

Flap Extension Technique Using Intrasocket Granulation Tissue in Peri-Implant Osseous Defect: Case Series

Abstract
1. Introduction
2. Detailed Case Description
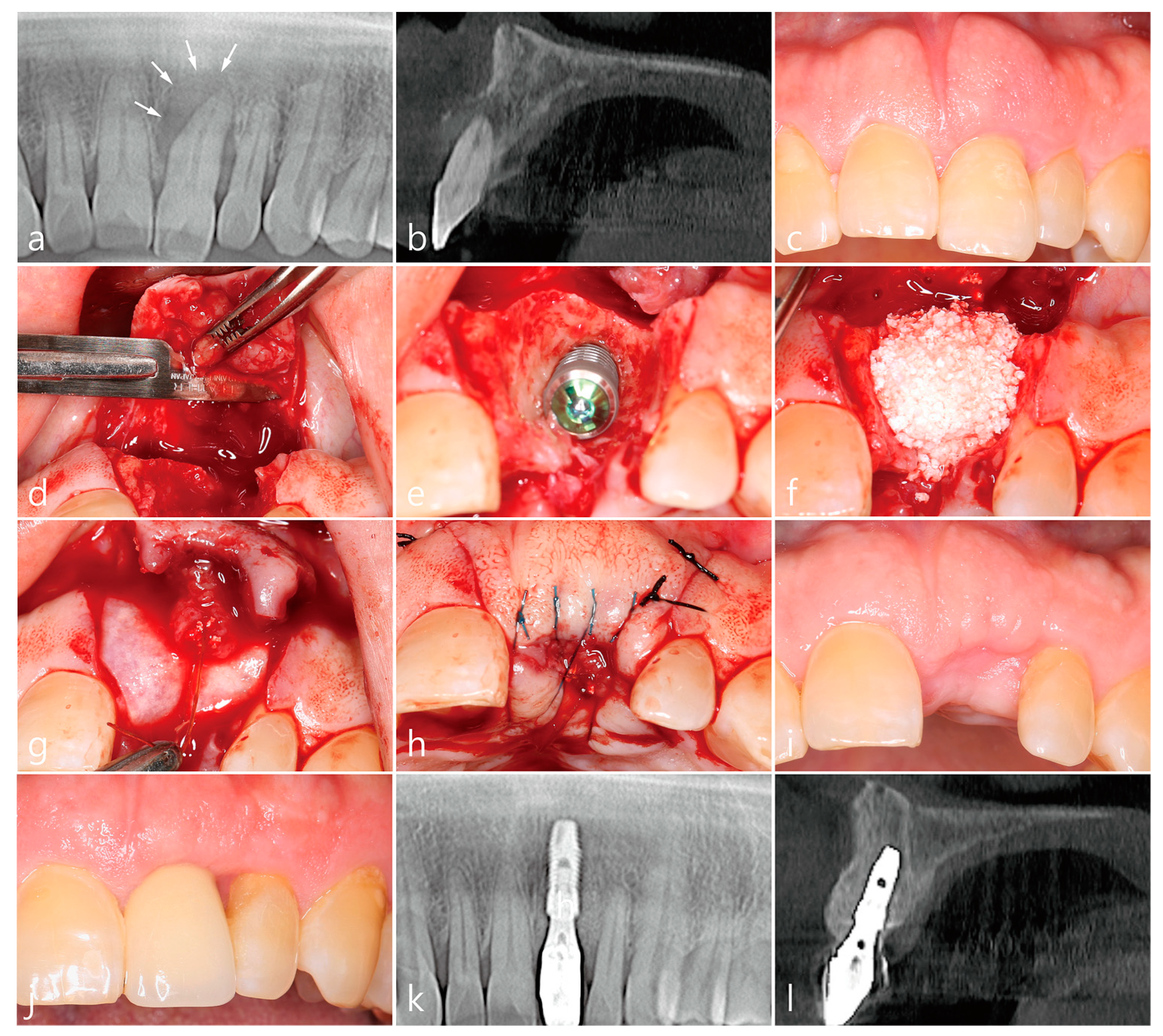
- A tooth or implant with severe bone loss was removed using extraction forceps under local anesthesia with 2% lidocaine containing 1:100,000 epinephrine;
- A midcrestal incision and two buccal vertical incisions were made. Before raising the flap, special care was taken to ensure a clean dissection of the IGT from the underlying flap without any damage and the IGT is still well-attached to the flap. The IGT was then further separated from the bony housing by using a curette with various curvatures and a periosteal elevator.
- The IGT attached to the buccal flap was dissected to an appropriate thickness using a #15 blade so that the base of the IGT was still attached to the existing flap, and the flap was eventually extended. Periosteal releasing incisions were not performed at the flap base.
- The extraction socket was thoroughly debrided using a Molt curette and a titanium brush.
- A surgical guided stent was used so that the implant (Implantium, Dentium, Suwon, Korea) was placed 2.0 mm subcrestal to the level of the adjacent bone in the extraction socket.
