
A Case of COVID-19 Pregnancy Complicated with Hydrops Fetalis and Intrauterine Death

 ,
, 

Abstract
:1. Introduction
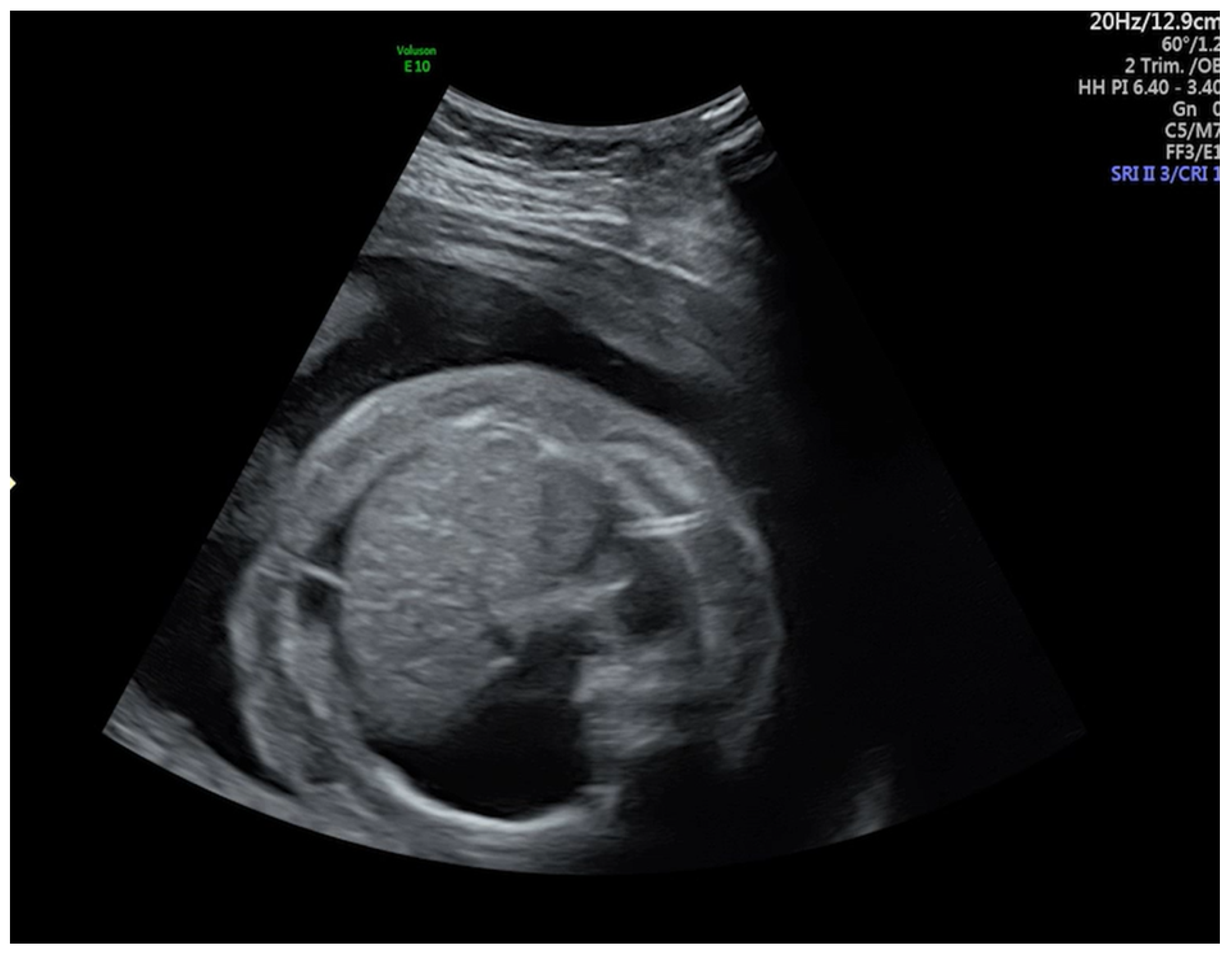
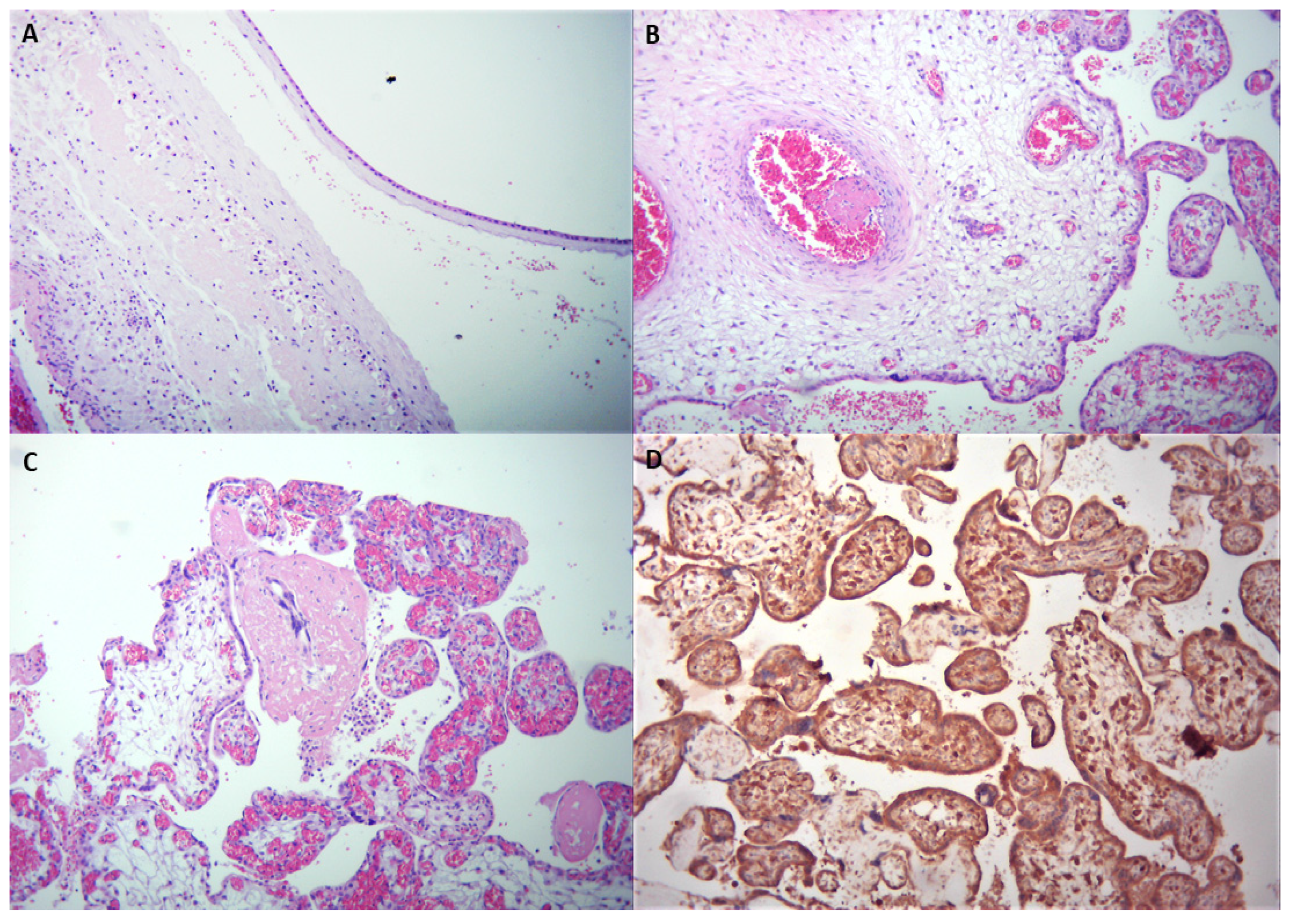
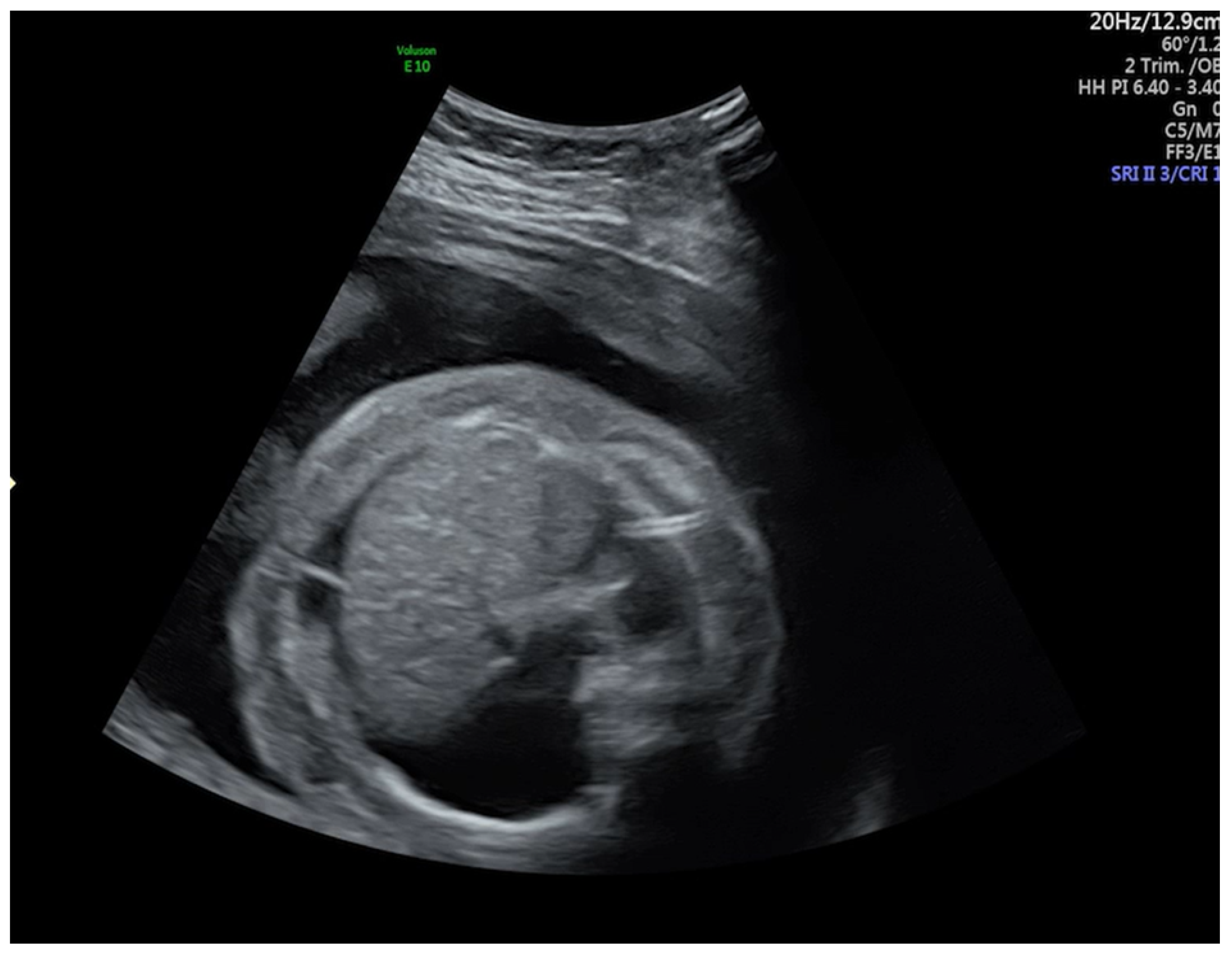
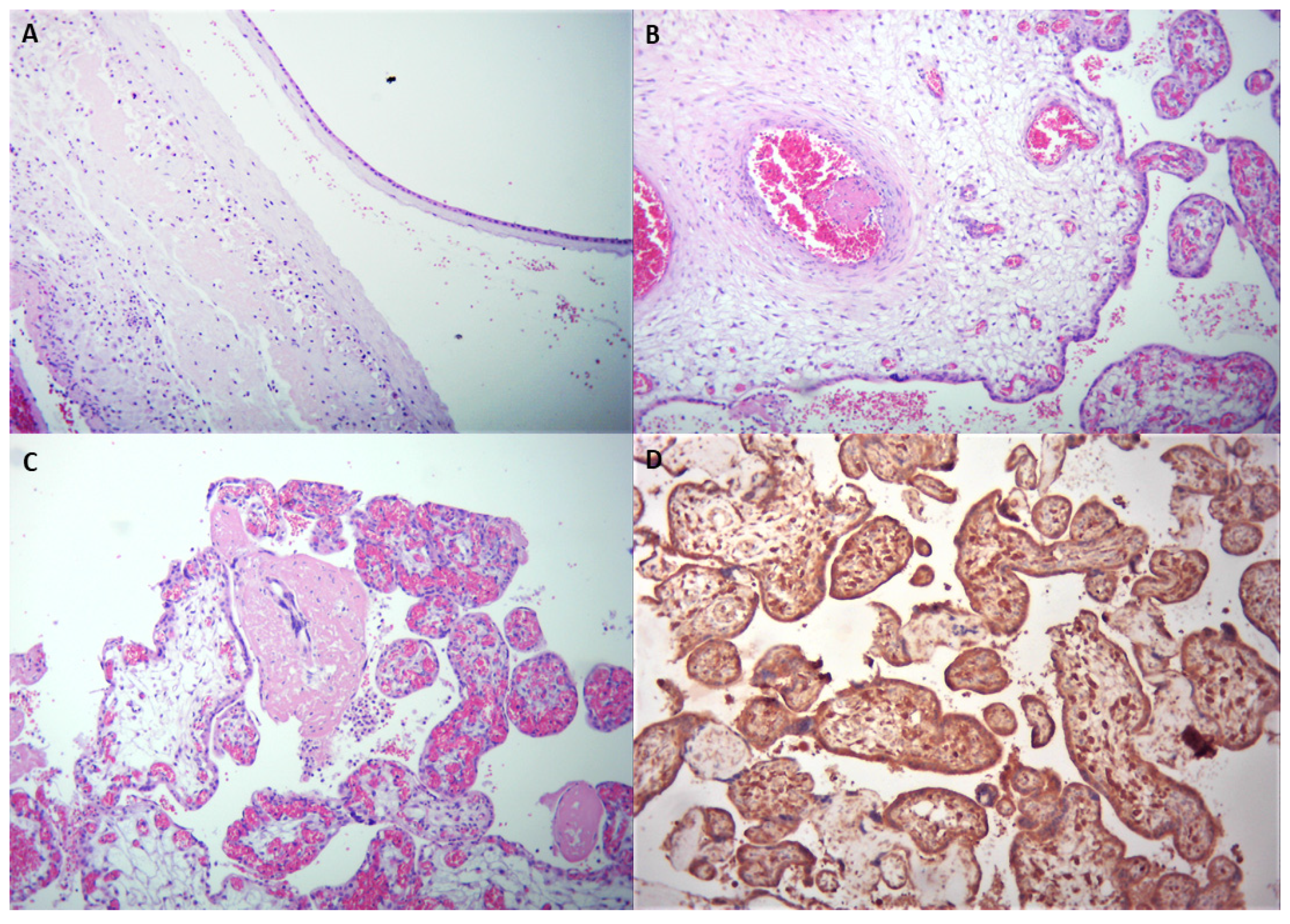
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Di Mascio, D.; Khalil, A.; Saccone, G.; Rizzo, G.; Buca, D.; Liberati, M.; Vecchiet, J.; Nappi, L.; Scambia, G.; Berghella, V.; et al. Outcome of coronavirus spectrum infections (SARS, MERS, COVID-19) during pregnancy: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2020, 2, 100107. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Graham, A.L. Potential Maternal and Infant Outcomes from (Wuhan) Coronavirus 2019-nCoV Infecting Pregnant Women: Lessons from SARS, MERS, and Other Human Coronavirus Infections. Viruses 2020, 12, 194. [Google Scholar] [CrossRef] [Green Version]
- Yan, J.; Guo, J.; Fan, C.; Juan, J.; Yu, X.; Li, J.; Feng, L.; Li, C.; Chen, H.; Qiao, Y.; et al. Coronavirus disease 2019 in pregnant women: A report based on 116 cases. Am. J. Obstet. Gynecol. 2020, 223, 111.e1–111.e14. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.A.; Dhaliwal, A. Infections in pregnancy with COVID-19 and other respiratory RNA virus diseases are rarely, if ever, transmitted to the fetus: Experiences with coronaviruses, HPIV, HMPV RSV, and Influenza. Arch. Pathol. Lab. