
Iris-Claw Intraocular Lens: Anterior Chamber or Retropupillary Implantation? A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
3. Results
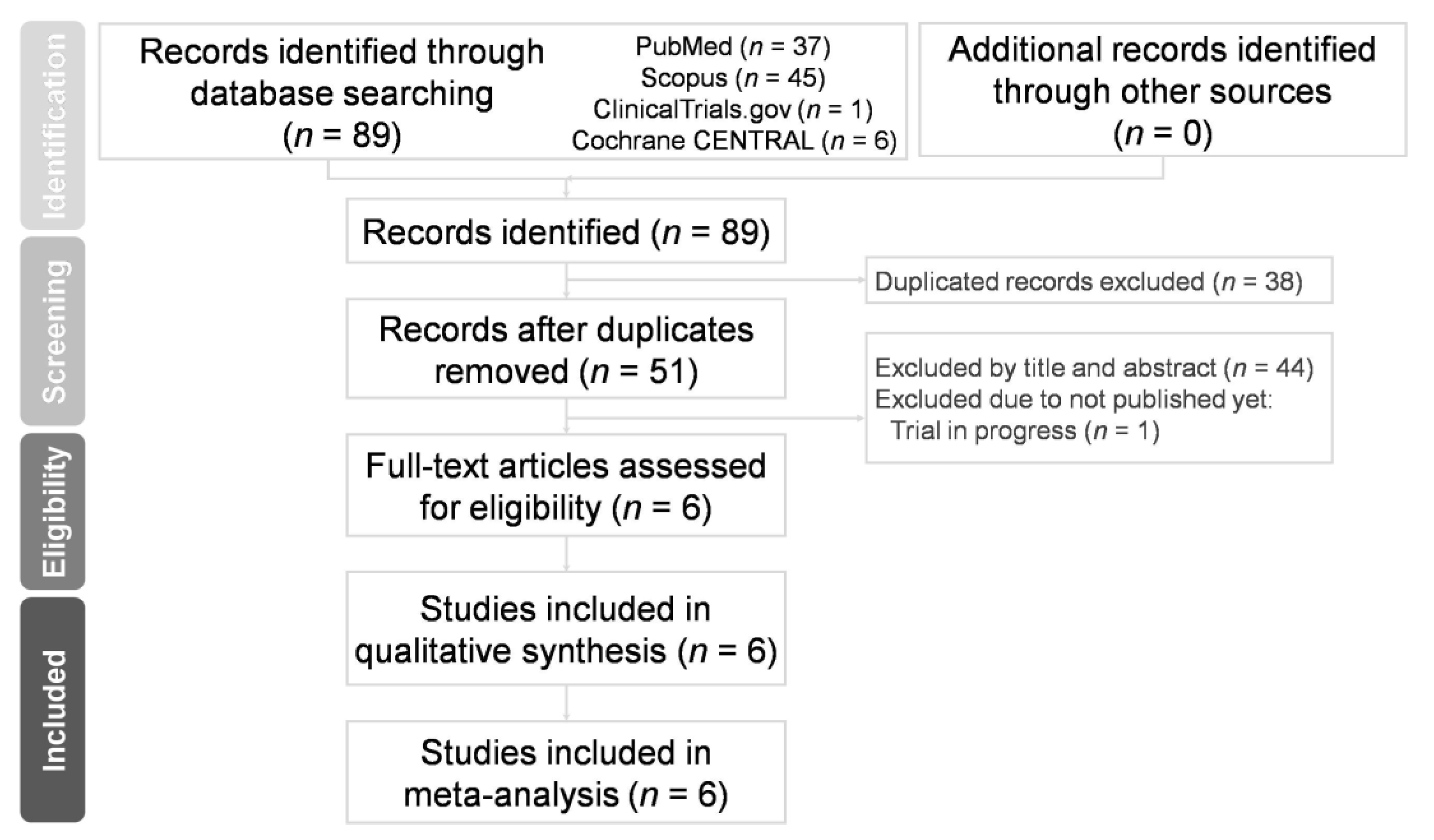
3.1. Study Search and Characteristics of Included Patients
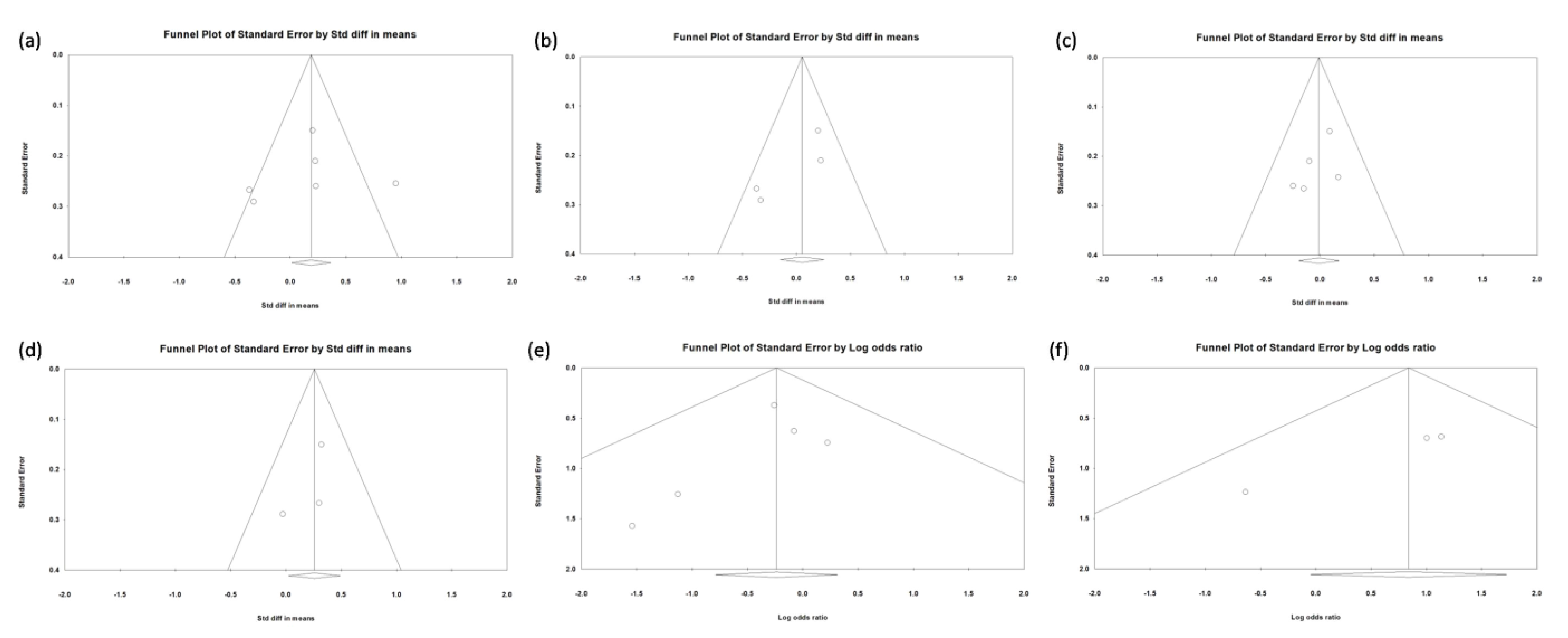
3.2. Quality Assessment and Risk of Bias
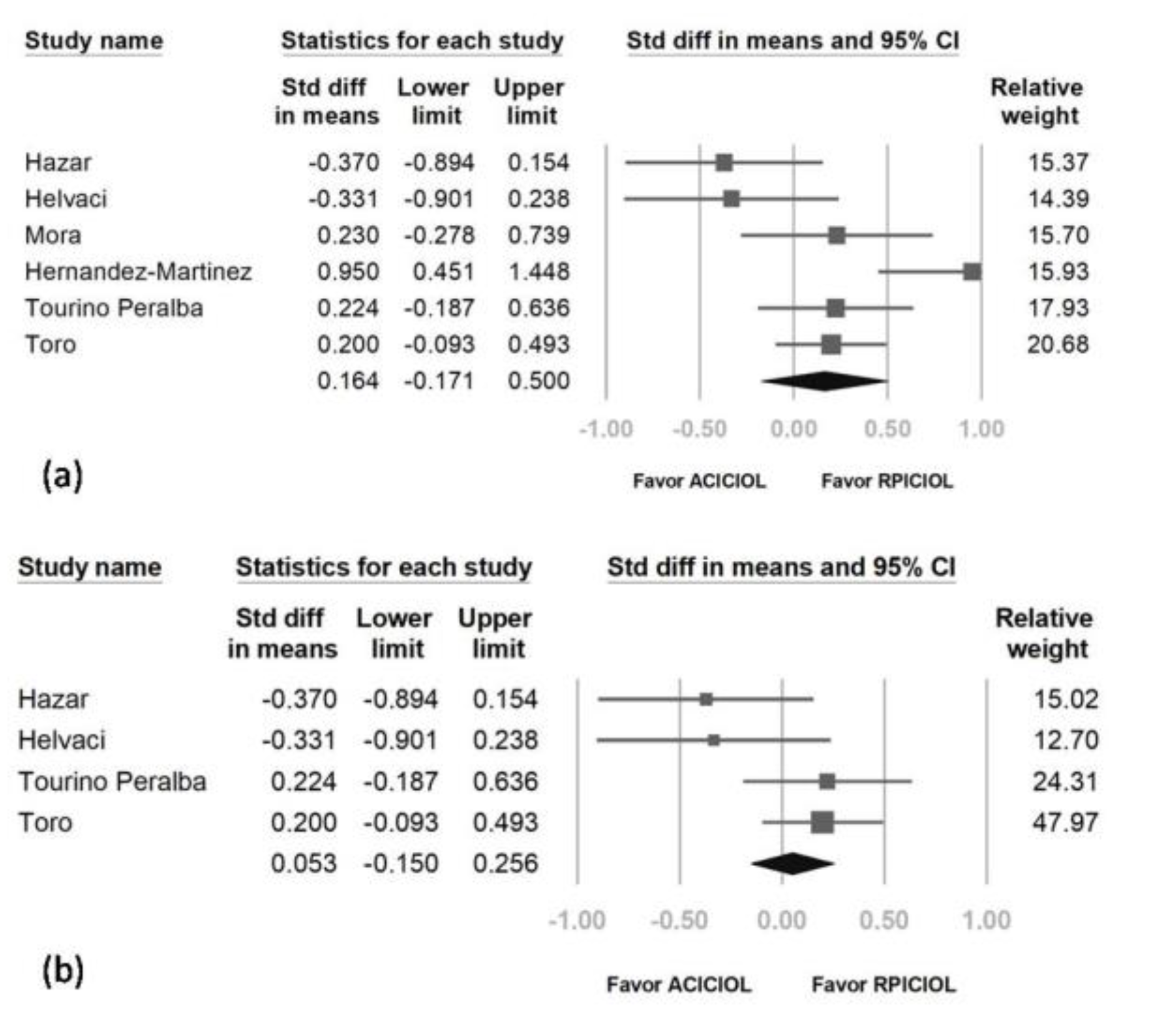
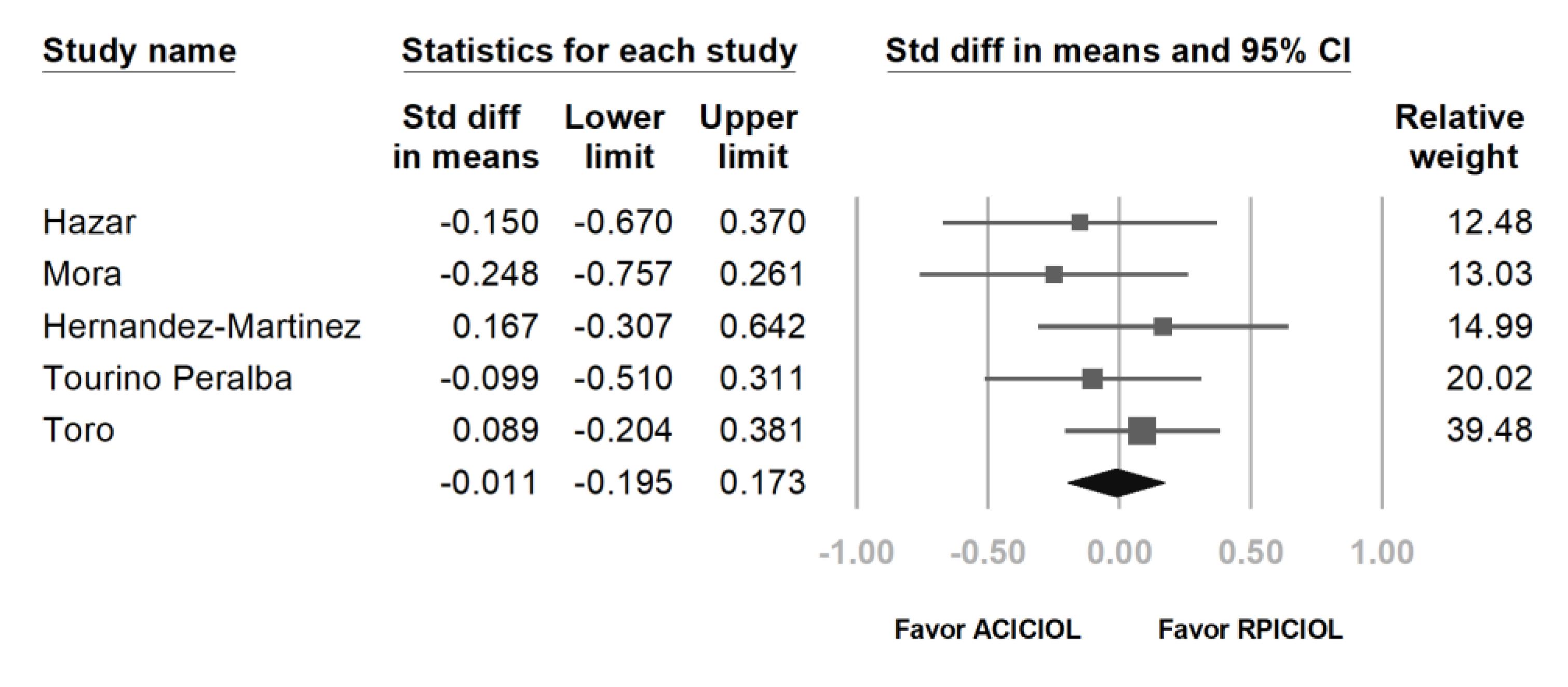
3.3. CDVA and ECC Outcomes between AC and RP ICIOL
3.4. IOP Outcome and Risk of IOP Elevation between AC and RP ICIOL
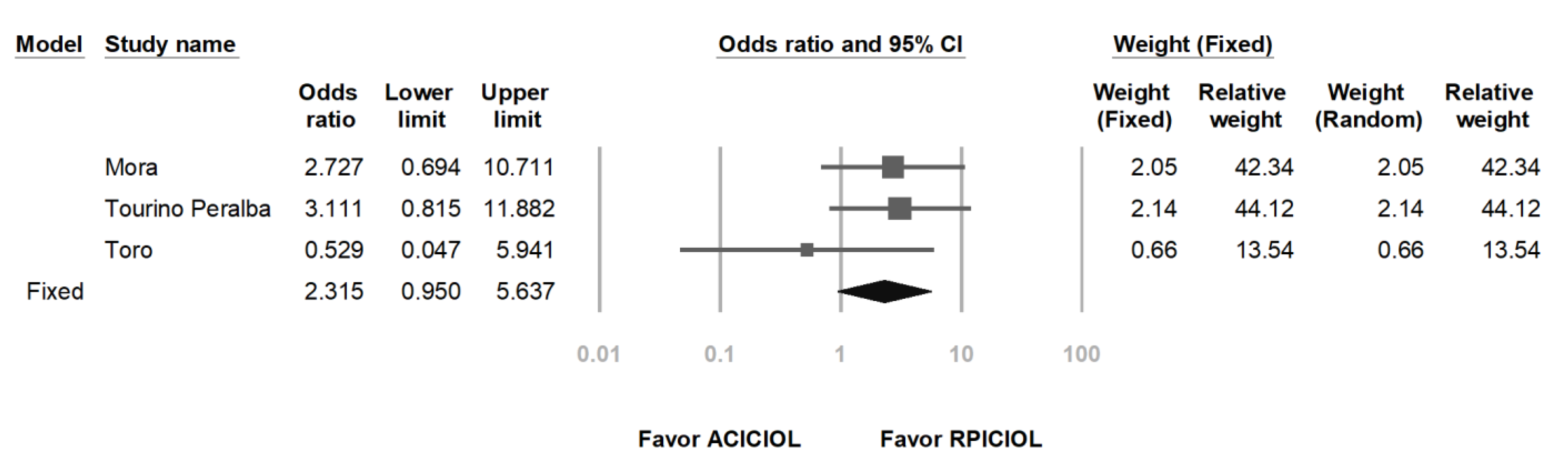
3.5. Risk of CME between AC and RP ICIOL
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wagoner, M.D.; Cox, T.A.; Ariyasu, R.G.; Jacobs, D.S.; Karp, C.L. Intraocular lens implantation in the absence of capsular support: A report by the American Academy of Ophthalmology. Ophthalmology 2003, 110, 840–859. [Google Scholar] [CrossRef]
- Shen, J.F.; Deng, S.; Hammersmith, K.M.; Kuo, A.N.; Li, J.Y.; Weikert, M.P.; Shtein, R.M. Intraocular Lens Implantation in the Absence of Zonular Support: An Outcomes and Safety Update: A Report by the American Academy of Ophthalmology. Ophthalmology 2020, 127, 1234–1258. [Google Scholar] [CrossRef]
- Sawada, T.; Kimura, W.; Kimura, T.; Suga, H.; Ohte, A.; Yamanishi, S.; Ohara, T. Long-term follow-up of primary anterior chamber intraocular lens implantation. J. Cataract. Refract. Surg. 1998, 24, 1515–1520. [Google Scholar] [CrossRef]
- Tang, Y.; Xu, J.; Chen, J.; Lu, Y. Long-Term Destiny of Corneal Endothelial Cells in Anterior Chamber Intraocular Lens-Implanted Eyes. J. Ophthalmol. 2020, 2020, 5967509. [Google Scholar] [CrossRef] [PubMed]
- Bellucci, R.; Pucci, V.; Morselli, S.; Bonomi, L. Secondary implantation of angle-supported anterior chamber and scleral-fixated posterior chamber intraocular lenses. J. Cataract. Refract. Surg. 1996, 22, 247–252. [Google Scholar] [CrossRef]
