

Association of Uric Acid Albumin Ratio with Recurrence of Atrial Fibrillation after Cryoballoon Catheter Ablation

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Study Design and Patient Population
2.2. Definitions and Study Outcome
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haïssaguerre, M.; Marcus, F.I.; Fischer, B.; Clémenty, J. Radiofrequency catheter ablation in unusual mechanisms of atrial fibrillation: Report of three cases. J. Cardiovasc. Electrophysiol. 1994, 5, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Calkins, H.; Reynolds, M.R.; Spector, P.; Sondhi, M.; Xu, Y.; Martin, A.; Williams, C.J.; Sledge, I. Treatment of atrial fibrillation with antiarrhythmic drugs or radiofrequency ablation: Two systematic literature reviews and meta-analyses. Circ. Arrhythm Electrophysiol. 2009, 2, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Dretzke, J.; Chuchu, N.; Agarwal, R.; Herd, C.; Chua, W.; Fabritz, L.; Bayliss, S.; Kotecha, D.; Deeks, J.; Kirchhof, P.; et al. Predicting recurrent atrial fibrillation after catheter ablation: A systematic review of prognostic models. Europace 2020, 22, 748–760. [Google Scholar] [CrossRef] [PubMed]
- Harada, M.; Nattel, S. Implications of Inflammation and Fibrosis in Atrial Fibrillation Pathophysiology. Card. Electrophysiol. Clin. 2021, 13, 25–35. [Google Scholar] [CrossRef]
- Guo, Y.; Lip, G.Y.; Apostolakis, S. Inflammation in atrial fibrillation. J. Am. Coll. Cardiol. 2012, 60, 2263–2270. [Google Scholar] [CrossRef]
- Kang, D.H.; Ha, S.K. Uric Acid Puzzle: Dual Role as Anti-oxidantand Pro-oxidant. Electrolyte Blood Press. 2014, 12, 1–6. [Google Scholar] [CrossRef]
- Deng, Y.; Liu, F.; Yang, X.; Xia, Y. The Key Role of Uric Acid in Oxidative Stress, Inflammation, Fibrosis, Apoptosis, and Immunity in the Pathogenesis of Atrial Fibrillation. Front. Cardiovasc. Med. 2021, 8, 641136. [Google Scholar] [CrossRef]
- Selçuk, M.; Çınar, T.; Şaylık, F.; Akbulut, T.; Asal, S.; Çiçek, V.; Hayiroglu, M.I.; Tanboğa, I.H. Predictive value of uric acid/albumin ratio for the prediction of new-onset atrial fibrillation in patients with ST-Elevation myocardial infarction. Rev. Investig. Clin. 2022, 74, 156–164. [Google Scholar]
- Blomström-Lundqvist, C.; Gizurarson, S.; Schwieler, J.; Jensen, S.M.; Bergfeldt, L.; Kenneback, G.; Rubulis, A.; Malmborg, H.; Raatikainen, P.; Lonnerholm, S.; et al. Effect of Catheter Ablation vs Antiarrhythmic Medication on Quality of Life in Patients with Atrial Fibrillation: The CAPTAF Randomized Clinical Trial. JAMA 2019, 321, 1059–1068. [Google Scholar] [CrossRef]
