
Central versus Peripheral CTEPH—Clinical and Hemodynamic Specifications

Abstract
1. Introduction
2. Aim of the Study
3. Patients and Methods
- The functional status of the patients defined by functional class (FC-WHO), 6-min walk test (6MWT), and laboratory heart failure assessment with N-terminal pro-brain natriuretic peptide (NTproBNP);
- The echocardiographic parameters acquired by transthoracic echocardiography (TTE): the severity of PAH estimated by the tricuspid regurgitation peak gradient (TR PG) and the left ventricular eccentricity index (LV IE), right-ventricular (RV) dilatation by long-axis diastolic diameter (RVd) measurement, and RV function by the assessment of tricuspid annular plane systolic excursion (TAPSE) and fractional area change (FAC);
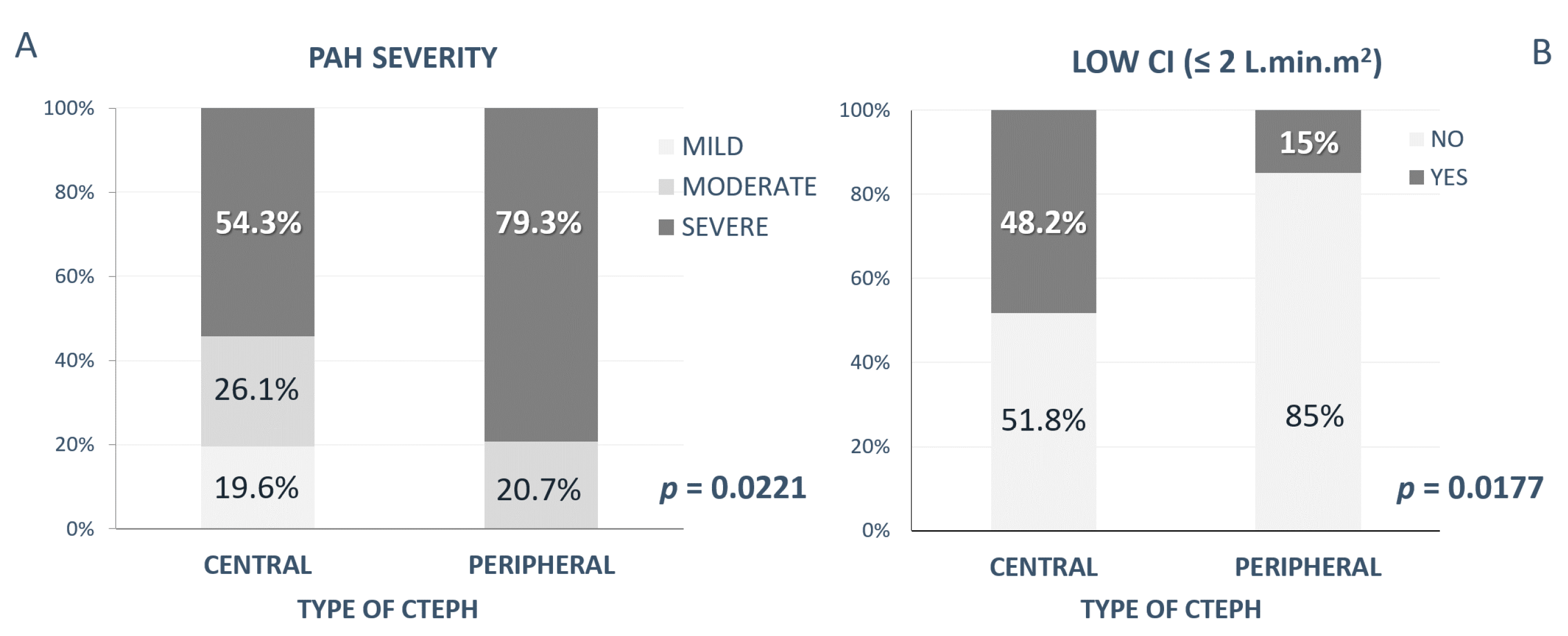
- Invasive hemodynamic parameters obtained by right heart catheterization: mPAP, transpulmonary gradient (TPG), cardiac index (CI), and pulmonary vascular resistance (PVR). The severity of PAH according to the mean pulmonary artery pressure (mPAP) was defined as mild (mPAP < 35 mmHg), moderate (mPAP 35–45 mmHg), and severe (mPAP > 45 mmHg);
- The presence of risk factors—acute pulmonary embolism (APE); deep venous thrombosis; congenital thrombophilia; blood type other than “0”; surgery and/or immobilization; thyreopathy; and other autoimmune diseases, such as Crohn disease or ulcerous colitis, pacemaker implantation, splenectomy and a history of malignity was obtained from patients´ medical history.
