
A Psychoanalytic-Derived Brief Psychotherapeutic Approach in the Treatment of Major Depression: Monotherapy Studies

 ,
, 
Abstract
:1. Introduction
1.1. Short-Term Psychodynamic Psychotherapy (STPP): Origins and Theoretical Foundation
- changes in the patient (better understanding of symptoms and conflicts, internalization of the alliance and ability to consciously manage the problem);
- modalities of change in the patient (active engagement, elaboration of relevant problems, ability to establish a therapeutic alliance);
- means used by the therapist (facilitation of expression, comprehension and reworking, ability to provide useful elements to integrate the patient’s information).
1.2. STPP in the Treatment of Major Depressive Disorder (MDD)
- decreasing intensity of symptoms through expression of suppressed negative feelings;
- modulation of Super-Egoic standards of perfection, in order to reduce feelings of inappropriateness and guilt and to strengthen self-esteem;
- increasing awareness on the patient’s current interpersonal relationships [32].
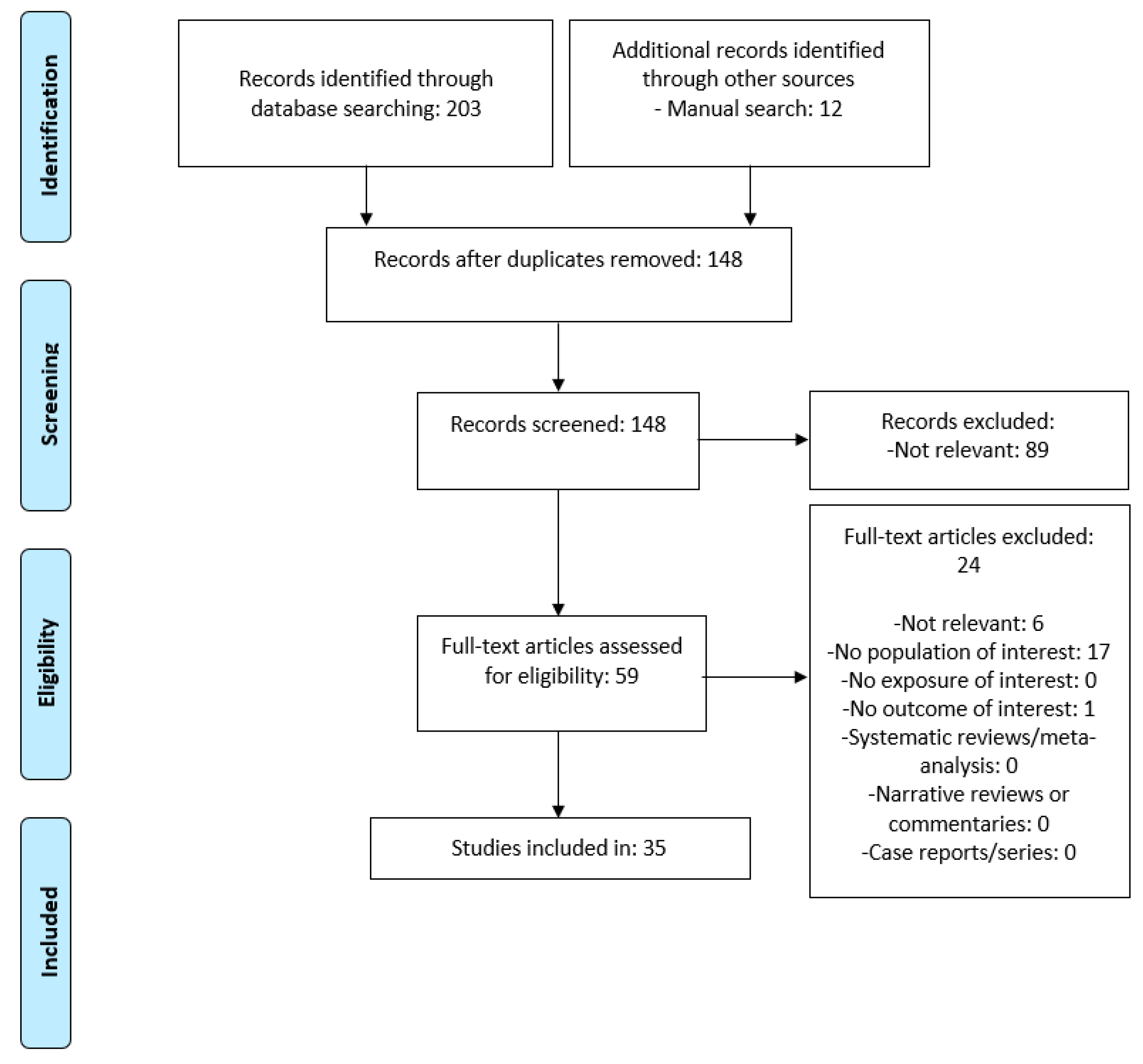
2. Methods
3. Results
- (1)
- STPP efficacy in MDD, compared with other treatment strategies, is more apparent at long-term follow-up rather than in the immediate post-treatment period.
