
Evolving Risk of Acute Kidney Injury in COVID-19 Hospitalized Patients: A Single Center Retrospective Study


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Hansrivijit, P.; Qian, C.; Boonpheng, B.; Thongprayoon, C.; Vallabhajosyula, S.; Cheungpasitporn, W.; Ghahramani, N. Incidence of acute kidney injury and its association with mortality in patients with COVID-19: A meta-analysis. J. Investig. Med. 2020, 68, 1261–1270. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; the Northwell COVID-19 Research Consortium; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, X.; Chen, H.; Yan, S.; Li, D.; Li, Y.; Gong, Z. Coronavirus Disease 19 Infection Does Not Result in Acute Kidney Injury: An Analysis of 116 Hospitalized Patients from Wuhan, China. Am. J. Nephrol. 2020, 51, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Khalili, S.; Sabaghian, T.; Sedaghat, M.; Soroureddin, Z.; Askari, E.; Khalili, N. Prevalence, Risk Factors and Outcomes Associated with Acute Kidney Injury in Patients Hospitalized for COVID-19: A Comparative Study between Diabetic and Nondiabetic Patients. J. Diabetes Res. 2021, 2021, 6666086. [Google Scholar] [CrossRef] [PubMed]
- WHO. Laboratory Testing of 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases: Interim Guidance, 17 January 2020; WHO: Geneva, Switzerland, 2020.
- Masoud, H.; Zaky, S.; Baki, A.; Ibrahim, H.; Amin, W. Ministry of Health and Population, Egypt. Management Protocol for COVID-19 Patients Version 1.4; Ministry of Health and Population (MOHP): Cairo, Egypt, 2020.
- Disease, K.J.K.I.S. Improving global outcomes (KDIGO) acute kidney injury work group: KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Vincent, J.-L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.; Suter, P.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, L.M.; Weinberg, J.; Keaney, J.F., Jr. Common Statistical Pitfalls in Basic Science Research. J. Am. Heart Assoc. 2016, 5, e004142. [Google Scholar] [CrossRef]
- Gaetano, A.; Annachiara, F.; Francesco, F.; Giacomo, M.; Riccardo, M.; Marianna, M.; Erica, F.; Marianna, M.; Gianluca, C.; Gabriella, O.J.m. Incidence, risk factors and outcome of acute kidney injury (AKI) in patients with COVID-19. Clin. Exp. Nephrol. 2021, 25, 1203–1214. [Google Scholar] [CrossRef]
