
The Accuracy of Serum Biomarkers in the Diagnosis of Steatosis, Fibrosis, and Inflammation in Patients with Nonalcoholic Fatty Liver Disease in Comparison to a Liver Biopsy

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
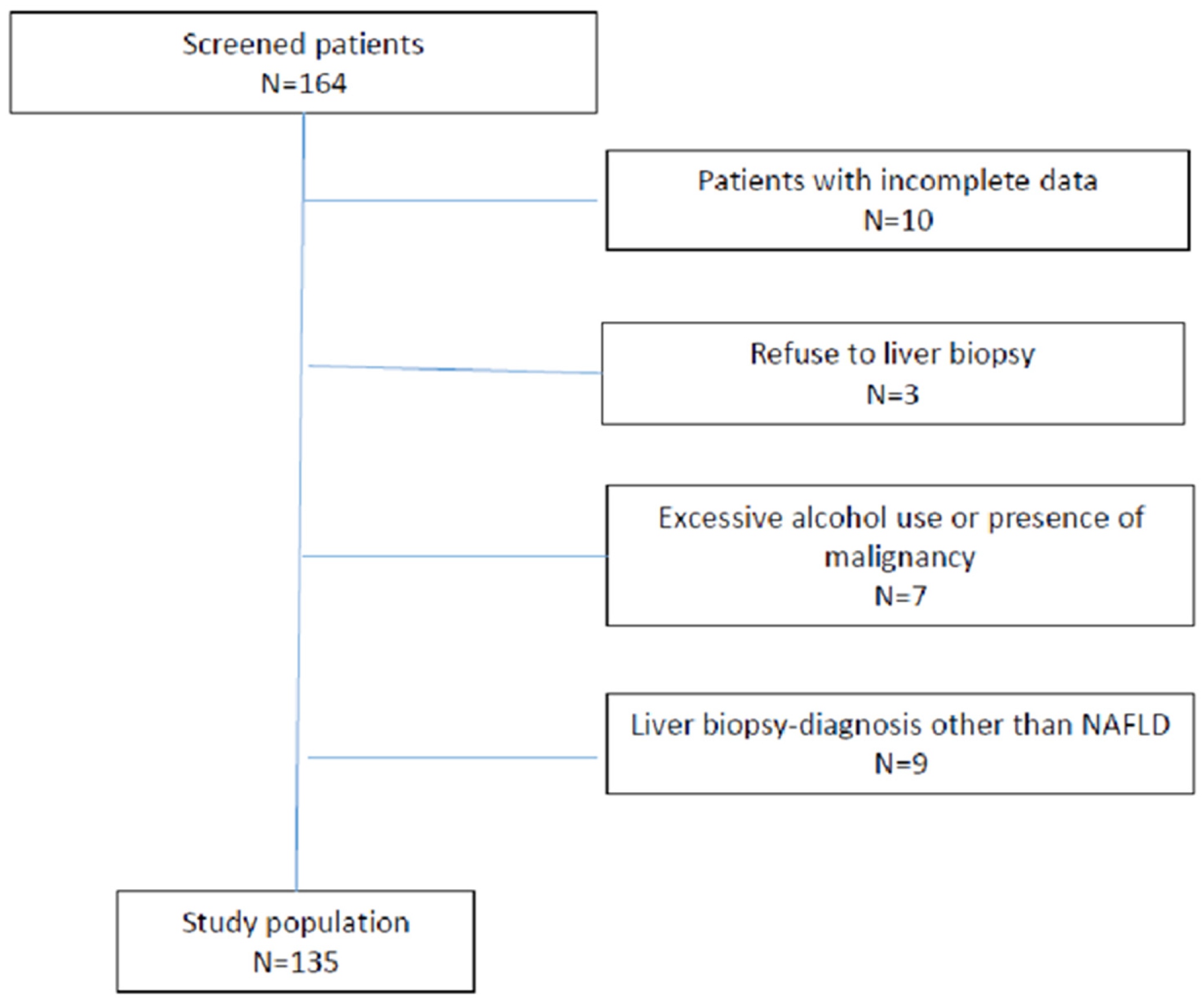
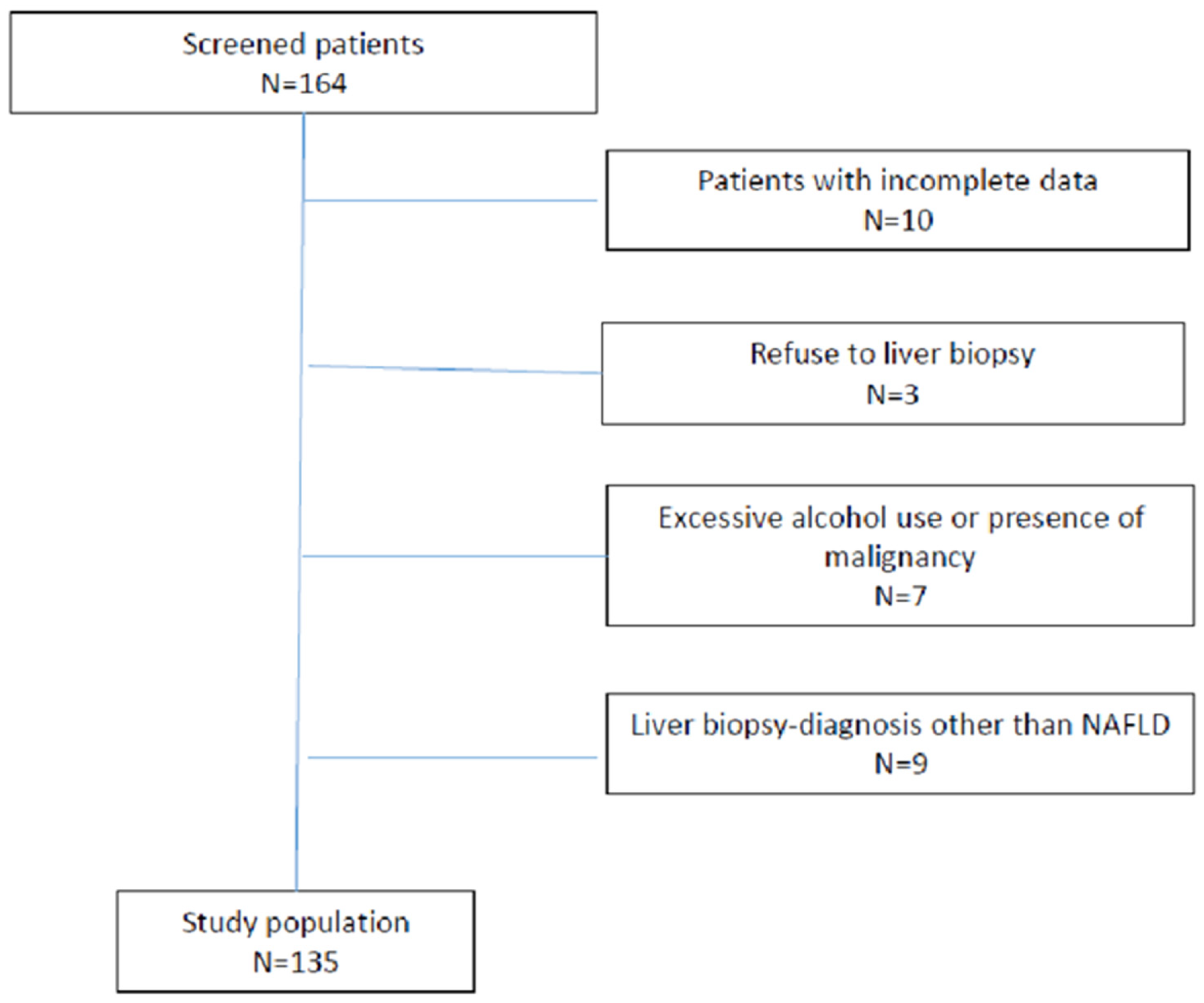
2.1. Exclusion Criteria
2.2. Patient Characteristics
- FIB-4 = (age (years) × aspartate aminotransferase (AST(IU/L))/(platelet count(109/L) × ((alanin aminotransferase (ALT) (IU/L))1/2) [10]
- APRI = ((AST/ULN)/platelet count (109/L)) × 100 [11]
- NAFLD fibrosis score: −1.675 + 0.037 × age (years) + 0.094 × BMI (kg/m2) + 1.13 × impaired fasting glycaemia or diabetes (yes = 1, no = 0) + 0.99 × AST/ALT ratio −0.013 × platelet (× 109/litre) − 0.66 × albumin (g/dl) [12]
- BARD score was calculated as the weighted sum of the three variables (BMI > 28 = 1 point, AST/ALT ratio > 0.8 = 2 points, and diabetes = 1 point) [13]
- FLI = (e 0.953 ∗ loge (triglycerides) + 0.139 ∗ BMI + 0.718 ∗ loge (ggt) + 0.053 ∗ waist circumference − 15.745)/(1 + e 0.953 ∗ loge (triglycerides) + 0.139 ∗ BMI + 0.718 ∗ loge (ggt) + 0.053 ∗ circumference − 15.745) ∗ 100 [14]
- HSI = 8 × (ALT/AST ratio) + BMI (+ 2 if female; + 2 if diabetes mellitus) [15]
2.3. Liver Biopsy and Histological Analysis
2.4. M30 and M60 Analysis
2.5. M30-Enzyme-Linked Immunosorbent Assay (ELISA)
2.6. M65-Enzyme-Linked Immunosorbent Assay (ELISA)
2.7. Statistical Analysis
3. Results
3.1. Detection of Steatosis
3.2. Detection of Nonalcoholic Steatohepatitis
3.3. Detection of Liver Fibrosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mikolasevic, I.; Milic, S.; Wensveen, T.T.; Grgic, I.; Jakopcic, I.; Stimac, D.; Wensveen, F.; Orlic, L. Nonalcoholic fatty liver disease—A multisystem disease? World J. Gastroenterol. 2016, 22, 9488–9505. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Chan, H.L.; Wong, G.L.; Choi, P.C.; Chan, A.W.; Chan, H.Y.; Chim, A.M.; Yeung, D.K.; Chan, F.K.; Woo, J.; et al. Non-invasive diagnosis of nonalcoholic steatohepatitis by combined serum biomarkers. J. Hepatol. 