
Fat Is Consistently Present within the Plantar Muscular Space of the Human Foot—An Anatomical Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimens and Preparation
2.2. Quantification of Fat within the Plantar Muscle Compartments of the Foot
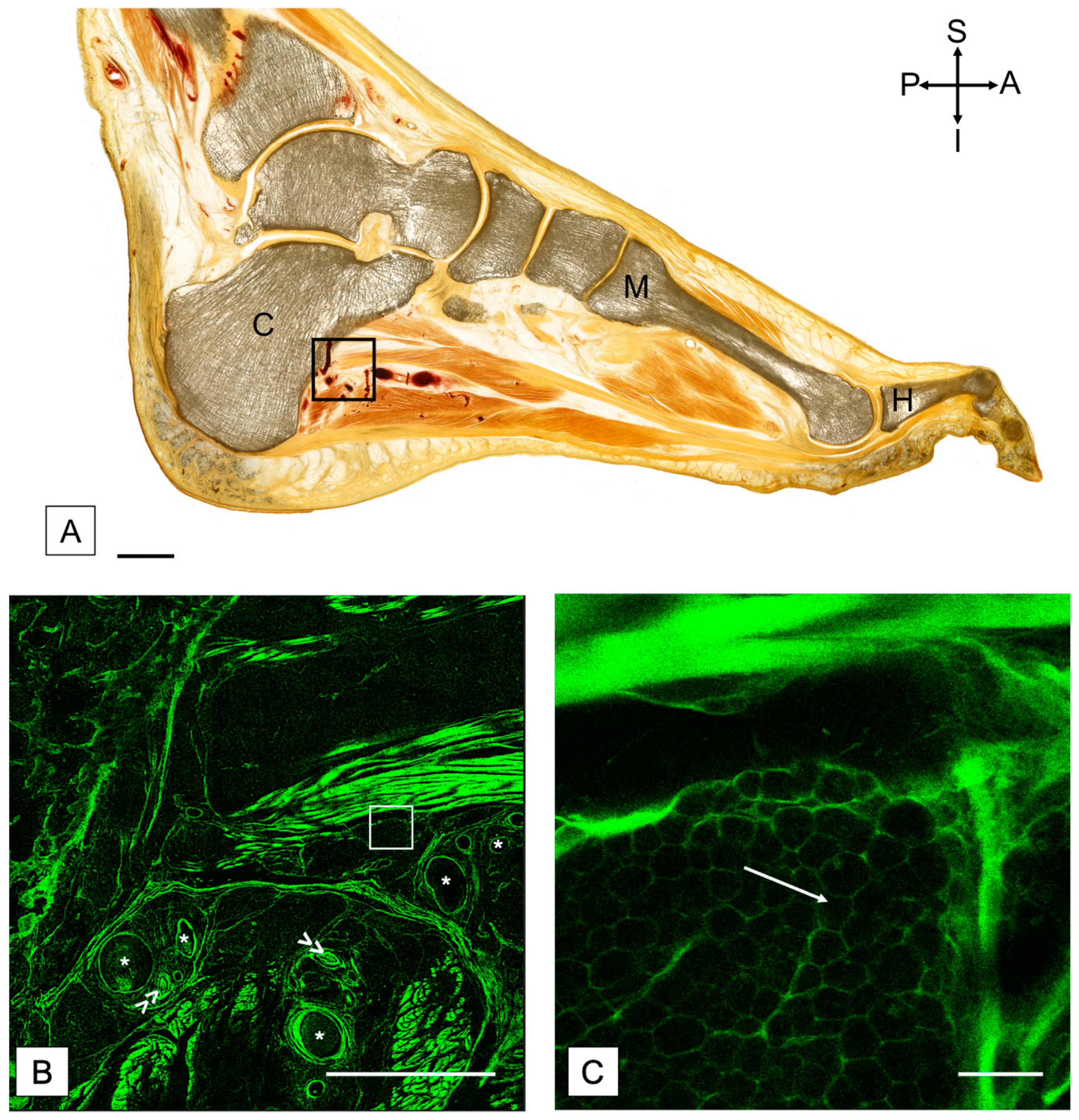
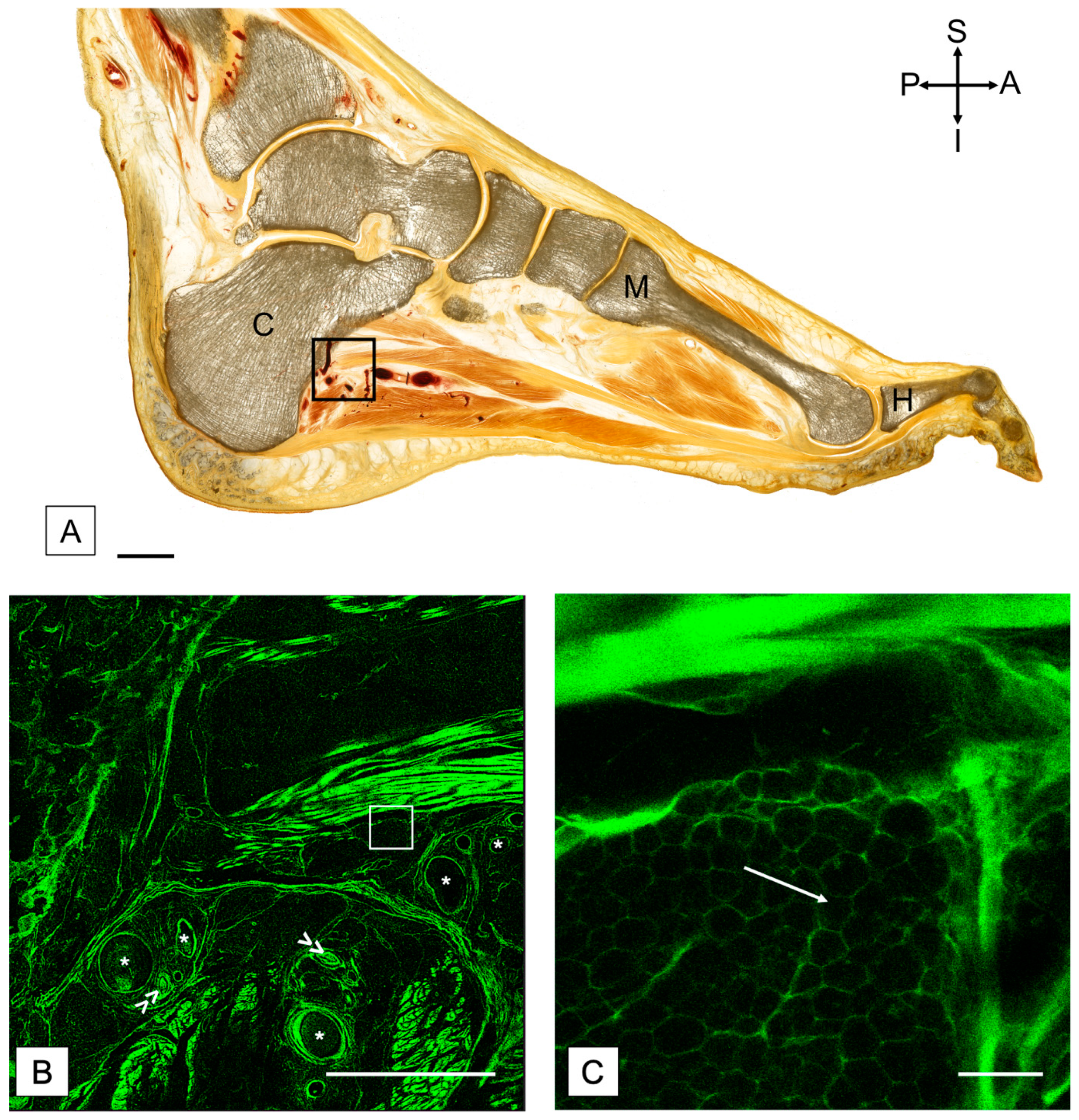
2.3. Plastination and Confocal Microscopy
2.4. Statistical Analysis
3. Results
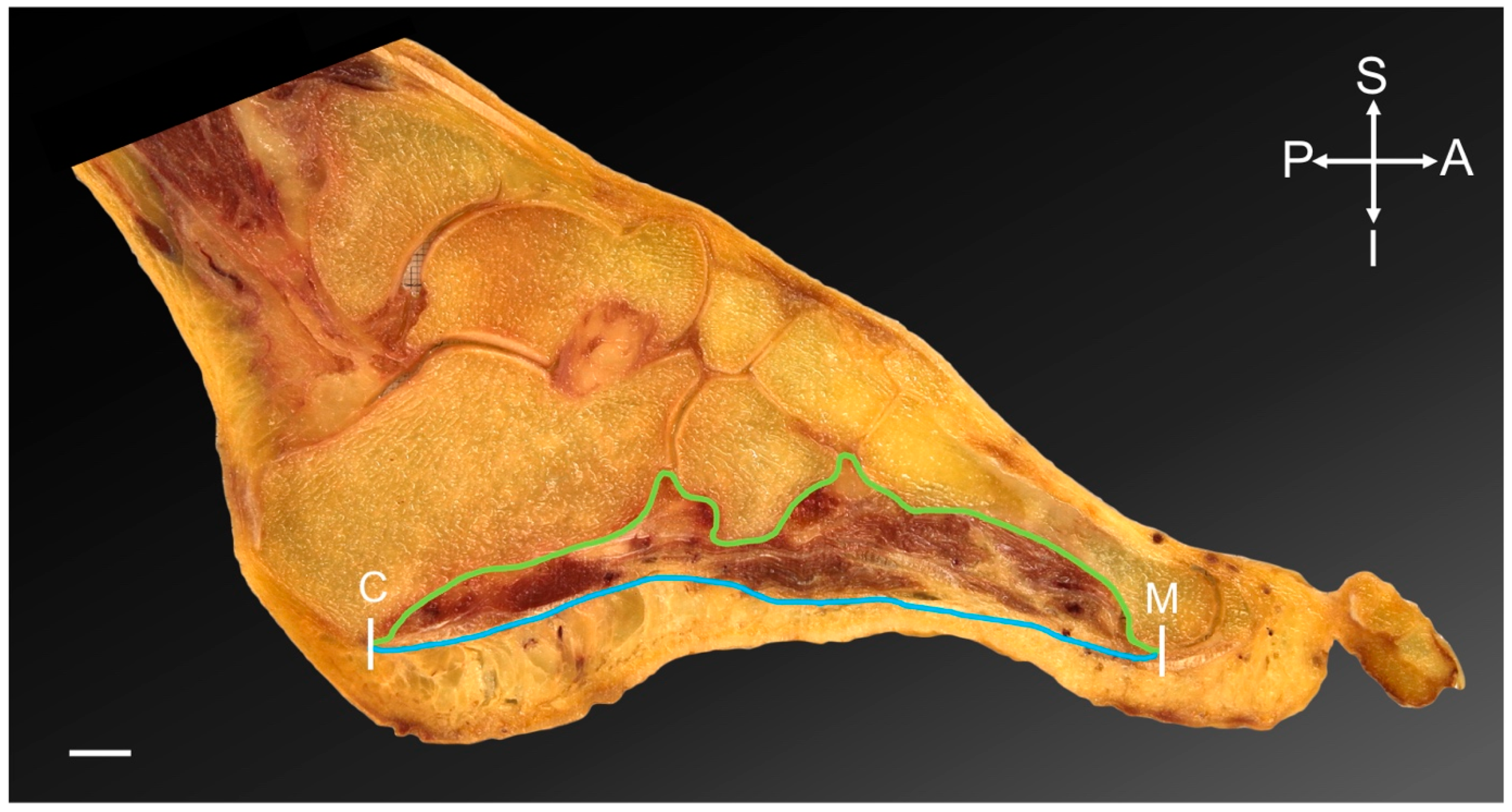
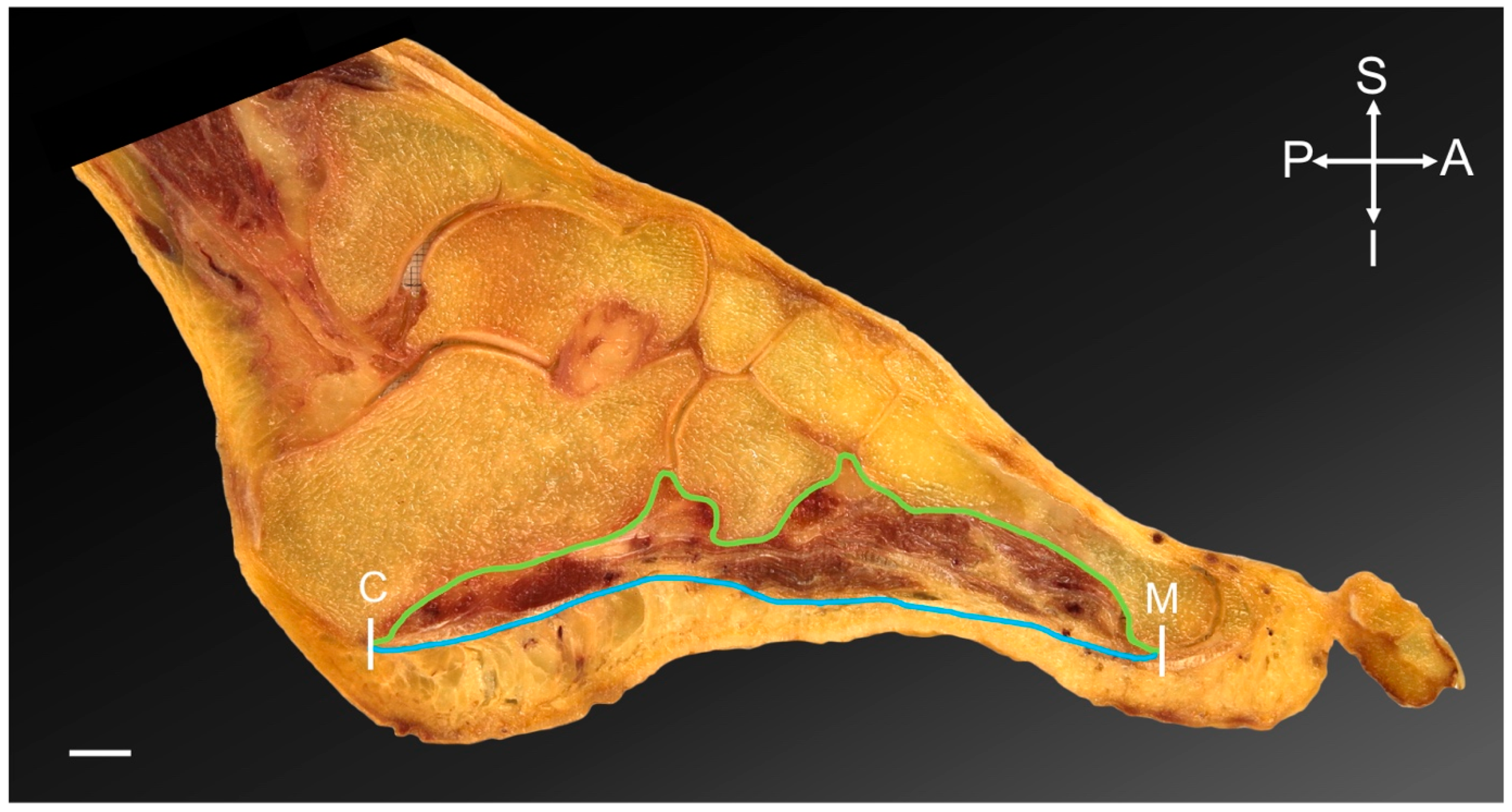
3.1. All Specimens Demonstrated Fat within the PMSF
3.2. Likely No Difference in Fat Percentage According to Foot Size
3.3. Percentage of Fat Was Similar between Sexes, Sides and Subregions
4. Discussion
4.1. Adipose Tissue within the PMSF Is Likely a Consistent Observation in Elderly Individuals
4.2. It Is Unclear Whether Fat within the PMSF Helps or Hinders Locomotion
4.3. Reciprocal Factors May Contribute to Fat in the PMSF
4.4. No Regional Differences in PMSF Fat Percentage Are Present in This Preliminary Cohort
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Light and Poor-Average Muscle Definition and Size | Average and Poor-Average Muscle Definition and Size | Average and Average-Good Muscle Definition and Size | Heavy and Poor-Average Muscle Definition and Size | |
|---|---|---|---|---|
| N | 3 | 3 | 1 | 1 |
| Mean | 26.72 | 28.53 | 26.60 | 17.60 |
| SD | 11.66 | 3.60 | NA | NA |
References
