
The Additional Role of the 3-Vessels and Trachea View in Screening for Congenital Heart Disease

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
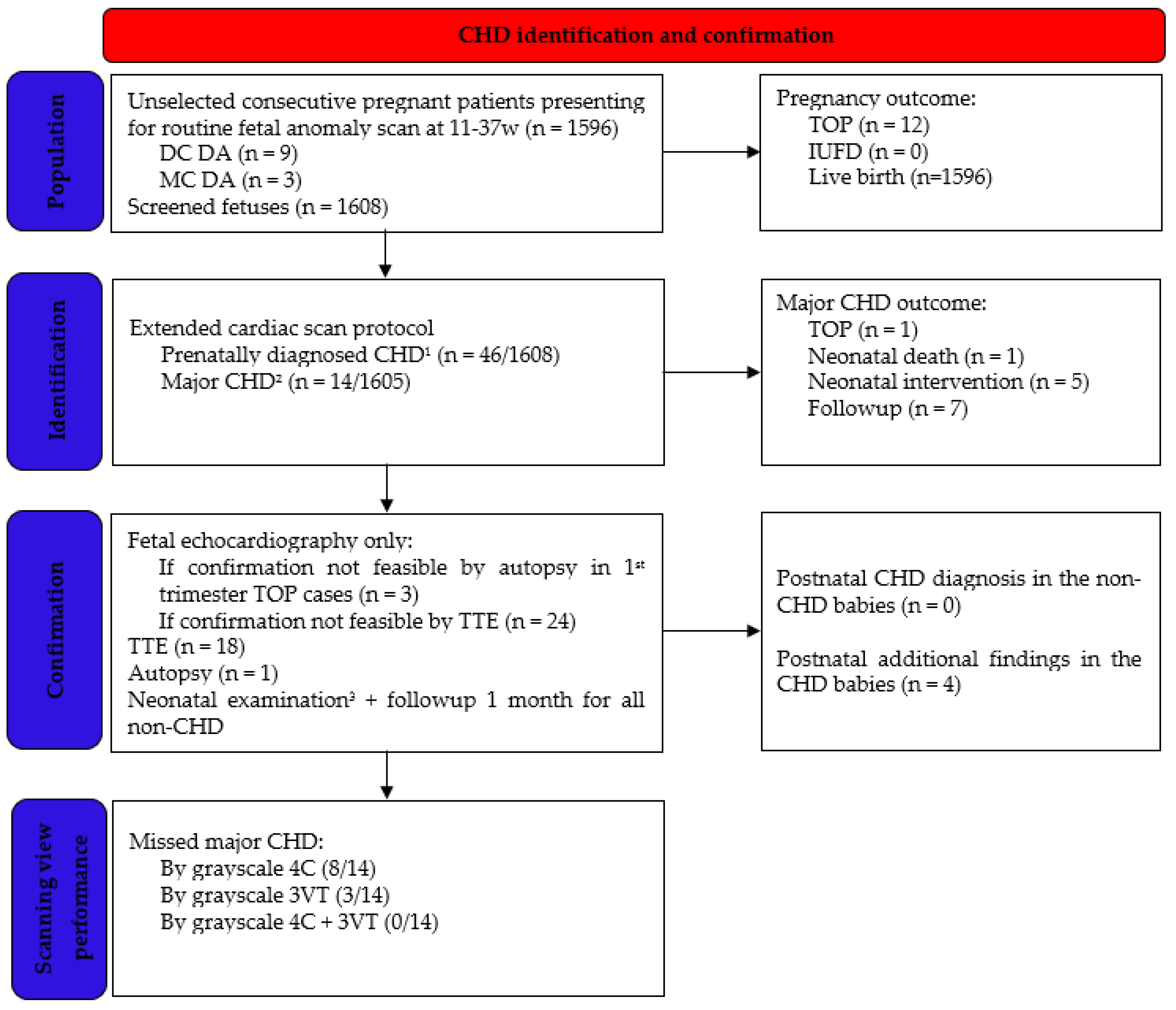
2.1. Study Population
2.2. Ultrasound Examination
2.3. Diagnosis Confirmation and Outcome Measures
2.4. Outcome Measures
2.5. Statistical Analysis
2.6. Ethical Approval
3. Results
4. Discussion
4.1. Comparison to Other Studies
4.2. Detecting Major CHD
4.3. Detecting Minor CHD
4.4. 3VT Advantages
4.5. 3VT Pitfalls
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, Y.; Chen, S.; Zühlke, L.; Black, G.C.; Choy, M.K.; Li, N.; Keavney, B.D. Global birth prevalence of congenital heart defects 1970–2017: Updated systematic review and meta-analysis of 260 studies. Int. J. Epidemiol. 2019, 48, 455–463. [Google Scholar] [CrossRef]
- Sanapo, L.; Pruetz, J.D.; Słodki, M.; Goens, M.B.; Moon-Grady, A.J.; Donofrio, M.T. Fetal echocardiography for planning perinatal and delivery room care of neonates with congenital heart disease. Echocardiography 2017, 34, 1804–1821. [Google Scholar] [CrossRef]
- Huang, H.; Cai, M.; Wang, Y.; Liang, B.; Lin, N.; Xu, L. SNP Array as a tool for prenatal diagnosis of congenital heart disease screened by echocardiography: Implications for precision assessment of fetal prognosis. Risk Manag. Healthc. Policy 2021, 14, 345–355. [Google Scholar] [CrossRef]
- International Society of Ultrasound in Obstetrics and Gynecology; Carvalho, J.S.; Allan, L.D.; Chaoui, R.; Copel, J.A.; DeVore, G.R.; Hecher, K.; Lee, W.; Munoz, H.; Paladini, D.; et al. ISUOG practice guidelines (updated): Sonographic screening examination of the fetal heart. Ultrasound Obstet. Gynecol. 2013, 41, 348–359. [Google Scholar] [CrossRef]
- Pellerito, J.; Bromley, B.; Allison, S.; Chauhan, A.; Destounis, S.; Dickman, E.; Wilkins, I. AIUM-ACR-ACOG-SMFM-SRU practice parameter for the performance of standard diagnostic obstetric ultrasound examina-tions. J. Ultrasound Med. 2018, 37, E13–E24. [Google Scholar] [CrossRef]
