
Impact of the Severity of Acquired von Willebrand Syndrome on the Short-Term Prognosis in Patients with Temporary Mechanical Circulatory Support



Abstract
:1. Introduction
2. Methods
2.1. Patient Selection
2.2. Device Selection
2.3. Clinical Management
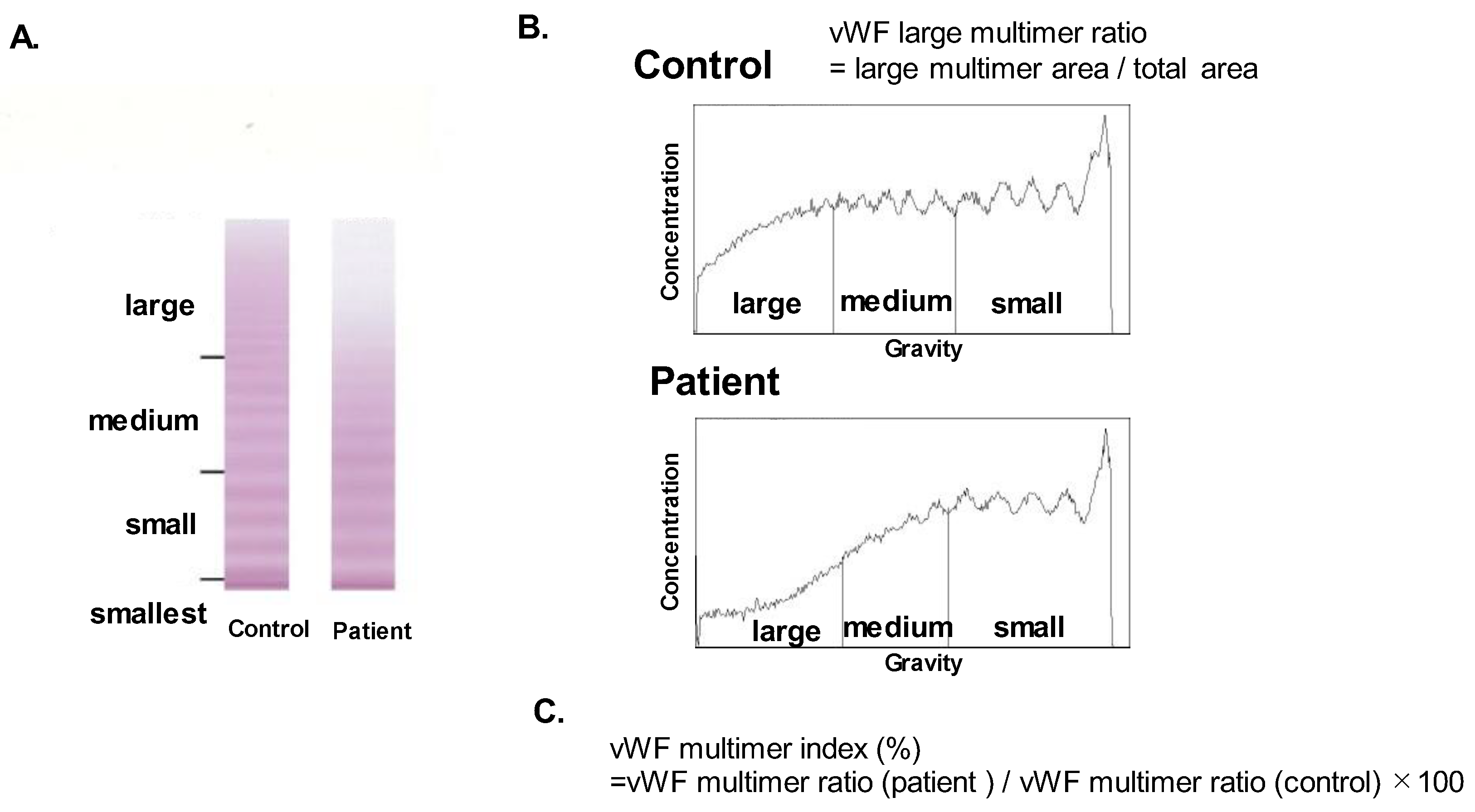
2.4. Measurement of vWF Multimer Index
2.5. Data Collection
2.6. Statistical Assessments
3. Results
3.1. Baseline Characteristics
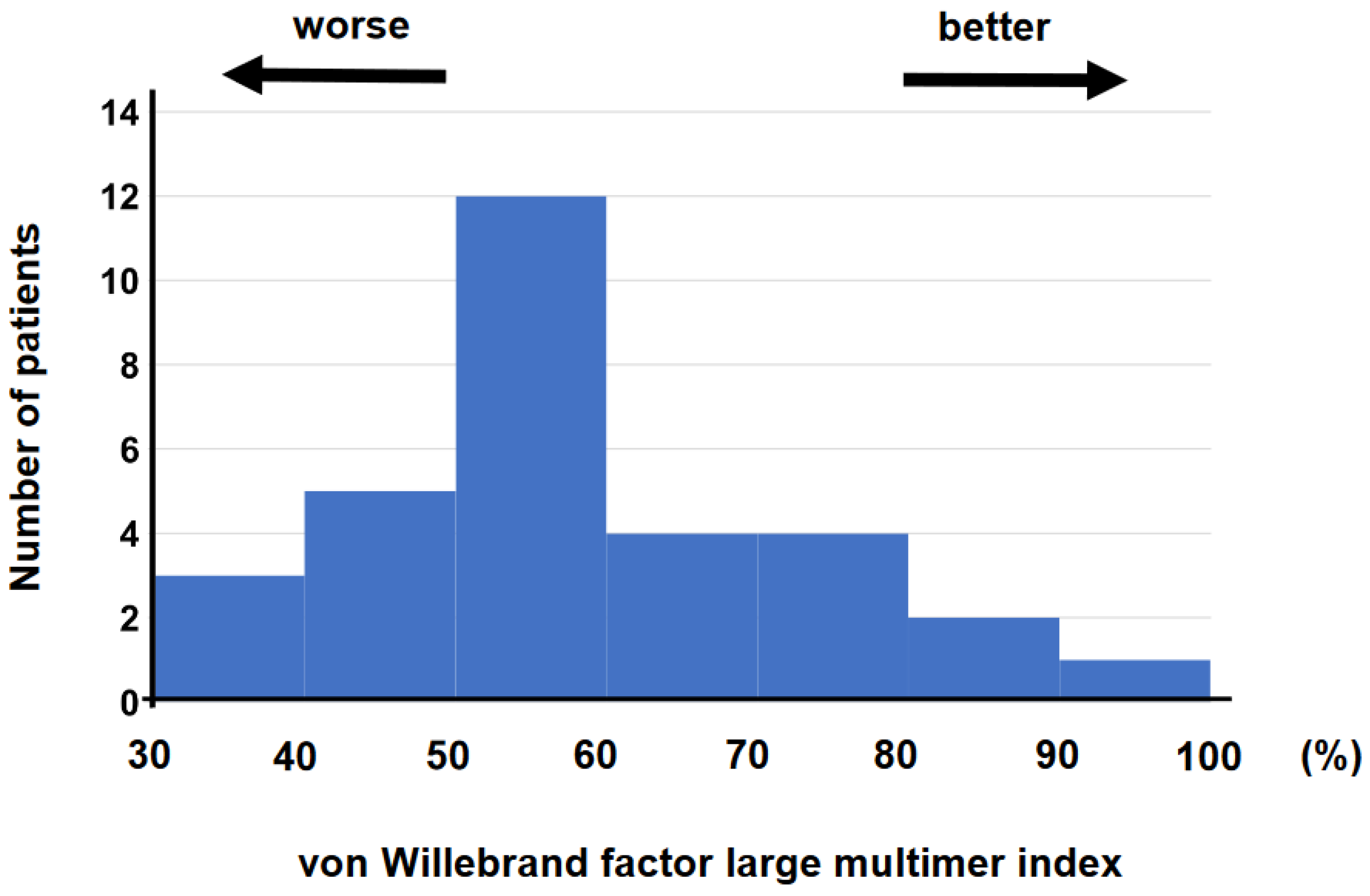
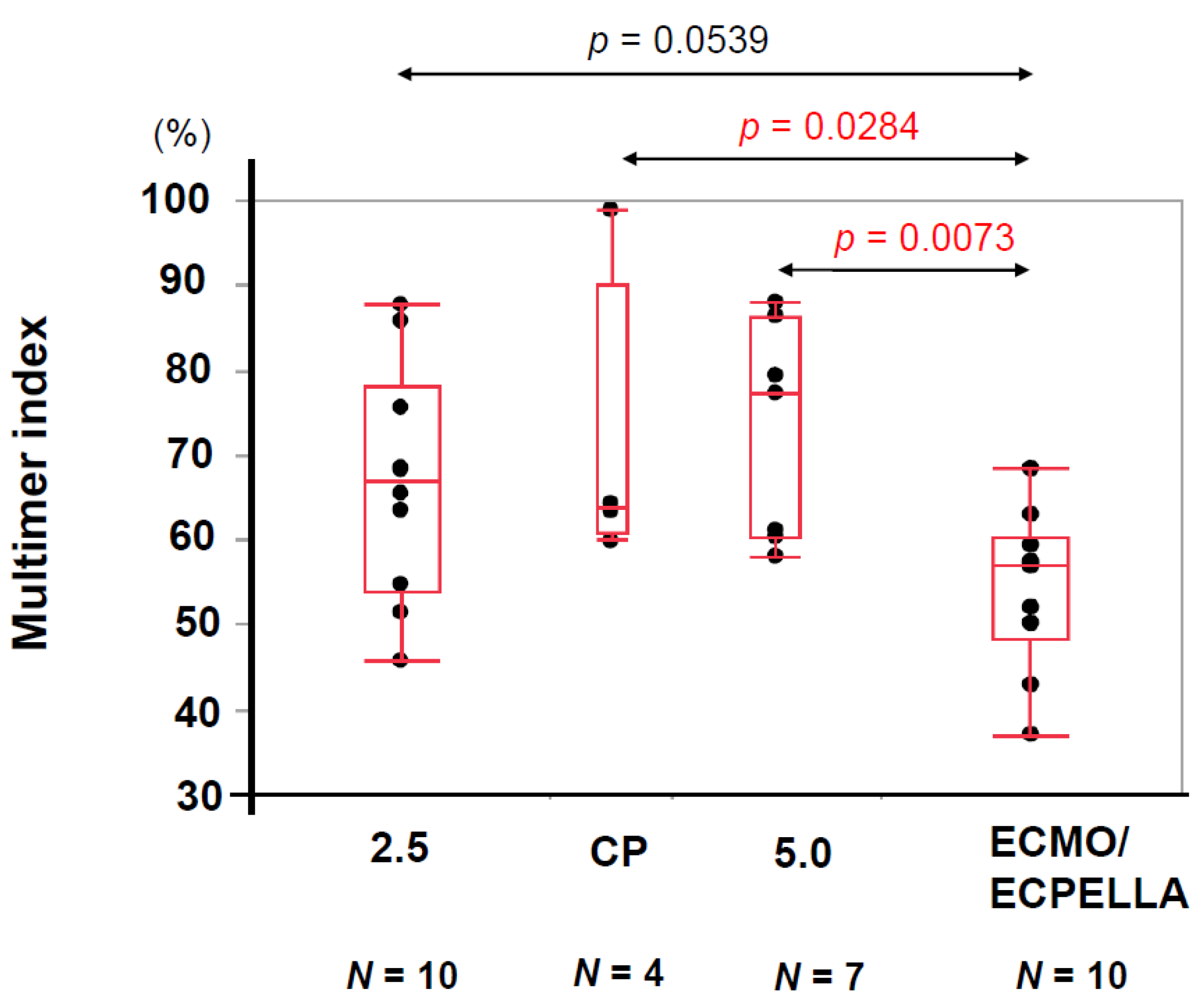
3.2. vWF Large-Multimer Index
3.3. Summary of Clinical Outcomes
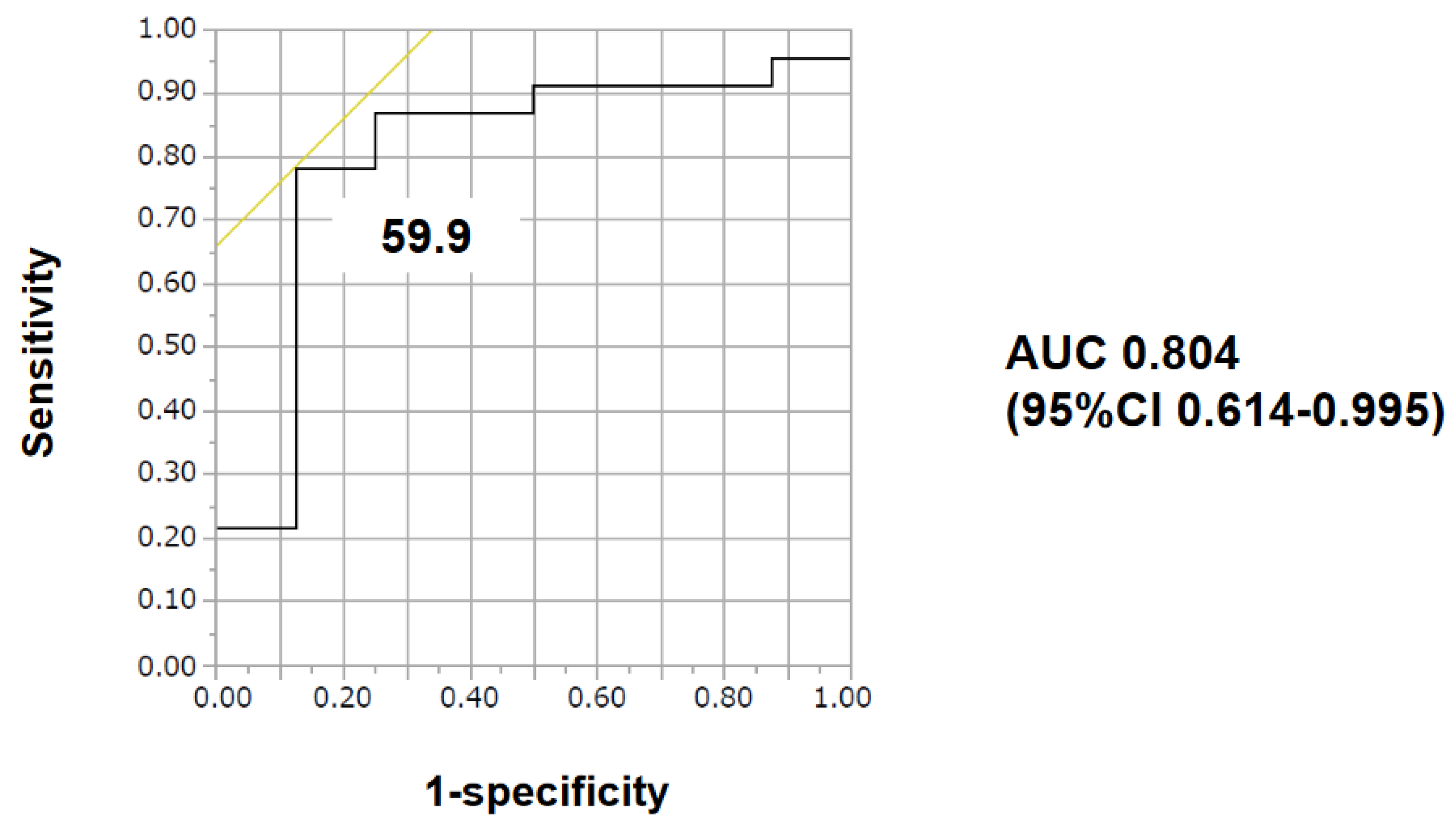
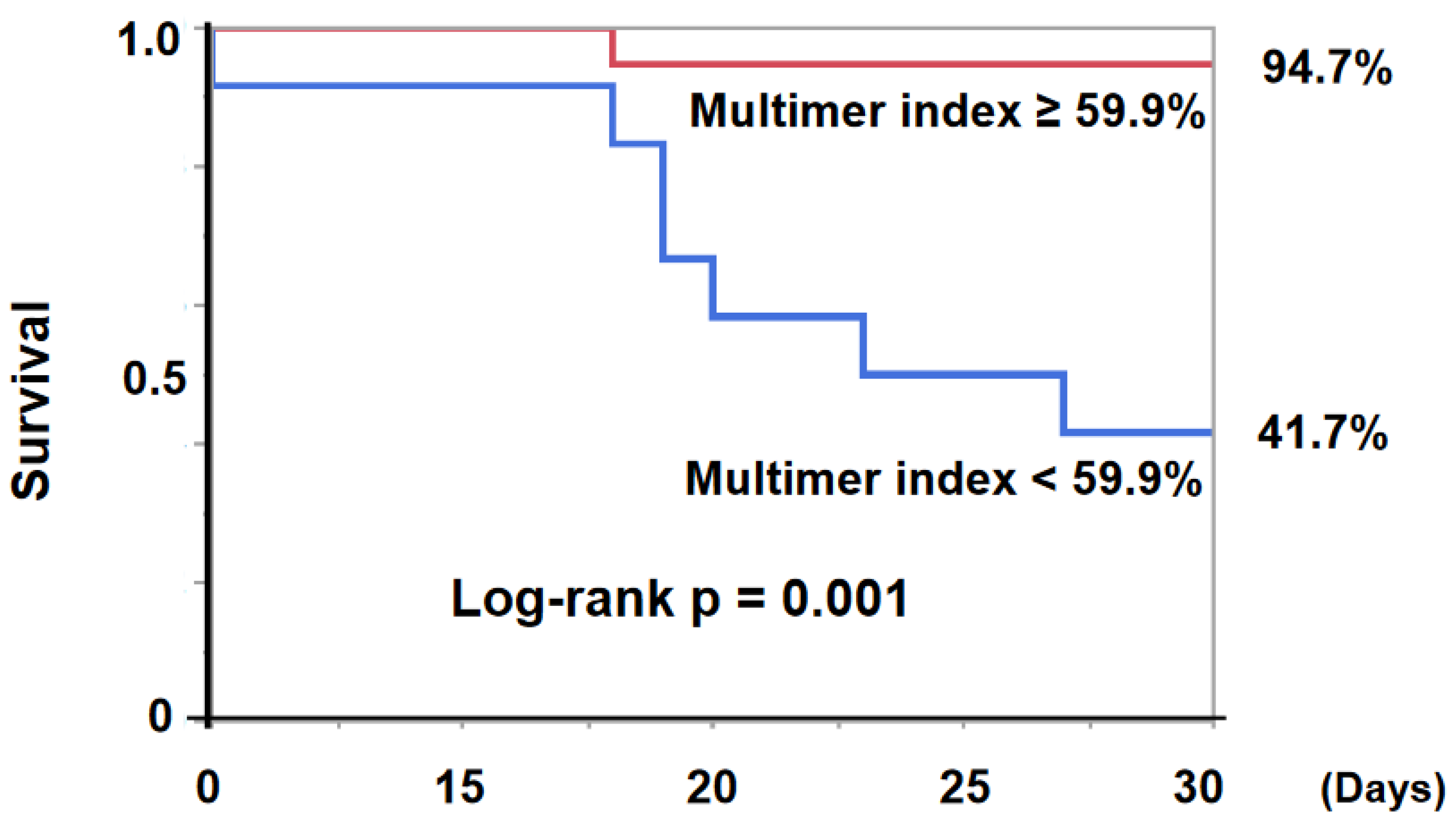
3.4. Impact of vWF Large-Multimer Index on the Primary Endpoint
3.5. Impact of vWF Multimer Index on the Secondary Endpoint
3.6. Characteristics of the Patients with Low vWF Multimer Index
4. Discussion
4.1. vWF Multimer Index
4.2. A Decrease in vWF Multimer Index
4.3. Prognostic Impact of Low vWF Multimer Index
4.4. Recommended Strategy to Manage AVWS
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hall, S.A.; Uriel, N.; Carey, S.A.; Edens, M.; Gong, G.; Esposito, M.; O’Kelly, R.; Annamalai, S.; Aghili, N.; Adatya, S.; et al. Use of a percutaneous temporary circulatory support device as a bridge to decision during acute decompensation of advanced heart failure. J. Heart Lung Transplant. 