2012, 56, 1363–1370. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive assessment of liver disease in patients with nonalcoholic fatty liver disease. Gastroenterology 2019, 156, 1264–1281.e4. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.-H.; Cai, J.-J.; She, Z.-G.; Li, H.-L. Noninvasive evaluation of nonalcoholic fatty liver disease: Current evidence and practice. World J. Gastroenterol. 2019, 25, 1307–1326. [Google Scholar] [CrossRef]
- Mikolasevic, I.; Filipec-Kanizaj, T.; Mijic, M.; Jakopcic, I.; Milic, S.; Hrstic, I.; Sobocan, N.; Stimac, D.; Burra, P. Nonalcoholic fatty liver disease and liver transplantation—Where do we stand? World J. Gastroenterol. 2018, 24, 1491–1506. [Google Scholar] [CrossRef]
- Kwok, R.; Tse, Y.K.; Wong, G.H.; Ha, Y.; Lee, A.U.; Ngu, M.C.; Chan, H.Y.; Wong, V.S. Systematic review with meta-analysis: Non-invasive assessment of non-alcoholic fatty liver disease—The role of transient elastography and plasma cytokeratin-18 fragments. Aliment. Pharmacol. Ther. 2014, 39, 254–269. [Google Scholar] [CrossRef]
- Alkhouri, N.; McCullough, A.J. Noninvasive Diagnosis of NASH and liver fibrosis within the spectrum of NAFLD. Gastroenterol. Hepatol. 2012, 8, 661–668. [Google Scholar]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. Comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar]
- Wai, C.T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S.F. A simple noninvasive index can predict both significant fibrosis cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [Green Version]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with, N.A.F.L.D. Hepatology 2007, 45, 847–854. [Google Scholar] [CrossRef]
- Harrison, S.A.; Oliver, D.; Arnold, H.L.; Gogia, S.; Neuschwander-Tetri, B.A. Development and validation of a simple NAFLD clinical scoring system for identifying patients without advanced disease. Gut 2008, 57, 1441–1447. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H.; Kim, D.; Kim, H.J.; Lee, C.-H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.