- Liu, H.; Zhou, J.; Feng, Q.L.; Gu, H.T.; Wan, G.; Zhang, H.M.; Xie, Y.J.; Li, X.S. Fetal echocardiography for congenital heart disease diagnosis: A meta-analysis, power analysis and missing data analysis. Eur. J. Prev. Cardiol. 2015, 22, 1531–1547. [Google Scholar] [CrossRef]
- Yagel, S.; Arbel, R.; Anteby, E.Y.; Raveh, D.; Achiron, R. The three vessels and trachea view (3VT) in fetal cardiac scanning. Ul-Trasound Obstet. Gynecol. 2002, 20, 340–345. [Google Scholar] [CrossRef]
- Pasternok, M.; Nocun, A.; Knafel, A.; Grzesiak, M.; Orzechowski, M.; Konarska, K.; Ludwin, A.; Ludwin, I.; Zymroz, P.; Parzynska, A.; et al. “Y Sign” at the level of the 3-vessel and trachea view: An effective fetal marker of aortic dextroposition anomalies in the first trimester. J. Ultrasound Med. 2018, 37, 1869–1880. [Google Scholar] [CrossRef] [Green Version]
- Palatnik, A.; Grobman, W.A.; Cohen, L.S.; Dungan, J.S.; Gotteiner, N.L. Role of the 3-vessel and trachea view in antenatal de-tection of tetralogy of fallot. J. Ultrasound Med. 2016, 35, 1799–1809. [Google Scholar] [CrossRef]
- Edwards, H.; Hamilton, R. Single centre audit of early impact of inclusion of the three vessel and trachea view in obstetric screening. Ultrasound 2018, 26, 93–100. [Google Scholar] [CrossRef]
- Lee, W.; Allan, L.; Carvalho, J.S.; Chaoui, R.; Copel, J.; Devore, G.; Hecher, K.; Munoz, H.; Nelson, T.; Paladini, D.; et al. ISUOG consensus statement: What constitutes a fetal echocardiogram? Ultrasound Obstet. Gynecol. 2008, 32, 239–242. [Google Scholar] [CrossRef]
- American Institute of Ultrasound in Medicine. AIUM practice parameter for the performance of fetal echocardiography. J. Ultrasound Med. 2020, 39, E5–E16. [Google Scholar] [CrossRef] [Green Version]
- Societatea de Obstetrică și Ginecologie din România (SOGR), Societarea Română de Ultrasonografie în Obstetrică și Ginecologie (SRUOG). Ghid de Examinare Ecografică de Screening pentru Anomalii de Sarcină in Trimestru 1. 2019. Available online: https://sogr.ro/wp-content/uploads/2019/11/22.1.-Ghid-de-examinare-ecografică-de-screening-pentru-anomalii-de-sarcină-în-trimestrul-1.docx.pdf (accessed on 15 December 2021).