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Delahoy, M.J.; Whitaker, M.; O’Halloran, A.; Chai, S.J.; Kirley, P.D.; Alden, N.; Kawasaki, B.; Meek, J.; Yousey-Hindes, K.; Anderson, E.J.; et al. Characteristics and Maternal and Birth Outcomes of Hospitalized Pregnant Women with Laboratory-Confirmed COVID-19—COVID-NET, 13 States, 1 March–22 August 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakopoulos, L.; Myers, T.R.; Gee, J.; Lipkind, H.S.; Kharbanda, E.O.; Ryan, D.S.; Williams, J.T.B.; Naleway, A.L.; Klein, N.P.; Hambidge, S.J.; et al. SARS-CoV-2 Infection Among Hospitalized Pregnant Women: Reasons for Admission and Pregnancy Characteristics—Eight U.S. Health Care Centers, 1 March–30 May 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1355–1359. [Google Scholar] [CrossRef]
- CDC. Stillbirth Homepage. Data and Statistics. Available online: https://www.cdc.gov/ncbddd/stillbirth/facts.html (accessed on 11 September 2020).
- Facchetti, F.; Bugatti, M.; Drera, E.; Tripodo, C.; Sartori, E.; Cancila, V.; Papaccio, M.; Castellani, R.; Casola, S.; Boniotti, M.B.; et al. SARS-CoV2 vertical transmission with adverse effects on the newborn revealed through integrated immunohistochemical, electron microscopy and molecular analyses of Placenta. EBioMedicine 2020, 59, 102951. [Google Scholar] [CrossRef]