- Li, Z.; Wu, M.; Yao, J.; Guo, J.; Liao, X.; Song, S.; Li, J.; Duan, G.; Zhou, Y.; Wu, X.; et al. Caution on Kidney Dysfunctions of COVID-19 Patients. medRxiv 2020. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Prasad, N.; Agrawal, S.K.; COVID-19 Working Group of Indian Society of Nephrology. COVID 19 and Acute Kidney Injury. Indian J. Nephrol. 2020, 30, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Reis, T. Kidney involvement in COVID-19 and rationale for extracorporeal therapies. Nat. Rev. Nephrol. 2020, 16, 308–310. [Google Scholar] [CrossRef] [Green Version]
- Bhatraju, P.K.; Zelnick, L.R.; Shlipak, M.; Katz, R.; Kestenbaum, B. Association of Soluble TNFR-1 Concentrations with Long-Term Decline in Kidney Function: The Multi-Ethnic Study of Atherosclerosis. J. Am. Soc. Nephrol. 2018, 29, 2713–2721. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.M.; Xu, G.; Wang, B.; Liu, B.C. Cytokine storm syndrome in coronavirus disease 2019: A narrative review. J. Intern. Med. 2021, 289, 147–161. [Google Scholar] [CrossRef] [PubMed]
- Rezoagli, E.; McNicholas, B.; Pham, T.; Bellani, G.; Laffey, J.G. Lung-kidney cross-talk in the critically ill: Insights from the Lung Safe study. Intensive Care Med. 2020, 46, 1072–1073. [Google Scholar] [CrossRef] [PubMed]
- Diao, B.; Wang, C.; Wang, R.; Feng, Z.; Tan, Y.; Wang, H.; Wang, C.; Liu, L.; Liu, Y.; Liu, Y.; et al. Human Kidney is a Target for Novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. medRxiv 2020. [CrossRef] [Green Version]
- Joseph, A.; Zafrani, L.; Mabrouki, A.; Azoulay, E.; Darmon, M. Acute kidney injury in patients with SARS-CoV-2 infection. Ann. Intensive Care 2020, 10, 117. [Google Scholar] [CrossRef]
- Taher, A.; Alalwan, A.A.; Naser, N.; Alsegai, O.; Alaradi, A. Acute Kidney Injury in COVID-19 Pneumonia: A Single-Center Experience in Bahrain. Cureus 2020, 12, e9693. [Google Scholar] [CrossRef]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Lee, J.; Johnson, A.E.; Mark, R.G.; Celi, L.A.; Danziger, J. Right Ventricular Function, Peripheral Edema, and Acute Kidney Injury in Critical Illness. Kidney Int. Rep. 2017, 2, 1059–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Post, A.; den Deurwaarder, E.S.G.; Bakker, S.J.L.; de Haas, R.J.; van Meurs, M.; Gansevoort, R.T.; Berger, S.P. Kidney Infarction in Patients With COVID-19. Am. J. Kidney Dis. 2020, 76, 431–435. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with COVID-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Su, H.; Yang, M.; Wan, C.; Yi, L.-X.; Tang, F.; Zhu, H.-Y.; Yi, F.; Yang, H.-C.; Fogo, A.B.; Nie, X.; et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef]
- Connors, J.M.; Levy, J.H. Thromboinflammation and the hypercoagulability of COVID-19. J. Thromb. Haemost. 2020, 18, 1559–1561. [Google Scholar] [CrossRef]
- Mohamed, M.M.B.; Lukitsch, I.; Torres-Ortiz, A.E.; Walker, J.B.; Varghese, V.; Hernandez-Arroyo, C.F.; Alqudsi, M.; LeDoux, J.R.; Velez, J.C.Q. Acute Kidney Injury Associated with Coronavirus Disease 2019 in Urban New Orleans. Kidney360 2020, 1, 614–622. [Google Scholar] [CrossRef]
- Panitchote, A.; Mehkri, O.; Hastings, A.; Hanane, T.; Demirjian, S.; Torbic, H.; Mireles-Cabodevila, E.; Krishnan, S.; Duggal, A. Factors associated with acute kidney injury in acute respiratory distress syndrome. Ann. Intensive Care 2019, 9, 74. [Google Scholar] [CrossRef]
- Gabarre, P.; Dumas, G.; Dupont, T.; Darmon, M.; Azoulay, E.; Zafrani, L. Acute kidney injury in critically ill patients with COVID-19. Intensive Care Med. 2020, 46, 1339–1348. [Google Scholar] [CrossRef]
- Yang, Q.; Yang, X. Incidence and risk factors of kidney impairment on patients with COVID-19: A systematic review and meta-analysis. medRxiv 2020. [CrossRef]
- Jin, M.; Tong, Q. Rhabdomyolysis as Potential Late Complication Associated with COVID-19. Emerg. Infect. Dis. 2020, 26, 1618–1620. [Google Scholar] [CrossRef]
- Kormann, R.; Jacquot, A.; Alla, A.; Corbel, A.; Koszutski, M.; Voirin, P.; Garcia Parrilla, M.; Bevilacqua, S.; Schvoerer, E.; Gueant, J.-L.; et al. Coronavirus disease 2019: Acute Fanconi syndrome precedes acute kidney injury. Clin. Kidney J. 2020, 13, 362–370. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Vardeny, O.; Michel, T.; McMurray, J.J.V.; Pfeffer, M.A.; Solomon, S.D. Renin-Angiotensin-Aldosterone System Inhibitors in Patients with COVID-19. N. Engl. J. Med. 2020, 382, 1653–1659. