
The Use of Targeted Monoclonal Antibodies in the Treatment of ABPA—A Case Series

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Series
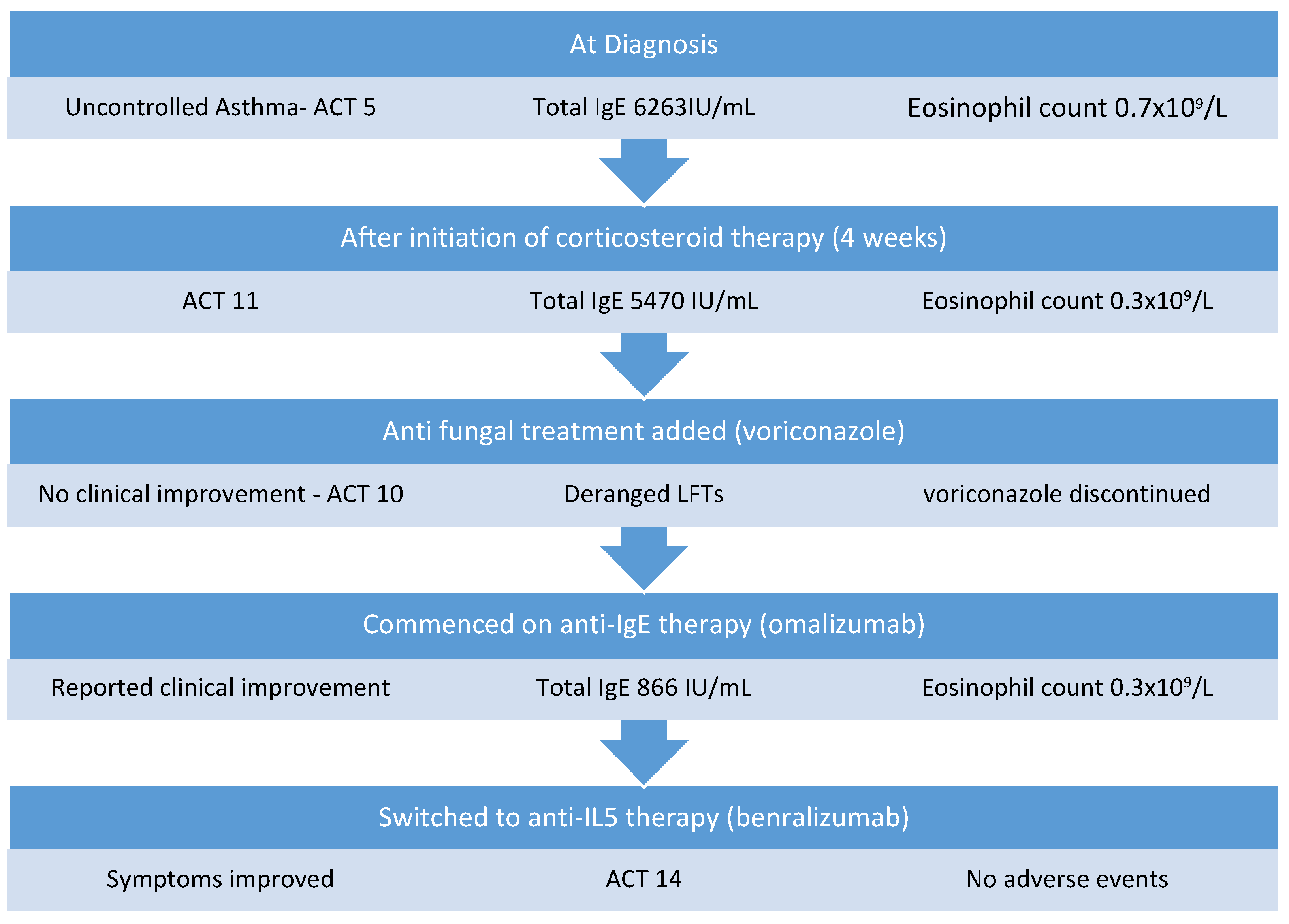
2.1. Case 1
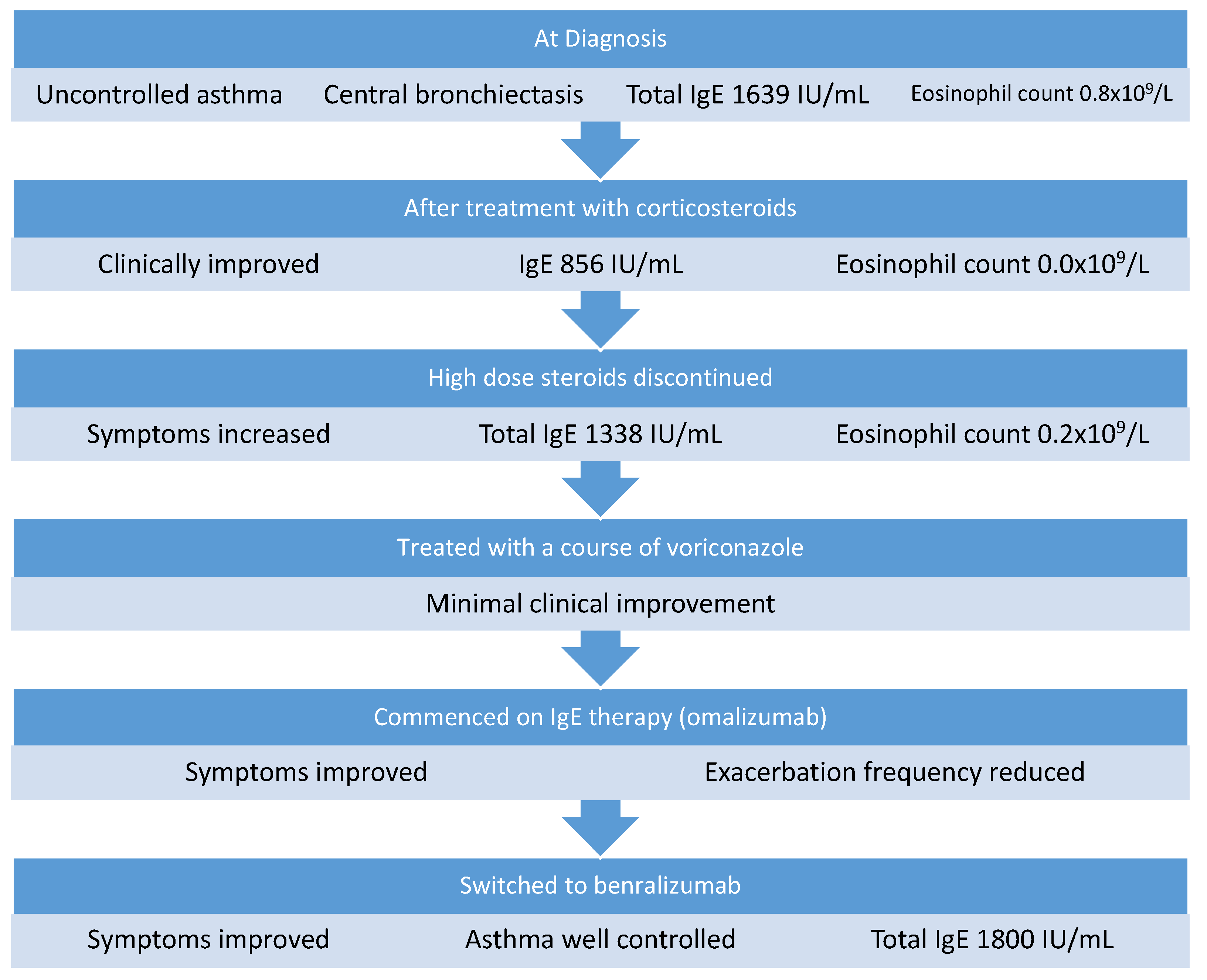
2.2. Case 2
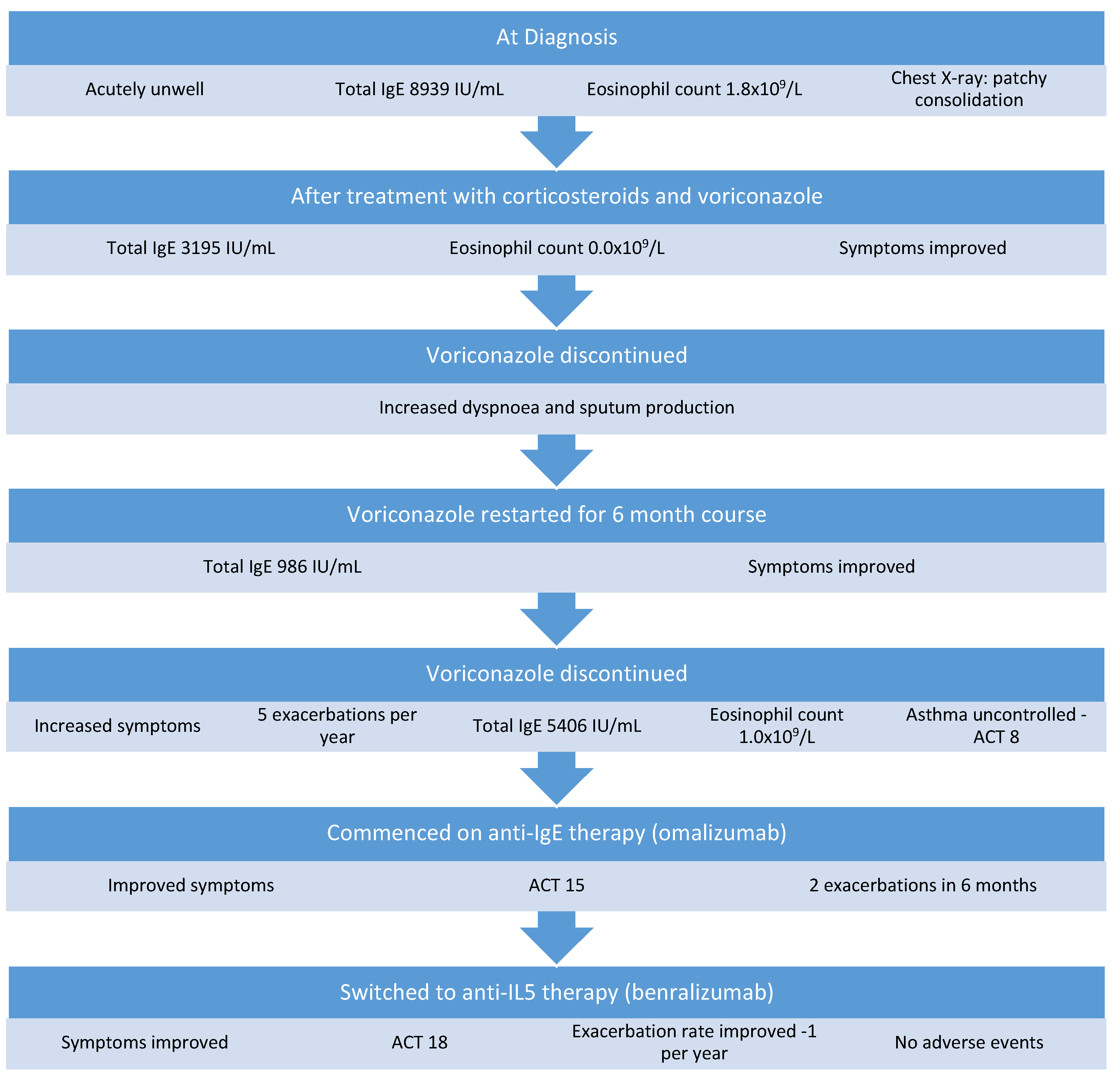
2.3. Case 3
3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Agarwal, R.; Chakrabarti, A.; Shah, A.; Gupta, D.; Meis, J.; Guleria, R.; Moss, R.; Denning, D.; ABPA Complicating Asthma ISHAM Working Group. Allergic bronchopulmonary aspergillosis: Review of literature and proposal of new diagnostic and classification criteria. Clin. Exp. Allergy 2013, 43, 850–873. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Aggarwal, A.N.; Gupta, D.; Jindal, S.K. Aspergillus hypersensitivity and allergic bronchopulmonary aspergillosis in patients with bronchial asthma: Systematic review and meta-analysis. Int. J. Tuberc. Lung Dis. 2009, 13, 936–944. [Google Scholar] [PubMed]
- Agarwal, R.; Aggarwal, A.N.; Dhooria, S.; Sehgal, I.S.; Garg, M.; Saikia, B.; Behera, D.; Chakrabarti, A. A randomised trial of glucocorticoids in acute-stage allergic bronchopulmonary aspergillosis complicating asthma. Eur. Respir. J. 2015, 47, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Dhooria, S.; Sehgal, I.S.; Aggarwal, A.N.; Garg, M.; Saikia, B.; Behera, D.; Chakrabarti, A. A