-H.; Cho, S.-H.; Sung, M.-W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Björnsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver fibrosis, but no other histologic features, is associated with long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology 2015, 149, 389–397.e10. [Google Scholar] [CrossRef] [Green Version]
- Darweesh, S.K.; AbdElAziz, R.A.; Abd-ElFatah, D.S.; AbdElazim, N.A.; Fathi, S.A.; Attia, D.; AbdAllah, M. Serum cytokeratin-18 and its relation to liver fibrosis and steatosis diagnosed by FibroScan and controlled attenuation parameter in nonalcoholic fatty liver disease and hepatitis C virus patients. Eur J. Gastroenterol. Hepatol. 2019, 31, 633–641. [Google Scholar] [CrossRef]
- Grgurevic, I.; Podrug, K.; Mikolasevic, I.; Kukla, M.; Madir, A.; Tsochatzis, E.A. Natural history of nonalcoholic fatty liver disease: Implications for clinical practice and an individualized approach. Can. J. Gastroenterol. Hepatol. 2020, 2020, 9181368. [Google Scholar] [CrossRef]
- Joka, D.; Wahl, K.; Moeller, S.; Schlue, J.; Vaske, B.; Bahr, M.J.; Manns, M.P.; Schulze-Osthoff, K.; Bantel, H. Prospective biopsy-controlled evaluation of cell death biomarkers for prediction of liver fibrosis and nonalcoholic steatohepatitis. Hepatology 2012, 55, 455–464. [Google Scholar] [CrossRef]
- Fedchuk, L.; Nascimbeni, F.; Pais, R.; Charlotte, F.; Housset, C.; Ratziu, V.; LIDO Study Group. Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2014, 40, 1209–1222. [Google Scholar] [CrossRef]
- McPherson, S.; Stewart, S.F.; Henderson, E.; Burt, A.D.; Day, C.P. Simple non-invasive fibrosis scoring systems can reliably exclude advanced fibrosis in patients with non-alcoholic fatty liver disease. Gut 2010, 59, 1265–1269. [Google Scholar] [CrossRef] [Green Version]
- Wong, V.W.S.; Wong, G.L.H.; Yip, G.W.K.; Lo, A.O.S.; Limquiaco, J.; Chu, W.C.W.; Chim, A.M.L.; Yu, C.M.; Yu, J.; Chan, F.K.L.; et al. Coronary artery disease and cardiovascular outcomes in patients with non-alcoholic fatty liver disease. Gut 2011, 60, 1721–1727. [Google Scholar] [CrossRef]