Statistical Analysis
4. Results
4.1. Functional Status
4.2. Echocardiographic Parameters
4.3. Hemodynamic Parameters
4.4. Risk Factors
5. Discussion
6. Study Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Galiè, N.; Humbert, M.; Vachiery, J.; Gibbs, S.; Lang, I.; Torbicki, A.; Simmonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [CrossRef]
- Delcroix, M.; Torbicki, A.; Gopalan, D.; Sitbon, O.; Klok, F.A.; Lang, I.; Jenkins, D.; Kim, N.H.; Humbert, M.; Jais, X.; et al. ERS statement on chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2020, 57, 2002828. [Google Scholar] [CrossRef]
- Kim, N.H.; Delcroix, M.; Jais, X.; Madani, M.M.; Matsubara, H.; Mayer, E.; Ogo, T.; Tapson, V.F.; Ghofrani, H.-A.; Jenkins, D.P. Chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801915. [Google Scholar] [CrossRef] [PubMed]
- Lang, I.M.; Campean, I.A.; Sadushi-Kolici, R.; Badr-Eslam, R.; Gerges, C.; Skoro-Sajer, N. Chronic Thromboembolic Disease and Chronic Thromboembolic Pulmonary Hypertension. Clin. Chest Med. 2021, 42, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Šimková, I. CTEPH: Patophysiology, clinical picture, diagnosis. In Pulmonary Hypertension by the Eye of a Cardiologist; Slovak Academic Press: Bratislava, Slovakia, 2009; pp. 199–215. [Google Scholar]
- Lang, I. Chronic thromboembolic pulmonary hypertension: A distinct disease entity. Eur. Respir. Rev. 2015, 24, 246–252. [Google Scholar] [CrossRef]
- Simonneau, G.; Torbicki, A.; Dorfmüller, P.; Kim, N. The pathophysiology of chronic thromboembolic pulmonary hypertension. Eur. Respir. Rev. 2017, 26, 160112. [Google Scholar] [CrossRef]
- Simonneau, G.; Dorfmüller, P.; Guignabert, C.; Mercier, O.; Humbert, M. Chronic thromboembolic pulmonary hypertension: The magic of pathophysiology. Ann. Cardiothorac. Surg. 2022, 11, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Lang, I.M.; Pesavento, R.; Bonderman, D.; Yuan, J.X.-J. Risk factors and basic mechanisms of chronic thromboembolic pulmonary hypertension: A current understanding. Eur. Respir. J. 2012, 41, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Delcroix, M.; Kerr, K.; Fedullo, P. Chronic Thromboembolic Pulmonary Hypertension. Epidemiology and Risk Factors. Ann. Am. Thorac. Soc. 2016, 13, S201–S206. [Google Scholar] [CrossRef] [PubMed]
- Jansa, P.; Ambrož, D.; Kuhn, M.; Dytrych, V.; Aschermann, M.; Černý, V.; Gressin, V.; Heller, S.; Kunstýř, J.; Širanec, M.; et al. Epidemiology of chronic thromboembolic pulmonary hypertension (CTEPH) in the Czech Republic. Pulm. Circ. 2022, 12, e12038. [Google Scholar] [CrossRef] [PubMed]
- Ciurzyński, M.; Kurzyna, M.; Kopeć, G.; Błaszczak, P.; Chrzanowski, Ł.; Kamiński, K.; Mizia-Stec, K.; Mularek-Kubzdela, T.; Biederman, A.; Zieliński, D.; et al. An expert opinion of the Polish Cardiac Society Working Group on Pulmonary Circulation on screening for chronic thromboembolic pulmonary hypertension patients after acute pulmonary embolism: Update. Kardiol. Polska 2022, 80, 723–732. [Google Scholar] [CrossRef] [PubMed]
