
The Importance of Diet in Predicting the Remission of Urticaria—Determination of Allergen-Specific IgE


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Evaluation of Specific IgEas Predictor of Disease Remission
3.2. Specific IgE Values in Dynamics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Choi, J.H.; Sim, J.K.; Oh, J.Y.; Hur, G.-Y.; Min, K.H.; Lee, S.Y.; Shim, J.J.; Kang, K.H. An IgE-Mediated Allergic Reaction Caused by Mulberry Fruit. Allergy Asthma Immunol. Res. 2015, 7, 195–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.; Ju, S.; Chang, H. Food allergy knowledge, perception of food allergy labeling, and levelof dietary practice: A comparison between children with and without food allergy experience. Nutr. Res. Pract. 2015, 9, 92–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cianferoni, A. Food allergy. Curr. Pharm. Des. 2014, 20, 931–945. [Google Scholar] [CrossRef] [PubMed]
- Cingolani, A.; Di Pillo, S.; Cerasa, M.; Rapino, D.; Consilvio, N.P.; Attanasi, M.; Scaparrotta, A.; Marcovecchio, M.L.; Mohn, A.; Chiarelli, F. Usefulness of nBos d 4, 5 and nBos d 8 specific IgE antibodies in cow’s milk allergic children. Allergy Asthma Immunol. Res. 2014, 2, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Dahdah, L.; Pecora, V.; Riccardi, C.; Fierro, V.; Valluzzi, R.L.; Mennini, M. How to predict and improve prognosis of food allergy. Curr. Opin. Allergy Clin. Immunol. 2018, 18, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; Thalayasingam, M.; Lee, B.W. Food allergy in Asia: How does it compare? Asia Pac. Allergy 2013, 3, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du Toit, G.; Roberts, G.; Sayre, P.H.; Plaut, M.; Bahnson, H.T.; Mitchell, H.; Radulovic, S.; Chan, S.; Fox, A.; Turcanu, V.; et al. Identifying infants and high risk of peanut allergy: The Learning Early About Peanut Allergy (LEAP) screening study. J. Allergy Clin. Immunol. 2013, 131, 135–143. [Google Scholar] [CrossRef]
- Machler, B.C.; Jacob, S.E. Carmine Red: A Potentially Overlooked Allergen in Children. Dermatitis 2018, 29, 92–93. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H.; Sampson, H.A. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention and management. J. Allergy Clin. Immunol. 2018, 141, 41–58. [Google Scholar] [CrossRef] [Green Version]
- Yan, J.; She, T.; Zhang, J.; Lin, S.; Zhang, Y.; Zhu, L.; Yin, Y.; Si, P.; Li, H. Egg white component-resolved diagnosis: Testing of serum ovalbumin-specific IgE by luminescent oxygen channeling immunoassay. J. Lumin. 2018, 200, 87–93. [Google Scholar] [CrossRef]
- Gamboa, P.M.; Garcia-Lirio, E.; Gonzalez, C.; Gonzalez, A.; Martinez-Aranguren, R.M.; Sanz Maria, L. Is the Quantification of Antigen-Specific Basophil Activation a Useful Tool for Monitoring Oral Tolerance Induction in Children with Egg Allergy? J. Investig. Allergol. Clin. Immunol. 2016, 26, 25–30. [Google Scholar] [PubMed] [Green Version]
- Dang, A.T.; Chundi, P.K.; Mousa, N.A.; Beyer, A.I.; Chansakulporn, S.; Venter, C.; Mersha, T.B.; Assa’Ad, A.H. The effect of age, sex, race/ethnicity, health insurance and food specific serum immunoglobulin E on outcomes of oral food challenges. World Allergy Organ. J. 2020, 13, 100100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klemans, R.J.; Otte, D.; Knol, M.; Knol, E.F.; Meijer, Y.; Gmelig-Meyling, F.H.; Bruijnzeel-Koomen, C.A.; Knulst, A.C.; Pasmans, S.G. The diagnostic value of specific IgE to Ara h 2 to predict peanut allergy in children is comparable to a validated and updated diagnostic prediction model. J. Allergy Clin. Immunol. 