- McKeon, P.O.; Hertel, J.; Bramble, D.; Davis, I. The foot core system: A new paradigm for understanding intrinsic foot muscle function. Br. J. Sports Med. 2015, 49, 290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tourillon, R.; Gojanovic, B.; Fourchet, F. How to Evaluate and Improve Foot Strength in Athletes: An Update. Front. Sports Act. Living 2019, 1, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fourchet, F.; Gojanovic, B. Foot core strengthening: Relevance in injury prevention and rehabilitation for runners. Swiss Sports Exerc. Med. 2016, 64, 26–30. [Google Scholar]
- Okamura, K.; Kanai, S.; Fukuda, K.; Tanaka, S.; Ono, T.; Oki, S. The effect of additional activation of the plantar intrinsic foot muscles on foot kinematics in flat-footed subjects. Foot 2019, 38, 19–23. [Google Scholar] [CrossRef]
- Kumar, C.G.; Rajagopal, K.V.; Hande, H.M.; Maiya, A.G.; Mayya, S.S. Intrinsic foot muscle and plantar tissue changes in type 2 diabetes mellitus. J. Diabetes 2015, 7, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Bruening, D.A.; Ridge, S.T.; Jacobs, J.L.; Olsen, M.T.; Griffin, D.W.; Ferguson, D.H.; Bassett, K.E.; Johnson, A.W. Functional assessments of foot strength: A comparative and repeatability study. BMC Musculoskelet. Disord. 2019, 20, 608. [Google Scholar] [CrossRef]
- Lee, E.; Cho, J.; Lee, S. Short-Foot Exercise Promotes Quantitative Somatosensory Function in Ankle Instability: A Randomized Controlled Trial. Med. Sci. Monit. 2019, 25, 618–626. [Google Scholar] [CrossRef]
- Gooding, T.M.; Feger, M.A.; Hart, J.M.; Hertel, J. Intrinsic Foot Muscle Activation During Specific Exercises: A T2 Time Magnetic Resonance Imaging Study. J. Athl. Train. 2016, 51, 644–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soysa, A.; Hiller, C.; Refshauge, K.; Burns, J. Importance and challenges of measuring intrinsic foot muscle strength. J. Foot Ankle Res. 2012, 5, 29. [Google Scholar] [CrossRef] [Green Version]