- Jing, W.; Guanlu, L.; Qianyin, Z.; Shuyi, L.; Fengying, H.; Jian, L.; Wen, X. Iris-Claw Intraocular Lens and Scleral-Fixated Posterior Chamber Intraocular Lens Implantations in Correcting Aphakia: A Meta-Analysis. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3530–3536. [Google Scholar] [CrossRef]
- Buckley, E.G. Hanging by a thread: The long-term efficacy and safety of transscleral sutured intraocular lenses in children (an American Ophthalmological Society thesis). Trans. Am. Ophthalmol. Soc. 2007, 105, 294–311. [Google Scholar] [PubMed]
- Ansah, D.O.; Li, X.; Gehlbach, P.L.; Jun, A.S.; Soiberman, U.S. Prediction error in iris suture fixated intraocular lenses and long-term stability. Clin. Exp. Ophthalmol. 2020, 48, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- Worst, J.G.; Massaro, R.G.; Ludwig, H.H. The introduction of an artificial lens into the eye using Binkhorst’s technique. Ophthalmologica 1972, 164, 387–391. [Google Scholar] [CrossRef]
- Galvis, V.; Tello, A.; Carreno, N.I.; Revelo, M.L. Retropupillary iris-claw intraocular lens in aphakic eyes. J. Cataract. Refract. Surg. 2013, 39, 970–971. [Google Scholar] [CrossRef] [PubMed]
- Galvis, V.; Villamil, J.F.; Acuna, M.F.; Camacho, P.A.; Merayo-Lloves, J.; Tello, A.; Zambrano, S.L.; Rey, J.J.; Espinoza, J.V.; Prada, A.M. Long-term endothelial cell loss with the iris-claw intraocular phakic lenses (Artisan(R)). Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 2775–2787. [Google Scholar] [CrossRef] [PubMed]
- Fechner, P.U.; Worst, J.G. A new concave intraocular lens for the correction of myopia. Eur. J. Implant Refract. Surg. 1989, 1, 41–43. [Google Scholar] [CrossRef]
- Amar, L. Posterior chamber iris claw lens. Am. Intra-Ocular Implant Soc. J. 1980, 6, 279. [Google Scholar] [CrossRef]
- Rijneveld, W.J.; Beekhuis, W.H.; Hassman, E.F.; Dellaert, M.M.; Geerards, A.J. Iris claw lens: Anterior and posterior iris surface fixation in the absence of capsular support during penetrating keratoplasty. J. Refract. Corneal Surg. 1994, 10, 14–19. [Google Scholar] [CrossRef]