2013, 131, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H.; Leung, D.Y. Advances in allergic skin diseases, anaphylaxis, and hypersensitivity reactions to foods, drugs, and insects in 2014. J. Allergy Clin. Immunol. 2015, 135, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Armentia, A.; Martín-Armentia, S.; Pineda, F.; Castro, M.; Fernández, S.; Moro, A.; Castillo, M. Allergic hypersensitivity to garlic and onion in children and adults. Allergol. Immunopathol. 2020, 48, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Rostam, S.R.K.; Shekhany, K.A.M.; Smail, H.O. Prevalence of common food allergies in Erbil Province, Kurdistan Region of Iraq. AIMS Allergy Immunol. 2020, 4, 117–127. [Google Scholar] [CrossRef]
- Krogulska, A.; Wood, R.A. Peanut allergy diagnosis: Moving from basic to more elegant testing. Pediatr. Allergy Immunol. 2020, 31, 346–357. [Google Scholar] [CrossRef] [PubMed]
- Ruinemas-Koerts, J.; Schmidt-Hieltjes, Y.; Jansen, A.; Savelkoul, H.F.J.; Plaisier, A.; van Setten, P. The Basophil Activation Test reduces the need for a food challenge test in children suspected of IgE-mediated cow′s milk allergy. Clin. Exp. Allergy 2019, 49, 350–356. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