- Odening, K.E.; Deiß, S.; Dilling-Boer, D.; Didenko, M.; Eriksson, U.; Nedios, S.; Ng, F.S.; Luque, I.R.; Borque, P.S.; Vernooy, K.; et al. Mechanisms of sex differences in atrial fibrillation: Role of hormones and differences in electrophysiology, structure, function, and remodelling. Europace 2019, 21, 366–376. [Google Scholar] [CrossRef]
- Schotten, U.; Verheule, S.; Kirchhof, P.; Goette, A. Pathophysiological mechanisms of atrial fibrillation: A translational appraisal. Physiol. Rev. 2011, 91, 265–325. [Google Scholar] [CrossRef]
- Şaylık, F.; Çınar, T.; Akbulut, T.; Hayıroğlu, M.İ. Comparison of catheter ablation and medical therapy for atrial fibrillation in heart failure patients: A meta-analysis of randomized controlled trials. Heart Lung 2022, 57, 69–74. [Google Scholar] [CrossRef]
- Saliba, W.; Schliamser, J.E.; Lavi, I.; Barnett-Griness, O.; Gronich, N.; Rennert, G. Catheter ablation of atrial fibrillation is associated with reduced risk of stroke and mortality: A propensity score-matched analysis. Heart Rhythm. 2017, 14, 635–642. [Google Scholar] [CrossRef]
- Mesquita, J.; Ferreira, A.M.; Cavaco, D.; Costa, F.M.; Carmo, P.; Marques, H.; Morgado, F.; Mendes, M.; Adragao, P. Development and validation of a risk score for predicting atrial fibrillation recurrence after a first catheter ablation procedure-ATLAS score. Europace 2018, 20, f428–f435. [Google Scholar] [CrossRef]
- Han, W.; Liu, Y.; Sha, R.; Liu, H.; Liu, A.; Maduray, K.; Ge, J.; Ma, C.; Zhong, J. A prediction model of atrial fibrillation recurrence after first catheter ablation by a nomogram: HASBLP score. Front. Cardiovasc. Med. 2022, 9, 934664. [Google Scholar] [CrossRef]
- Danesh, J.; Collins, R.; Appleby, P.; Peto, R. Association of fibrinogen, C-reactive protein, albumin, or leukocyte count with coronary heart disease: Meta-analyses of prospective studies. JAMA 1998, 279, 1477–1482. [Google Scholar] [CrossRef]
- Kushiyama, A.; Nakatsu, Y.; Matsunaga, Y.; Yamamotoya, T.; Mori, K.; Ueda, K.; Inoue, Y.; Sakoda, H.; Fujishiro, M.; Ono, H.; et al. Role of Uric Acid Metabolism-Related Inflammation in the Pathogenesis of Metabolic Syndrome Components Such as Atherosclerosis and Nonalcoholic Steatohepatitis. Mediat. Inflamm. 2016, 2016, 8603164. [Google Scholar] [CrossRef]
- Liese, A.D.; Hense, H.-W.; Löwel, H.; Döring, A.; Tietze, M.; Keil, U. Association of serum uric acid with all-cause and cardiovascular disease mortality and incident myocardial infarction in the MONICA Augsburg cohort. World Health Organization Monitoring Trends and Determinants in Cardiovascular Diseases. Epidemiology 1999, 10, 391–397. [Google Scholar] [CrossRef]