- E Cannon, J.; Jenkins, D.P.; Hoole, S.P. Chronic thromboembolic pulmonary hypertension: A review of risk factors, management and current challenges. Expert Rev. Cardiovasc. Ther. 2022, 20, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Dorfmüller, P.; Günther, S.; Ghigna, M.-R.; De Montpréville, V.T.; Boulate, D.; Paul, J.-F.; Jais, X.; Decante, B.; Simonneau, G.; Dartevelle, P.; et al. Microvascular disease in chronic thromboembolic pulmonary hypertension: A role for pulmonary veins and systemic vasculature. Eur. Respir. J. 2014, 44, 1275–1288. [Google Scholar] [CrossRef]
- Quarck, R.; Wynants, M.; Verbeken, E.; Meyns, B.; Delcroix, M. Contribution of inflammation and impaired angiogenesis to the pathobiology of chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2015, 46, 431–443. [Google Scholar] [CrossRef] [PubMed]
- Remková, A.; Šimková, I.; Valkovičová, T. Platelet abnormalities in chronic thromboembolic pulmonary hypertension. Int. J. Clin. Exp. Med. 2015, 8, 9700–9707. [Google Scholar]
- Colebank, M.J.; Qureshi, M.U.; Rajagopal, S.; Krasuski, R.A.; Olufsen, M.S. A multiscale model of vascular function in chronic thromboembolic pulmonary hypertension. Am. J. Physiol. Circ. Physiol. 2021, 321, H318–H338. [Google Scholar] [CrossRef] [PubMed]
- D’Armini, A.M. Diagnostic advances and opportunities in chronic thromboembolic pulmonary hypertension. Eur. Respir. Rev. 2015, 24, 253–262. [Google Scholar] [CrossRef]
- Delcroix, M.; Lang, I.; Pepke-Zaba, J.; Jansa, P.; D’Armini, A.M.; Snijder, R.; Bresser, P.; Torbicki, A.; Mellemkjaer, S.; Lewczuk, J.; et al. Long-Term Outcome of Patients with Chronic Thromboembolic Pulmonary Hypertension:Results From an International Prospective Registry. Circulation 2016, 133, 859–871. [Google Scholar] [CrossRef]
- Kopeć, G.; Dzikowska-Diduch, O.; Mroczek, E.; Mularek-Kubzdela, T.; Chrzanowski, Ł.; Skoczylas, I.; Tomaszewski, M.; Peregud-Pogorzelska, M.; Karasek, D.; Lewicka, E.; et al. Characteristics and outcomes of patients with chronic thromboembolic pulmonary hypertension in the era of modern therapeutic approaches: Data from the Polish multicenter registry (BNP-PL). Ther. Adv. Chronic. Dis. 2021, 12, 204062232110029. [Google Scholar] [CrossRef]
- Ruaro, B.; Confalonieri, P.; Caforio, G.; Baratella, E.; Pozzan, R.; Tavano, S.; Bozzi, C.; Lerda, S.; Geri, P.; Biolo, M.; et al. Chronic Thromboembolic Pulmonary Hypertension: An Observational Study. Medicina 2022, 58, 1094. [Google Scholar] [CrossRef]
- Mahmud, E.; Madani, M.M.; Kim, N.H.; Poch, D.; Ang, L.; Behnamfar, O.; Patel, M.P.; Auger, W.R. Chronic Thromboembolic Pulmonary Hypertension. J. Am. Coll. Cardiol. 2018, 71, 2468–2486. [Google Scholar] [CrossRef] [PubMed]