2018, 37, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Goldfarb, M.; Czer, L.S.; Lam, L.D.; Moriguchi, J.; Arabia, F.A.; Volod, O. High Molecular Weight von Willebrand Factor Multimer Loss and Bleeding in Patients with Short-Term Mechanical Circulatory Support Devices: A Case Series. J. Extra Corpor. Technol. 2018, 50, 77–82. [Google Scholar] [PubMed]
- Kirklin, J.K.; Naftel, D.C.; Pagani, F.D.; Kormos, R.L.; Stevenson, L.W.; Blume, E.D.; Myers, S.L.; Miller, M.A.; Baldwin, J.T.; Young, J.B. Seventh INTERMACS annual report: 15,000 patients and counting. J. Heart Lung Transplant. 2015, 34, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Schlagenhauf, A.; Kalbhenn, J.; Geisen, U.; Beyersdorf, F.; Zieger, B. Acquired von Willebrand Syndrome and Platelet Function Defects during Extracorporeal Life Support (Mechanical Circulatory Support). Hamostaseologie 2020, 40, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Flierl, U.; Tongers, J.; Berliner, D.; Sieweke, J.T.; Zauner, F.; Wingert, C.; Riehle, C.; Bauersachs, J.; Schafer, A. Acquired von Willebrand syndrome in cardiogenic shock patients on mechanical circulatory microaxial pump support. PLoS ONE 2017, 12, e0183193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalbhenn, J.; Schlagenhauf, A.; Rosenfelder, S.; Schmutz, A.; Zieger, B. Acquired von Willebrand syndrome and impaired platelet function during venovenous extracorporeal membrane oxygenation: Rapid onset and fast recovery. J. Heart Lung Transplant. 2018, 37, 985–991. [Google Scholar] [CrossRef] [PubMed]
