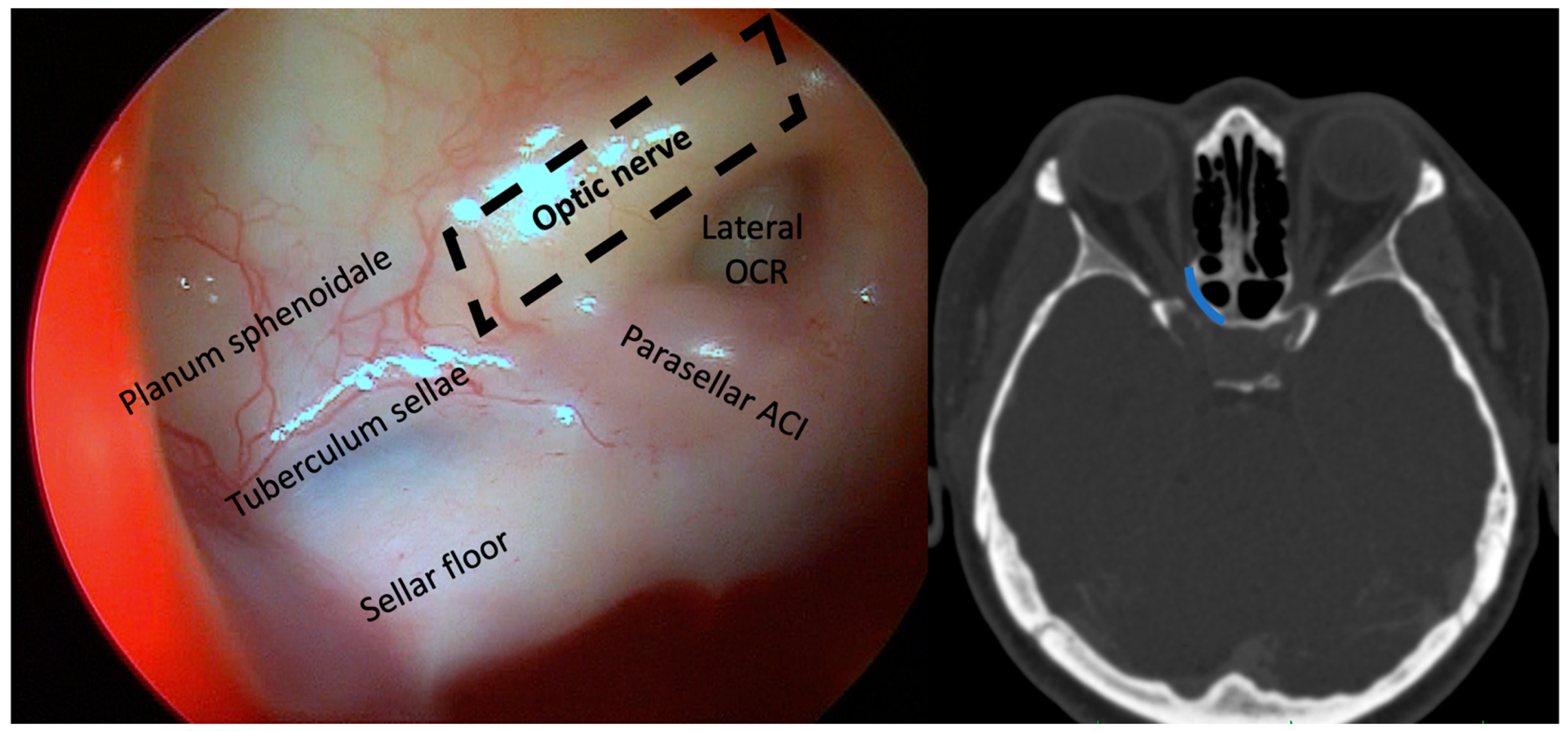
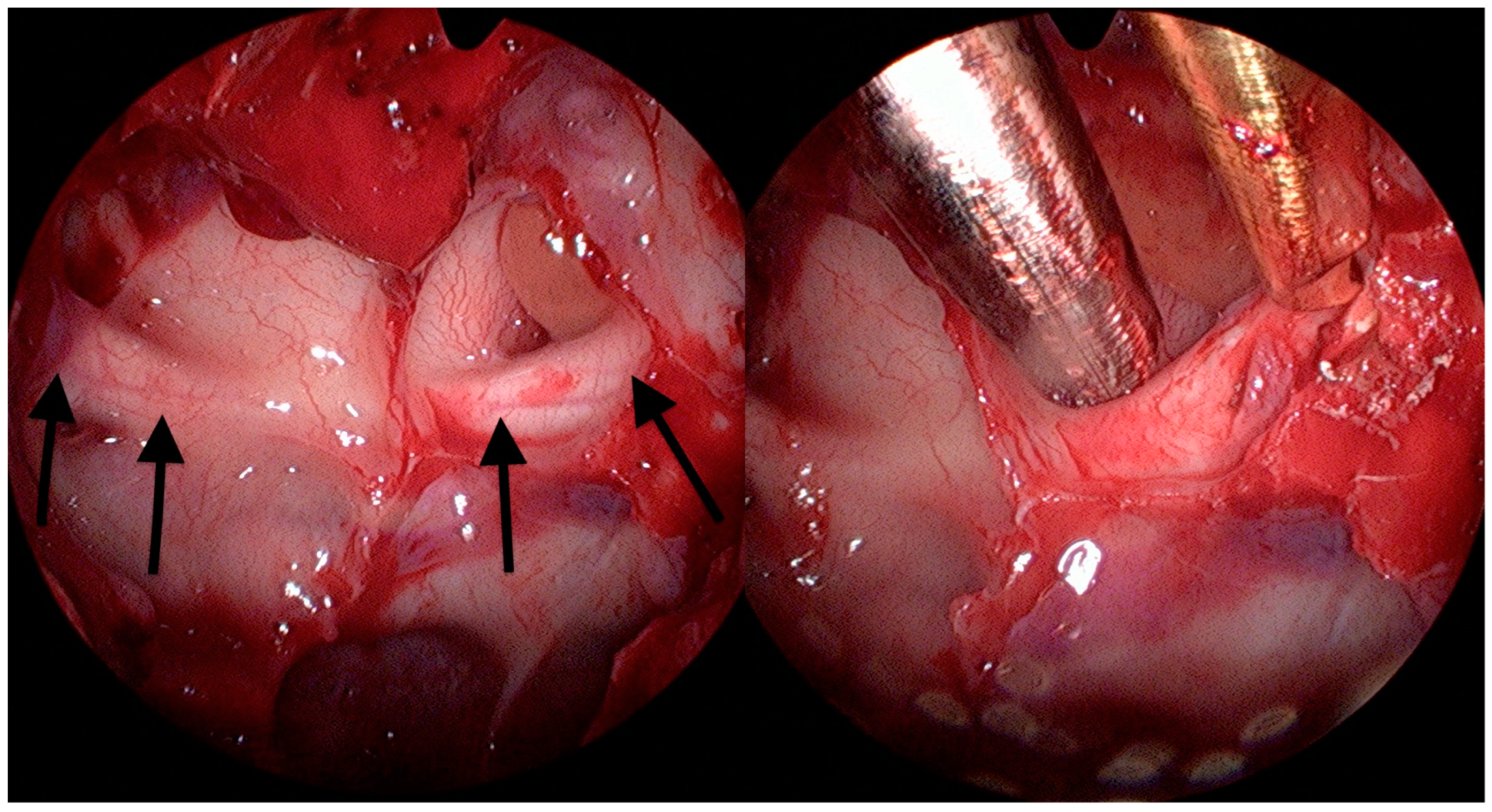
2.3. Surgical Technique
3. Results
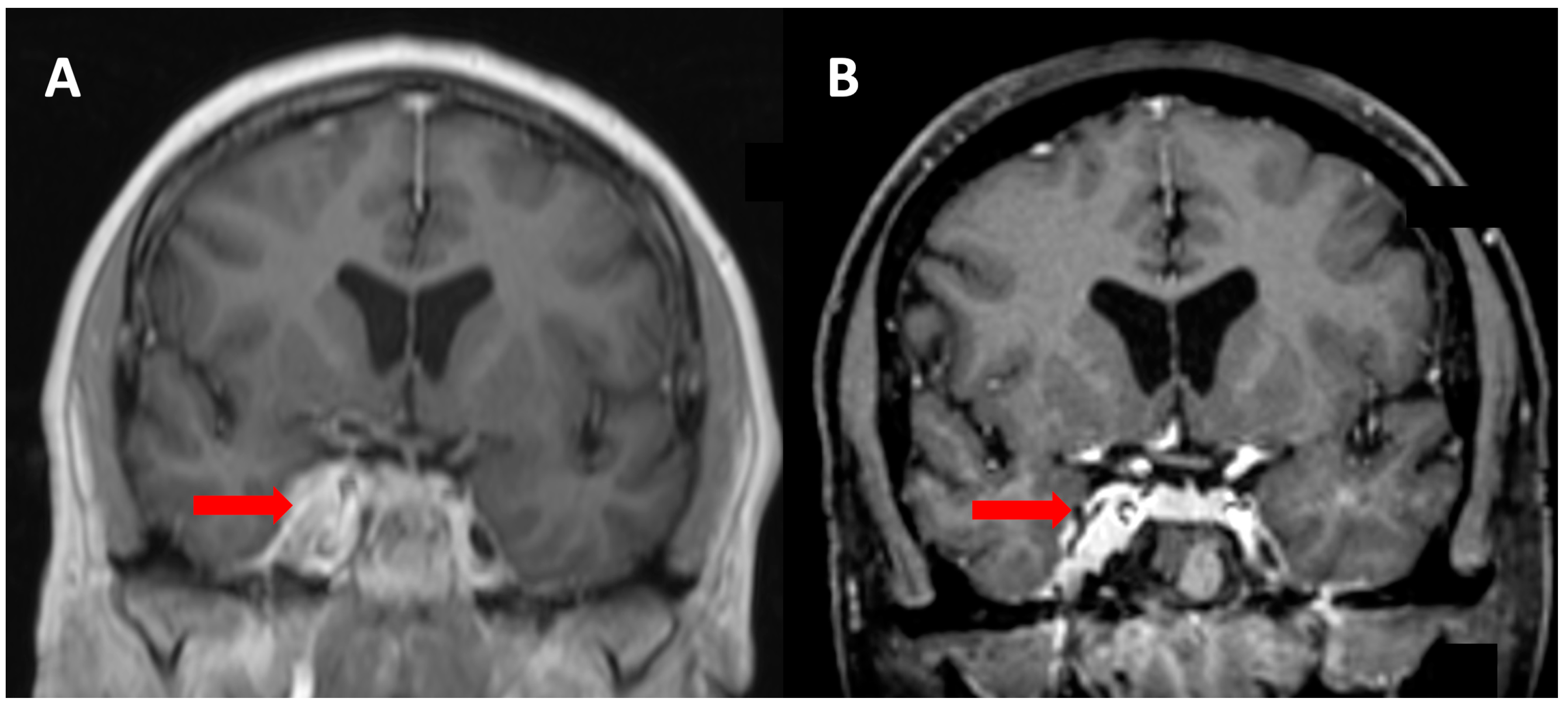
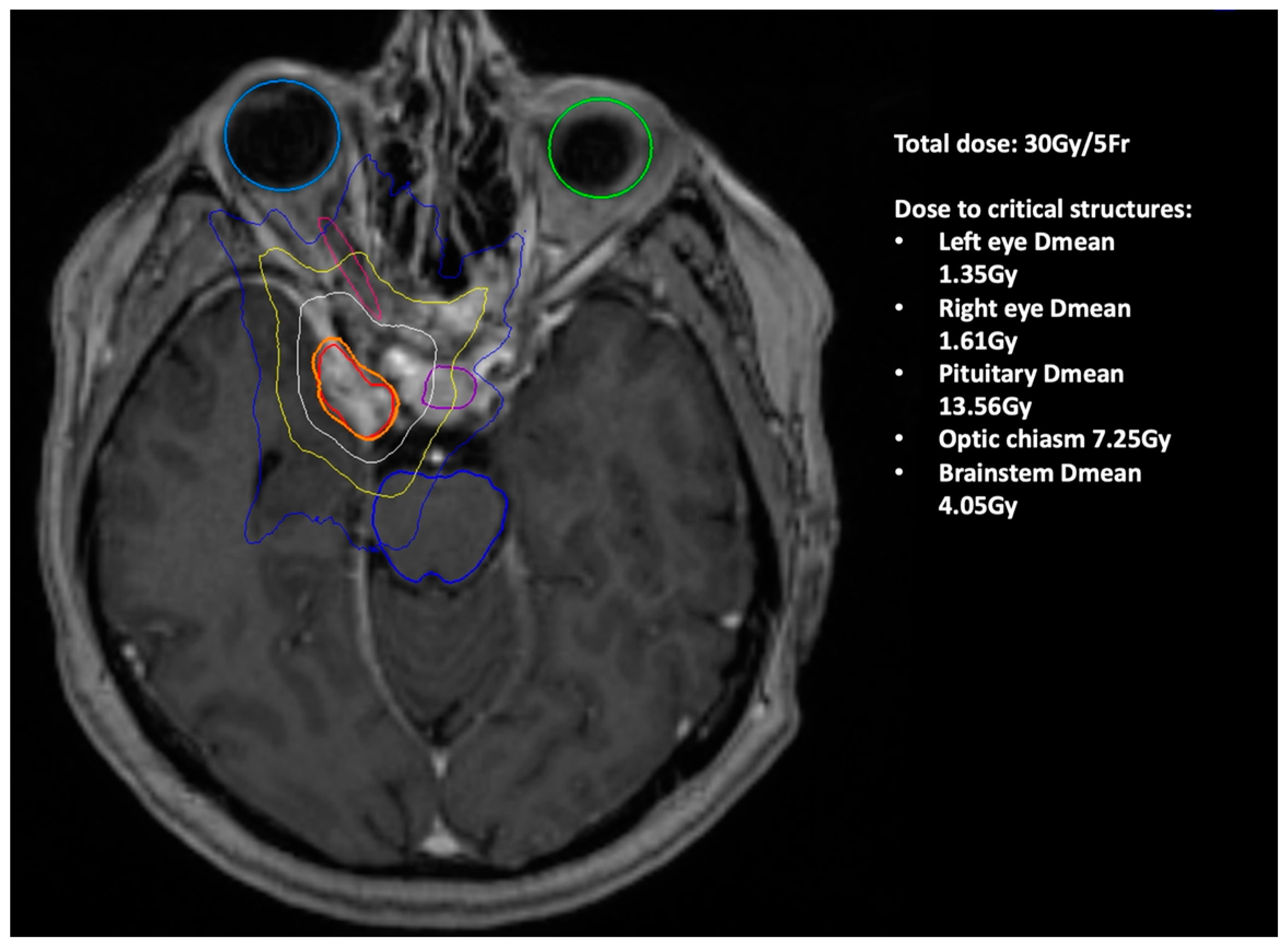
Illustrative Case Report
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Graillon, T.; Regis, J.; Barlier, A.; Brue, T.; Dufour, H.; Buchfelder, M. Parasellar Meningiomas. Neuroendocrinology 2020, 110, 780–796. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Inbar, O.; Tata, A.; Moosa, S.; Lee, C.-C.; Sheehan, J.P. Stereotactic radiosurgery in the treatment of parasellar meningiomas: Long-term volumetric evaluation. J. Neurosurg. 2018, 128, 362–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mastantuoni, C.; Cavallo, L.M.; Esposito, F.; d’Avella, E.; de Divitiis, O.; Somma, T.; Bocchino, A.; Fabozzi, G.L.; Cappabianca, P.; Solari, D. Midline Skull Base Meningiomas: Transcranial and Endonasal Perspectives. Cancers 2022, 14, 2878. [Google Scholar] [CrossRef] [PubMed]
- Avcı, E.; Aktüre, E.; Seçkin, H.; Uluç, K.; Bauer, A.M.; Izci, Y.; Morcos, J.J.; Başkaya, M.K. Level I to III craniofacial approaches based on Barrow classification for treatment of skull base meningiomas: Surgical technique, microsurgical anatomy, and case illustrations. Neurosurg. Focus 2011, 30, E5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, E.J.; Cho, Y.H.; Yoon, K.; Cho, B.; Park, E.S.; Kim, C.J.; Roh, S.W. Radiosurgical decompression for benign perioptic tumors causing compressive cranial neuropathies: A feasible alternative to microsurgery? J. Neurooncol. 2017, 131, 73–81. [Google Scholar] [CrossRef]