- Targher, G.; Day, C.P.; Bonora, E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N. Engl. J. Med. 2010, 363, 1341–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.K.; Seo, M.H.; Shin, H.C.; Ryoo, J.-H. Clinical availability of nonalcoholic fatty liver disease as an early predictor of type 2 diabetes mellitus in korean men: 5-year prospective cohort study. Hepatology 2013, 57, 1378–1383. [Google Scholar] [CrossRef]
- Adams, L.A.; Waters, O.R.; Knuiman, M.W.; Elliott, R.R.; Olynyk, J.K. NAFLD as a risk factor for the development of diabetes and the metabolic syndrome: An eleven-year follow-up study. Am. J. Gastroenterol. 2009, 104, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Mikolasevic, I.; Racki, S.; Bubic, I.; Jelic, I.; Stimac, D.; Orlic, L. Chronic kidney disease and nonalcoholic Fatty liver disease proven by transient elastography. Kidney Blood Press Res. 2013, 37, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, A.E.; Wieckowska, A.; Lopez, A.R.; Liu, Y.C.; Zein, N.N.; McCullough, A.J. Cytokeratin-18 fragment levels as noninvasive biomarkers for nonalcoholic steatohepatitis: A multicenter validation study. Hepatology 2009, 50, 1072–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Variable (n = 135) | Value |
|---|---|
| Age, years (IQR) | 59.3 (52–68) |
| Female gender, n (%) | 65 (48.14) |
| BMI, kg/m2 (IQR) | 32.3 (29.3–37) |
| Diabetes mellitus, n (%) | 61 (45.1) |
| Arterial hypertension, n (%) | 101 (74.8) |
| Hyperlipidaemia, n (%) | 98 (72.6) |
| Platelet count, 109/L (IQR) | 222 (182–251) |
| AST, IU/L (IQR) | 27.5 (22–38.5) |
| ALT, IU/L (IQR) | 44 (28–57) |
| GGT, IU/L (IQR) | 49 (26.5–82) |
| Alkaline phosphatase, IU/L (IQR) | 72.5 (58–86) |
| Albumin, g/L (IQR) | 44.4 (42–46.5) |
| Fasting glucose, mmol/L (IQR) | 6.4 (5.6–7.8) |
| HOMA-IR score (IQR) | 5.9 (3.8–8.6) |
| Waist circumference, cm (IQR) Male Female | 111 (100–120) 112 (106–121) 104 (99–112) |
| Total cholesterol, mmol/L (IQR) | 5.0 (4.2–6.0) |
| LDL cholesterol, mmol/L (IQR) | 2.8 (2.1–3.7) |