- Ruggeri, Z.M.; Zimmerman, T.S. The complex multimeric composition of factor VIII/von Willebrand factor. Blood 1981, 57, 1140–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamura, T.; Horiuchi, H.; Imai, M.; Tada, T.; Shiomi, H.; Kuroda, M.; Nishimura, S.; Takahashi, Y.; Yoshikawa, Y.; Tsujimura, A.; et al. Unexpectedly High Prevalence of Acquired von Willebrand Syndrome in Patients with Severe Aortic Stenosis as Evaluated with a Novel Large Multimer Index. J. Atheroscler. Thromb. 2015, 22, 1115–1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakatsume, K.; Saito, K.; Akiyama, M.; Sasaki, K.; Kawatsu, S.; Takahashi, G.; Adachi, O.; Kawamoto, S.; Horiuchi, H.; Saiki, Y. Association between the severity of acquired von Willebrand syndrome and gastrointestinal bleeding after continuous-flow left ventricular assist device implantation. Eur. J. Cardiothorac. Surg. 2018, 54, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Dufour, N.; Radjou, A.; Thuong, M. Hemolysis and Plasma Free Hemoglobin During Extracorporeal Membrane Oxygenation Support: From Clinical Implications to Laboratory Details. ASAIO J. 2020, 66, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Kalbhenn, J.; Schmidt, R.; Nakamura, L.; Schelling, J.; Rosenfelder, S.; Zieger, B. Early diagnosis of acquired von Willebrand Syndrome (AVWS) is elementary for clinical practice in patients treated with ECMO therapy. J. Atheroscler. Thromb. 2015, 22, 265–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabit, C.E.; Chen, P.; Kim, G.H.; Fedson, S.E.; Sayer, G.; Coplan, M.J.; Jeevanandam, V.; Uriel, N.; Liao, J.K. Elevated Angiopoietin-2 Level in Patients with Continuous-Flow Left Ventricular Assist Devices Leads to Altered Angiogenesis and Is Associated With Higher Nonsurgical Bleeding. Circulation 2016, 134, 141–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skelton, J.K.; Purcell, R. Preclinical models for studying immune responses to traumatic injury. Immunology 2021, 162, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Uriel, N.; Colombo, P.C.; Cleveland, J.C.; Long, J.W.; Salerno, C.; Goldstein, D.J.; Patel, C.B.; Ewald, G.A.; Tatooles, A.J.; Silvestry, S.C.; et al. Hemocompatibility-Related Outcomes in the MOMENTUM 3 Trial at 6 Months: A Randomized Controlled Study of a Fully Magnetically Levitated Pump in Advanced Heart Failure. Circulation 2017, 135, 2003–2012. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 31 | |
|---|---|
| age (years) | 69 (60, 82) |
| male sex | 16 (52%) |
| ischemic etiology | 20 (65%) |