- Fourchet, F.; McKeon, P. Foot core strengthening: An update about the intrinsic foot muscles recruitment. Br. J. Sports Med. 2015, 49 (Suppl. S1), A6. [Google Scholar] [CrossRef]
- Unver, B.; Erdem, E.U.; Akbas, E. Effects of Short-Foot Exercises on Foot Posture, Pain, Disability, and Plantar Pressure in Pes Planus. J. Sport Rehabil. 2019, 29, 436–440. [Google Scholar] [CrossRef]
- Fraser, J.J.; Hertel, J. Effects of a 4-Week Intrinsic Foot Muscle Exercise Program on Motor Function: A Preliminary Randomized Control Trial. J. Sport Rehabil. 2019, 28, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Estrada, M.; Kleppinger, A.; Judge, J.O.; Walsh, S.J.; Kuchel, G.A. Functional impact of relative versus absolute sarcopenia in healthy older women. J. Am. Geriatr. Soc. 2007, 55, 1712–1719. [Google Scholar] [CrossRef]
- Perkisas, S.; Vandewoude, M. Where frailty meets diabetes. Diabetes Metab. Res. Rev. 2016, 32 (Suppl. S1), 261–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delmonico, M.J.; Harris, T.B.; Visser, M.; Park, S.W.; Conroy, M.B.; Velasquez-Mieyer, P.; Boudreau, R.; Manini, T.M.; Nevitt, M.; Newman, A.B.; et al. Body, Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am. J. Clin. Nutr. 2009, 90, 1579–1585. [Google Scholar] [PubMed]
- Rahemi, H.; Nigam, N.; Wakeling, J.M. The effect of intramuscular fat on skeletal muscle mechanics: Implications for the elderly and obese. J. R. Soc. Interface 2015, 12, 20150365. [Google Scholar] [CrossRef] [Green Version]