Randomized Trial of Itraconazole vs. Prednisolone in Acute-Stage Allergic Bronchopulmonary Aspergillosis Complicating Asthma. Chest 2018, 153, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Muthu, V.; Sehgal, I.S.; Dhooria, S.; Prasad, K.T.; Garg, M.; Aggarwal, A.N.; Chakrabarti, A. A randomised trial of prednisolone and itraconazole in acute-stage allergic bronchopulmonary aspergillosis complicating asthma. Eur. Respir. J. 2021, 58, 2101787. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Dhooria, S.; Sehgal, I.S.; Aggarwal, A.N.; Garg, M.; Saikia, B.; Chakrabarti, A. A randomised trial of voriconazole and prednisolone monotherapy in acute-stage allergic bronchopulmonary aspergillosis complicating asthma. Eur. Respir. J. 2018, 52, 1801159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.R.; Patel, A.R.; Singh, S.; Singh, S.; Khawaja, I. Treating Allergic Bronchopulmonary Aspergillosis: A Review. Cureus 2019, 11, e4538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benitez, L.L.; Carver, P.L. Adverse Effects Associated with Long-Term Administration of Azole Antifungal Agents. Drugs 2019, 79, 833–853. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.L. Side effects of corticosteroid therapy. J. Clin. Gastroenterol. 