| dilated cardiomyopathy | 6 (19%) |
| others | 5 (16%) |
| left ventricular ejection fraction (%) | 25 (20, 36) |
| Impella 2.5 | 14 (45%) |
| Impella CP | 5 (16%) |
| Impella 5.0 | 7 (23%) |
| extra corporeal membrane oxygenation | 10 (32%) |
| extra corporeal membrane oxygenation and Impella | 5 (16%) |
| systolic blood pressure (mmHg) | 94 (79, 108) |
| mean arterial pressure (mmHg) | 73 (63, 76) |
| pulse pressure (mmHg) | 32 (8, 55) |
| heart rate (bpm) | 90 (80, 106) |
| hemoglobin (g/dL) | 10.2 (9.3, 11.1) |
| platelet (×104/μL) | 8.0 (5.9, 13.5) |
| total bilirubin (mg/dL) | 1.4 (1.0, 2.2) |
| serum creatinine (mg/dL) | 1.26 (0.83, 1.79) |
| C-reactive protein (mg/dL) | 4.3 (1.8, 12.3) |
| B-type natriuretic peptide (pg/mL) | 437 (186, 646) |
| log10 B-type natriuretic peptide (pg/mL) | 2.64 (2.27, 2.81) |
| activated partial thromboplastin time (s) | 50.1 (41.3, 65.5) |
| lactate dehydrogenase (U/mL) | 838 (607, 1530) |
| Von Willebrand factor large-multimer index (%) | 63.0 (56.9, 75.6) |
| antiplatelets | 16 (52%) |
| Support duration (days) | 4 (2, 8) |
| Univariable Analysis | p-Value | Odds Ratio | 95% CI |
|---|---|---|---|
| age (years old) | 0.991 | 1.000 | 0.943–1.060 |
| male sex | 0.076 | 4.667 | 0.766–28.406 |
| mean arterial pressure (mmHg) | 0.196 | 1.065 | 0.966–1.175 |
| pulse pressure (mmHg) | 0.352 | 1.017 | 0.981–1.054 |