- A synthetic osteoconductive bone graft substitute composed of hydroxyapatite (HA) and beta-Tricalcium phosphate (β-TCP) (Osteon III, Genoss, Suwon, Korea) and a resorbable collagen membrane (Genoss, Suwon, Korea) were placed to cover the implant and the peri-implant osseous defect.
- After covering the bone graft with the collagen membrane, the extended IGT was sutured with the palatal flap with 4-0 Catgut. Next, the buccal flap was closed using 4-0 nylon or black silk.
- Antibiotics (Cefradine 500 mg, Yuhan Pharmaceutical Co., LTD. Seoul, Korea) and anti-inflammatory drugs (Etodol® 200 mg, Yuhan Pharmaceutical Co., LTD. Seoul, Korea) were prescribed for 10 days. The patient was recommended to use 0.12% chlorhexidine solution (Hexamedine, Bukwang Pharmaceutical, Seoul, Korea) twice a day for two weeks. Sutures were removed after 10 days.
- Uncovering procedures were performed 4–6 months after initial surgery. Under local anesthesia, the buccal flap was reflected, the regenerated tissue above the implant cover screw was removed, and the healing abutment was connected to the implant. The buccal flap was closed using 4-0 Catgut or black silk. Antibiotics and anti-inflammatory drugs were prescribed for 5 days. The prosthesis was installed 2 months after uncovering.
3. Case 1
4. Case 2
5. Case 3
6. Case 4
7. Case 5
8. Case 6
9. Discussion
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Retzepi, M.; Donos, N. Guided bone regeneration: Biological principle and therapeutic applications. Clin. Oral Implants Res. 2010, 21, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Elgali, I.; Omar, O.; Dahlin, C.; Thomsen, P. Guided bone regeneration: Materials and biological mechanisms revisited. Eur. J. Oral Sci. 2017, 125, 315–337. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Kems, D. Mechanisms of guided bone regeneration: A review. Open Dent. J. 2014, 8, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Darby, I.B.; Adams, G.G.; Reynolds, E.C. A prospective clinical study of bone augmentation techniques at immediate implants. Clin. Oral Implants Res. 2005, 16, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Novaes, A.B., Jr.; Novaes, A.B. Soft tissue management for primary closure in guided bone regeneration: Surgical technique and case report. Int. J. Oral Maxillofac. Implants. 1997, 12, 84–87. [Google Scholar]
- Kim, J.J.; Amara, H.B.; Schwarz, F.; Kim, H.Y.; Lee, J.W.; Wikesjo, U.M.E.; Koo, K.T. Is ridge preservation/augmentation at periodontally compromised extraction sockets safe? A retrospective study. J. Clin. Periodontol. 2017, 44, 1051–1058. [Google Scholar] [CrossRef]
- Mardinger, O.; Chaushu, G.; Ghelfan, O.; Nissan, J.; Mardinger, O. Intrasocket reactive soft tissue for primary closure after augmentation of extraction sites with severe bone loss before implant placement. J. Oral Maxillofac. Surg. 2009, 67, 1294–1299. [Google Scholar] [CrossRef]
- Mardinger, O.; Vered, M.; Chaushu, G.; Nissan, J. Histomorphometrical analysis following augmentation of infected extraction sites exhibiting severe bone loss and primarily closed by intrasocket reactive soft tissue. Clin. Implant Dent. Relat. Res. 2012, 14, 359–365. [Google Scholar] [CrossRef]
- Hur, Y.S.; Lim, H.C.; Herr, Y. Utilizing chronic intrasocket granulation tissue for ridge preservation: A novel approach. J. Oral Implantol. 2020, 46, 438–445. [Google Scholar] [CrossRef]
- An, X.; Jeong, S.M.; Choi, B.H. Natural Bone Healing In Compromised Sockets After Tooth Extraction: Digital Measurement Methods With Cone-Beam Computed Tomography. J. Oral Implantol. 2021, 47, 236–241. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implants Res. 2012, 23 (Suppl. S5), 1–21. [Google Scholar] [CrossRef] [PubMed]
- Fugazzotto, P.A. Maintaining primary closure after guided bone regeneration procedures: Introduction of a new flap design and preliminary results. J. Periodontol. 2006, 77, 1452–1457. [Google Scholar] [CrossRef] [PubMed]
- Machtei, E.E. The effect of membrane exposure on the outcome of regenerative procedures in humans: A meta-analysis. J. Periodontol. 2001, 72, 512–516. [Google Scholar] [CrossRef]
- Engler-Hamm, D.; Cheung, W.S.; Yen, A.; Stark, P.C.; Griffin, T. Ridge preservation using a composite bone graft and a bioabsorbable membrane with and without primary wound closure: A comparative clinical trial. J. Periodontol. 2011, 82, 377–387. [Google Scholar] [CrossRef]