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Naicker, S.; Yang, C.-W.; Hwang, S.-J.; Liu, B.-C.; Chen, J.-H.; Jha, V. The Novel Coronavirus 2019 epidemic and kidneys. Kidney Int. 2020, 97, 824–828. [Google Scholar] [CrossRef]
- Martinez-Rojas, M.A.; Vega-Vega, O.; Bobadilla, N.A. Is the kidney a target of SARS-CoV-2? Am. J. Physiol. Ren. Physiol. 2020, 318, F1454–F1462. [Google Scholar] [CrossRef]
- Chan, L.; Chaudhary, K.; Saha, A.; Chauhan, K.; Vaid, A.; Zhao, S.; Paranjpe, I.; Somani, S.; Richter, F.; Miotto, R.; et al. AKI in Hospitalized Patients with COVID-19. J. Am. Soc. Nephrol. 2021, 32, 151–160. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e278. [Google Scholar] [CrossRef]
- Wang, K.; Chen, W.; Zhou, Y.-S.; Lian, J.-Q.; Zhang, Z.; Du, P.; Gong, L.; Zhang, Y.; Cui, H.-Y.; Geng, J.-J.; et al. SARS-CoV-2 invades host cells via a novel route: CD147-spike protein. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Zhang, Y.; Zeng, X.; Chen, H.; Chen, Y.; Yang, D.; Shen, Z.; Wang, X.; Liu, X.; Xiong, M.; et al. Kidney injury molecule-1 is a potential receptor for SARS-CoV-2. J. Mol. Cell Biol. 2021, 13, 185–196. [Google Scholar] [CrossRef]
- Helms, L.; Marchiano, S.; Stanaway, I.B.; Hsiang, T.-Y.; Juliar, B.A.; Saini, S.; Zhao, Y.T.; Khanna, A.; Menon, R.; Alakwaa, F.J.J.i. Cross-validation of SARS-CoV-2 responses in kidney organoids and clinical populations. JCI Insight 2021, 6, e154882. [Google Scholar] [CrossRef]
- Feder, K.A.; Pearlowitz, M.; Goode, A.; Duwell, M.; Williams, T.W.; Chen-Carrington, P.A.; Patel, A.; Dominguez, C.; Keller, E.N.; Klein, L.J.M.; et al. Linked clusters of SARS-CoV-2 variant B. 1.351—Maryland, January–February 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 627. [Google Scholar] [CrossRef]
- Firestone, M.J.; Lorentz, A.J.; Meyer, S.; Wang, X.; Como-Sabetti, K.; Vetter, S.; Smith, K.; Holzbauer, S.; Beaudoin, A.; Garfin, J.J.M.; et al. First identified cases of SARS-CoV-2 variant P. 1 in the United States—Minnesota, January 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 346. [Google Scholar] [CrossRef]