2001, 33, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Sehgal, I.S.; Dhooria, S.; Aggarwal, A.N. Developments in the diagnosis and treatment of allergic bronchopulmonary aspergillosis. Expert Rev. Respir. Med. 2016, 10, 1317–1334. [Google Scholar] [CrossRef] [PubMed]
- Eraso, I.C.; SanGiovanni, S.; Morales, E.I.; Fernández-Trujillo, L. Use of monoclonal antibodies for allergic bronchopulmonary aspergillosis in patients with asthma and cystic fibrosis: Literature review. Ther. Adv. Respir. Dis. 2020, 14, 1753466620961648. [Google Scholar] [CrossRef] [PubMed]
- Tracy, M.C.; Okorie, C.U.A.; Foley, E.A.; Moss, R.B. Allergic Bronchopulmonary Aspergillosis. J. Fungi 2016, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- Rathore, V.B.; Johnson, B.; Fink, J.N.; Kelly, K.; Greenberger, P.A.; Kurup, V.P. T Cell Proliferation and Cytokine Secretion to T Cell Epitopes of Asp f 2 in ABPA Patients. Clin. Immunol. 2001, 100, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Kauffman, H.F.; Tomee, J. Inflammatory cells and airway defense against aspergillus fumigatus. Immunol. Allergy Clin. N. Am. 1998, 18, 619–640. [Google Scholar] [CrossRef]
- Stevens, D.A.; Schwartz, H.J.; Lee, J.Y.; Moskovitz, B.L.; Jerome, D.C.; Catanzaro, A.; Bamberger, D.M.; Weinmann, A.J.; Tuazon, C.U.; Judson, M.; et al. A Randomized Trial of Itraconazole in Allergic Bronchopulmonary