- Gonnermann, J.; Amiri, S.; Klamann, M.; Maier, A.K.; Joussen, A.M.; Rieck, P.W.; Torun, N.; Bertelmann, E. Endothelial cell loss after retropupillary iris-claw intraocular lens implantation. Klin. Monbl. Augenheilkd 2014, 231, 784–787. [Google Scholar] [CrossRef] [PubMed]
- Forlini, M.; Soliman, W.; Bratu, A.; Rossini, P.; Cavallini, G.M.; Forlini, C. Long-term follow-up of retropupillary iris-claw intraocular lens implantation: A retrospective analysis. BMC Ophthalmol. 2015, 15, 143. [Google Scholar] [CrossRef]
- Teng, H.; Zhang, H. Comparison of Artisan iris-claw intraocular lens implantation and posterior chamber intraocular lens sulcus fixation for aphakic eyes. Int. J. Ophthalmol. 2014, 7, 283–287. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Vounotrypidis, E.; Schuster, I.; Mackert, M.J.; Kook, D.; Priglinger, S.; Wolf, A. Secondary intraocular lens implantation: A large retrospective analysis. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 125–134. [Google Scholar] [CrossRef]
- Hara, S.; Borkenstein, A.F.; Ehmer, A.; Auffarth, G.U. Retropupillary fixation of iris-claw intraocular lens versus transscleral suturing fixation for aphakic eyes without capsular support. J. Refract. Surg. 2011, 27, 729–735. [Google Scholar] [CrossRef]
- Helvaci, S.; Demirduzen, S.; Oksuz, H. Iris-claw intraocular lens implantation: Anterior chamber versus retropupillary implantation. Indian J. Ophthalmol. 2016, 64, 45–49. [Google Scholar] [CrossRef]
- Hazar, L.; Kara, N.; Bozkurt, E.; Ozgurhan, E.B.; Demirok, A. Intraocular lens implantation procedures in aphakic eyes with insufficient capsular support associated with previous cataract surgery. J. Refract. Surg. 2013, 29, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Mora, P.; Calzetti, G.; Favilla, S.; Forlini, M.; Tedesco, S.; Date, P.; Tagliavini, V.; Carta, A.; Frisina, R.; Pedrotti, E.; et al. Comparative Analysis of the Safety and Functional Outcomes of Anterior versus Retropupillary Iris-Claw IOL Fixation. J. Ophthalmol. 2018, 2018, 8463569. [Google Scholar] [CrossRef] [PubMed]