- (2)
- STPP may be more effective in moderate than in mild depression.
- (3)
- In case of depression with concomitant psychiatric comorbidities, the efficacy of STPP must be evaluated on a case-by-case basis.
- (4)
- STPP is effective in preventing MDD recurrences.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sripada, B. Toward a re-appraisal of the relationship between psychoanalysis and dynamic psychotherapy. Psychodyn. Psychiatry 2015, 43, 396–422. [Google Scholar] [CrossRef] [PubMed]
- Gabbard, G.O. Psychodynamic Psychiatry in Clinical Practice; American Psychiatric Publishing: Washington, DC, USA, 2014. [Google Scholar]
- Baée, J.; Jeyasingam, N. Short-term psychodynamic psychotherapy: A brief history. Aust. Psychiatry 2019, 27, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Ferenczi, S.; Rank, O. Entwicklungsziele der Psychoanalys. Zur Wechselbeziehung von Thorie und Praxis, Italian Translation: Prospettive di Sviluppo della Psicoanalisi. Sull’interdipendenza tra Teoria e Pratica. In Opere; Cortina: Milano, Italy, 1924; Volume III. [Google Scholar]
- Alexander, F.; French, T. Psychoanalytic Therapy: Principles and Applications; Ronald Press: New York, NY, USA, 1946. [Google Scholar]
- Luborsky, L. Principles of Psychoanalytic Psychotherapy; Basic Books: New York, NY, USA, 1984. [Google Scholar]
- Luborsky, L.; DeRubeis, R. The use of psychotherapy manuals: A small revolution in psychotherapy research style. Clin. Psychol. Rev. 1984, 4, 5–14. [Google Scholar] [CrossRef]
- Messer, S.B. What makes brief psychodynamic therapy time effect. Clin. Psychol. Sci. Pract. 2001, 8, 5–22. [Google Scholar] [CrossRef]
- Strupp, H.H.; Binder, J.L. Psychotherapy in a New Key; Basic Books: New York, NY, USA, 1984. [Google Scholar]
- Pavan, L.; Mangini, E.; Bogetto, F.; Bellino, S.; Banon, D. Psicoterapie brevi. In Trattato Italiano di Psichiatria; Masson: Padova, Italy, 1999. [Google Scholar]
- Sifneos, P.E. Short Term Psychotherapy and Emotional Crisis. Italian translation: Psicoterapia Breve e Crisi Emotiva; Martinelli: Firenze, Italy, 1982. [Google Scholar]
- Davanloo, H. La Psicoterapia Dinamica Breve; Armando: Roma, Italy, 1987. [Google Scholar]
- Barten, H.H. The Coming of Age of the Brief Psychotherapies. In Progress in Community Mental Health; Grune and Stratton: New York, NY, USA, 1969. [Google Scholar]
- Small, L. The Briefer Psychotherapies; Brunner/Mazel: New York, NY, USA, 1979. [Google Scholar]
- Budman, S.H.; Gurman, A.S. The practice of brief therapy. Prof. Psychol. Res. Pract. 1983, 14, 277–292. [Google Scholar] [CrossRef]
- Svartberg, M.; Stiles, T.C. Comparative effects of short-term psychodynamic psychotherapy: A meta-analysis. J. Consult. Clin. Psychol. 1991, 59, 704–714. [Google Scholar] [CrossRef]
- Crits-Christoph, P. The efficacy of brief dynamic psychotherapy: A meta-analysis. Am. J. Psychiatry 1992, 149, 151–158. [Google Scholar] [PubMed]
- Grawe, K.; Donati, R.; Bernauer, F. Psychotherapie im Wandel: Von der Konfession zur Profession Gottingeny; Hogrefe: Berlin, Germany, 1994. [Google Scholar]
- Anderson, E.M.; Lambert, M.J. Short-term dynamically oriented psychotherapy: A review and meta-analysis. Clin. Psychol. Rev. 1995, 15, 503–514. [Google Scholar] [CrossRef]