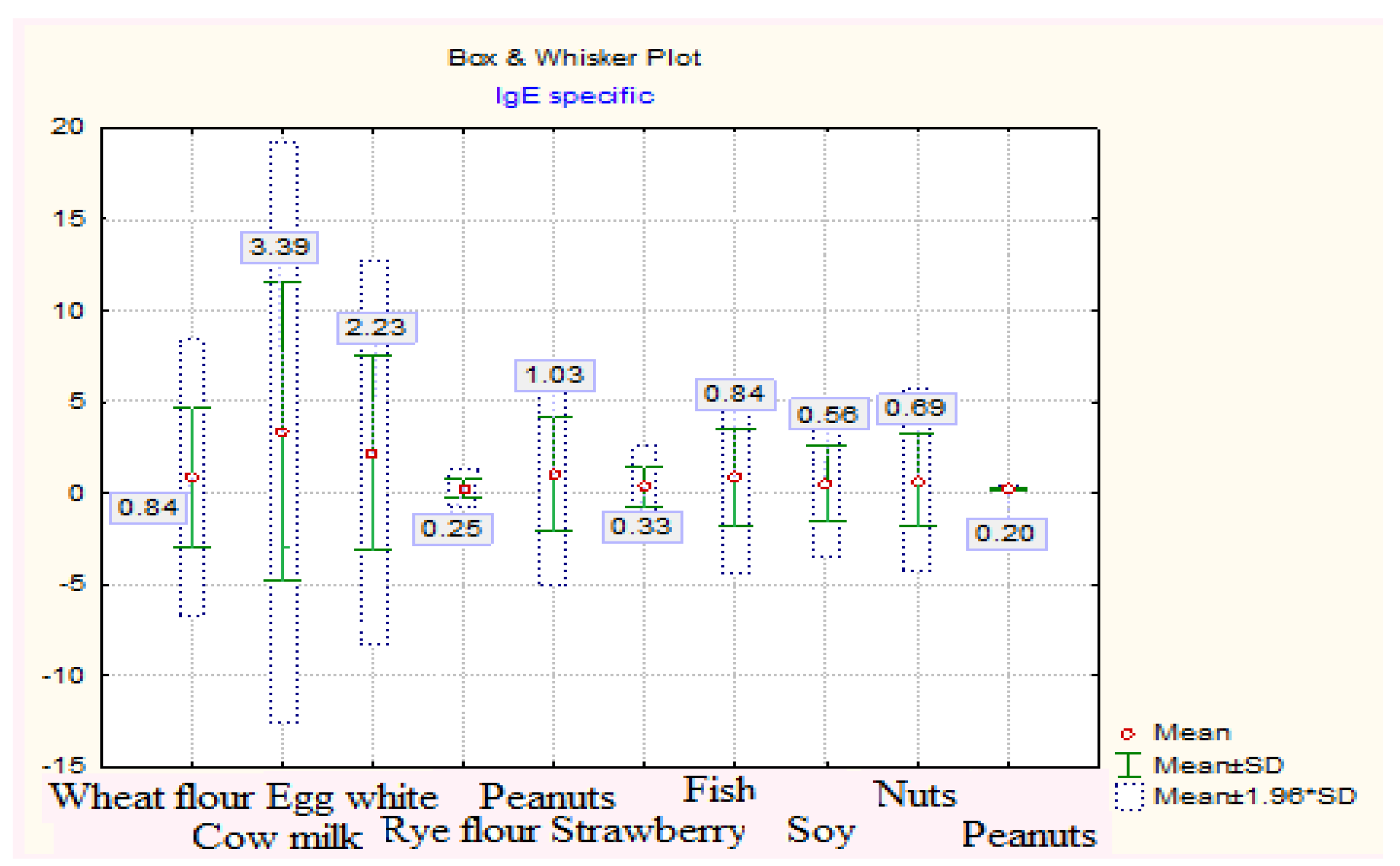
| Title Allergen | Average IgE Specific | Media | Dev.std | Er.std | Min | Max | Q25 | Median | Q75 | |
|---|---|---|---|---|---|---|---|---|---|---|
| −95% | +95% | |||||||||
| wheat flour | 0.84 | 0.18 | 1.50 | 3.83 | 0.33 | 0.10 | 36.30 | 0.15 | 0.19 | 0.27 |
| Cow’s milk | 3.39 | 1.99 | 4.79 | 8.11 | 0.71 | 0.10 | 51.30 | 0.14 | 0.20 | 0.31 |
| egg white | 2.23 | 1.31 | 3.16 | 5.36 | 0.47 | 0.10 | 21.60 | 0.16 | 0.20 | 0.30 |
| rye flour | 0.25 | 0.16 | 0.35 | 0.55 | 0.05 | 0.10 | 6.50 | 0.15 | 0.19 | 0.27 |
| hazelnuts | 1.03 | 0.50 | 1.56 | 3.08 | 0.27 | 0.10 | 16.80 | 0.14 | 0.18 | 0.27 |
| strawberries | 0.33 | 0.14 | 0.52 | 1.12 | 0.10 | 0.10 | 11.50 | 0.14 | 0.18 | 0.27 |
| fish | 0.84 | 0.38 | 1.30 | 2.67 | 0.23 | 0.10 | 16.20 | 0.15 | 0.18 | 0.28 |
| soy | 0.56 | 0.21 | 0.92 | 2.07 | 0.18 | 0.10 | 18.90 | 0.15 | 0.19 | 0.25 |
| nuts | 0.69 | 0.26 | 1.13 | 2.52 | 0.22 | 0.10 | 21.50 | 0.14 | 0.19 | 0.27 |
| peanuts | 0.20 | 0.19 | 0.22 | 0.07 | 0.01 | 0.10 | 0.35 | 0.14 | 0.19 | 0.27 |
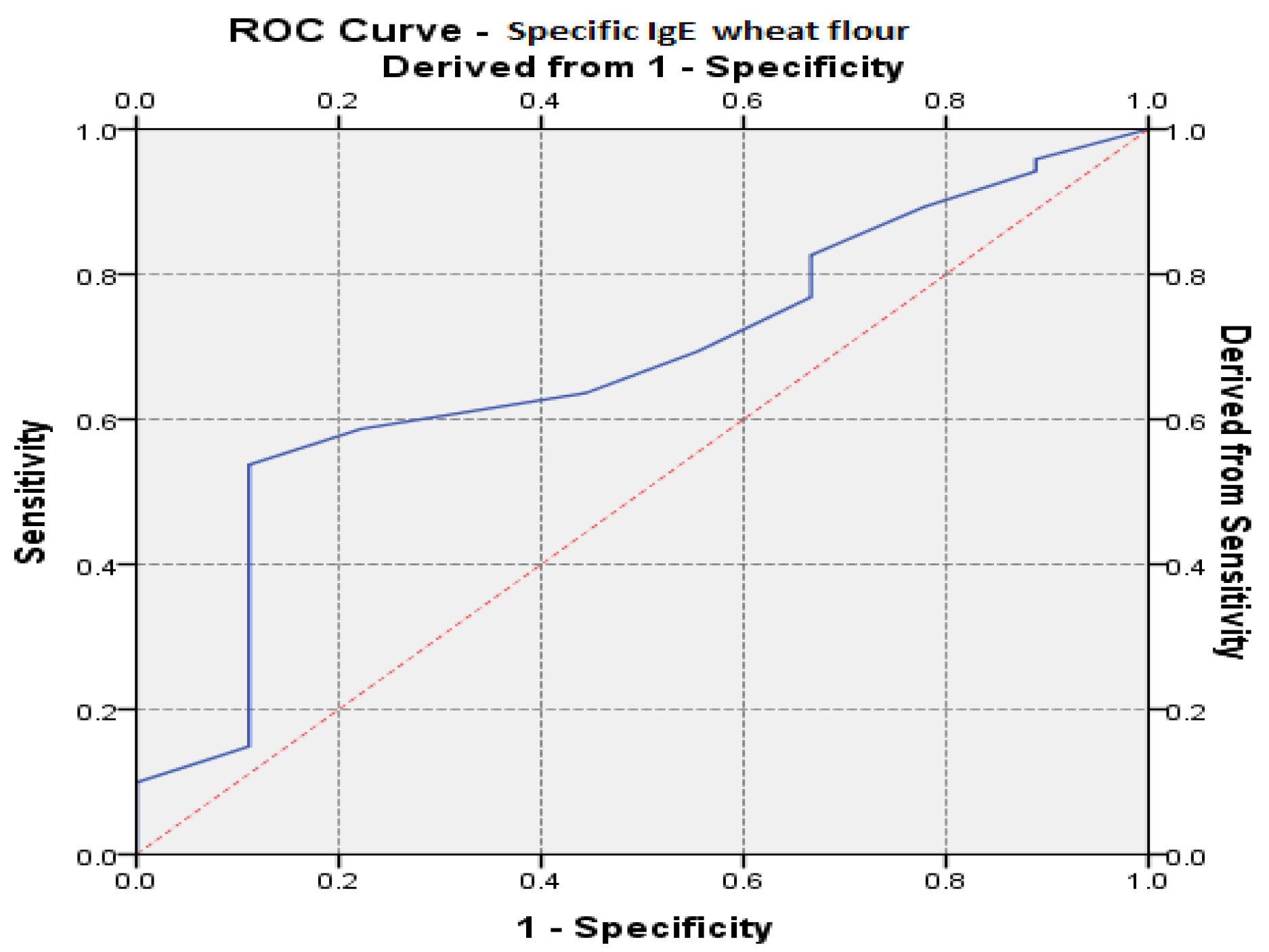
| Area under the ROC Curve | |||||
|---|---|---|---|---|---|