- Hernandez Martinez, A.; Almeida Gonzalez, C.V. Iris-claw intraocular lens implantation: Efficiency and safety according to technique. J. Cataract. Refract. Surg. 2018, 44, 1186–1191. [Google Scholar] [CrossRef]
- Tourino Peralba, R.; Lamas-Francis, D.; Sarandeses-Diez, T.; Martinez-Perez, L.; Rodriguez-Ares, T. Iris-claw intraocular lens for aphakia: Can location influence the final outcomes? J. Cataract. Refract. Surg. 2018, 44, 818–826. [Google Scholar] [CrossRef]
- Toro, M.D.; Longo, A.; Avitabile, T.; Nowomiejska, K.; Gagliano, C.; Tripodi, S.; Choragiewicz, T.; Kaminska, A.; Figus, M.; Posarelli, C.; et al. Five-year follow-up of secondary iris-claw intraocular lens implantation for the treatment of aphakia: Anterior chamber versus retropupillary implantation. PLoS ONE 2019, 14, e0214140. [Google Scholar] [CrossRef]
- Saxena, R.; Boekhoorn, S.S.; Mulder, P.G.; Noordzij, B.; van Rij, G.; Luyten, G.P. Long-term follow-up of endothelial cell change after Artisan phakic intraocular lens implantation. Ophthalmology 2008, 115, 608–613 e601. [Google Scholar] [CrossRef]
- Landesz, M.; Worst, J.G.; van Rij, G. Long-term results of correction of high myopia with an iris claw phakic intraocular lens. J. Refract. Surg. 2000, 16, 310–316. [Google Scholar] [CrossRef]
- Catala-Mora, J.; Cuadras, D.; Diaz-Cascajosa, J.; Castany-Aregall, M.; Prat-Bartomeu, J.; Garcia-Arumi, J. Anterior iris-claw intraocular lens implantation for the management of nontraumatic ectopia lentis: Long-term outcomes in a paediatric cohort. Acta Ophthalmol. 2017, 95, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Guell, J.L.; Verdaguer, P.; Elies, D.; Gris, O.; Manero, F.; Mateu-Figueras, G.; Morral, M. Secondary iris-claw anterior chamber lens implantation in patients with aphakia without capsular support. Br. J. Ophthalmol. 