- Verbelen, T.; Godinas, L.; Maleux, G.; Coolen, J.; Claessen, G.; Belge, C.; Meyns, B.; Delcroix, M. Chronic thromboembolic pulmonary hypertension: Diagnosis, operability assessment and patient selection for pulmonary endarterectomy. Ann. Cardiothorac. Surg. 2021, 11, 82–97. [Google Scholar] [CrossRef] [PubMed]
- Lindner, J.; Ambroz, D.; Novotný, R.; Nižňanský, M.; Simkova, I.; Boháčeková, M.; Pecha, O.; Jansa, P. Pulmonary endarterectomy combined with cardiac surgery: A 7-year retrospective analysis. Cor. Vasa 2015, 57, e115–e120. [Google Scholar] [CrossRef]
- Jenkins, D. Pulmonary endarterectomy: The potentially curative treatment for patients with chronic thromboembolic pulmonary hypertension. Eur. Respir. Rev. 2015, 24, 263–271. [Google Scholar] [CrossRef]
- Skoro-Sajer, N.; Marta, G.; Gerges, C.; Hlavin, G.; Nierlich, P.; Taghavi, S.; Sadushi-Kolici, R.; Klepetko, W.; Lang, I.M. Surgical specimens, haemodynamics and long-term outcomes after pulmonary endarterectomy. Thorax 2013, 69, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Lang, I.; Meyer, B.C.; Ogo, T.; Matsubara, H.; Kurzyna, M.; Ghofrani, H.-A.; Mayer, E.; Brenot, P. Balloon pulmonary angioplasty in chronic thromboembolic pulmonary hypertension. Eur. Respir. Rev. 2017, 26, 160119. [Google Scholar] [CrossRef]
- Coghlan, J.G.; Rothman, A.M.; Hoole, S.P. Balloon Pulmonary Angioplasty: State of the Art. Interv. Cardiol. Rev. Res. Resour. 2021, 16, e02. [Google Scholar] [CrossRef]
- Gerges, C.; Friewald, R.; Gerges, M.; Shafran, I.; Sadushi-Koliçi, R.; Skoro-Sajer, N.; Moser, B.; Taghavi, S.; Klepetko, W.; Lang, I.M. Efficacy and Safety of Percutaneous Pulmonary Artery Subtotal Occlusion and Chronic Total Occlusion Intervention in Chronic Thromboembolic Pulmonary Hypertension. Circ. Cardiovasc. Interv. 2021, 14, e010243. [Google Scholar] [CrossRef]
- Butler, O.; Ju, S.; Hoernig, S.; Vogtländer, K.; Bansilal, S.; Heresi, G.A. Assessment for residual disease after pulmonary endarterectomy in patients with chronic thromboembolic pulmonary hypertension. ERJ Open Res. 2022, 8, 00572–02021. [Google Scholar] [CrossRef]
- Ghofrani, H.-A.; D’Armini, A.M.; Grimminger, F.; Hoeper, M.M.; Jansa, P.; Kim, N.H.; Mayer, E.; Simonneau, G.; Wilkins, M.R.; Fritsch, A.; et al. Riociguat for the Treatment of Chronic Thromboembolic Pulmonary Hypertension. N. Engl. J. Med. 2013, 369, 319–329. [Google Scholar] [CrossRef]
- Hoeper, M.M. Pharmacological therapy for patients with chronic thromboembolic pulmonary hypertension. Eur. Respir. Rev. 2015, 24, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Sadushi-Kolici, R.; Jansa, P.; Kopeć, G.; Torbicki, A.; Skoro-Sajer, N.; Campean, I.-A.; Halank, M.; Simkova, I.; Karlocai, K.; Steringer-Mascherbauer, R.; et al. Subcutaneous treprostinil for the treatment of severe non-operable chronic thromboembolic pulmonary hypertension (CTREPH): A double-blind, phase 3, randomised controlled trial. Lancet Respir. Med. 2018, 7, 239–248. [Google Scholar] [CrossRef]