| HDL cholesterol, mmol/L (IQR) Male Female | 1.2 (1.1–1.4) 1.1 (1.0–1.4) 1.2 (1.1–1.4) |
| Triglycerides, mmol/L (IQR) | 1.8 (1.3–2.5) |
| FLI (IQR) | 92 (80.2–97) |
| HSI (IQR) | 46 (41.8–49.8) |
| APRI (IQR) | 0.48 (0.33–0.80) |
| FIB-4 (IQR) | 1.24 (0.92–1.90) |
| NFS (IQR) | −0.88 (−2.1–0.03) |
| BARD (IQR) | 2 (1–3) |
| M30 (IQR) | 199 (74–258) |
| M65 (IQR) | 259 (199–330) |
| Fibrosis stage, n (%) F0 F1 F2 F3 F4 | 29 (21.5) 49 (36.3) 32 (23.7) 17 (12.6) 8 (5.9) |
| Steatosis grade, n (%) S0 S1 S2 S3 | 5 (3.7) 57 (42.2) 40 (29.6) 33 (24.5) |
| NAS score, n (%) <5 ≥5 | 69 (51.1) 66 (49.9) |
| FLI | HSI | |||
|---|---|---|---|---|
| S ≥ S2 | S = S3 | S ≥ S2 | S = 3 | |
| cut-off | 69 | 90 | 42.25 | 45.20 |
| Se: | 25.53% (13.9%–40.3%) | 64.0% (42.5%–82.0%) | 87.01% (77.4%–93.6%) | 78.12% (60.0%–90.7%) |
| Sp: | 85.71% (71.5%–94.6%) | 59.38% (46.4%–71.5%) | 47.54% (34.6%–60.7%) | 51.89% (42.0%–61.7%) |
| PPV: | 66.7% (41.0%–86.7%) | 38.1% (23.6%–54.4%) | 67.7% (57.5%–76.7%) | 32.9% (22.5%–44.6%) |
| NPV: | 50.7% (38.6%–62.8%) | 80.9% (66.7%–90.9%) | 74.4% (57.9%–87.0%) | 88.7% (78.1%–95.3%) |
| LR+ | 1.79 (0.7–4.3) | 1.58 (1.0–2.4) | 1.66 (1.3–2.1) | 1.62 (1.2–2.1) |
| LR− | 0.87 (0.7–1.1) | 0.61 (0.3–1.1) | 0.27 (0.1–0.5) | 0.42 (0.2–0.8) |
| AUC | 0.526 | 0.598 | 0.683 | 0.636 |
| SE | 0.062 | 0.068 | 0.046 | 0.054 |
| 0.95 CI | 0.418–0.633 | 0.488–0.700 | 0.598–0.759 | 0.550–0.716 |
| M30 | M65 | M30 and M65 | |
|---|---|---|---|
| NAS score ≥ 5 | NAS score ≥ 5 | NAS score ≥ 5 | |
| Cut-off | 74 | 274 | M30 = 74/M65 = 274 |
| Se: | 49.23% (36.6%–61.9%) | 38.46% (26.7%–51.4%) | 49.23% (36.6%–61.9%) |
| Sp: | 85.71% (75.3%–92.9%) | 94.20% (85.8%–98.4%) | 85.51% (75.0%–92.8%) |
| PPV: | 76.2% (60.5%–87.9%) | 86.2% (68.3%–96.1%) | 76.2% (60.5%–87.9%) |
| NPV: | 64.5% (53.9%–74.2%) | 61.9% (51.9%–71.2%) | 64.1% (53.5%–73.9%) |
| LR+ | 3.45 (1.8–6.4) | 6.63 (2.4–18.0) | 3.40 (1.8–6.3) |
| LR− | 0.59 (0.5–0.8) | 0.65 (0.5–0.8) | 0.59 (0.5–0.8) |
| AUC | 0.683 | 0.662 | 0.691 |
| SE | 0.0378 | 0.037 | 0.039 |