| left ventricular ejection fraction (%) | 0.993 | 1.002 | 0.946–1.062 |
| hemoglobin (g/dL) | 0.203 | 1.511 | 0.780–2.927 |
| platelet (×104/μL) | 0.024 | 1.278 | 0.979–1.669 |
| platelet < 9.8 × 104/μL | 0.038 | 0.131 | 0.014–1.242 |
| total bilirubin (mg/dL) | 0.365 | 0.878 | 0.663–1.163 |
| serum creatinine (mg/dL) | 0.262 | 0.405 | 0.081-2.026 |
| C-reactive protein (mg/dL) | 0.272 | 0.948 | 0.864–1.042 |
| log10B-type natriuretic peptide | 0.436 | 1.939 | 0.359–10.460 |
| activated partial thromboplastin time (s) | 0.747 | 0.993 | 0.954–1.033 |
| vWF large-multimer index (%) | 0.0318 | 1.079 | 0.995–1.171 |
| vWF large-multimer index < 59.9% | 0.0008 | 0.040 | 0.004–0.403 |
| support duration (days) | 0.223 | 0.856 | 0.664–1.102 |
| Impella 2.5 | 0.612 | 1.528 | 0.293–7.945 |
| Impella CP | 0.998 | NA | NA |
| Impella 5.0 | 0.439 | 2.471 | 0.250–24.463 |
| extracorporeal membrane oxygenation | 0.007 | 0.070 | 0.011–0.483 |
| ECPELLA | 0.436 | 0.450 | 0.060–3.353 |
| antiplatelets | 0.477 | 0.550 | 0.106–2.860 |
| multivariable analysis | p-value | Odds ratio | 95% CI |
| platelet < 9.8 × 104/μL | 0.172 | 0.126 | 0.006–2.462 |
| vWF large-multimer index < 59.9% | 0.035 | 0.044 | 0.002–0.805 |
| extracorporeal membrane oxygenation | 0.691 | 0.572 | 0.036–9.024 |
| C-Statistics | 95% CI | |
|---|---|---|
| Platelet | 0.747 | 0.545–0.950 |