- Ghofrani, H.-A.; D’Armini, A.M.; Kim, N.H.; Mayer, E.; Simonneau, G. Interventional and pharmacological management of chronic thromboembolic pulmonary hypertension. Respir. Med. 2021, 177, 106293. [Google Scholar] [CrossRef] [PubMed]
- Pepke-Zaba, J.; Delcroix, M.; Lang, I.; Mayer, E.; Jansa, P.; Ambroz, D.; Treacy, C.; Monforte, A.D.; Morsolini, M.; Snijder, R.; et al. Chronic thromboembolic pulmonary hypertension (CTEPH): Results from an international prospective registry. Circulation 2011, 124, 1973–1981. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Okada, O.; Sakuma, M.; Nakanishi, N.; Miyahara, Y.; Yamada, N.; Fujioka, H.; Kuriyama, T.; Kunieda, T.; Sugimoto, T.; et al. Incidence and Clinical Characteristics of Chronic Pulmonary Thromboembolism in Japan Compared with Acute Pulmonary Thromboembolism. Circ. J. 2002, 66, 257–260. [Google Scholar] [CrossRef]
- Chausheva, S.; Naito, A.; Ogawa, A.; Seidl, V.; Winter, M.-P.; Sharma, S.; Sadushi-Kolici, R.; Campean, I.-A.; Taghavi, S.; Moser, B.; et al. Chronic thromboembolic pulmonary hypertension in Austria and Japan. J. Thorac. Cardiovasc. Surg. 2019, 158, 604–614. [Google Scholar] [CrossRef] [PubMed]
- Bohacekova, M.; Kaldararova, M.; Valkovicova, T.; Remkova, A.; Vesely, J.; Simkova, I. Risk factors detection in chronic thromboembolic pulmonary hypertension, a tool for risk quantification? Bratisl. Med. J. 2017, 117, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Gerges, C.; Skoro-Sajer, N.; Lang, I.M. Right Ventricle in Acute and Chronic Pulmonary Embolism (2013 Grover Conference Series). Pulm. Circ. 2014, 4, 378–386. [Google Scholar] [CrossRef]
- Tello, K.; Dalmer, A.; Axmann, J.; Vanderpool, R.; Ghofrani, H.A.; Naeije, R.; Roller, F.; Seeger, W.; Sommer, N.; Wilhelm, J.; et al. Reserve of Right Ventricular-Arterial Coupling in the Setting of Chronic Overload. Circ. Heart Fail. 2019, 12, e005512. [Google Scholar] [CrossRef] [PubMed]
- Greyson, C.R. Pathophysiology of right ventricular failure. Crit. Care Med. 2008, 36, S57–S65. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.E. The remarkable right ventricle of patients with Eisenmenger syndrome. Coron. Artery Dis. 2005, 16, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Valkovicova, T.; Kaldararova, M.; Reptova, A.; Bohacekova, M.; Bacharova, L.; Hatala, R.; Simkova, I. Eisenmenger syndrome —An electrocardiographic and echocardiographic assessment of the right ventricle. Bratisl. Med. J. 2018, 119, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Diller, G.-P.; Dimopoulos, K.; Kafka, H.; Ho, S.Y.; Gatzoulis, M.A. Model of chronic adaptation: Right ventricular function in Eisenmenger syndrome. Eur. Heart J. Suppl. 2007, 9, H54–H60. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Gr. 1 (CENTRAL) (n = 51) | Gr. 2 (PERIPHERAL) (n = 30) | p Value | |