- Shook, L.L.; Collier, A.Y.; Goldfarb, I.T.; Diouf, K.; Akinwunmi, B.O.; Young, N.; Brown, A.; Hacker, M.R.; Kaimal, A.M.; Gray, K.J.; et al. Vertical transmission of SARS-CoV-2: Consider the denominator. Am. J. Obstet. Gynecol. MFM 2021, 28, 100386. [Google Scholar] [CrossRef]
- Linehan, L.; O’Donoghue, K.; Dineen, S.; White, J.; Higgins, J.R.; Fitzgerald, B. SARS-CoV-2 placentitis: An uncommon complication of maternal COVID-19. Placenta 2021, 104, 261–266. [Google Scholar] [CrossRef]
- Komine-Aizawa, S.; Takada, K.; Hayakawa, S. Placental barrier against COVID-19. Placenta 2020, 99, 45–49. [Google Scholar] [CrossRef]
- Poisson, T.M.; Pierone, G., Jr. Placental pathology and fetal demise at 35 weeks of gestation in a woman with SARS-CoV-2 infection: A case report. Case Rep. Women’s Health 2021, 30, e00289. [Google Scholar] [CrossRef] [PubMed]
- Baergen, R.N.; Heller, D.S. Placental pathology in covid-19 positive mothers: Preliminary findings. Pediatr. Dev. Pathol. 2020, 23, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Menter, T.; Mertz, K.D.; Jiang, S.; Chen, H.; Monod, C.; Tzankov, A.; Waldvogel, S.; Schulzke, S.M.; Hösli, I.; Bruder, E. Placental Pathology Findings during and after SARS-CoV-2 Infection: Features of Villitis and Malperfusion. Pathobiology 2021, 88, 69–77. [Google Scholar] [CrossRef]