2014, 98, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.Y.; Lee, C.H.; Kang, H.G.; Han, J.Y.; Byeon, S.H.; Kim, S.S.; Koh, H.J.; Kim, M. Long-term surgical outcomes of primary retropupillary iris claw intraocular lens implantation for the treatment of intraocular lens dislocation. Sci. Rep. 2021, 11. [Google Scholar] [CrossRef]
- Anbari, A.; Lake, D.B. Posteriorly enclavated iris claw intraocular lens for aphakia: Long-term corneal endothelial safety study. Eur. J. Ophthalmol. 2015, 25, 208–213. [Google Scholar] [CrossRef]
- Drolsum, L.; Kristianslund, O. Implantation of retropupillary iris-claw lenses: A review on surgical management and outcomes. Acta Ophthalmol. 2021. [Google Scholar] [CrossRef]
- Gazzard, G.; Friedman, D.S.; Devereux, J.G.; Chew, P.; Seah, S.K. A prospective ultrasound biomicroscopy evaluation of changes in anterior segment morphology after laser iridotomy in Asian eyes. Ophthalmology 2003, 110, 630–638. [Google Scholar] [CrossRef]
- See, J.L.; Chew, P.T.; Smith, S.D.; Nolan, W.P.; Chan, Y.H.; Huang, D.; Zheng, C.; Foster, P.J.; Aung, T.; Friedman, D.S. Changes in anterior segment morphology in response to illumination and after laser iridotomy in Asian eyes: An anterior segment OCT study. Br. J. Ophthalmol. 2007, 91, 1485–1489. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Guzman, C.P.; Cheung, C.Y.; He, Y.; Friedman, D.S.; Ong, S.H.; Narayanaswamy, A.K.; Chew, P.T.; Perera, S.A.; Aung, T. Analysis of anterior segment dynamics using anterior segment optical coherence tomography before and after laser peripheral iridotomy. JAMA Ophthalmol. 2013, 131, 44–49. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Massa, H.F.; Gobej, I.; Jacquier, P.; Jonescu-Cuypers, C.; Le Quoy, O. Cystoid macular oedema and iris-fixated intraocular lens treated with intraocular lens exchange: A case series and review. J. Int. Med. Res. 2019, 47, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Faria, M.; Pinto Ferreira, N.; Medeiros Pinto, J.; Cordeiro-Sousa, D.; Cardoso-Leal, I.; Neto, E.; Marques-Neves, C. Retropupillary iris claw intraocular lens implantation in aphakia for dislocated intraocular lens. Int. Med. Case Rep. J. 2016, 9, 261–265. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Study Design | Enrolled Sample Number, Eyes (Male/Female) | Age Mean ± SD, Years | Outcome Measurement | Follow-Up Time, Months | Quality Assessment |
|---|---|---|---|---|---|---|---|
| Hazar et al., 2013 | Turkey | RCS | AC ICIOL: 35 (24/11) RP ICIOL: 24 (14/10) | AC ICIOL: 52 ± 18 RP ICIOL: 61 ± 16 | CDVA, IOP, slit-lamp exam, fundus exam, ECC, FA (if needed) | AC ICIOL: 12.0 ± 7.7 CIOL: 10.1 ± 7.3 (mean ± SD) | 4 ** |
| Helvaci et al., 2016 | Turkey | RCT | AC ICIOL: 20 (11/9) RP ICIOL: 30 (13/7) | AC ICIOL: 68.5 ± 6.8 RP ICIOL: 69.9 ± 8.2 | CDVA, IOP, slit-lamp exam, fundus exam | 6 | 1 * |
| Mora et al., 2018 | Italy | RCS | AC ICIOL: 28 (20/8) RP ICIOL: 32 (21/11) | AC ICIOL: 72.7 ± 13.5 RP ICIOL:73.8 ± 13.4 | CDVA, IOP, slit-lamp exam, fundus exam, ECC, CMT on OCT | 12 | 4 ** |
| Hernández-Martínez et al., 2018 | Spain | RCS | AC ICIOL: 28 (14/14) RP ICIOL: 44 (23/21) | AC ICIOL: 74.0 ± 14.0 RP ICIOL: 70.4 ± 12.8 | UDVA, CDVA, SIA, ECC | 33 ± 21.8 (mean ± SD) | 2 ** |
| Tourino Peralba et al., 2018 | Spain | RCS | AC ICIOL: 57 (32/25) RP ICIOL: 38 (20/18) | AC ICIOL: 66 ± 15.6 RP ICIOL: 72.5 ± 11.1 | CDVA, IOP, slit-lamp exam, fundus exam, corneal astigmatism, ECC, CMT on OCT | 12 | 3 ** |
| Toro et al., 2019 | Italy | RCS | AC ICIOL: 87 (49/38) RP ICIOL: 93 (53/40) | AC ICIOL: 70.6 ± 5.5 RP ICIOL: 69.5 ± 6.3 | CDVA, IOP, slit-lamp exam, fundus exam, CCT, ECC, CMT on OCT | 60 | 4 ** |
| Author, Year | ICIOL | Main Wound Location | Side Ports Location | Vitrectomy | Instrument for Iris Fixation | Peripheral Iridotomy | Wound Closure |
|---|---|---|---|---|---|---|---|