- Galloway, S.E.; Paul, P.; MacCannell, D.R.; Johansson, M.A.; Brooks, J.T.; MacNeil, A.; Slayton, R.B.; Tong, S.; Silk, B.J.; Armstrong, G.L.J.M.; et al. Emergence of SARS-CoV-2 b. 1.1. 7 lineage—united states, december 29, 2020–january 12, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 95. [Google Scholar] [CrossRef]
- Bedford, T.; Greninger, A.L.; Roychoudhury, P.; Starita, L.M.; Famulare, M.; Huang, M.-L.; Nalla, A.; Pepper, G.; Reinhardt, A.; Xie, H.J.S. Cryptic transmission of SARS-CoV-2 in Washington state. Science 2020, 370, 571–575. [Google Scholar] [CrossRef]
- Rabb, H. Kidney diseases in the time of COVID-19: Major challenges to patient care. J. Clin. Investig. 2020, 130, 2749–2751. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D.; Northwell, C.-R.C.; et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020, 98, 209–218. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | Serum Creatinine | Urine Output |
|---|---|---|
| 1 | 1.5–1.9 folds baseline OR ≥0.3 mg/dL increase | <0.5 mL/kg/h for 6–12 h |
| 2 | 2.0–2.9 folds baseline | <0.5 mL/kg/h for ≥12 h |
| 3 | 3 folds baseline OR Increase in serum creatinine to ≥4.0 mg/dL OR Initiation of renal replacement therapy | <0.3 mL/kg/h for ≥24 h OR Anuria for ≥12 h |
| SOFA Score | 0 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|
| PaO2/FiO2 (mmHg) | >400 | <400 | <300 | <200 with respiratory support | <100 with respiratory support |
| Platelet (×109/L) | ≥150 | 100–149 | 50–99 | 20–49 | <20 |
| Bilirubin (mg/dL) | <1.2 | 1.2–1.9 | 2.0–5.9 | 6.0–11.9 | ≥12.0 |
| Hypotension | No hypotension | MAP < 70 mmHg | Dopamine ≤ 5 or dobutamine (any dose) | Dopamine > 5, epinephrine ≤ 0.1, or norepinephrine ≤0.1 | Dopamine > 15, epinephrine > 0.1, or norepinephrine > 0.1 |
| Glasgow Coma Score | 15 | 13–14 | 10–12 | 6–9 | <6 |
| Creatinine (mg/dL) | <1.2 | 1.2–1.9 | 2.0–3.4 | 3.5–4.9 | ≥5.0 |
| Variables | Total Patients | Non-AKI Group | AKI Group | p-Value |
|---|---|---|---|---|
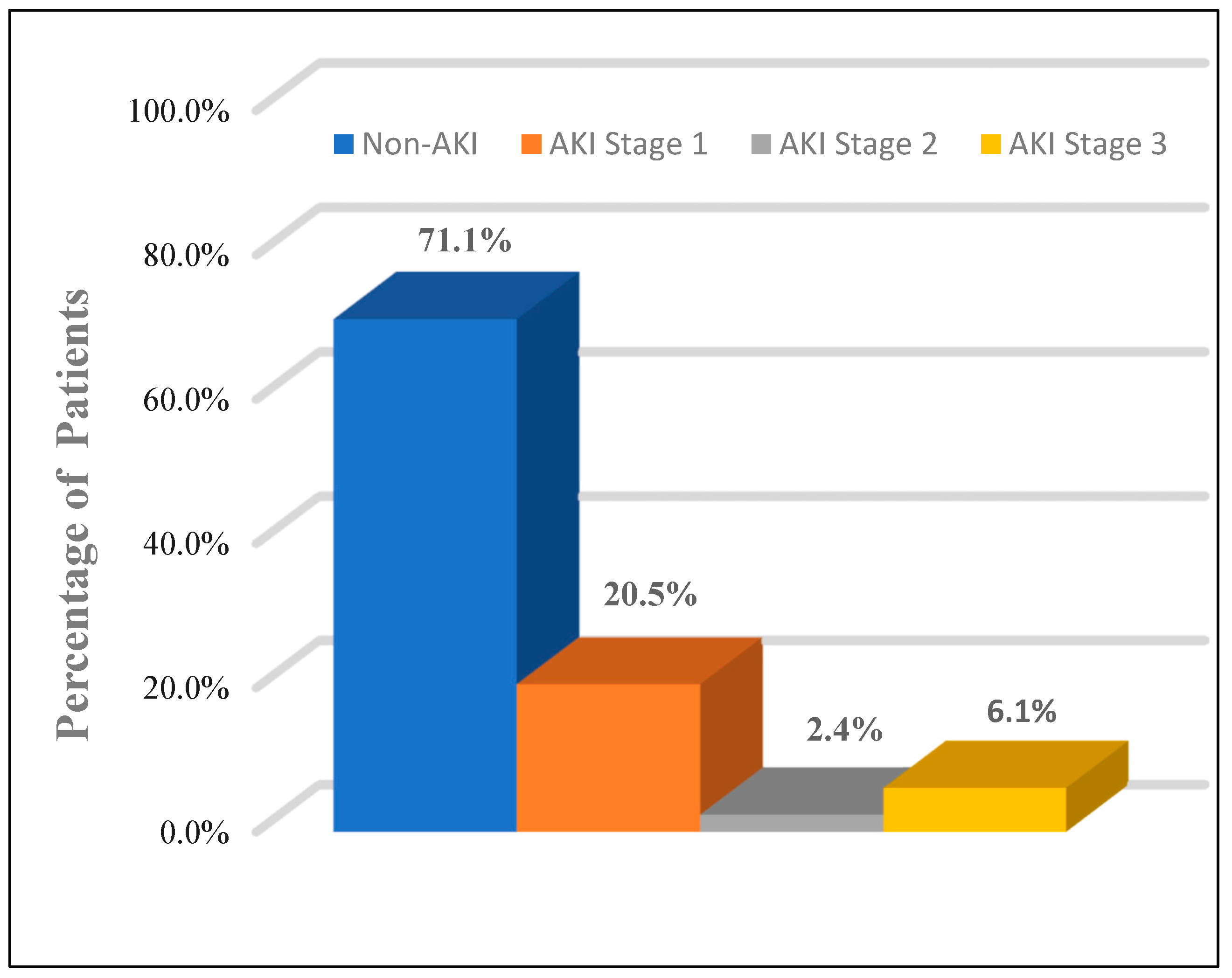
| No. of patients (%) | 83 (100.0%) | 59 (71.1%) | 24 (28.9%) | - |
| Age (years) (mean ± SD) | 52.9 ± 12.4 | 51.07 ± 12.5 | 57.71 ± 11.0 | - |