- Bertero, L.; Borella, F.; Botta, G.; Carosso, A.; Cosma, S.; Bovetti, M.; Carosso, M.; Abboma, G.; Collemi, G.; Papotti, M.; et al. Placenta histopathology in SARS-CoV-2 infection: Analysis of a consecutive series and comparison with control cohorts. Virchows Arch. 2021, 1–14. [Google Scholar] [CrossRef]
- Birindwa, E.K.; Mulumeoderhwa, G.M.; Nyakio, O.; Mbale, G.M.; Mushamuka, S.Z.; Materanya, J.M.; Kahasha, P.M.; Bisimwa, Y.K.; Kampara, F.M.; Irenge, J.M.; et al. A case study of the first pregnant woman with COVID-19 in Bukavu, eastern Democratic Republic of the Congo. Matern. Health Neonatol. Perinatol. 2021, 20, 7. [Google Scholar] [CrossRef]
- Richtmann, R.; Torloni, M.R.; Oyamada Otani, A.R.; Levi, J.E.; Crema Tobara, M.; de Almeida Silva, C.; Dias, L.; Miglioli-Galvao, L.; Martins Silva, P.; Macoto Kondo, M. Fetal deaths in pregnancies with SARS-CoV-2 infection in Brazil: A case series. Case Rep. Women’s Health 2020, 27, e00243. [Google Scholar] [CrossRef]
- Baud, D.; Greub, G.; Favre, G.; Gengler, C.; Jaton, K.; Dubruc, E. Second-trimester miscarriage in a pregnant woman with SARS-CoV-2 infection. JAMA J. Am. Med. Assoc. 2020, 323, 2198–2200. [Google Scholar] [CrossRef] [PubMed]