- Høieggen, A.; Alderman, M.H.; Kjeldsen, S.E.; Julius, S.; Devereux, R.B.; de Faire, U.; Fyhrquist, F.; Ibsen, H.; Kristianson, K.; Lederballe-Pedersen, O.; et al. LIFE Study Group. The impact of serum uric acid on cardiovascular outcomes in the LIFE study. Kidney Int. 2004, 65, 1041–1049. [Google Scholar] [CrossRef]
- Tamariz, L.; Hernandez, F.; Bush, A.; Palacio, A.; Hare, J.M. Association between serum uric acid and atrial fibrillation: A systematic review and meta-analysis. Heart Rhythm. 2014, 11, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Maharani, N.; Kuwabara, M.; Hisatome, I. Hyperuricemia and Atrial Fibrillation. Int. Heart J. 2016, 57, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Carnes, C.; Chung, M.K.; Nakayama, T.; Nakayama, H.; Baliga, R.S.; Piao, S.; Kanderian, A.; Pavia, S.; Hamlin, R.L.; McCarthy, P.M.; et al. Ascorbate attenuates atrial pacing-induced peroxynitrite formation and electrical remodeling and decreases the incidence of postoperative atrial fibrillation. Circ. Res. 2001, 89, E32–E38. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, D.R.; Treuer, A.; Sun, Q.-A.; Stamler, J.S.; Hare, J.M. S-Nitrosylation of cardiac ion channels. J. Cardiovasc. Pharmacol. 2009, 54, 188–195. [Google Scholar] [CrossRef]
- Gill, J.S.; McKenna, W.J.; Camm, A.J. Free radicals irreversibly decrease Ca2+ currents in isolated guinea-pig ventricular myocytes. Eur. J. Pharmacol. 1995, 292, 337–340. [Google Scholar] [CrossRef]
- Çınar, T.; Şaylık, F.; Hayıroğlu, M.; Asal, S.; Selçuk, M.; Çiçek, V.; Tanboğa, I.H. The Association of Serum Uric Acid/Albumin Ratio with No-Reflow in Patients with ST Elevation Myocardial Infarction. Angiology 2022. ahead of print. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 170 | Recurrence (+) n = 53 | Recurrence (−) n = 117 | p Value | |
|---|---|---|---|---|
| Age, year | 59.1 ± 11.7 | 61.3 ± 11.5 | 57.6 ± 11.4 | 0.07 |
| Male, n (%) | 96 (56) | 29 (55) | 67 (57) | 0.44 |
| Hypertension, n (%) | 93 (54.7) | 43 (81.1) | 50 (42.7) | <0.01 |
| Coronary artery disease, n (%) | 41 (24.1) | 26 (49.1) | 15 (12.8) | <0.01 |
| Heart Failure, n (%) | 29 (17.1) | 24 (45.3) | 5 (4.3) | <0.01 |
| COPD, n (%) | 15 (8.8) | 6 (11.3) | 9 (7) | 0.10 |
| Diabetes mellitus, n (%) | 24 (14.1) | 12 (22.6) | 12 (10.3) | 0.03 |
| Chronic kidney disease, n (%) | 10 (5.9) | 3 (5.6) | 7 (6) | 0.50 |
| Smoking, n (%) | 54 (31.8) | 16 (30.2) | 38 (32.5) | 0.76 |
| CHA2DS2-VASC score | 1.8 ± 0.9 | 2.9 ± 1 | 1.4 ± 0.9 | <0.01 |
| AF duration, month | 17 {30} | 36 {43} | 12 {22.5} | <0.01 |
| AF pattern (PAF), n (%) | 121 (71.2) | 22 (41.5) | 99 (84.6) | <0.01 |
| Hemoglobin, g/L | 14.2 ± 5.6 | 14.7 ± 9.7 | 13.9 ± 1.8 | 0.40 |
| Serum creatinine, mg/dL | 0.9 ± 0.2 | 0.9 ± 0.2 | 0.8 ± 0.2 | 0.17 |
