
Lower Limb Amputation Rates in Germany



Abstract
1. Introduction
2. Materials and Methods
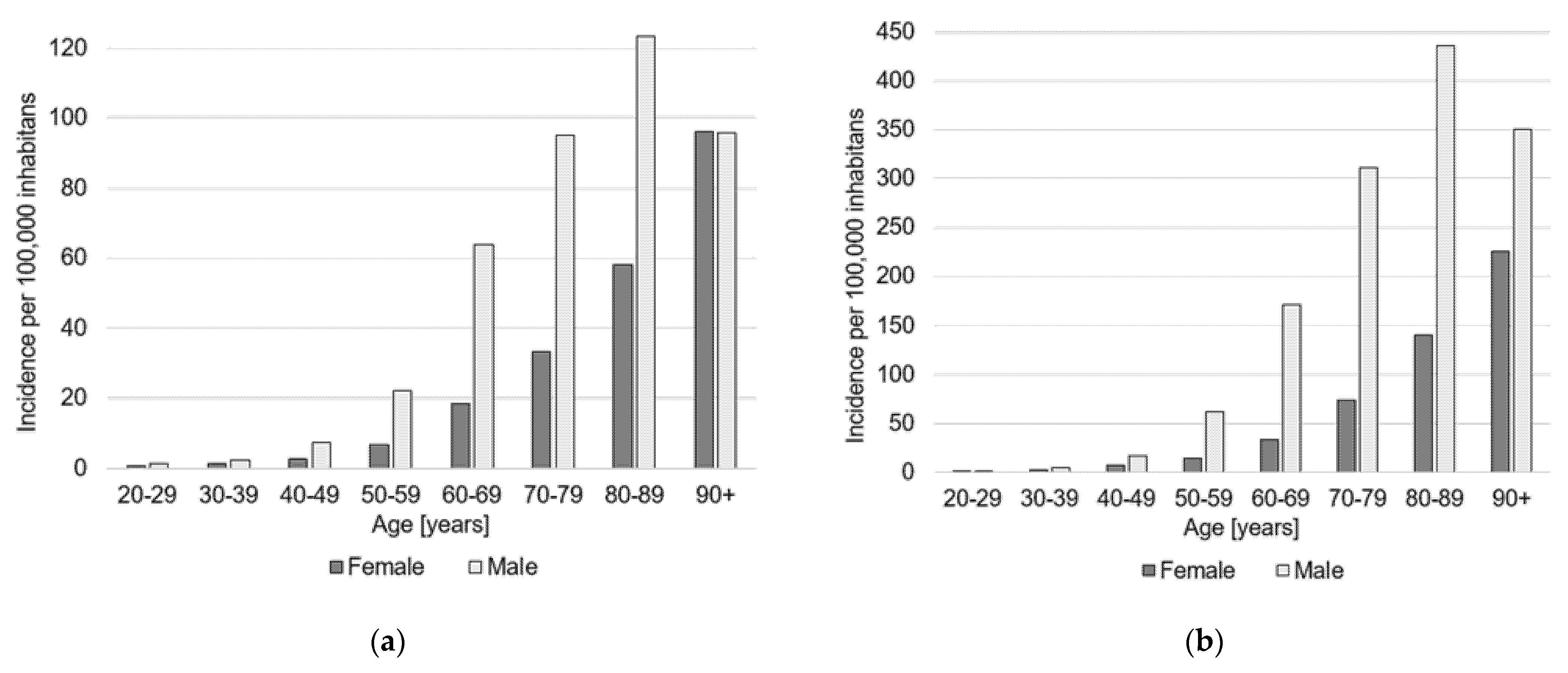
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Molina, C.S.; Faulk, J.B. Lower Extremity Amputation. Available online: https://www.ncbi.nlm.nih.gov/books/NBK546594/ (accessed on 1 December 2021).