| Hazar et al., 2013 | Artisan or Verisyse | Superior 6.0mm clear corneal incision | AC ICIOL: 2 and 10 o’clock RP ICIOL: 3 o’clock for left eye/9 o’clock for right eye | Anterior vitrectomy if vitreous in AC | AC ICIOL: enclavation needle RP ICIOL: Sinskey hook or iris spatula | AC ICIOL: 12 o’clock RP ICIOL: not performed | Interrupted 10-0 nylon |
| Helvaci et al., 2016 | Artisan | Superior 5.5 mm limbal corneal incision | 2 and 10 o’clock | Anterior vitrectomy or PPV for cases with IOL luxation, lens luxation, luxated nigra cataract | Enclavation needle | AC ICIOL: superior RP ICIOL: not performed | Interrupted sutures |
| Mora et al., 2018 | Artisan | Superior 5.5 mm limbal corneal incision | 3 and 9 o’clock | Anterior vitrectomy as required or PPV if indicated | Enclavation microspatula | AC ICIOL: superior RP ICIOL: not performed | Noncontinuous 10-0 nylon |
| Hernández-Martínez et al., 2018 | Artisan | Superior 5.5 mm corneal incision or scleral tunnel 2.0 mm from the limbus | 2 and 10 o’clock | PPV or anterior vitrectomy through corneal access in eyes that did not require a PPV | AC ICIOL: 16 cases- claw needle/12 cases- Vacufix system (Ophtec BV) RP ICIOL: claw needle | AC ICIOL: 12 o’clock RP ICIOL: not performed | AC ICIOL: 5 cases- scleral incision(Interrupted 10-0 nylon)/23 cases- corneal incision (Continued 10-0 nylon) RP ICIOL: 31 cases- scleral incision (Interrupted 10-0 nylon)/13 cases- corneal incision (Continued 10-0 nylon) |
| Tourino Peralba et al., 2018 | Artisan | Superior clear corneal incision | AC ICIOL: 2 and 10 o’clock RP ICIOL: 3 o’clock for left eye/9 o’clock for right eye | Extensive anterior vitrectomy if no previous peripheral iridectomy performed previously | AC ICIOL: enclavation needle RP ICIOL: reverse Sinskey hook or 27-gauge needle bent 45 degrees | Most cases: peripheral iridectomy performed during previous procedures Remaining cases: not performed | Interrupted 10-0 nylon |