|---|---|---|---|
| General characteristics | |||
| Age (years) | 59 (25–85) | 64 (26–75) | 0.2 |
| Male gender (%) | 72.5 | 46.7 | 0.0198 |
| Functional status | |||
| FC-WHO—II/III/IV (% of patients) | 34/60/6 | 26.7/70/3.3 | 0.64 |
| 6MWT (m) | 407 (100–650) | 388 (120–519) | 0.28 |
| NTproBNP (ng/L) | 1320 (79.2–8388) | 2335 (71.6–8155) | 0.1 |
| Echocardiographic parameters | |||
| RVd (mm) | 42 (29–58) | 40 (32–56) | 0.44 |
| TR PG (mmHg) | 77.5 (33–126) | 85 (55–180) | 0.07 |
| FAC (%) | 40 (23–65) | 42 (29–68) | 0.8443 |
| TAPSE (mm) | 18 (9–30) | 19 (7–29) | 0.8829 |
| Invasive hemodynamic parameters | |||
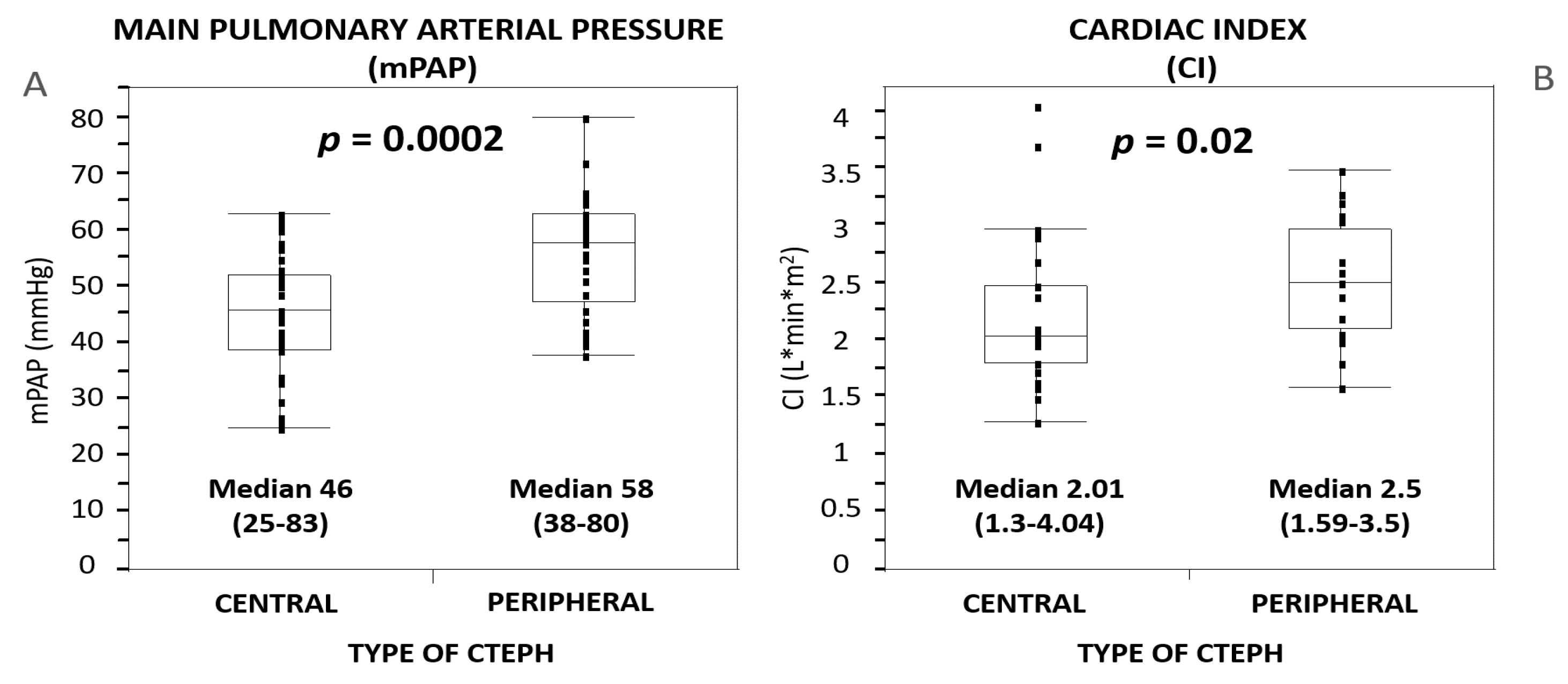
| mPAP (mmHg) | 46 (25–83) | 58 (38–80) | 0.0002 |
| TPG (mmHg) | 34 (5–61) | 47 (14–62) | 0.0005 |
| CI (L·min·m2) | 2.04 (1.3–4.04) | 2.5 (1.59–3.5) | 0.02 |
| PVR (W.U.) | 9 (1.23–22.2) | 10 (3.31–20.5) | 0.0621 |
| Risk Factors (n = 81)—in % | |||
|---|---|---|---|
| Gr. 1 (Central) (n = 51) | Gr. 2 (Peripheral) (n = 30) | p Value | |
| Acute PE | 93.8 | 60 | 0.0002 |
| Recurrent acute PE | 31.3 | 26.7 | 0.66 |
| Deep venous thrombosis | 66.7 | 55.2 | 0.31 |
| Thrombolytic therapy | 10.4 | 10 | 0.9529 |
| Congenital thrombophilia | 37 | 34.8 | 0.86 |
| Blood type other than “0” | 88.4 | 71.4 | 0.07 |
| History of surgery and/or immobilization | 64 | 69 | 0.65 |
| Thyreopathy | 16 | 26.7 | 0.25 |
| Other autoimmune disease (Crohn disease, ulcerous colitis, …) | 10 | 6.7 | 0.61 |
| Splenectomy | 2 | 3.33 | 0.71 |
| Pacemaker implantation | 4% | 0 | 0.27 |
| Malignancy | 2% | 13.3% | 0.0426 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaldararova, M.; Simkova, I.; Bohacekova, M.; Reptova, A.; Hlavata, T.; Pacak, J.; Lindner, J.; Jansa, P. Central versus Peripheral CTEPH—Clinical and Hemodynamic Specifications. Medicina 2022, 58, 1538. https://doi.org/10.3390/medicina58111538
Kaldararova M, Simkova I, Bohacekova M, Reptova A, Hlavata T, Pacak J, Lindner J, Jansa P. Central versus Peripheral CTEPH—Clinical and Hemodynamic Specifications. Medicina. 2022; 58(11):1538. https://doi.org/10.3390/medicina58111538
Chicago/Turabian StyleKaldararova, Monika, Iveta Simkova, Marcela Bohacekova, Adriana Reptova, Tereza Hlavata, Jozef Pacak, Jaroslav Lindner, and Pavel Jansa. 2022. "Central versus Peripheral CTEPH—Clinical and Hemodynamic Specifications" Medicina 58, no. 11: 1538. https://doi.org/10.3390/medicina58111538
APA StyleKaldararova, M., Simkova, I., Bohacekova, M., Reptova, A., Hlavata, T., Pacak, J., Lindner, J., & Jansa, P. (2022). Central versus Peripheral CTEPH—Clinical and Hemodynamic Specifications. Medicina, 58(11), 1538. https://doi.org/10.3390/medicina58111538