- Cardaropoli, D.; Tamagnone, L.; Roffredo, A.; Gaveglio, L.; Cardaropoli, G. Socket preservation using bovine bone mineral and collagen membrane: A randomized controlled clinical trial with histologic analysis. Int. J. Periodontics Restorative Dent. 2012, 32, 421–430. [Google Scholar] [PubMed]
- Sun, D.J.; Lim, H.C.; Lee, D.W. Alveolar ridge preservation using an open membrane approach for sockets with bone deficiency: A randomized controlled clinical trial. Clin. Implant Dent. Relat. Res. 2019, 21, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Ronda, M.; Rebaudi, A.; Torelli, L.; Stacchi, C. Expanded vs. dense polytetrafluoroethylene membranes in vertical ridge augmentation around dental implants: A prospective randomized controlled clinical trial. Clin. Oral Implants Res. 2014, 25, 859–866. [Google Scholar] [CrossRef]
- Kim, D.M.; Angelis, N.D.; Camelo, M.; Nevins, M.L.; Schupbach, P.; Nevins, M. Ridge preservation with and without primary wound closure: A case series. Int. J. Periodontics Restorative Dent. 2013, 33, 71–78. [Google Scholar] [CrossRef]
- Eskan, M.A.; Girouard, M.E.; Morton, D.; Greenwell, H. The effect of membrane exposure on lateral ridge augmentation: A case-controlled study. Int. J. Implant Dent. 2017, 3, 26. [Google Scholar] [CrossRef]
- Garcia, J.; Dodge, A.; Luepke, P.; Wang, H.L.; Kapila, K.; Lin, G.H. Effect of membrane exposure on guided bone regeneration: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, 328–338. [Google Scholar] [CrossRef]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of collagen membranes for bone regeneration: A literature review. Materials 2020, 9, 786. [Google Scholar] [CrossRef] [PubMed]
- Khoury, F.; Happe, A. The palatal subepithelial connective tissue flap method for soft tissue management to cover maxillary defects: A clinical report. Int. J. Oral Maxillofac. Implants. 2000, 15, 415–418. [Google Scholar] [PubMed]
- Greenstein, G.; Greenstein, B.; Cavallaro, J.; Elian, N.; Tarnow, D. Flap advancement: Practical techniques to attain tension-free primary closure. J. Periodontol. 2009, 80, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Hur, Y.; Tsukiyama, T.; Yoon, T.H.; Griffin, T. Double flap incision design for guided bone regeneration: A novel technique and clinical considerations. J. Periodontol. 2010, 81, 945–952. [Google Scholar] [CrossRef]
- Park, J.C.; Kim, C.S.; Choi, S.C.; Cho, K.S.; Chai, J.K.; Jung, U.W. Flap extension attained by vertical and periosteal-releasing incisions: A prospective cohort study. Clin. Oral Implants Res. 2012, 23, 993–998. [Google Scholar] [CrossRef]
- Romanos, G.E. Periosteal releasing incision for successful coverage of augmented sites. A technical note. J. Oral Implantol. 2010, 36, 25–30. [Google Scholar] [CrossRef]
- Ogata, Y.; Griffin, T.J.; Ko, A.C.; Hur, Y. Comparison of double-flap incision to periosteal releasing incision for flap advancement: A prospective clinical trial. Int. J. Oral Maxillofac. Implants. 2013, 28, 597–604. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age/Sex | Smoking | Compromised Socket Site | Implant Size | Follow-Up Period (Months) |
|---|---|---|---|---|---|
| 1 | 52/M | No | #21 | 3.8 × 12 | 12 |
| 2 | 53/F | No | #23 | 3.8 × 10 | 29 |
| 3 | 72/M | Yes | #13 | 3.8 × 12 | 35 |
| 4 | 76/F | No | #13 | 3.8 × 12 | 28 |
| 5 | 54/M | Yes | #36 | 4.3 × 10 | 19 |
| 6 | 72/F | No | #35/#36 | 4.3 × 10 | 26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, W.-B.; Ko, J.-M.; Han, J.-Y.; Kang, P. Flap Extension Technique Using Intrasocket Granulation Tissue in Peri-Implant Osseous Defect: Case Series. Medicina 2022, 58, 1555. https://doi.org/10.3390/medicina58111555
Park W-B, Ko J-M, Han J-Y, Kang P. Flap Extension Technique Using Intrasocket Granulation Tissue in Peri-Implant Osseous Defect: Case Series. Medicina. 2022; 58(11):1555. https://doi.org/10.3390/medicina58111555
Chicago/Turabian StylePark, Won-Bae, Jung-Min Ko, Ji-Young Han, and Philip Kang. 2022. "Flap Extension Technique Using Intrasocket Granulation Tissue in Peri-Implant Osseous Defect: Case Series" Medicina 58, no. 11: 1555. https://doi.org/10.3390/medicina58111555
APA StylePark, W.-B., Ko, J.-M., Han, J.-Y., & Kang, P. (2022). Flap Extension Technique Using Intrasocket Granulation Tissue in Peri-Implant Osseous Defect: Case Series. Medicina, 58(11), 1555. https://doi.org/10.3390/medicina58111555