- Wampold, B.E.; Mondin, G.W.; Moody, M.; Stich, F.; Benson, K.; Ahn, H. Meta-analysis of outcome studies comparing brief psychotherapies: Empirically, “all must have prizes”. Psychol. Bull. 1997, 122, 203–215. [Google Scholar] [CrossRef]
- Grissom, R.J. The magical number. 7+/−2, 2: A meta-analysis of the probability of superior outcome in comparisons involving therapy, placebo, and control. JCCP 1996, 64, 973–982. [Google Scholar] [CrossRef]
- Ogrodniczuck, J.S.; Piper, W.E.; Joyce, A.S.; Mccallum, M. Transference interpretations in short-term dynamic psychotherapies. J. Nerv. Ment. Dis. 1999, 187, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Piper, W.E.; McCallum, M.; Joyce, A.S.; Azim, H.F.; Ogrodniczuk, J.S. Follow up findings for interpretative and supportive forms of psychotherapy and patient personality variables. JCCP 1999, 67, 267–273. [Google Scholar]
- Leichsenring, F.; Rabung, S.; Leibing, E. The efficacy of short-term psychodynamic psychotherapy in specific psychiatric disorders: A meta-analysis. Arch. Gen. Psychiatry 2004, 61, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Steinert, C.; Munder, T.; Rabung, S.; Hoyer, J.; Leichsenring, F. Psychodynamic therapy: As efficacious as other empirically supported tretments? A meta-analysis testing equivalence of outcomes. Am. J. Psychiatry 2017, 174, 943–953. [Google Scholar] [CrossRef] [PubMed]
- Abbass, A.; Lumley, M.A.; Town, J.; Holmes, H.; Luyten, P.; Cooper, A.; Russel, L.; Schubiner, H.; De Meulemeester, C.; Kisely, S. Short-term psychodynamic psychotherapy for functional somatic disorders: A systematic review and meta-analysis of within-treatment effects. J. Psychosom. Res. 2021, 145, 110473. [Google Scholar] [CrossRef] [PubMed]
- Prien, R.F. Somatic Treatment of Unipolar Depressive Disorder. In American Psychiatric Press Review of Psychiatry; American Psychiatric Press: Washington, DC, USA, 1988. [Google Scholar]
- Akil, H.; Gordon, J.; Hen, R.; Javitch, J.; Mayberg, H.; McEwen, B.; Meaney, M.J.; Nestler, E.J. Treatment resistant depression: A multi-scale, systems biology approach. Neurosci. Biobehav. Rev. 2018, 84, 272–288. [Google Scholar] [CrossRef]
- Akiskal, H.S. Diagnosis and classification of affective disorders: New insights from clinical and laboratory approaches. Psychiatry Dev. 1983, 2, 123–160. [Google Scholar]
- Bekhuis, E.; Boschloo, L.; Rosmalen, J.G.M.; de Boer, M.K.; Schoetvers, R.A. The impact of somatic symptoms on the course of major depressive disorder. J. Affect. Disord. 2016, 205, 112–118. [Google Scholar] [CrossRef]
- Lui, P.; Tu, H.; Zhang, A.; Yang, C.; Liu, Z.; Lei, L.; Wu, P.; Sun, N.; Zhang, K. Brain functional alterations in MDD patients with somatic symptoms: A resting-state fMRI study. J. Affect. Disord. 2021, 295, 788–796. [Google Scholar]
- Pavan, L.; Conforti, D. La Psicoterapia della Depressione; Minerva Psichiatrica: Rome, Italy, 1999; Volume 40, pp. 263–269. [Google Scholar]
- Malhi, G.S.; Bassett, D.; Boyce, P.; Bryant, R.; Fitzgerald, P.B.; Fritz, K.; Hopwood, M.; Lyndon, B.; Mulder, R.; Murray, G.; et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust. N. Z. J. Psychiatry 2015, 49, 1087–1206. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Depression in Adults: Treatment and Management. 2022. Available online: www.nice.org.uk/guidance/ng222 (accessed on 1 July 2022).