| LDL, mg/dL | 116 ± 34.5 | 116.2 ± 31.1 | 115.8 ± 36.1 | 0.94 |
| TSH, mIU/L | 2.1 ± 1 | 2.3 ± 1 | 1.8 ± 0,9 | 0.25 |
| CRP, mg/L | 0.2 {0.25} | 0.2 {0.3} | 0.2 {0.2} | 0.81 |
| Uric acid, mg/dL | 7.1 ± 2.3 | 8.1 ± 2.6 | 6.5 ± 2.1 | <0.01 |
| Albumin, g/dL | 3.6 ± 0.6 | 3.5 ± 0.6 | 3.7 ± 0.5 | 0.03 |
| UAR | 2.03 ± 0.9 | 2.4 ± 0.9 | 1.8 ± 0.7 | <0.01 |
| LVEF,% | 57.6 ± 13.7 | 48.4 ± 11 | 61.7 ± 8.9 | <0.01 |
| LA diameter | 39.7 ± 6.3 | 44.1 ± 5.5 | 37.7 ± 5.6 | <0.01 |
| Left ventricular hypertrophy, n (%) | 18 (10.6) | 7 (13,2) | 11 (9.4) | 0.45 |
| Mild aortic or mitral valve disease, n (%) | 68 (40) | 22 (42) | 46 (39) | 0.80 |
| Duration of procedure, min | 123.9 ± 22.5 | 121.8 ± 26.7 | 124.8 ± 20.3 | 0.41 |
| Peri-ablation therapy | ||||
| Beta blocker/Ca channel blocker, n (%) | 153 (90) | 47 (89) | 106 (90) | 0.86 |
| Amiodarone, n (%) | 47 (27) | 14 (26) | 33 (28) | 0.74 |
| Propafenon, n (%) | 74 (44) | 22 (41) | 52 (44) | 0.69 |
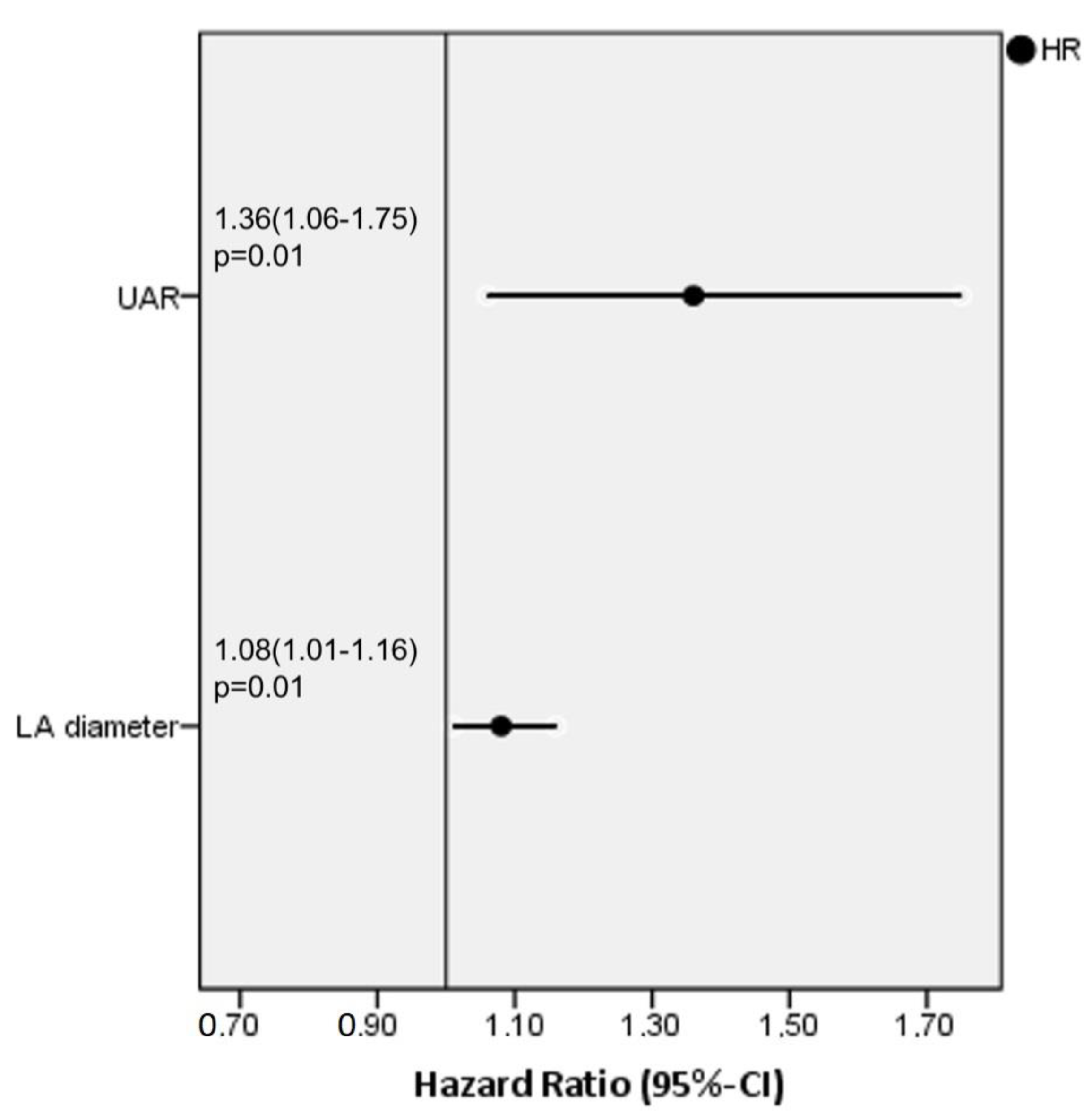
| Unadjusted HR | 95% CI | p Value | Adjusted HR | 95% CI | p Value | |
|---|---|---|---|---|---|---|
| LA diameter | 1.15 | 1.08–1.21 | <0.01 | 1.08 | 1.01–1.16 | 0.01 |
| UAR | 1.59 | 1.25–2.02 | <0.01 | 1.36 | 1.06–1.75 | 0.01 |
| CHA2DS2-VASC score | 1.34 | 1.13–1.59 | <0.01 | 1.02 | 0.83–1.25 | 0.81 |
| AF pattern | 0.29 | 0.16–0.51 | <0.01 | 0.55 | 0.27–1.1 | 0.09 |
| AF duration | 1.01 | 1.01–1.02 | <0.01 | 1.02 | 0.99–1.02 | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karataş, M.B.; Durmuş, G.; Zengin, A.; Gökalp, M.; Hayıroğlu, M.İ.; Çınar, T.; Gürkan, K.; Çam, N. Association of Uric Acid Albumin Ratio with Recurrence of Atrial Fibrillation after Cryoballoon Catheter Ablation. Medicina 2022, 58, 1872. https://doi.org/10.3390/medicina58121872
Karataş MB, Durmuş G, Zengin A, Gökalp M, Hayıroğlu Mİ, Çınar T, Gürkan K, Çam N. Association of Uric Acid Albumin Ratio with Recurrence of Atrial Fibrillation after Cryoballoon Catheter Ablation. Medicina. 2022; 58(12):1872. https://doi.org/10.3390/medicina58121872
Chicago/Turabian StyleKarataş, Mehmet Baran, Gündüz Durmuş, Ahmet Zengin, Murat Gökalp, Mert İlker Hayıroğlu, Tufan Çınar, Kadir Gürkan, and Neşe Çam. 2022. "Association of Uric Acid Albumin Ratio with Recurrence of Atrial Fibrillation after Cryoballoon Catheter Ablation" Medicina 58, no. 12: 1872. https://doi.org/10.3390/medicina58121872
APA StyleKarataş, M. B., Durmuş, G., Zengin, A., Gökalp, M., Hayıroğlu, M. İ., Çınar, T., Gürkan, K., & Çam, N. (2022). Association of Uric Acid Albumin Ratio with Recurrence of Atrial Fibrillation after Cryoballoon Catheter Ablation. Medicina, 58(12), 1872. https://doi.org/10.3390/medicina58121872