- Societatea de Obstetrică și Ginecologie din România (SOGR), Societarea Română de Ultrasonografie în Obstetrică și Ginecologie (SRUOG). Ghid de Examinare Ecografică de Screening pentru Anomalii de Sarcină in Trimestru 2. 2019. Available online: https://sogr.ro/wp-content/uploads/2019/11/23.1.-Ghid-de-examinare-ecografică-de-screening-pentru-anomalii-de-sarcină-în-trimestrul-2.docx.pdf (accessed on 15 December 2021).
- Societatea de Obstetrică și Ginecologie din România (SOGR), Societarea Română de Ultrasonografie în Obstetrică și Ginecologie (SRUOG). Ghid de Examinare Ecografică de Screening pentru Anomalii de Sarcină in Trimestru 3. 2020. Available online: https://sruog.ro/wp-content/uploads/2021/04/ghidul-privind-examinarea-ecografic-de-screening-pentru-anomalii-de-sarcin-n-trimestrul-3.pdf (accessed on 15 December 2021).
- Bronshtein, M.; Blumenfeld, Z.; Khoury, A.; Gover, A. Diverse outcome following early prenatal diagnosis of pulmonary stenosis. Ultrasound Obstet. Gynecol. 2017, 49, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Guirado, L.; Crispi, F.; Masoller, N.; Bennasar, M.; Marimon, E.; Carretero, J.; Gratacós, E.; Martínez, J.M.; Friedberg, M.K.; Gómez, O. Biventricular impact of mild to moderate fetal pulmonary valve stenosis. Ultrasound Obstet. Gynecol. 2018, 51, 349–356. [Google Scholar] [CrossRef] [Green Version]
- Fricke, K.; Liuba, P.; Weismann, C.G. Fetal echocardiographic dimension indices: Important predictors of postnatal coarctation. Pediatr. Cardiol. 2021, 42, 517–552. [Google Scholar] [CrossRef]
- Familiari, A.; Morlando, M.; Khalil, A.; Sonesson, S.E.; Scala, C.; Rizzo, G.; Del Sordo, G.; Vassallo, C.; Flacco, M.E.; Manzoli, L.; et al. Risk factors for coarctation of the aorta on prenatal ultrasound: A systematic review and meta-analysis. Circulation 2017, 135, 772–785. [Google Scholar] [CrossRef]
- Zheng, M.M.; Tang, H.R.; Zhang, Y.; Ru, T.; Li, J.; Xu, B.Y.; Xu, Y.; Hu, Y.L. Contribution of the fetal cardiac axis and v-sign angle in first-trimester screening for major cardiac defects. J. Ultrasound Med. 2019, 38, 1179–1187. [Google Scholar] [CrossRef]
- Stativa, E.; Rus, A.V.; Suciu, N.; Pennings, J.S.; Butterfield, M.E.; Wenyika, R.; Webster, R. Characteristics and prenatal care utili-sation of Romanian pregnant women. Eur. J. Contracept. Reprod. Health Care 2014, 19, 220–226. [Google Scholar] [CrossRef]
- Pinette, M.G.; Pan, Y.; Pinette, S.G.; Blackstone, J.; Stubblefield, P.G. Fetal atrial septal aneurysm. Prenatal diagnosis by ultraso-nography. J. Reprod. Med. 1997, 42, 459–462. [Google Scholar]
- Sun, H.Y.; Fripp, R.R.; Printz, B.F. Unusual consequence of a fetal atrial septal aneurysm. Clin. Case Rep. 2015, 3, 368–369. [Google Scholar] [CrossRef]