- Sheehan, J.P.; Starke, R.M.; Kano, H.; Kaufmann, A.M.; Mathieu, D.; Zeiler, F.A.; West, M.; Chao, S.T.; Varma, G.; Chiang, V.L.S.; et al. Gamma Knife radiosurgery for sellar and parasellar meningiomas: A multicenter study: Clinical article. J. Neurosurg. 2014, 120, 1268–1277. [Google Scholar] [CrossRef]
- Starke, R.M.; Williams, B.J.; Hiles, C.; Nguyen, J.H.; Elsharkawy, M.Y.; Sheehan, J.P. Gamma knife surgery for skull base meningiomas. J. Neurosurg. 2012, 116, 588–597. [Google Scholar] [CrossRef] [Green Version]
- Faramand, A.; Kano, H.; Niranjan, A.; Park, K.-J.; Flickinger, J.C.; Lunsford, L.D. Tumor Control and Cranial Nerve Outcomes After Adjuvant Radiosurgery for Low-Grade Skull Base Meningiomas. World Neurosurg. 2019, 127, e221–e229. [Google Scholar] [CrossRef]
- Attia, M.; Kandasamy, J.; Jakimovski, D.; Bedrosian, J.; Alimi, M.; Lee, D.L.Y.; Anand, V.K.; Schwartz, T.H. The importance and timing of optic canal exploration and decompression during endoscopic endonasal resection of tuberculum sella and planum sphenoidale meningiomas. Neurosurgery 2012, 71, 58–67. [Google Scholar] [CrossRef]
- Liu, Y.; Yu, H.; Zhen, H. Navigation-assisted, endonasal, endoscopic optic nerve decompression for the treatment of nontraumatic optic neuropathy. J. Cranio Maxillofac. Surg. 2019, 47, 328–333. [Google Scholar] [CrossRef]
- Lund, V.J.; Rose, G.E. Endoscopic transnasal orbital decompression for visual failure due to sphenoid wing meningioma. Eye Lond. Engl. 2006, 20, 1213–1219. [Google Scholar] [CrossRef] [PubMed]