Aspergillosis. N. Engl. J. Med. 2000, 342, 756–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, R.M.; Haq, Y.; Denning, D.; Stevens, D.A. Adverse events associated with itraconazole in 189 patients on chronic therapy. J. Antimicrob. Chemother. 1990, 26, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Chishimba, L.; Niven, R.M.; Cooley, J.; Denning, D.W. Voriconazole and Posaconazole Improve Asthma Severity in Allergic Bronchopulmonary Aspergillosis and Severe Asthma with Fungal Sensitization. J. Asthma 2012, 49, 423–433. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Reilly, A.; Dunican, E. The Use of Targeted Monoclonal Antibodies in the Treatment of ABPA—A Case Series. Medicina 2022, 58, 53. https://doi.org/10.3390/medicina58010053
O’Reilly A, Dunican E. The Use of Targeted Monoclonal Antibodies in the Treatment of ABPA—A Case Series. Medicina. 2022; 58(1):53. https://doi.org/10.3390/medicina58010053
Chicago/Turabian StyleO’Reilly, Aoife, and Eleanor Dunican. 2022. "The Use of Targeted Monoclonal Antibodies in the Treatment of ABPA—A Case Series" Medicina 58, no. 1: 53. https://doi.org/10.3390/medicina58010053
APA StyleO’Reilly, A., & Dunican, E. (2022). The Use of Targeted Monoclonal Antibodies in the Treatment of ABPA—A Case Series. Medicina, 58(1), 53. https://doi.org/10.3390/medicina58010053