| Sex, n (%) | - | |||
| Male | 46 (55.4%) | 32 (54.2%) | 14 (58.3%) | - |
| Female | 37 (44.6%) | 27 (45.8%) | 10 (41.7%) | - |
| Comorbid conditions, n (%) | - | |||
| Cardiovascular diseases | 10 (12.1%) | 6 (10.2%) | 4 (16.6%) | - |
| Chronic liver diseases | 3 (3.6) | 2 (3.4%) | 1 (4.1%) | - |
| Chronic obstructive lung diseases | 7 (8.4%) | 5 (8.2%) | 2 (8.5%) | - |
| Diabetes mellitus | 19 (22.9%) | 12 (20.3%) | 7 (29.2%) | - |
| Hypertension | 23 (27.7%) | 15 (25.4%) | 8 (33.3%) | - |
| Mean arterial pressure (mmHg) | 90.1 ± 5.4 | 90.6 ± 4.2 | 88.7 ± 7.5 | 0.222 |
| Variables | Total Patients | Non-AKI Group | AKI Group | p-Value |
|---|---|---|---|---|
| Lab Test, Mean (±SD) | ||||
| Hemoglobin (g/dL) | 12.5 ± 2.1 | 12.8 ± 2.1 | 12.1 ± 1.9 | 0.175 |
| White blood cells (×109/L) | 7.8 ± 4.3 | 7.9 ± 4.2 | 7.5 ± 4.7 | 0.635 |
| Lymphocyte (×109/L) | 1.2 ± 0.5 | 1.3 ± 0.6 | 1 ± 0.3 | 0.076 |
| Neutrophil (×109/L) | 5.9 ± 3.7 | 5.9 ± 3.6 | 5.8 ± 3.9 | 0.908 |
| Platelet (×109/L) | 262.4 ± 89.4 | 283.6 ± 95.8 | 241.2 ± 83.2 | 0.216 |
| Albumin (g/dL) | 3.8 ± 0.6 | 3.8 ± 0.6 | 3.7 ± 0.7 | 0.359 |
| Total bilirubin (mg/dL) | 0.97 ± 0.3 | 0.9 ± 0.2 | 1.03 ± 0.3 | 0.112 |
| Alanine aminotransferase (IU/L) | 44.9 ± 22.2 | 43.6 ± 16.5 | 48 ± 32.5 | 0.415 |
| Aspartate aminotransferase (IU/L) | 39.5 ± 15.9 | 38.8 ± 13 | 41.4 ± 21.5 | 0.496 |
| Prothrombin time (seconds) | 13.1 ± 1.1 | 13 ± 0.9 | 13.3 ± 1.4 | 0.279 |
| Partial thromboplastin time (seconds) | 30.5 ± 4.3 | 30.5 ± 4.5 | 30.7 ± 3.7 | 0.811 |
| Ferritin (ng/mL) | 582.9 ± 182.3 | 575.3 ± 169.9 | 601.1 ± 193.8 | 0.565 |
| C-reactive protein (mg/L) | 8.28 ± 3.13 | 8.04 ± 3.02 | 8.87 ± 3.39 | 0.275 |
| D-dimer (ng/mL) | 422.94 ± 75.18 | 416.53 ± 68.81 | 438.81 ± 88.54 | 0.223 |
| Serum Na (mmol/L) | 138.6 ± 6.4 | 139.3 ± 5.9 | 136.8 ± 6.9 | 0.107 |
| Serum K (mmol/L) | 4.3 ± 0.7 | 4.23 ± 0.7 | 4.59 ± 0.7 | 0.099 |
| Serum Ca (mg/dL) | 8.1 ± 0.5 | 8.12 ± 0.5 | 8.14 ± 0.5 | 0.909 |
| Serum Urea (mg/dL) | 90.5 ± 50.3 | 86.5 ± 46.1 | 100.3 ± 59.4 | 0.261 |
| Serum Creatinine (mg/dL) | 1.7 ± 1.3 | 1.5 ± 0.8 | 2.5 ± 1.9 | 0.007 * |
| PaO2/FiO2 (mmHg) | 412.02 ± 29.43 | 416.49 ± 28.46 | 401.33 ± 29.81 | 0.029 * |