- Maza, G.; Subramaniam, S.; Yanez-Siller, J.C.; Otto, B.A.; Prevedello, D.M.; Carrau, R.L. The Role of Endonasal Endoscopic Optic Nerve Decompression as the Initial Management of Primary Optic Nerve Sheath Meningiomas. J. Neurol. Surg. Part B Skull Base. 2019, 80, 568–576. [Google Scholar] [CrossRef]
- Ryu, G.; Al-Magribi, A.Z.; Lee, K.E.; Lee, J.J.; Kim, S.B.; Kim, H.Y.; Dhong, H.-J.; Chung, S.-K.; Kong, D.-S.; Hong, S.D. Endoscopic Optic Nerve Decompression for Optic Neuropathy in Sinonasal Fibro-Osseous Tumors. World Neurosurg. 2020, 138, e260–e266. [Google Scholar] [CrossRef] [PubMed]
- Krayenbühl, N.; Hafez, A.; Hernesniemi, J.A.; Krisht, A.F. Taming the cavernous sinus: Technique of hemostasis using fibrin glue. Neurosurgery 2007, 61, E52, discussion E52. [Google Scholar] [CrossRef] [PubMed]
- DeMonte, F.; Smith, H.K.; Al-Mefty, O. Outcome of aggressive removal of cavernous sinus meningiomas. J. Neurosurg. 1994, 81, 245–251. [Google Scholar] [CrossRef]
- Couldwell, W.T.; Kan, P.; Liu, J.K.; Apfelbaum, R.I. Decompression of cavernous sinus meningioma for preservation and improvement of cranial nerve function: Technical note. J. Neurosurg. 2006, 105, 148–152. [Google Scholar] [CrossRef]
- Lobo, B.; Zhang, X.; Barkhoudarian, G.; Griffiths, C.F.; Kelly, D.F. Endonasal Endoscopic Management of Parasellar and Cavernous Sinus Meningiomas. Neurosurg. Clin. N. Am. 2015, 26, 389–401. [Google Scholar] [CrossRef]
- Starnoni, D.; Tuleasca, C.; Levivier, M.; Daniel, R.T. Surgery for clinoidal meningiomas with cavernous sinus extension: Near-total excision and chiasmopexy. Acta Neurochir. (Wien) 2022. [Google Scholar] [CrossRef]