- Shanes, E.D.; Mithal, L.B.; Otero, S.; Azad, H.A.; Miller, E.S.; Goldstein, J.A. Placental Pathology in COVID-19. Am. J. Clin. Pathol. 2020, 154, 23–32. [Google Scholar] [CrossRef]
- Ferraiolo, A.; Barra, F.; Kratochwila, C.; Paudice, M.; Vellone, V.G.; Godano, E.; Varesano, S.; Noberasco, G.; Ferrero, S.; Arioni, C. Report of Positive Placental Swabs for SARS-CoV-2 in an Asymptomatic Pregnant Woman with COVID-19. Medicina 2020, 56, 306. [Google Scholar] [CrossRef]
- Martínez-Varea, A.; Desco-Blay, J.; Monfort, S.; Hueso-Villanueva, M.; Perales-Marín, A.; Diago-Almela, V.J. Transitory Fetal Skin Edema in a Pregnant Patient with a Mild SARS-CoV-2 Infection. Case Rep. Obstet. Gynecol. 2021, 16, 5552877. [Google Scholar] [CrossRef]
- Garcia-Manau, P.; Garcia-Ruiz, I.; Rodo, C.; Sulleiro, E.; Maiz, N.; Catalan, M.; Fernández-Hidalgo, N.; Balcells, J.; Antón, A.; Carreras, E.; et al. Fetal Transient Skin Edema in Two Pregnant Women With Coronavirus Disease 2019 (COVID-19). Obstet. Gynecol. 2020, 136, 1016–1020. [Google Scholar] [CrossRef] [PubMed]
- Shende, P.; Gaikwad, P.; Gandhewar, M.; Ukey, P.; Bhide, A.; Patel, V.; Bhagat, S.; Bhor, V.; Mahale, S.; Gajbhiye, R.; et al. Persistence of SARS-CoV-2 in the first trimester placenta leading to transplacental transmission and fetal demise from an asymptomatic mother. Hum. Reprod. 2021, 36, 899–906. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | GA | Histopathological Findings | |