- Tsuyuguchi, R.; Kurose, S.; Seto, T.; Takao, N.; Tagashira, S.; Tsutsumi, H.; Otsuki, S.; Kimura, Y. Toe grip strength in middle-aged individuals as a risk factor for falls. J. Sports Med. Phys. Fit. 2018, 58, 1325–1330. [Google Scholar] [CrossRef]
- Rosen, E.D.; Spiegelman, B.M. Adipocytes as regulators of energy balance and glucose homeostasis. Nature 2006, 444, 847–853. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, J.; Tierney, P.; Murray, P.; O’Brien, M. The infrapatellar fat pad: Anatomy and clinical correlations. Knee Surg. Sports Traumatol. Arthrosc. 2005, 13, 268–272. [Google Scholar] [CrossRef]
- Zwick, R.K.; Guerrero-Juarez, C.F.; Horsley, V.; Plikus, M.V. Anatomical, Physiological, and Functional Diversity of Adipose Tissue. Cell Metab. 2018, 27, 68–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanabe, Y.; Koga, M.; Saito, M.; Matsunaga, Y.; Nakayama, K. Inhibition of adipocyte differentiation by mechanical stretching through ERK-mediated downregulation of PPARgamma2. J. Cell Sci. 2004, 117 Pt 16, 3605–3614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoham, N.; Gottlieb, R.; Sharabani-Yosef, O.; Zaretsky, U.; Benayahu, D.; Gefen, A. Static mechanical stretching accelerates lipid production in 3T3-L1 adipocytes by activating the MEK signaling pathway. Am. J. Physiol. Cell Physiol. 2012, 302, C429–C441. [Google Scholar] [CrossRef] [Green Version]