- Gewillig, M.; Brown, S.C.; Roggen, M.; Eyskens, E.; Heying, R.; Givron, P.; Cools, B.; de Catte, L. Dysfunction of the foetal arterial duct results in a wide spectrum of cardiovascular pathology. Acta Cardiol. 2017, 72, 625–635. [Google Scholar] [CrossRef]
- Liang, M.; Wen, H.; Li, S. Two fetuses in one family of arterial tortuosity syndrome: Prenatal ultrasound diagnosis. BMC Pregnancy Childbirth 2021, 21, 548. [Google Scholar] [CrossRef]
- Aly, S.A.; Contreras, J.; Honjo, O.; Villemain, O. Antenatal occlusion of a ductal arteriosus aneurysm: A potential postnatal surgical emergency. Case report and literature review. Cardiol. Young 2020, 30, 1750–1752. [Google Scholar] [CrossRef]
- Takajo, D.; Kobayashi, D. Ductus arteriosus aneurysm with left pulmonary artery obstruction. Echocardiography 2021, 38, 1128–1130. [Google Scholar] [CrossRef]
- Doğan, V.; Aksoy, Ö.N.; Sayıcı, İ.U.; Çitli, R. Thrombosis of isolated ductus arteriosus aneurysm in a newborn. Echocardiography 2021, 38, 716–717. [Google Scholar] [CrossRef]
- Ranzini, A.C.; Hyman, F.; Jamaer, E.; van Mieghem, T. Aberrant right subclavian artery: Correlation between fetal and neonatal abnormalities and abnormal genetic screening or testing. J Ultrasound Med. 2017, 36, 785–790. [Google Scholar] [CrossRef]
- Minsart, A.F.; Boucoiran, I.; Delrue, M.A.; Audibert, F.; Abadir, S.; Lapierre, C.; Lemyre, E.; Raboisson, M.J. Left superior vena cava in the fetus: A rarely isolated anomaly. Pediatr. Cardiol. 2020, 41, 230–236. [Google Scholar] [CrossRef]
- Abuhamad, A.; Chaoui, R. The Three-Vessel-Trachea View and Upper Mediastinum. In A Practical Guide to Fetal Echocardiography: Normal and Abnormal Hearts, 3rd ed.; Elfrank, J., Fischer, A., Eds.; Wolters Kluwer: Philadelphia, PA, USA, 2016; pp. 115–116. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total, n = 46 | Value |
|---|---|
| Maternal age | 30 ± 4.85 y |
| Gravida | 1 (1–4) |
| Nulliparity | 67.3% |
| Male fetuses | 60.4% |
| Syndromic/genetic | 6.5% (3/46) |
| TOP | 8.7% (4/46) |
| Livebirth | 91.3% (42/46) |
| Neonatal death 1 | 2.1% (1/46) |
| Gestational age at birth | 39 ± 1.2 w |
| Birthweight | 3320 ± 497 g (2250–4300) |
| C-section (%) | 71.7% |
| Anomaly | Total | Associated, Prenatally 1 | Associated, Postnatally 1 | Main Suspicious View | Abnormal 3VT 2D | 1st | 2nd | 3rd | Detected at First Presentation |
|---|---|---|---|---|---|---|---|---|---|
| ASD type II | 2 | Late FGR | 1 hypospadias | 4C | - | 0 | 1 | 1 | 2/2 |
| ASA | 9 | 1 hypoplastic aortic arch in 3rd T | 1 aortic valve malformation + double ASD type II | 4C | −/+ | 0 | 4 | 5 | 7/9 |
| VSD, muscular | 2 | - | - | 4C color | - | 0 | 0 | 2 | 0/2 |
| VSD, perimembranous | 2 | 2 × T18 (hygroma + multiple defects) | - | other | - | 2 | 0 | 0 | 2/2 |
| AVSD, complete | 1 | hygroma + multiple defects (no genetics) | - | 4C | - | 1 | 0 | 0 | 1/1 |