- Berhouma, M.; Jacquesson, T.; Abouaf, L.; Vighetto, A.; Jouanneau, E. Endoscopic endonasal optic nerve and orbital apex decompression for nontraumatic optic neuropathy: Surgical nuances and review of the literature. Neurosurg. Focus 2014, 37, E19. [Google Scholar] [CrossRef] [Green Version]
- Fukado, Y.; Hamada, Y.; Miyashita, S.; Okamoto, M. Remote results of surgery for decompression of the optic canal. Rinsho Ganka Jpn. J. Clin. Ophthalmol. 1963, 17, 617–619. [Google Scholar]
- Koutourousiou, M.; Fernandez-Miranda, J.C.; Stefko, S.T.; Wang, E.W.; Snyderman, C.H.; Gardner, P.A. Endoscopic endonasal surgery for suprasellar meningiomas: Experience with 75 patients: Clinical article. J. Neurosurg. 2014, 120, 1326–1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitano, M.; Taneda, M.; Nakao, Y. Postoperative improvement in visual function in patients with tuberculum sellae meningiomas: Results of the extended transsphenoidal and transcranial approaches. J. Neurosurg. 2007, 107, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Sencer, A.; Akcakaya, M.O.; Basaran, B.; Yorukoglu, A.G.; Aydoseli, A.; Aras, Y.; Sencan, F.; Satana, B.; Aslan, I.; Unal, O.F.; et al. Canbolat, Unilateral endoscopic optic nerve decompression for idiopathic intracranial hypertension: A series of 10 patients. World Neurosurg. 2014, 82, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Inbar, O.; Lee, C.; Schlesinger, D.; Xu, Z.; Sheehan, J.P. Long-Term Results of Stereotactic Radiosurgery for Skull Base Meningiomas. Neurosurgery 2016, 79, 58–68. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Best-Corrected Visual Acuity | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case Number | Sex/Age | Meningioma Type | Who Grade | Eye | Associated Surgery Type | Previous Transcran. Surgery | Preoperative | Postoperative | Postop. Visual Field Test | Other Cranial Nerves Lesion | Srs * | Surgical Complications | Follow-Up (Months) |
| 1. | F/60 | Cavernous sinus | I | right | biopsy | No | 20/400 | 20/50 | improved | None | Yes | None | 54 |
| 2. | M/66 | Petroclival | I | right | extradural portion resection | Yes | 20/200 | 20/200 | stable | None | Yes | None | 22 |
| 3. | F/57 | Spheno-orbital | I | left | transorbital, endoscopic resection | No | 20/30 | 20/30 | normal | None | No | None | 31 |
| 4. | F/66.5 | Spheno-orbital | I | right | biopsy | Yes | 20/20 | 20/20 | normal | Blindness, CN III, VI left | No | None | 6 |
| 5. | M/46.5 | Tuberculum sellae and planum sphenoidale | I | bilaterally | extended approach | Yes | Right: 20/100 Left: 20/200 | Right: 20/20 Left: 20/50 | improved | None | Yes | None | 14 |
| 6. | F/75 | Spheno-orbital | I | left | extradural portion resection | Yes | Hand motion | 20/100 | improved | CN V left | No | None | 6 |
| 7. | M/58 | Cavernous sinus | I | left | none | Yes | Finger count/20 cm | 20/70 | improved | None | Yes | None | 23 |
| 8. | M/59 | Optic nerve sheat | N/A | right | none | No | 20/200 | 20/70 | improved | None | Yes | None | 27 |
| 9. | F/44 | Spheno-orbital | I | bilaterally | none | Yes | Right: 20/200 Left: finger count/20 cm | Right: 20/70 Left: 20/100 | improved | None | Yes | None | 34 |