|---|---|---|---|
| FVM | Other Findings | ||
| Poisson et al. [12] | 35 weeks | Thrombosis, Avascular villi | Acute chorionitis, Maternal vascular malperfusion |
| Baergen et al. [13] | 33 weeks–40 weeks | Thrombosis, Fibrin deposition, Karyorrhexis, Chorangiosis | Maternal vascular malperfusion Intervillous thrombus, Focal increase in fibrin |
| Menter et al. [14] | 39 weeks–41 weeks | Thrombosis, Avascular villi, Chorangiosis, Delayed villous maturation | Chorioamnionitis, Chronic vilittis, Subchorionitis, Chronic deciduitis, Maternal vascular malperfusion |
| Bertero et al. [15] | 32 weeks–40 weeks | Thrombosis, Chorangiosis, Accelerated maturation, Fibrin deposition, Avascular villi | Chronic villitis, Intervillous hematoma, Maternal vascular malperfusion |
| Birindwa et al. [16] | 34 weeks | Thrombosis, Chorangiosis | |
| Richtmann et al. [17] | 21 weeks–38 weeks | Fibrin deposition | Chorioamnionitis, Chronic villitis, Acute deciduitis |
| Baud et al. [18] | 19 weeks | Subchorionitis, Funisitis | |
| Shanes et al. [19] | 33 weeks–40 weeks | Fetal vessel mural fibrin, Avascular villi, Delayed villous maturation, Chorangiosis | Maternal vascular malperfusion |