- Macchi, V.; Porzionato, A.; Sarasin, G.; Petrelli, L.; Guidolin, D.; Rossato, M.; Fontanella, C.G.; Natali, A.; De Caro, R. The Infrapatellar Adipose Body: A Histotopographic Study. Cells Tissues Organs 2016, 201, 220–231. [Google Scholar] [CrossRef]
- Clockaerts, S.; Bastiaansen-Jenniskens, Y.M.; Runhaar, J.; Van Osch, G.J.; Van Offel, J.F.; Verhaar, J.A.; De Clerck, L.S.; Somville, J. The infrapatellar fat pad should be considered as an active osteoarthritic joint tissue: A narrative review. Osteoarthr. Cartil. 2010, 18, 876–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, D.T.; Hodler, J.; Mengiardi, B.; Pfirmann, C.W.A.; Espinosa, N.; Zanetti, M. Fatty Muscle Atrophy: Prevalence in the Hindfoot Muscles on MR Images of Asymptomatic Volunteers and Patients with Foot Pain. Radiology 2009, 253, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Tian, Z.; Torigoe, D.; Zhao, J.; Xie, P.; Sugizaki, T.; Sato, M.; Horiguchi, H.; Terada, K.; Kadomatsu, T.; et al. Aging- and obesity-related peri-muscular adipose tissue accelerates muscle atrophy. PLoS ONE 2019, 14, e0221366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheuy, V.A.; Commean, P.K.; Hastings, M.K.; Mueller, M.J. Reliability and validity of a MR-based volumetric analysis of the intrinsic foot muscles. J. Magn. Reson. Imaging 2013, 38, 1083–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bus, S.A.; Maas, M.; Lindeboom, R. Reproducibility of foot structure measurements in neuropathic diabetic patients using magnetic resonance imaging. J. Magn. Reson. Imaging 2006, 24, 25–32. [Google Scholar] [CrossRef]