| vWF large-multimer index | 0.804 | 0.614–0.995 |
| extracorporeal membrane oxygenation | 0.788 | 0.589–0.987 |
| vWF Multimer Index (<59.9%) (N = 12) | vWF Multimer Index (≧59.9%) (N = 19) | p Value | |
|---|---|---|---|
| age (years) | 67.5 (57, 71.8) | 71 (65, 83) | 0.173 |
| male sex | 5 (42%) | 11 (58%) | 0.473 |
| ischemic etiology | 10 (83%) | 10 (52%) | 0.128 |
| dilated cardiomyopathy | 1 (8%) | 5 (26%) | 0.363 |
| others | 1 (8%) | 4 (21%) | 0.624 |
| left ventricular ejection fraction (%) | 25 (21, 48.5) | 30 (20, 26) | 0.951 |
| Impella 2.5 | 6 (50%) | 8 (42%) | 0.724 |
| Impella CP | 1 (8%) | 4 (25%) | 0.624 |
| Impella 5.0 | 1 (8%) | 6 (32%) | 0.202 |
| extra corporeal membrane oxygenation | 8 (67%) | 2 (11%) | 0.002 * |
| mean arterial pressure (mmHg) | 73 (61, 77) | 73 (63, 76) | 0.880 |
| pulse pressure (mmHg) | 31 (9, 51) | 32 (8, 56) | 0.745 |
| hemoglobin (g/dL) | 10.9 (8.8, 11.9) | 10.2 (9.3, 10.9) | 0.516 |
| platelet (× 104/μL) | 7.4 (4.1, 11.2) | 8.9 (5.9, 14.1) | 0.264 |
| total bilirubin (mg/dL) | 1.8 (1.1, 2.8) | 1.3 (0.8, 2.2) | 0.247 |
| serum creatinine (mg/dL) | 1.24 (1.02, 1.72) | 1.32 (0.78, 1.81) | 0.792 |
| C-reactive protein (mg/dL) | 6.9 (1.0, 20.0) | 4.2 (3.1, 11.8) | 0.655 |
| B-type natriuretic peptide (pg/mL) | 458 (222, 817) | 402 (184, 617) | 0.715 |
| lactate dehydrogenase (U/mL) | 1297 (900, 2247) | 633 (265, 1389) | 0.007 * |