| Variables Tested Factors | Area under the Curve (AUC) | Standard Error | Level of Significance. b (p) | AUC 95% Reference Interval | |
| Inf. Limit | Upper Limit | ||||
| Specific IgE-wheat flour | 0.674 | 0.085 | 0.0383 | 0.507 | 0.840 |
| t-Test for Dependent Samples | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mean | Std.Dv. | N | Diff. | Std.Dv.-Diff. | t | df | p | |
| Wheat flour | 15.29259 | 11.73761 | ||||||
| Wheat flour 2 | 8.63333 | 8.15867 | 27 | 6.659259 | 4.347524 | 7.959133 | 26 | 0.000000 |
| Egg white | 14.92222 | 4.874128 | ||||||
| Egg white 2 | 9.71667 | 4.505585 | 18 | 5.205556 | 2.377213 | 9.290416 | 17 | 0.000000 |
| t-Test for Dependent Samples | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mean | Std.Dv. | N | Diff. | Std.Dv.-Diff. | t | df | p | |
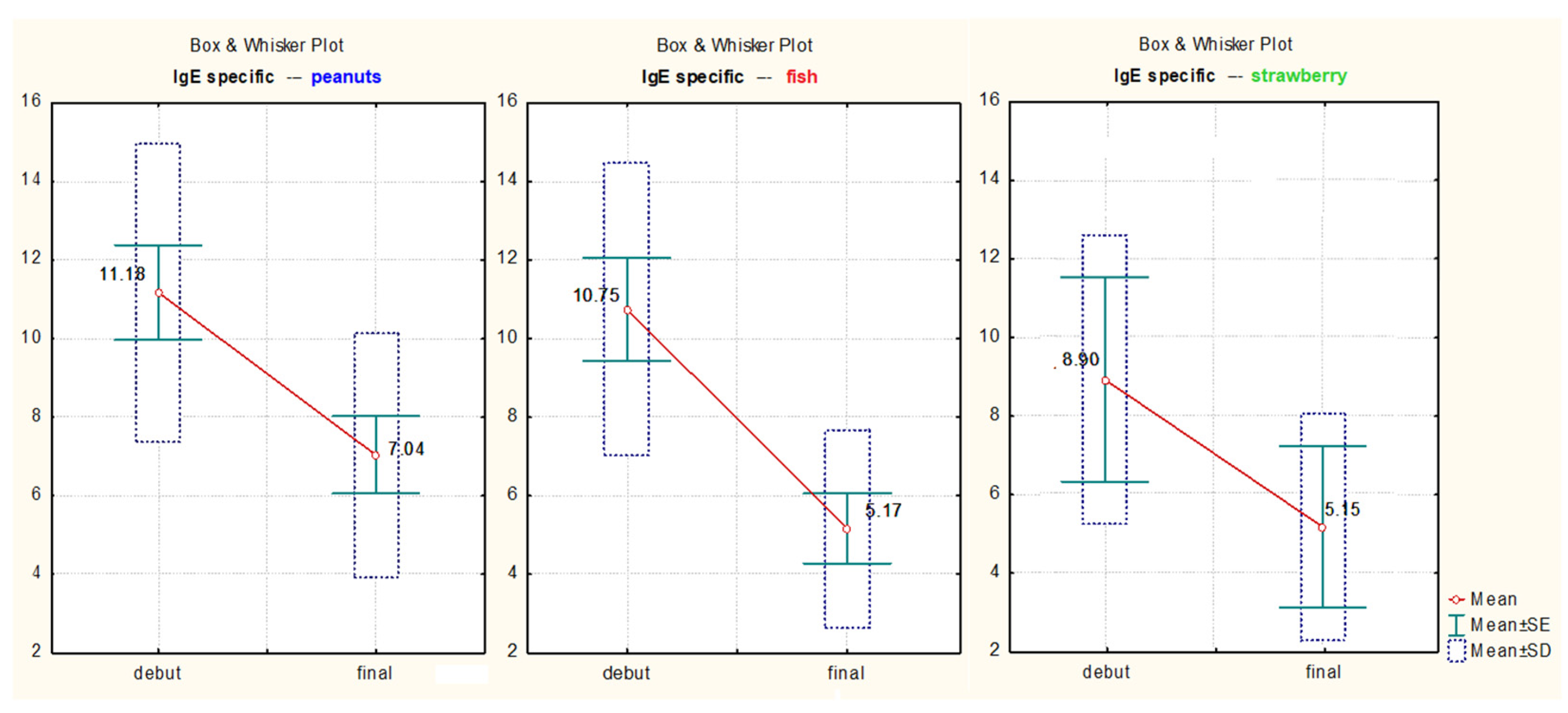
| hazelnuts | 11.18000 | 3.808120 | ||||||
| hazelnuts 2 | 7.04000 | 3.115267 | 10 | 4.140000 | 1.455411 | 8.995278 | 9 | 0.000009 |
| strawberries | 8.900000 | 3.676955 | ||||||
| strawberries 2 | 5.150000 | 2.899138 | 2 | 3.750000 | 0.777817 | 9.818182 | 1 | 0.022710 |
| fish | 10.75000 | 3.722135 | ||||||
| fish 2 | 5.17500 | 2.518361 | 8 | 5.575000 | 2.554408 | 6.173047 | 7 | 0.000457 |
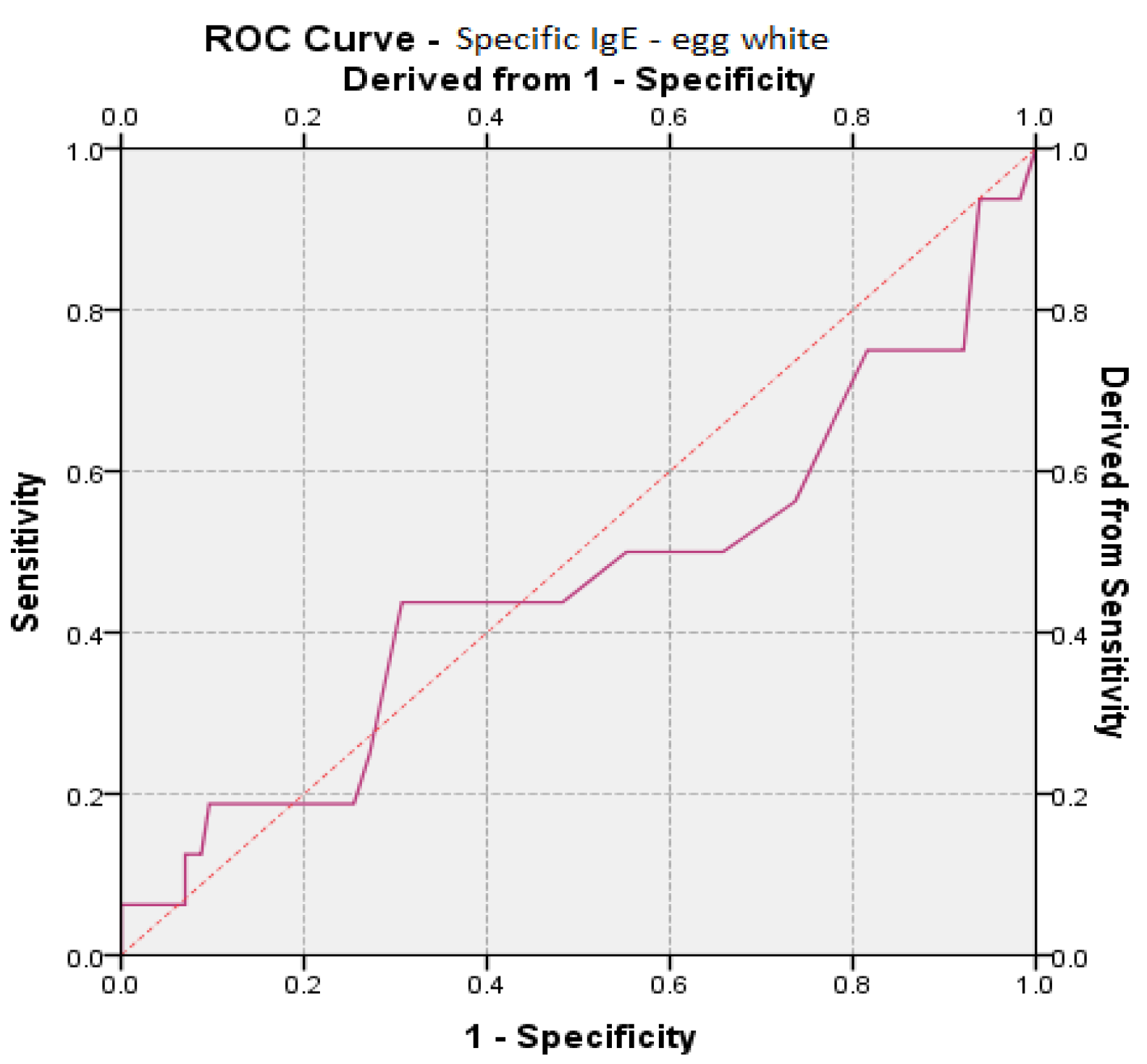