- Driessen, E.; Dekker, J.J.M.; Peen, J.; Van, H.L.; Maina, G.; Rosso, G.; Rigardetto, S.; Cuniberti, F.; Vitriol, V.G.; Florenzano, R.U.; et al. The efficacy of adding short-term psychodynamic psychotherapy to antidepressants in the treatment of depression: A systematic review and meta-analysis of individual participant data. Clin. Psychol. Rev. 2020, 80, 101886. [Google Scholar] [CrossRef] [PubMed]
- Maina, G.; Rosso, G.; Crespi, C.; Bogetto, F. Combined brief dynamic therapy and pharmacotherapy in the treatment of major depressive disorder: A pilot study. Psychother. Psychosom. 2007, 76, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Maina, G.; Rosso, G.; Bogetto, F. Brief dynamic therapy combined with pharmacotherapy in the treatment of major depressive disorder: Long-term results. J. Affect. Disord. 2009, 114, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Maina, G.; Rosso, G.; Rigardetto, S.; Piat, S.C.; Bogetto, F. No effect of adding brief dynamic therapy to pharmacotherapy in the treatment of obsessive-compulsive disorder with concurrent major depression. Psychother. Psychosom. 2010, 79, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Martini, B.; Rosso, G.; Chiodelli, D.F.; De Cori, D.; Maina, G. Brief dynamic therapy combined with pharmacotherapy in the treatment of panic disorder with concurrent depressive symptoms. Clin. Neuropsychiatr. 2011, 8, 204–211. [Google Scholar]
- Salminen, J.K.; Karlsson, H.; Hietala, J.; Kajander, J.; Aalto, S.; Markkula, J.; Rasi-Hakala, H.; Toikka, T. Short-term psychodynamic psychotherapy and fluoxetine in major depressive disorder: A randomized comparative study. Psychother. Psychosom. 2008, 77, 351–357. [Google Scholar] [CrossRef]
- Rosso, G.; Martini, B.; Maina, G. Brief dynamic therapy and depression severity: A single-blind, randomized study. J. Affect. Disord. 2013, 147, 101–106. [Google Scholar] [CrossRef]
- Maina, G.; Forner, F.; Bogetto, F. Randomized controlled trial comparing brief dynamic and supportive therapy with waiting list condition in minor depressive disorders. Psychother. Psychosom. 2005, 74, 43–50. [Google Scholar] [CrossRef]
- American Psychiatry Association. Practice Guideline for the Treatment of Patients with Major Depressive Disorder; APA: Washington, DC, USA, 2004. [Google Scholar]
- Parikh, S.V.; Quilty, L.C.; Ravitz, P.; Rosenbluth, M.; Pavlova, B.; Grigoriadis, S.; Velyvis, V.; Kennedy, S.H.; Lam, R.W.; MacQueen, G.M.; et al. Canadian network for mood and anxiety treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: Section 2. Psychological treatments. Can. J. Psychiatry 2016, 61, 524–539. [Google Scholar] [CrossRef]
- American Psychological Association. Clinical Practice Guideline for the Treatment of Depression across Three Age Cohorts; APA: Washington, DC, USA, 2019. [Google Scholar]
- Malhi, G.S.; Bell, E.; Bassett, D.; Boyce, P.; Bryant, R.; Hazell, P.; Hopwood, M.; Lyndon, B.; Mulder, R.; Porter, R.; et al. The 2020 Royal Australian and New Zealand College of Psychiatrist clinical practice guidelines for mood disorders. Aust. N. Z. J. Psychiatry 2021, 55, 7–117. [Google Scholar]
- Malan, D. A Study of Brief Psychotherapy; Plenum: New York, NY, USA, 1976. [Google Scholar]
- Piper, W.E.; Francois, L.d.C.; Szkrumelack, N. Patient predictors of process and outcome in short-term individual psychotherapy. J. Nerv. Ment. Dis. 1985, 173, 726–733. [Google Scholar] [CrossRef]
- Piper, W.E.; Hassan, F.A.; McCallum, M.; Joyce, A.S. Patient suitability and outcome in short term individual psychotherapy. J. Consult. Clin. Psychol. 1990, 58, 475–481. [Google Scholar] [CrossRef]