| SOFA Score | 1.48 ± 0.79 | 1.33 ± 0.66 | 1.88 ± 0.95 | 0.004 * |
| KDIGO stage | ||||
| Stage 1 | 17 (20.5%) | 0 (0) | 17 (70.8%) | - |
| Stage 2 | 2 (2.4%) | 0 (0) | 2 (8.3%) | - |
| Stage 3 | 5 (6.1%) | 0 (0) | 5 (20.9%) | - |
| Proteinuria on hospital admission | ||||
| Positive | 26 (31.3%) | 15 (25.4%) | 11 (45.8%) | 0.287 |
| Negative | 57 (68.7%) | 44 (74.6%) | 13 (54.2%) | - |
| Hematuria on hospital admission | ||||
| Positive | 16 (19.3%) | 10 (16.9%) | 6 (25%) | 0.703 |
| Negative | 67 (80.7%) | 49 (83.1%) | 18 (75%) | - |
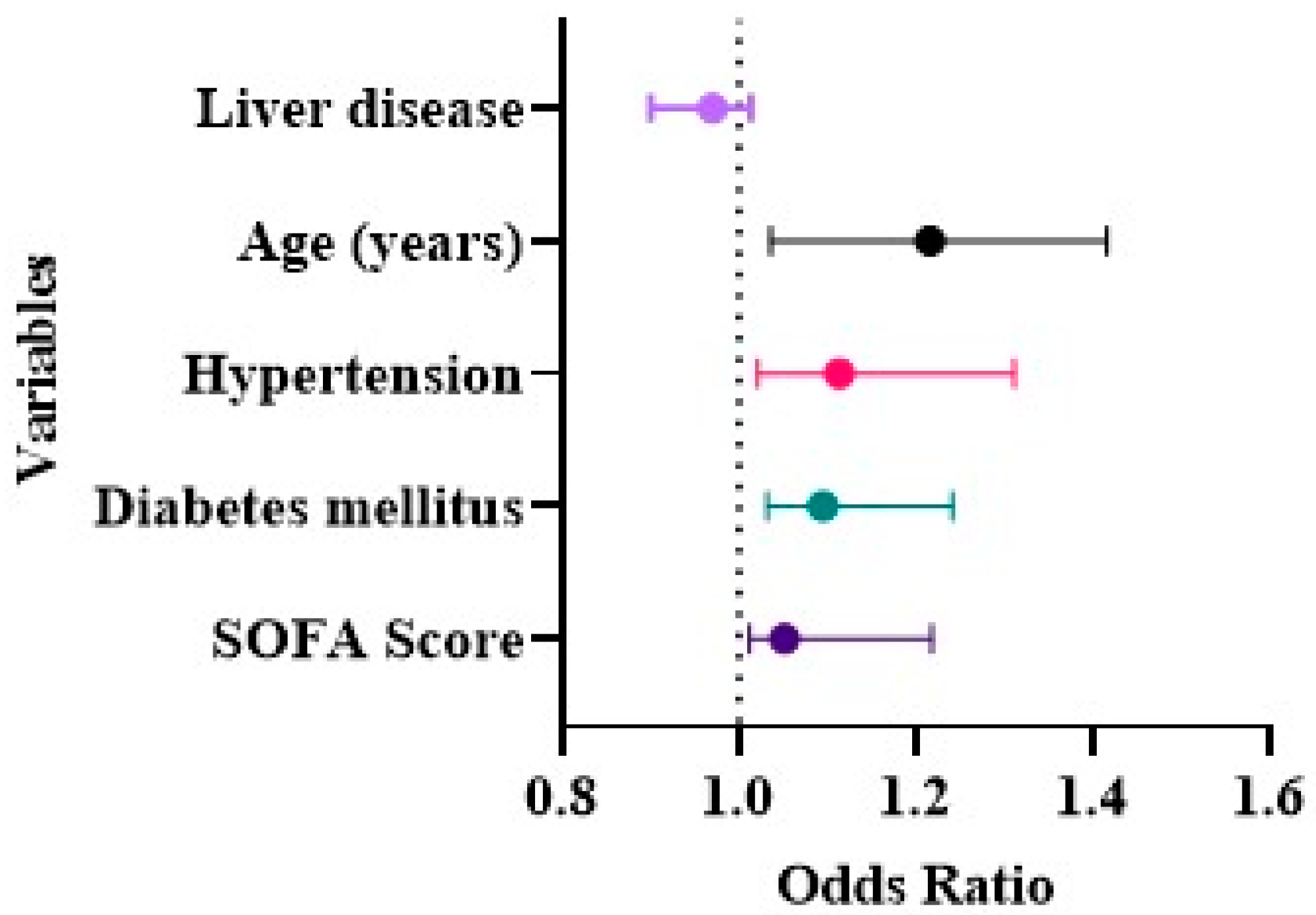
| Variables | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Age (years) | 2.051 | 1.771–2.373 | 0.000 * |
| Cardiovascular diseases | 0.993 | 0.938–1.261 | 0.294 |
| Chronic liver disease | 0.812 | 0.692–1.494 | 0.953 |
| Chronic obstructive pulmonary disease | 0.741 | 0.504–1.112 | 0.151 |
| Diabetes mellitus | 1.094 | 1.032–1.241 | 0.012 * |
| Hypertension | 1.612 | 1.424–1.823 | 0.002 * |
| SOFA Score | 1.051 | 1.012–1.218 | 0.023 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Algahtani, F.D.; Elabbasy, M.T.; Alshammari, F.; Atta, A.; El-Fateh, A.M.; Ghoniem, M.E. Evolving Risk of Acute Kidney Injury in COVID-19 Hospitalized Patients: A Single Center Retrospective Study. Medicina 2022, 58, 443. https://doi.org/10.3390/medicina58030443
Algahtani FD, Elabbasy MT, Alshammari F, Atta A, El-Fateh AM, Ghoniem ME. Evolving Risk of Acute Kidney Injury in COVID-19 Hospitalized Patients: A Single Center Retrospective Study. Medicina. 2022; 58(3):443. https://doi.org/10.3390/medicina58030443
Chicago/Turabian StyleAlgahtani, Fahad D., Mohamed T. Elabbasy, Fares Alshammari, Amira Atta, Ayman M. El-Fateh, and Mohamed E. Ghoniem. 2022. "Evolving Risk of Acute Kidney Injury in COVID-19 Hospitalized Patients: A Single Center Retrospective Study" Medicina 58, no. 3: 443. https://doi.org/10.3390/medicina58030443
APA StyleAlgahtani, F. D., Elabbasy, M. T., Alshammari, F., Atta, A., El-Fateh, A. M., & Ghoniem, M. E. (2022). Evolving Risk of Acute Kidney Injury in COVID-19 Hospitalized Patients: A Single Center Retrospective Study. Medicina, 58(3), 443. https://doi.org/10.3390/medicina58030443