| Area under the ROC Curve | |||||
|---|---|---|---|---|---|
| Variables Tested Factors | Area under the Curve (AUC) | Standard Error | Level of Significance. b (p) | AUC 95% Reference Interval | |
| Inf. Limit | Upper Limit | ||||
| Specific IgE-egg white | 0.461 | 0.088 | 0.617 | 0.289 | 0.633 |
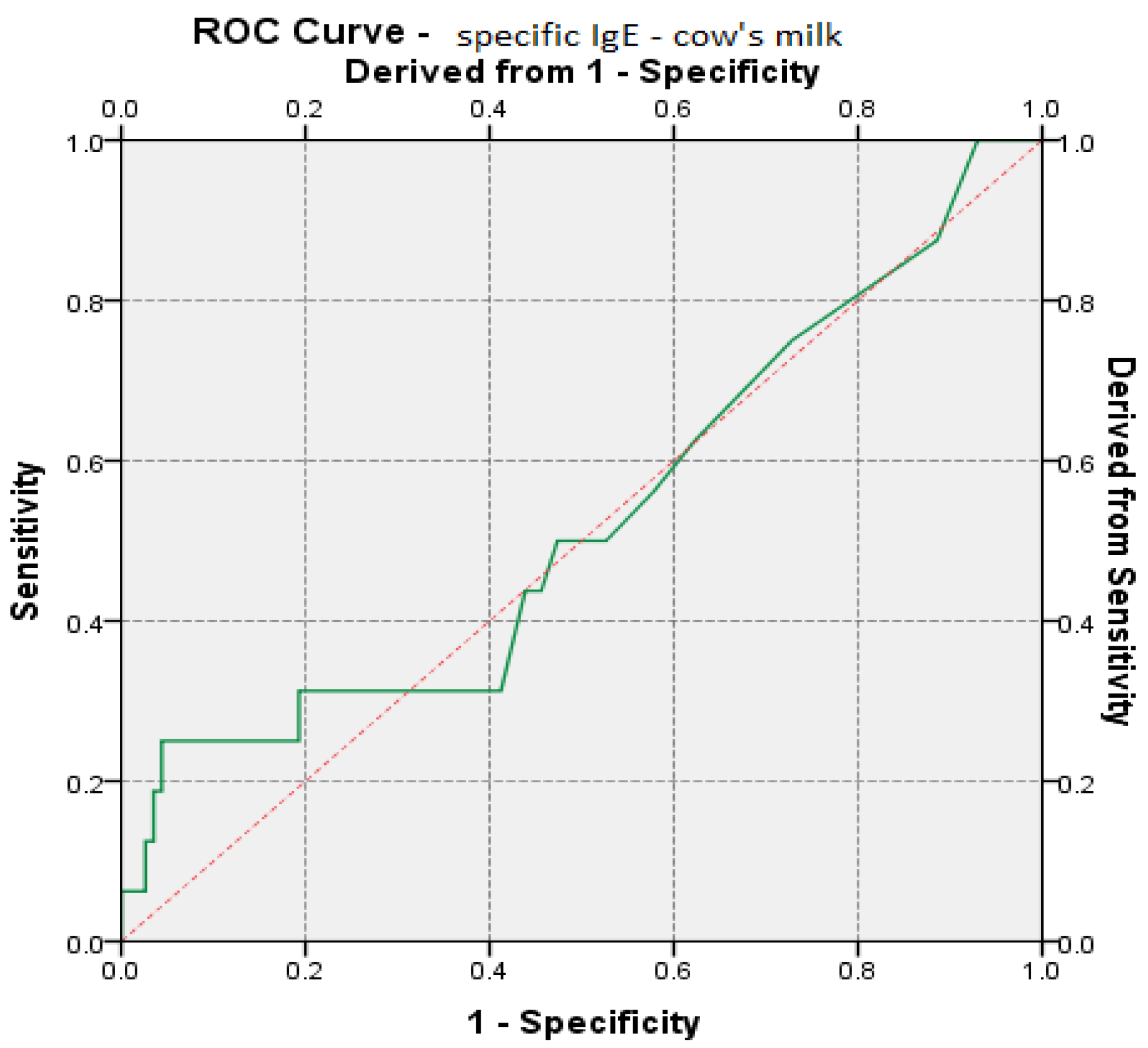
| Area under the ROC Curve | |||||
|---|---|---|---|---|---|
| Variables Tested Factors | Area under the Curve (AUC) | Standard Error | Level of Significance. b (p) | AUC 95% Reference Interval | |
| Inf. Limit | Upper Limit | ||||
| specific IgE-cow’s milk | 0.528 | 0.083 | 0.715 | 0.366 | 0.691 |
| t-Test for Dependent Samples | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mean | Std.Dv. | N | Diff. | Std.Dv.-Diff. | t | df | p | |
| rye flour | 6.5 | 0.02 | ||||||
| rye flour 2 | 3.2 | 0.07 | 3.300000 | 2.377213 | 5.6415 | 1 | 0.0254 | |
| soy | 8.266667 | 6.137643 | ||||||
| soy 2 | 4.116667 | 3.619622 | 6 | 4.150000 | 2.893959 | 3.512621 | 5 | 0.017053 |
| nuts | 11.10000 | 5.445365 | ||||||
| nuts 2 | 5.43333 | 2.919361 | 6 | 5.666667 | 2.665833 | 5.206793 | 5 | 0.003448 |
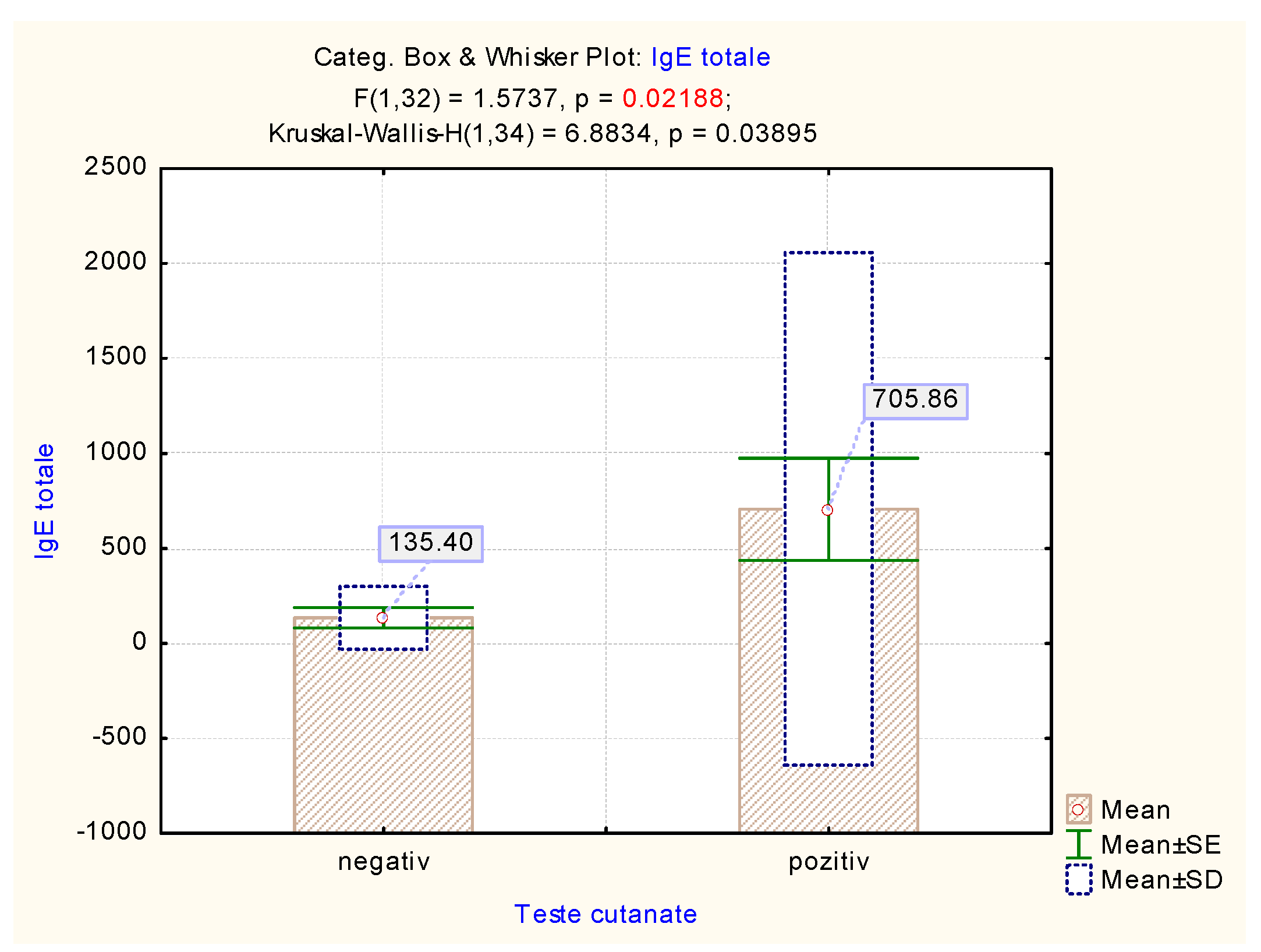