- Hoglend, P.; Sorbye, O.; Sorlie, T.; Fossum, A.; Engelstad, V. Selection criteria for brief dynamic psychotherapy: Reliability, factor structure and long term predictive validity. Psychother. Psychosom. 1992, 57, 67–74. [Google Scholar]
- Barber, J.; Crits-Christoph, P.; Luborsky, L. Effect of therapist adherence and competence on patient outcome in short term psychodynamic therapy. J. Consult. Clin. Psychol. 1996, 64, 619–622. [Google Scholar] [CrossRef]
- Gaston, L.; Thompson, L.; Gallagher, D.; Cournoyer, L.G.; Gahnon, R. Alliance, technique and their interactions in predicting outcome of behavioural, cognitive and brief dynamic psychotherapy. Psychother. Res. 1998, 8, 190–209. [Google Scholar] [CrossRef]
- Lueger, R.; Lutz, W.; Howard, K. The predicted and observed course of psychotherapy for anxiety and mood disorders. J. Nerv. Ment. Dis. 2000, 188, 127–134. [Google Scholar] [CrossRef]
- Shapiro, D.; Rees, A.; Barkham, M.; Hardy, G.; Reynolds, S.; Startup, M. Effects of treatment duration and severity of depression on the maintenance of gains after cognitive-behavioural and psychodynamic-interpersonal psychotherapy. J. Consult. Psychol. 1995, 63, 378–387. [Google Scholar] [CrossRef]
- Hilsenroth, M.; Ackerman, S.; Blagys, M.; Baity, M.R.; Mooney, M.A. Short term psychodynamic psychotherapy for depression: An examination of statistical, clinically significant, and technique-specific change. J. Nerv. Ment. Dis. 2003, 191, 349–375. [Google Scholar] [CrossRef] [PubMed]
- Bressi, C.; Porcellana, M.; Marinaccio, P.M.; Nocito, E.P.; Magri, L. Short-term psychodynamic psychotherapy versus treatment as usual for depressive and anxiety disorders: A randomized clinical trial of efficacy. J. Nerv. Ment. Dis. 2010, 198, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Barber, J.P.; Barrett, M.S.; Gallop, R.; Rynn, M.A.; Rickels, K. Short-term dynamic psychotherapy versus pharmacotherapy for major depressiove disorder: A randomized, placebo-controlled trial. J. Clin. Psychiatry 2012, 73, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Leichsenring, F. Comparative effects of short term psychodynamic psychotherapy and cognitive-behavioural therapy in depression: A meta-analytic approach. Clin. Psychol. Rev. 2001, 21, 401–419. [Google Scholar] [CrossRef]
- Driessen, E.; Van, H.L.; Don, F.J.; Peen, J.; Kool, S.; Westra, D.; Hendriksen, M.; Schoevers, R.A.; Cuijpers, P.; Twisk, J.W.R.; et al. The efficacy of cognitive-behavioral therapy and psychodynamic therapy in the outpatient treatment of major depression: A randomized clinical trial. Am. J. Psychiatry 2013, 170, 1041–1050. [Google Scholar] [CrossRef]
- Driessen, E.; Cuijpiers, P.; de Maat, S.C.M.; Abbass, A.A.; de Jonghe, F.; Dekker, J.J.M. The efficacy of short-term psychodynamic psychotherapy for depression: A meta-analysis. Clin. Psychol. Rev. 2010, 30, 25–36. [Google Scholar] [CrossRef]
- Shedler, J. The efficacy of psychodynamic psychotherapy. Am. Psychol. 2010, 65, 98–109. [Google Scholar] [CrossRef]
- Hoglend, P. Long-term effects of brief dynamic psychotherapy. Psychother. Res. 2003, 13, 271–292. [Google Scholar] [CrossRef] [PubMed]
- Leichsenring, F.; Schauenburg, H. Empirically supported methods of short-term psychodynamic therapy in depression—Towards an evidence based unified protocol. J. Affect. Disord. 2014, 169, 128–143. [Google Scholar] [CrossRef]
- Abbass, A.; Town, J.; Driesen, E. The efficacy of short-term psychodynamic psychotherapy for depressive disorders with comorbid personality disorder. Psychiatry 2011, 74, 58–71. [Google Scholar] [CrossRef]