- Rathnayake, A.; Saboo, A.; Malabu, U.H.; Falhammar, H. Lower extremity amputations and long-term outcomes in diabetic foot ulcers: A systematic review. World J. Diabetes 2020, 11, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, P.A.; Clark, D.; Derhy, P.H. What are the major causes of lower limb amputations in a major Australian teaching hospital? The Queensland Diabetic Foot Innovation Project, 2006–2007. J. Foot Ankle Res. 2011, 4, O24. [Google Scholar] [CrossRef]
- Diabetes care and research in Europe: The Saint Vincent declaration. Diabetes Med. 1990, 7, 360. [CrossRef]
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes—Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Rudan, D.; Zhu, Y.; Fowkes, F.J.I.; Rahimi, K.; Fowkes, F.G.R.; Rudan, I. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: An updated systematic review and analysis. Lancet Glob. Health 2019, 7, e1020–e1030. [Google Scholar] [CrossRef]
- Barnes, J.A.; Eid, M.A.; Creager, M.A.; Goodney, P.P. Epidemiology and Risk of Amputation in Patients With Diabetes Mellitus and Peripheral Artery Disease. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1808–1817. [Google Scholar] [CrossRef]
- Lombardo, F.L.; Maggini, M.; de Bellis, A.; Seghieri, G.; Anichini, R. Lower extremity amputations in persons with and without diabetes in Italy: 2001–2010. PLoS ONE 2014, 9, e86405. [Google Scholar] [CrossRef]
- Kröger, K.; Berg, C.; Santosa, F.; Malyar, N.; Reinecke, H. Lower Limb Amputation in Germany. Dtsch. Arztebl. Int. 2017, 114, 130–136. [Google Scholar] [CrossRef]
- Moxey, P.W.; Gogalniceanu, P.; Hinchliffe, R.J.; Loftus, I.M.; Jones, K.J.; Thompson, M.M.; Holt, P.J. Lower extremity amputations—A review of global variability in incidence. Diabetes Med. 2011, 28, 1144–1153. [Google Scholar] [CrossRef]
- Goodney, P.P.; Tarulli, M.; Faerber, A.E.; Schanzer, A.; Zwolak, R.M. Fifteen-year trends in lower limb amputation, revascularization, and preventive measures among medicare patients. JAMA Surg. 2015, 150, 84–86. [Google Scholar] [CrossRef]
- Vamos, E.P.; Bottle, A.; Edmonds, M.E.; Valabhji, J.; Majeed, A.; Millett, C. Changes in the incidence of lower extremity amputations in individuals with and without diabetes in England between 2004 and 2008. Diabetes Care 2010, 33, 2592–2597. [Google Scholar] [CrossRef]
- Claessen, H.; Avalosse, H.; Guillaume, J.; Narres, M.; Kvitkina, T.; Arend, W.; Morbach, S.; Lauwers, P.; Nobels, F.; Boly, J.; et al. Decreasing rates of major lower-extremity amputation in people with diabetes but not in those without: A nationwide study in Belgium. Diabetologia 2018, 61, 1966–1977. [Google Scholar] [CrossRef]
- Winell, K.; Venermo, M.; Ikonen, T.; Sund, R. Indicators for comparing the incidence of diabetic amputations: A nationwide population-based register study. Eur. J. Vasc. Endovasc. Surg. 2013, 46, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Rümenapf, G.; Morbach, S. Amputation Statistics-How to Interpret Them? Dtsch. Arztebl. Int. 2017, 114, 128–129. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Santosa, F.; Moysidis, T.; Kanya, S.; Babadagi-Hardt, Z.; Luther, B.; Kröger, K. Decrease in major amputations in Germany. Int. Wound J. 2015, 12, 276–279. [Google Scholar] [CrossRef]
- Spoden, M.; Nimptsch, U.; Mansky, T. Amputation rates of the lower limb by amputation level—Observational study using German national hospital discharge data from 2005 to 2015. BMC Health Serv. Res. 2019, 19, 8. [Google Scholar] [CrossRef]