| 0.95 CI | 0.598–0.761 | 0.575–0.741 | 0.605–0.768 |
| F ≥ F1 | F ≥ F2 | F ≥ F3 | |
|---|---|---|---|
| cut-off | 74 | 91 | 109 |
| Se: | 32.40% (23.6%–42.2%) | 46.43% (33.0%–60.3%) | 66.67% (44.7%–84.4%) |
| Sp: | 73.33% (54.1%–87.7%) | 81.01% (70.6%–89.0%) | 81.08% (72.5%–87.9%) |
| PPV: | 85.1% (65.9%–91.4%) | 63.4% (46.9%–77.9%) | 43.2% (27.1%–60.5%) |
| NPV: | 23.7% (15.5%–33.6%) | 68.1% (57.7%–77.3%) | 91% (84.5%–96.4%) |
| LR+ | 1.21 (0.6–2.3) | 2.45 (1.4–4.2) | 3.52 (2.2–5.7) |
| LR− | 0.92 (0.7–1.2) | 0.66 (0.5–0.9) | 0.41 (0.2–0.7) |
| AUC | 0.542 | 0.649 | 0.745 |
| SE | 0.045 | 0.042 | 0.057 |
| 0.95 CI | 0.455–0.628 | 0.562–0.729 | 0.663–0.816 |
| F ≥ F1 | F ≥ F2 | F ≥ F3 | |
|---|---|---|---|
| cutoff | 199 | 230 | 319 |
| Se: | 29.52% (21%–39.2%) | 37.5% (24.9%–51.5%) | 58.33% (36.6%–77.9%) |
| Sp: | 79.3% (60.3%–90.2%) | 84.62% (74.7%–91.8%) | 90.0% (82.8%–94.9%) |
| PPV: | 83.8% (60%–93.8%) | 63.6% (45.1%–79.6%) | 56.0% (34.9%–75.6%) |
| NPV: | 23.7% (15.7%–33.4%) | 65.3% (55.2%–74.5%) | 90.8% (83.8%–95.5%) |
| LR+ | 1.43 (0.7–3.1) | 2.44 (1.3–4.5) | 5.83 (3.0–11.2) |
| LR− | 0.89 (0.7–1.1) | 0.74 (0.6–0.9) | 0.46 (0.3–0.7) |
| AUC | 0.551 | 0.64 | 0.732 |
| SE | 0.043 | 0.04 | 0.057 |
| 0.95 CI | 0.462–0.637 | 0.553–0.721 | 0.649–0.805 |
| F ≥ F1 | F ≥ F2 | F ≥ F3 | |
|---|---|---|---|
| cut-off | M30 F1 = 74 M65 F1 = 199 | M30 F2 = 91 M65 F2 = 230 | M30 F3 = 109 M65 F3 = 319 |
| Se: | 13.33% (7.5%–21.4%) | 46.43% (33.0%–60.3%) | 66.67% (44.7%–84.4%) |
| Sp: | 96.55% (82.2%–99.9%) | 83.33% (73.2%–90.8%) | 79.09% (70.3%–86.3%) |
| PPV: | 93.3% (68.1%–99.8%) | 66.7% (49.8%–80.9%) | 41.0% (25.6%–57.9%) |
| NPV: | 23.5% (16.2%–32.2%) | 68.4% (58.1%–77.6%) | 91.6% (84.1%–96.3%) |
| LR+ | 3.87 (0.5–28.2) | 2.79 (1.6–4.9) | 3.19 (2.0–5.1) |
| LR− | 0.90 (0.8–1.0) | 0.64 (0.5–0.8) | 0.42 (0.2–0.7) |
| AUC | 0.558 | 0.629 | 0.739 |
| SE | 0.051 | 0.046 | 0.06 |
| 0.95 CI | 0.470–0.643 | 0.541–0.711 | 0.656–0.811 |
| F ≥ F1 | F ≥ F2 | F ≥ F3 | |
|---|---|---|---|
| cut-off | 0.4144 | 0.4639 | 0.5214 |