| Kruskal–Wallis Test | H (95% Confidence Interval) | p |
| 6.8834 | 0.03895 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ungureanu, M.I.; Sachelarie, L.; Ciorap, R.; Stana, B.A.; Croitoru, I.; Popa, T.O. The Importance of Diet in Predicting the Remission of Urticaria—Determination of Allergen-Specific IgE. Medicina 2021, 57, 679. https://doi.org/10.3390/medicina57070679
Ungureanu MI, Sachelarie L, Ciorap R, Stana BA, Croitoru I, Popa TO. The Importance of Diet in Predicting the Remission of Urticaria—Determination of Allergen-Specific IgE. Medicina. 2021; 57(7):679. https://doi.org/10.3390/medicina57070679
Chicago/Turabian StyleUngureanu, Monica Iuliana, Liliana Sachelarie, Radu Ciorap, Bogdan Aurelian Stana, Irina Croitoru, and Tudor Ovidiu Popa. 2021. "The Importance of Diet in Predicting the Remission of Urticaria—Determination of Allergen-Specific IgE" Medicina 57, no. 7: 679. https://doi.org/10.3390/medicina57070679
APA StyleUngureanu, M. I., Sachelarie, L., Ciorap, R., Stana, B. A., Croitoru, I., & Popa, T. O. (2021). The Importance of Diet in Predicting the Remission of Urticaria—Determination of Allergen-Specific IgE. Medicina, 57(7), 679. https://doi.org/10.3390/medicina57070679