| Ferraiolo et al. [20] | Microchorangiosis, Fibrin deposition | Subchorionitis, Intervillous hemorrhages | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popescu, D.E.; Cioca, A.; Muresan, C.; Navolan, D.; Gui, A.; Pop, O.; Marcovici, T.; Ilie, C.; Craina, M.; Boia, M. A Case of COVID-19 Pregnancy Complicated with Hydrops Fetalis and Intrauterine Death. Medicina 2021, 57, 667. https://doi.org/10.3390/medicina57070667
Popescu DE, Cioca A, Muresan C, Navolan D, Gui A, Pop O, Marcovici T, Ilie C, Craina M, Boia M. A Case of COVID-19 Pregnancy Complicated with Hydrops Fetalis and Intrauterine Death. Medicina. 2021; 57(7):667. https://doi.org/10.3390/medicina57070667
Chicago/Turabian StylePopescu, Daniela Eugenia, Andreea Cioca, Cezara Muresan, Dan Navolan, Arina Gui, Ovidiu Pop, Tamara Marcovici, Constantin Ilie, Marius Craina, and Marioara Boia. 2021. "A Case of COVID-19 Pregnancy Complicated with Hydrops Fetalis and Intrauterine Death" Medicina 57, no. 7: 667. https://doi.org/10.3390/medicina57070667
APA StylePopescu, D. E., Cioca, A., Muresan, C., Navolan, D., Gui, A., Pop, O., Marcovici, T., Ilie, C., Craina, M., & Boia, M. (2021). A Case of COVID-19 Pregnancy Complicated with Hydrops Fetalis and Intrauterine Death. Medicina, 57(7), 667. https://doi.org/10.3390/medicina57070667