- Bus, S.A.; Maas, M.; Michels, R.P.; Levi, M. Role of intrinsic muscle atrophy in the etiology of claw toe deformity in diabetic neuropathy may not be as straightforward as widely believed. Diabetes Care 2009, 32, 1063–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheuy, V.A.; Hastings, M.K.; Commean, P.K.; Ward, S.R.; Mueller, M.J. Intrinsic foot muscle deterioration is associated with metatarsophalangeal joint angle in people with diabetes and neuropathy. Clin. Biomech. 2013, 28, 1055–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.C.; Wu, J.; Baltzis, D.; Veves, A.; Greenman, R.L. MRI assessment of regional differences in phosphorus-31 metabolism and morphological abnormalities of the foot muscles in diabetes. J. Magn. Reson. Imaging 2016, 44, 1132–1142. [Google Scholar] [CrossRef] [PubMed]
- Gallardo, E.; Garcia, A.; Combarros, O.; Berciano, J. Charcot-Marie-Tooth disease type 1A duplication: Spectrum of clinical and magnetic resonance imaging features in leg and foot muscles. Brain 2006, 129 Pt 2, 426–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Recht, M.P.; Grooff, P.; Ilaslan, H.; Recht, H.S.; Sferra, J.; Donley, B.G. Selective atrophy of the abductor digiti quinti: An MRI study. AJR Am. J. Roentgenol. 2007, 189, W123–W127. [Google Scholar] [CrossRef] [PubMed]
- Franettovich Smith, M.M.; Elliott, J.M.; Al-Najjar, A.; Weber, K.A., 2nd; Hoggarth, M.A.; Vicenzino, B.; Hodges, P.W.; Collins, N.J. New insights into intrinsic foot muscle morphology and composition using ultra-high-field (7-Tesla) magnetic resonance imaging. BMC Musculoskelet. Disord. 2021, 22, 97. [Google Scholar] [CrossRef] [PubMed]