| 10. | F/39 | Spheno-orbital | N/A | right | biopsy | No | 20/100 | 20/40 | improved | CN III, VI right | Yes | None | 28 |
| 11. | F/36 | Cavernous sinus | III | right | extended approach | Yes | 20/70 | 20/30 | improved | Blindness, V left | Yes | None | 86 |
| 12. | M/55 | Cavernous sinus | I | right | biopsy | No | 20/50 | 20/50 | stable | CN III, V right | Yes | None | 21 |
| Case Number | Sex/Age | Dosage (gy) | Fractions | PTV (cm3) | Isodose | Associated Complications (CN Deficit) | Tumor Response |
|---|---|---|---|---|---|---|---|
| 1. | F/60 | 30 | 5 | 5.13 | 66 | none | regression |
| 2. | M/66 | 25 | 5 | 33.47 | 61 | none | stable |
| 5. | M/46.5 | 30 | 6 | 9.3 | 71 | none | regression |
| 7. | M/58 | 30 | 5 | 6.41 | 65 | none | stable |
| 8. | M/59 | 25 | 5 | 0.521 | 74 | none | regression |
| 9. | F/44 | 30 | 5 | 5.96 | 61 | none | stable |
| 10. | F/39 | 30 | 5 | 17.01 | 65 | none | stable |
| 11. | F/36 | 80 | 5 | 11.6 | 82 | none | regression (after last SRS) |
| 3 | 15.84 | 62 | |||||
| 12. | M/55 | 30 | 5 | 7.65 | 73 | none | regression |
| Case Number | Tumor Volume Pre Etond (cm3) | Associated Surgery Type | Tumor Volume Pre Srs/Post-Surgery (cm3) | End of Follow-up Volume (cm3) | Follow-Up (Months) |
|---|---|---|---|---|---|
| 1. | 5.13 | biopsy | 5.13 | 3.69 | 54 |
| 2. | 37.82 | extradural portion resection | 33.47 | 32.9 | 22 |
| 3. | 24.8 | transorbital, endoscopic resection | 17.2 | 17.1 | 31 |
| 4. | 16.56 | biopsy | 16.56 | 16.56 | 6 |
| 5. | 12.8 | extended approach | 9.3 | 5.4 | 14 |