| Se: | 60.61% (51.7%–69%) | 70.89% (59.6%–80.6%) | 79.49% (63.5%–90.7%) |
| Sp: | 42.42% (25.5%–60.8%) | 61.63% (50.5%–71.9%) | 65.87% (56.9%–74.1%) |
| PPV: | 80.8% (71.7%–88%) | 62.9% (52.0%–72.9%) | 41.9% (30.5%–53.9%) |
| NPV: | 21.2% (12.1%–33.0%) | 69.7% (58.1%–79.8%) | 91.2% (83.4%-96.1%) |
| LR+ | 1.05 (0.8–1.5) | 1.85 (1.4–2.5) | 2.33 (1.7–3.1) |
| LR− | 0.93 (0.6–1.5) | 0.47 (0.4–0.7) | 0.31 (0.2–0.6) |
| AUC | 0.569 | 0.703 | 0.739 |
| SE | 0.051 | 0.042 | 0.047 |
| 0.95 CI | 0.490–0.646 | 0.627–0.772 | 0.665–0.804 |
| F ≥ F1 | F ≥ F2 | F ≥ F3 | |
|---|---|---|---|
| cut-off | 1.3895 | 1.5455 | 1.8137 |
| Se: | 47.33% (38.5%–56.2%) | 50.63% (39.1%–62.1%) | 58.97% (42.1%–74.4%) |
| Sp: | 81.82% (64.5%–93.0%) | 81.18% (71.2%–88.8%) | 84% (76.4%–89.9%) |
| PPV: | 91.2% (81.8%–96.7%) | 71.4% (57.8%–82.7%) | 53.5% (37.7%–68.8%) |
| NPV: | 28.1% (19.4%–38.2%) | 63.9% (54.1%–72.9%) | 86.8% (79.4%–92.2%) |
| LR+ | 2.60 (1.2–5.5) | 2.69 (1.6–4.4) | 3.69 (2.3–6.0) |
| LR– | 0.64 (0.5–0.8) | 0.61 (0.5–0.8) | 0.49 (0.3–0.7) |
| AUC | 0.634 | 0.638 | 0.68 |
| SE | 0.055 | 0.044 | 0.054 |
| 0.95 CI | 0.556–0.708 | 0.559–0.711 | 0.602–0.705 |
| F ≥ F1 | F ≥ F2 | F ≥ F3 | |
|---|---|---|---|
| cut-off | −1.8394 | −1.6172 | −0.0405 |
| Se: | 78.31% (67.9%–86.6%) | 83.72% (69.3%–93.2%) | 52.38% (29.8%–74.3%) |
| Sp: | 52.17% (30.6%–73.2%) | 46.03% (33.4%–59.1%) | 80.0% (69.9%–87.9%) |
| PPV: | 85.5% (75.6%–92.5%) | 51.4% (39.2%–63.6%) | 39.3% (21.5%–59.4%) |
| NPV: | 40.0% (22.7%–59.4%) | 80.6% (64.0%–91.8%) | 87.2% (77.7%–93.7%) |
| LR+ | 1.64 (1.1–2.5) | 1.55 (1.2–2.0) | 2.62 (1.5–4.7) |
| LR− | 0.42 (0.2–0.7) | 0.35 (0.2–0.7) | 0.60 (0.4–0.9) |
| AUC | 0.622 | 0.658 | 0.658 |
| SE | 0.069 | 0.055 | 0.075 |
| 0.95 CI | 0.522–0.714 | 0.559–0.747 | 0.559–0.747 |
| F ≥ F1 | F ≥ F2 | F ≥ F3 | |
|---|---|---|---|
| cut-off | 1 | 2 | 3 |
| Se: | 71.56% (62.1%–79.8%) | 38.33% (26.1%–51.8%) | 39.29% (21.5%–59.4%) |
| Sp: | 51.72% (32.5%–70.6%) | 62.82% (51.1%–73.5%) | 82.73% (74.3%–89.3%) |
| PPV: | 84.8% (75.8%–91.4%) | 42.2% (30.5%–58.7%) | 36.7% (19.9%–56.1%) |