- Driessen, E.; Smits, N.; Dekker, J.J.M.; Peen, J.; Don, F.J.; Kool, S.; Westra, D.; Hendriksen, M.; Cuijpers, P.; Van, H.L. Differential efficacy of cognitive behavioral therapy and psychodynamic therapy for major depression: A study of prescriptive factors. Psychol. Med. 2016, 46, 731–734. [Google Scholar] [CrossRef]
- Cuijpers, P.; Sijbrandij, M.; Koole, S.L.; Andersson, G.; Beekman, A.T.; Iii, C.F.R. The efficacy of psychotherapy and pharmacotherapy in treating depressive and anxiety disorders: A meta-analysis. World Psychiatry 2013, 12, 137–148. [Google Scholar] [CrossRef]
- Cuijpers, P.; Turner, E.H.; Mohr, D.C.; Hofmann, S.G.; Andersson, G.; Berking, M.; Coyne, J. Comparison of psychotherapies for adult depression to pill placebo control groups: A meta-analysis. Psychol. Med. 2013, 44, 685–695. [Google Scholar] [CrossRef]
- Spielmans, G.I.; Berman, M.I.; Usitalo, A.N. Psychotherapy versus second- generation antidepressants in the treatment of depression: A meta-analysis. J. Nerv. Ment. Dis. 2011, 199, 142–149. [Google Scholar] [CrossRef]
- Abbass, A.A.; Hancock, J.T.; Henderson, J.; Kisely, S. Short-term psychodynamic psychotherapy for common mental disorders. Cochrane Database Syst. Rev. 2006, 4, CD004687. [Google Scholar]
- Driessen, E.; Hegelmaier, L.M.; Abbass, A.A.; Barber, J.P.; Dekker, J.J.; Van, H.L.; Jansma, E.P.; Cuijpers, P. The efficacy of short-term psychodynamic psychotherapy for depression: A meta-analysis update. Clin. Psychol. Rev. 2015, 42, 1–15. [Google Scholar] [CrossRef]
- Rosso, G.; Aragno, E.; Cuomo, A.; Fagiolini, A.; Di Salvo, G.; Maina, G. Five-year follow-up of first-episode depression treated with psychodynamic psychotherapy or antidepressants. Psychiatry Res. 2019, 275, 27–30. [Google Scholar] [CrossRef]
- Koppers, D.; Peen, J.; Niekerken, S.; Van, R.; Dekker, J. Prevalence and risk factors for recurrence of depression five years after short term psychodynamic therapy. J. Affect. Disord. 2011, 134, 468–472. [Google Scholar] [CrossRef]

{kind=link}
| Malan | Sifneos | Davanloo | Mann | |
|---|---|---|---|---|
| Selection criteria | Yes | Strict | Yes | Broad |
| Number of meetings | 20–40 | 12–20 | 5–40 | 12 |
| Predetermined endpoint | Yes | No | No | Yes |
| Active therapist | Yes | Very active | Very active | Yes |
| Neutrality | Yes | No | No | No |
| Focus | Yes | Yes | Yes | Yes |
| Transference interpretation | Yes | No | Yes | Yes |
| Targeting defence mechanisms | No | Yes | Yes | No |
| Confrontational approach | No | No | Yes | No |
| Suggestive approach | No | No | No | Yes |
| Pedagogical approach | No | Yes | No | Yes |
| Relaxation techniques | No | No | No | No |
| Pharmacological treatment | No | No | No | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Salvo, G.; Bianco, M.; Teobaldi, E.; Maina, G.; Rosso, G. A Psychoanalytic-Derived Brief Psychotherapeutic Approach in the Treatment of Major Depression: Monotherapy Studies. Medicina 2022, 58, 1335. https://doi.org/10.3390/medicina58101335
Di Salvo G, Bianco M, Teobaldi E, Maina G, Rosso G. A Psychoanalytic-Derived Brief Psychotherapeutic Approach in the Treatment of Major Depression: Monotherapy Studies. Medicina. 2022; 58(10):1335. https://doi.org/10.3390/medicina58101335
Chicago/Turabian StyleDi Salvo, Gabriele, Matteo Bianco, Elena Teobaldi, Giuseppe Maina, and Gianluca Rosso. 2022. "A Psychoanalytic-Derived Brief Psychotherapeutic Approach in the Treatment of Major Depression: Monotherapy Studies" Medicina 58, no. 10: 1335. https://doi.org/10.3390/medicina58101335
APA StyleDi Salvo, G., Bianco, M., Teobaldi, E., Maina, G., & Rosso, G. (2022). A Psychoanalytic-Derived Brief Psychotherapeutic Approach in the Treatment of Major Depression: Monotherapy Studies. Medicina, 58(10), 1335. https://doi.org/10.3390/medicina58101335