- Carmona, G.A.; Hoffmeyer, P.; Herrmann, F.R.; Vaucher, J.; Tschopp, O.; Lacraz, A.; Vischer, U.M. Major lower limb amputations in the elderly observed over ten years: The role of diabetes and peripheral arterial disease. Diabetes Metab. 2005, 31, 449–454. [Google Scholar] [CrossRef]
- Moysidis, T.; Nowack, T.; Eickmeyer, F.; Waldhausen, P.; Brunken, A.; Hochlenert, D.; Engels, G.; Santosa, F.; Luther, B.; Kröger, K. Trends in amputations in people with hospital admissions for peripheral arterial disease in Germany. VASA 2011, 40, 289–295. [Google Scholar] [CrossRef]
- Dinh, T.; Veves, A. The influence of gender as a risk factor in diabetic foot ulceration. Wounds 2008, 20, 127–131. [Google Scholar] [PubMed]
- Low, E.E.; Inkellis, E.; Morshed, S. Complications and revision amputation following trauma-related lower limb loss. Injury 2017, 48, 364–370. [Google Scholar] [CrossRef]
- Paul, S.K.; Bhatt, D.L.; Montvida, O. The association of amputations and peripheral artery disease in patients with type 2 diabetes mellitus receiving sodium-glucose cotransporter type-2 inhibitors: Real-world study. Eur. Heart J. 2021, 42, 1728–1738. [Google Scholar] [CrossRef] [PubMed]
- Creager, M.A.; Matsushita, K.; Arya, S.; Beckman, J.A.; Duval, S.; Goodney, P.P.; Gutierrez, J.A.T.; Kaufman, J.A.; Joynt Maddox, K.E.; Pollak, A.W.; et al. Reducing Nontraumatic Lower-Extremity Amputations by 20% by 2030: Time to Get to Our Feet: A Policy Statement From the American Heart Association. Circulation 2021, 143, e875–e891. [Google Scholar] [CrossRef]
- Narres, M.; Kvitkina, T.; Claessen, H.; Droste, S.; Schuster, B.; Morbach, S.; Rümenapf, G.; van Acker, K.; Icks, A. Incidence of lower extremity amputations in the diabetic compared with the non-diabetic population: A systematic review. PLoS ONE 2017, 12, e0182081. [Google Scholar] [CrossRef] [PubMed]
- Geiss, L.S.; Li, Y.; Hora, I.; Albright, A.; Rolka, D.; Gregg, E.W. Resurgence of Diabetes-Related Nontraumatic Lower-Extremity Amputation in the Young and Middle-Aged Adult U.S. Population. Diabetes Care 2019, 42, 50–54. [Google Scholar] [CrossRef]
- Li, D.; Yang, J.Y.; Wang, T.; Shen, S.; Tang, H. Risks of diabetic foot syndrome and amputation associated with sodium glucose co-transporter 2 inhibitors: A Meta-analysis of Randomized Controlled Trials. Diabetes Metab. 2018, 44, 410–414. [Google Scholar] [CrossRef]
- Pütter, C.; Stausberg, J.; von Beckerath, O.; Reinecke, H.; Schäfer, E.; Kröger, K. Determinants of decreasing major amputation rates in Germany. VASA 2016, 45, 311–315. [Google Scholar] [CrossRef] [PubMed][Green Version]



{kind=link}
{kind=link}
| Operation and Procedure Classification System Code | Description |
|---|---|
| 5-864.0 + 5-864.1 | Hemipelvectomy |
| 5-864.2 | Hip disarticulation |
| 5-864.3 + 5-864.4 + 5-864.5 | Transfemoral amputation (above-the-knee) |
| 5-864.6 + 5-864.7 | Knee disarticulation |
| 5-864.8 + 5-864.9 + 5-864.a | Transtibial amputation |
| 5-864.x + 5-864.y | Lower extremity unspecified |
| 5-865.0 | Transmalleolar amputation |
| 5-865.1 + 5-865.2 + 5-865.3 | Foot amputation |
| 5-865.4 + 5-865.5 + 5-854.6 | Partial food amputation |
| 5-865.7 + 5-865.8 | Toe amputation |
| Anatomical Localization | Total Numbers | Incidence per 100,000 Inhabitants | Incidence in 2019 Relative to 2015 (%) | Incidence Rate Ratio [95% CI] | ||
|---|---|---|---|---|---|---|
| 2019 | 2015 | 2019 | 2015 | |||
| Major amputations | 16,452 | 17,546 | 24.2 | 26.1 | −7.3% | 0.93 [0.91–0.95] |
| Hemipelvectomy | 63 | 28 | 0.1 | 0.0 | +122.5% | 2.22 [1.32–3.76] |