- Morrison, T.; Jones, S.; Causby, R.S.; Thoirs, K. Can ultrasound measures of intrinsic foot muscles and plantar soft tissues predict future diabetes-related foot disease? A systematic review. PLoS ONE 2018, 13, e0199055. [Google Scholar] [CrossRef] [Green Version]
- Guglielmi, V.; Maresca, L.; D’Adamo, M.; Di Roma, M.; Lanzillo, C.; Federici, M.; Lauro, D.; Preziosi, P.; Bellia, A.; Sbraccia, P. Age-related different relationships between ectopic adipose tissues and measures of central obesity in sedentary subjects. PLoS ONE 2014, 9, e103381. [Google Scholar] [CrossRef] [Green Version]
- Crosado, B.; Loffler, S.; Ondruschka, B.; Zhang, M.; Zwirner, J.; Hammer, N. Phenoxyethanol-Based Embalming for Anatomy Teaching: An 18 Years’ Experience with Crosado Embalming at the University of Otago in New Zealand. Anat. Sci. Educ. 2020, 13, 778–793. [Google Scholar] [CrossRef] [Green Version]
- Poilliot, A.; Doyle, T.; Tomlinson, J.; Zhang, M.; Zwirner, J.; Hammer, N. Quantification of fat in the posterior sacroiliac joint region: Fat volume is sex and age dependant. Sci. Rep. 2019, 9, 14935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, M.N.; Nash, L.G.; Barnett, R.; Nicholson, H.; Zhang, M. The Use of Confocal Microscopy for the Examination of E12 Sheet Plastinated Human Tissue. J. Plast. 2002, 17, 12–16. [Google Scholar]
- Chan, Y.H. Biostatistics 104: Correlation Analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar] [PubMed]
- Kohn, M.A.; Senyak, J. Sample Size Calculators. Available online: https://www.sample-size.net/ (accessed on 18 October 2021).