| activated partial thromboplastin time (s) | 53.1 (37.9, 65.4) | 50.1 (43.5, 67.7) | 0.871 |
| antiplatelets | 8 (67%) | 8 (42%) | 0.273 |
| support duration (days) | 6.5 (3, 8) | 3 (2, 6) | 0.149 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, M.; Imamura, T.; Ueno, H.; Kinugawa, K. Impact of the Severity of Acquired von Willebrand Syndrome on the Short-Term Prognosis in Patients with Temporary Mechanical Circulatory Support. Medicina 2022, 58, 238. https://doi.org/10.3390/medicina58020238
Nakamura M, Imamura T, Ueno H, Kinugawa K. Impact of the Severity of Acquired von Willebrand Syndrome on the Short-Term Prognosis in Patients with Temporary Mechanical Circulatory Support. Medicina. 2022; 58(2):238. https://doi.org/10.3390/medicina58020238
Chicago/Turabian StyleNakamura, Makiko, Teruhiko Imamura, Hiroshi Ueno, and Koichiro Kinugawa. 2022. "Impact of the Severity of Acquired von Willebrand Syndrome on the Short-Term Prognosis in Patients with Temporary Mechanical Circulatory Support" Medicina 58, no. 2: 238. https://doi.org/10.3390/medicina58020238
APA StyleNakamura, M., Imamura, T., Ueno, H., & Kinugawa, K. (2022). Impact of the Severity of Acquired von Willebrand Syndrome on the Short-Term Prognosis in Patients with Temporary Mechanical Circulatory Support. Medicina, 58(2), 238. https://doi.org/10.3390/medicina58020238