| Toro et al., 2019 | Artisan | Superior 5.5 mm limbal corneal incision | 3 and 9 o’clock | Anterior vitrectomy as required | Enclavation microspatula | AC ICIOL: superior RP ICIOL: not performed | Interrupted 10-0 nylons |
| Analysis | No. of Studies | Subjects (No.) | SMD/OR | 95% CI | p Value for Differences | Heterogeneity | Egger’s Test | |
|---|---|---|---|---|---|---|---|---|
| p Value | I2 | p Value | ||||||
| CDVA | 6 | 516 | 0.164 | −0.171, 0.500 | 0.337 | 0.005 | 69.855 | 0.741 |
| CDVA | 4 | 384 | 0.053 | −0.151, 0.256 | 0.610 | 5.888 | 49.051 | 0.136 |
| ECC | 5 | 466 | −0.011 | −0.195, 0.173 | 0.908 | 0.686 | 0.000 | 0.290 |
| IOP | 3 | 289 | 0.119 | 0.023, 0.490 | 0.031 | 0.553 | 0.000 | 0.488 |
| IOP elevation event | 5 | 444 | 0.788 | 0.454, 1.368 | 0.398 | 0.801 | 0.000 | 0.339 |
| CME event | 3 | 347 | 2.315 | 0.950, 5.637 | 0.065 | 0.433 | 0.000 | 0.044 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, I.-C.; Chang, Y.-H.; Hernández Martínez, A.; Hung, C.-F. Iris-Claw Intraocular Lens: Anterior Chamber or Retropupillary Implantation? A Systematic Review and Meta-Analysis. Medicina 2021, 57, 785. https://doi.org/10.3390/medicina57080785
Liang I-C, Chang Y-H, Hernández Martínez A, Hung C-F. Iris-Claw Intraocular Lens: Anterior Chamber or Retropupillary Implantation? A Systematic Review and Meta-Analysis. Medicina. 2021; 57(8):785. https://doi.org/10.3390/medicina57080785
Chicago/Turabian StyleLiang, I-Chia, Yun-Hsiang Chang, Adrián Hernández Martínez, and Chi-Feng Hung. 2021. "Iris-Claw Intraocular Lens: Anterior Chamber or Retropupillary Implantation? A Systematic Review and Meta-Analysis" Medicina 57, no. 8: 785. https://doi.org/10.3390/medicina57080785
APA StyleLiang, I.-C., Chang, Y.-H., Hernández Martínez, A., & Hung, C.-F. (2021). Iris-Claw Intraocular Lens: Anterior Chamber or Retropupillary Implantation? A Systematic Review and Meta-Analysis. Medicina, 57(8), 785. https://doi.org/10.3390/medicina57080785