- Addison, O.; Marcus, R.L.; Lastayo, P.C.; Ryan, A.S. Intermuscular fat: A review of the consequences and causes. Int. J. Endocrinol. 2014, 2014, 309570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagano, A.F.; Brioche, T.; Arc-Chagnaud, C.; Demangel, R.; Chopard, A.; Py, G. Short-term disuse promotes fatty acid infiltration into skeletal muscle. J. Cachexia Sarcopenia Muscle 2018, 9, 335–347. [Google Scholar] [CrossRef]
- Niyomchan, A.; Panichareon, B.; Siriphorn, A.; Wongtawatchai, T. Age-related structural-mechanical property changes in human peroneus longus muscle. Folia Morphol. 2019, 78, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Lanza, M.B.; Ryan, A.S.; Gray, V.; Perez, W.J.; Addison, O. Intramuscular Fat Influences Neuromuscular Activation of the Gluteus Medius in Older Adults. Front. Physiol. 2020, 11, 614415. [Google Scholar] [CrossRef] [PubMed]
- Addison, O.; Young, P.; Inacio, M.; Bair, W.; Prettyman, M.G.; Beamer, B.; Ryan, A.S.; Rogers, M.W. Hip but Not Thigh Intramuscular Adipose Tissue is Associated with Poor Balance and Increased Temporal Gait Variability in Older Adults. Curr. Aging Sci. 2014, 7, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Suwa, M.; Imoto, T.; Kida, A.; Iwase, M.; Yokochi, T. Age-related reduction and independent predictors of toe flexor strength in middle-aged men. J. Foot Ankle Res. 2017, 10, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalin, P.S.; Crawford, R.J.; Marcon, M.; Manoliu, A.; Bouaicha, S.; Fischer, M.A.; Ulbrich, E.J. Shoulder muscle volume and fat content in healthy adult volunteers: Quantification with DIXON MRI to determine the influence of demographics and handedness. Skeletal. Radiol. 2018, 47, 1393–1402. [Google Scholar] [CrossRef]
- Riddiford-Harland, D.L.; Steele, J.R.; Baur, L.A. Medial midfoot fat pad thickness and plantar pressures: Are these related in children? Int. J. Pediatr. Obes. 2011, 6, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Trevino, J.H., III; Yuri, T.; Hatta, T.; Kiyoshige, Y.; Jacobs, P.M.; Giambini, H. Three-dimensional quantitative measurements of atrophy and fat infiltration in sub-regions of the supraspinatus muscle show heterogeneous distributions: A cadaveric study. Arch. Orthop. Trauma Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Meyer, D.C.; Pirkl, C.; Pfirrmann, C.W.; Zanetti, M.; Gerber, C. Asymmetric atrophy of the supraspinatus muscle following tendon tear. J. Orthop. Res. 2005, 23, 254–258. [Google Scholar] [CrossRef]
- Smyth, N.A.; Aiyer, A.A.; Kaplan, J.R.; Carmody, C.A.; Kadakia, A.R. Adult-acquired flatfoot deformity. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Kodithuwakku Arachchige, S.N.K.; Chander, H.; Knight, A. Flatfeet: Biomechanical implications, assessment and management. Foot 2019, 38, 81–85. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomlinson, J.; Klima, S.; Poilliot, A.; Zwirner, J.; Hammer, N. Fat Is Consistently Present within the Plantar Muscular Space of the Human Foot—An Anatomical Study. Medicina 2022, 58, 154. https://doi.org/10.3390/medicina58020154
Tomlinson J, Klima S, Poilliot A, Zwirner J, Hammer N. Fat Is Consistently Present within the Plantar Muscular Space of the Human Foot—An Anatomical Study. Medicina. 2022; 58(2):154. https://doi.org/10.3390/medicina58020154
Chicago/Turabian StyleTomlinson, Joanna, Stefan Klima, Amélie Poilliot, Johann Zwirner, and Niels Hammer. 2022. "Fat Is Consistently Present within the Plantar Muscular Space of the Human Foot—An Anatomical Study" Medicina 58, no. 2: 154. https://doi.org/10.3390/medicina58020154
APA StyleTomlinson, J., Klima, S., Poilliot, A., Zwirner, J., & Hammer, N. (2022). Fat Is Consistently Present within the Plantar Muscular Space of the Human Foot—An Anatomical Study. Medicina, 58(2), 154. https://doi.org/10.3390/medicina58020154