| Hypertrophic cardiomyopathy | 1 | gestational diabetes | - | 4C | - | 0 | 0 | 1 | 1/1 |
| Left cardiac axis deviation 2 | 1 | echogenic CSP | mild supravalvular PS + facial dysmorphism | 4C | + | 0 | 1 | 0 | 1/1 |
| Severe aortic stenosis | 1 | - | - | 4C | + | 0 | 1 | 0 | 0/1 |
| Aortic coarctation | 3 | 1 × (hypoplastic NB and late FGR) | - | 3VT | + | 0 | 2 | 1 | 2/3 |
| IAoA | 1 | perimembranous VSD | - | 3VT | + | 0 | 1 | 0 | 1/1 |
| HLHS | 1 | mitral atresia + aortic atresia | - | 4C | + | 0 | 1 | 0 | 1/1 |
| Valvular PS, mild | 1 | - | - | 3VT | + | 0 | 1 | 0 | 1/1 |
| PA/IVS | 1 | - | - | 4C | + | 0 | 0 | 1 | 1/1 |
| Fallot | 1 | - | - | 3VT | + | 0 | 1 | 0 | 1/1 |
| RAA | 1 | - | perimembranous VSD | 3VT | + | 1 | 0 | 0 | 1/1 |
| D-transposition 3 | 1 | - | - | 3VT | + | 0 | 0 | 1 | 1/1 |
| Isolated ARSA | 6 | - | - | 3VT color | - | 0 | 6 | 0 | 2/5 |
| PLSVC | 4 | - | - | 3VT color | + | 0 | 4 | 0 | 4/4 |
| Intrathymic LBCV | 3 | - | - | 3VT color | - | 0 | 3 | 0 | 3/3 |
| DAA | 1 | Tortuous DA at 20 w + late FGR | - | 3VT | + | 0 | 0 | 1 | 1/1 |
| Cardiac tumors, rhabdomyoma | 1 | - | - | 4C | - | 0 | 1 | 0 | 1/1 |
| DV agenesis | 2 | 1 × (ARSA + bilateral pielectasis) | - | other | - | 2 | 0 | 0 | 2/2 |
| View | Detected CHD, All n = 46 | Missed CHD, Major 1 n = 14 |
|---|---|---|
| Grayscale 4C only | 47.8% (22/46) | 57.1% (8/14) |
| Grayscale 3VT only | 36.9% (17/46) | 21.4% (3/14) |
| Color 3VT only | 58.6% (27/46) | 14.2% (2/14) |
| Grayscale 4C + 3VT | 71.7% (33/46) | 0% (0/14) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gireadă, R.; Socolov, D.; Mihălceanu, E.; Matasariu, R.; Ursache, A.; Akad, M.; Bujor, I.; Scripcariu, I.; Popa, R.F.; Socolov, R. The Additional Role of the 3-Vessels and Trachea View in Screening for Congenital Heart Disease. Medicina 2022, 58, 262. https://doi.org/10.3390/medicina58020262
Gireadă R, Socolov D, Mihălceanu E, Matasariu R, Ursache A, Akad M, Bujor I, Scripcariu I, Popa RF, Socolov R. The Additional Role of the 3-Vessels and Trachea View in Screening for Congenital Heart Disease. Medicina. 2022; 58(2):262. https://doi.org/10.3390/medicina58020262
Chicago/Turabian StyleGireadă, Roxana, Demetra Socolov, Elena Mihălceanu, Roxana Matasariu, Alexandra Ursache, Mona Akad, Iuliana Bujor, Ioana Scripcariu, Radu Florin Popa, and Răzvan Socolov. 2022. "The Additional Role of the 3-Vessels and Trachea View in Screening for Congenital Heart Disease" Medicina 58, no. 2: 262. https://doi.org/10.3390/medicina58020262
APA StyleGireadă, R., Socolov, D., Mihălceanu, E., Matasariu, R., Ursache, A., Akad, M., Bujor, I., Scripcariu, I., Popa, R. F., & Socolov, R. (2022). The Additional Role of the 3-Vessels and Trachea View in Screening for Congenital Heart Disease. Medicina, 58(2), 262. https://doi.org/10.3390/medicina58020262