| 6. | 18.8 | extradural portion resection | 15.4 | 15.4 | 6 |
| 7. | 6.41 | none | 6.41 | 6.11 | 23 |
| 8. | 0.521 | none | 0.521 | 0.42 | 27 |
| 9. | 5.96 | none | 5.96 | 5.9 | 34 |
| 10. | 17 | biopsy | 17.01 | 17 | 28 |
| 11. | 19.31 | extended approach | 15.84 | 11.8 | 86 |
| 12. | 7.6 | biopsy | 7.65 | 6.2 | 21 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matoušek, P.; Cvek, J.; Čábalová, L.; Misiorzová, E.; Krejčí, O.; Lipina, R.; Krejčí, T. Does Endoscopic Transnasal Optic Nerve Decompression Followed by Radiosurgery Improve Outcomes in the Treatment of Parasellar Meningiomas? Medicina 2022, 58, 1137. https://doi.org/10.3390/medicina58081137
Matoušek P, Cvek J, Čábalová L, Misiorzová E, Krejčí O, Lipina R, Krejčí T. Does Endoscopic Transnasal Optic Nerve Decompression Followed by Radiosurgery Improve Outcomes in the Treatment of Parasellar Meningiomas? Medicina. 2022; 58(8):1137. https://doi.org/10.3390/medicina58081137
Chicago/Turabian StyleMatoušek, Petr, Jakub Cvek, Lenka Čábalová, Eva Misiorzová, Ondřej Krejčí, Radim Lipina, and Tomáš Krejčí. 2022. "Does Endoscopic Transnasal Optic Nerve Decompression Followed by Radiosurgery Improve Outcomes in the Treatment of Parasellar Meningiomas?" Medicina 58, no. 8: 1137. https://doi.org/10.3390/medicina58081137
APA StyleMatoušek, P., Cvek, J., Čábalová, L., Misiorzová, E., Krejčí, O., Lipina, R., & Krejčí, T. (2022). Does Endoscopic Transnasal Optic Nerve Decompression Followed by Radiosurgery Improve Outcomes in the Treatment of Parasellar Meningiomas? Medicina, 58(8), 1137. https://doi.org/10.3390/medicina58081137