| NPV: | 32.6% (19.5%–48.0%) | 57.0% (45.8%–67.6%) | 84.3% (76.0%–90.6%) |
| LR+ | 1.48 (1.0–2.2) | 1.03 (0.7–1.6) | 2.27 (1.2–4.2) |
| LR− | 0.55 (0.3–0.9) | 0.98 (0.8–1.3) | 0.73 (0.5–1.0) |
| AUC | 0.666 | 0.591 | 0.636 |
| SE | 0.057 | 0.047 | 0.056 |
| 0.95 CI | 0.580–0.744 | 0.504–0.674 | 0.549–0.716 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mikolasevic, I.; Domislovic, V.; Krznaric-Zrnic, I.; Krznaric, Z.; Virovic-Jukic, L.; Stojsavljevic, S.; Grgurevic, I.; Milic, S.; Vukoja, I.; Puz, P.; et al. The Accuracy of Serum Biomarkers in the Diagnosis of Steatosis, Fibrosis, and Inflammation in Patients with Nonalcoholic Fatty Liver Disease in Comparison to a Liver Biopsy. Medicina 2022, 58, 252. https://doi.org/10.3390/medicina58020252
Mikolasevic I, Domislovic V, Krznaric-Zrnic I, Krznaric Z, Virovic-Jukic L, Stojsavljevic S, Grgurevic I, Milic S, Vukoja I, Puz P, et al. The Accuracy of Serum Biomarkers in the Diagnosis of Steatosis, Fibrosis, and Inflammation in Patients with Nonalcoholic Fatty Liver Disease in Comparison to a Liver Biopsy. Medicina. 2022; 58(2):252. https://doi.org/10.3390/medicina58020252
Chicago/Turabian StyleMikolasevic, Ivana, Viktor Domislovic, Irena Krznaric-Zrnic, Zeljko Krznaric, Lucija Virovic-Jukic, Sanja Stojsavljevic, Ivica Grgurevic, Sandra Milic, Ivan Vukoja, Petra Puz, and et al. 2022. "The Accuracy of Serum Biomarkers in the Diagnosis of Steatosis, Fibrosis, and Inflammation in Patients with Nonalcoholic Fatty Liver Disease in Comparison to a Liver Biopsy" Medicina 58, no. 2: 252. https://doi.org/10.3390/medicina58020252
APA StyleMikolasevic, I., Domislovic, V., Krznaric-Zrnic, I., Krznaric, Z., Virovic-Jukic, L., Stojsavljevic, S., Grgurevic, I., Milic, S., Vukoja, I., Puz, P., Aralica, M., & Hauser, G. (2022). The Accuracy of Serum Biomarkers in the Diagnosis of Steatosis, Fibrosis, and Inflammation in Patients with Nonalcoholic Fatty Liver Disease in Comparison to a Liver Biopsy. Medicina, 58(2), 252. https://doi.org/10.3390/medicina58020252