| Hip disarticulation | 154 | 109 | 0.2 | 0.2 | +39.7% | 1.40 [1.07–1.82] |
| Transfemoral amputation | 9015 | 5201 | 13.3 | 7.8 | +71.4% | 1.71 [1.65–1.78] |
| Knee disarticulation | 700 | 4972 | 1.0 | 7.4 | −86.1% | 0.14 [0.13–0.15] |
| Transtibial amputation | 6455 | 5963 | 9.5 | 8.9 | +7.0% | 1.07 [1.03–1.11] |
| Lower extremity unspecified | 65 | 1273 | 0.1 | 1.9 | −95.0% | 0.05 [0.04–0.06] |
| Minor amputations | 45,564 | 40,308 | 67.1 | 60.1 | +11.8% | 1.12 [1.10–1.13] |
| Transmalleolar amputation | 157 | 47 | 0.2 | 0.1 | +230.3% | 3.30 [2.20–4.95] |
| Foot amputation | 223 | 346 | 0.3 | 0.5 | −36.3% | 0.64 [0.55–0.74] |
| Partial foot amputation | 9189 | 5166 | 13.5 | 7.7 | +75.9% | 1.76 [1.69–1.82] |
| Toe amputation | 35,995 | 34,749 | 53.0 | 51.8 | +2.4% | 1.02 [1.01–1.04] |
| 20–29 Years (Males, Females, Total) | 30–39 Years (Males, Females, Total) | 40–49 Years (Males, Females, Total) | 50–59 Years (Males, Females, Total) | 60–69 Years (Males, Females, Total) | 70–79 Years (Males, Females, Total) | 80–89 Years (Males, Females, Total) | 90 Years or Older (Males, Females, Total) | All (Males, Females, Total) | |
|---|---|---|---|---|---|---|---|---|---|
| Major amputations in 2015 | 1.2, 0.2, 0.7 | 2.1, 0.8, 1.5 | 5.8., 3.4, 4.6 | 24.3, 8.1, 16.2 | 65.2, 19.3, 41.5 | 102.5, 37.5, 67.0 | 148.0, 82.3, 106.4 | 103.7, 142.1, 130.5 | 34.6, 18.1, 26.1 |
| Major amputations in 2019 | 1.2, 0.5, 0.9 | 2.3, 1.4, 1.9 | 7.2, 2.7, 4.9 | 22.2, 6.7, 14.4 | 63.9, 18.4, 40.4 | 95.0, 33.1, 61.4 | 123.3, 58.0, 83.4 | 95.6, 96.0, 95.9 | 33.8, 15.2, 24.3 |
| IRR major amputations | 0.98, 2.16, 1.16 | 1.07, 1.70, 1.25 | 1.24, 0.78, 1.07 | 0.92, 0.83, 0.89 | 0.98, 0.95, 0.98 | 0.93, 0.88, 0.92 | 0.83, 0.71, 0.78 | 0.92, 0.68, 0.73 | 0.98, 0.84, 0.93 |
| Minor amputations in 2015 | 1.8, 0.6, 1.2 | 4.2, 2.1, 3.1 | 14.6, 5.6, 10.2 | 53.5, 14.8, 34.2 | 149.6, 34.4, 90.1 | 271.0, 82.5, 168.0 | 389.0, 169.9, 250.3 | 265.3, 241.5, 248.7 | 85.4, 35.9, 60,1 |
| Minor amputations in 2019 | 1.5, 1.1, 1.3 | 4.7, 1.9, 3.4 | 17.0, 6.4, 11.7 | 61.0, 13.9, 37.4 | 171.1, 33.3, 100.1 | 310.8, 74.0, 182.3 | 435.2, 140.1, 254.9 | 350.4, 225.0, 266.7 | 102.5, 33.5, 67.2 |
| IRR minor amputations | 0.97, 1.81, 1.10 | 1.14, 0.94, 1.07 | 1.16, 1.15, 1.16 | 1.14, 0.94, 1.09 | 1.14, 0.97, 1.11 | 1.15, 0.90, 1.09 | 1.12, 0.82, 1.02 | 1.32, 0.93, 1.07 | 1.20, 0.93, 1.12 |
| Anatomical Localization | Total Numbers | Revision Rate | Revision Rate 2019 Relative to 2015 (%) | Percentage Female/Male | Incidence Female/Male | Percentage Aged ≤70 Years/>70 Years | Incidence Aged ≤70 Years/>70 Years |
|---|---|---|---|---|---|---|---|
| Femur | 1502 | 0.16 | +11.8% | 38/62 | 1.7/2.8 | 56/44 | 1.5/5.0 |
| Lower leg | 1546 | 0.24 | +14.5% | 25/75 | 1.1/3.5 | 61/39 | 1.7/4.5 |
| Foot | 5785 | 0.13 | +1.3% | 20/80 | 3.3/14.0 | 44/56 | 4.6/24.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walter, N.; Alt, V.; Rupp, M. Lower Limb Amputation Rates in Germany. Medicina 2022, 58, 101. https://doi.org/10.3390/medicina58010101
Walter N, Alt V, Rupp M. Lower Limb Amputation Rates in Germany. Medicina. 2022; 58(1):101. https://doi.org/10.3390/medicina58010101
Chicago/Turabian StyleWalter, Nike, Volker Alt, and Markus Rupp. 2022. "Lower Limb Amputation Rates in Germany" Medicina 58, no. 1: 101. https://doi.org/10.3390/medicina58010101
APA StyleWalter, N., Alt, V., & Rupp, M. (2022). Lower Limb Amputation Rates in Germany. Medicina, 58(1), 101. https://doi.org/10.3390/medicina58010101