
Early Surgery Does Not Improve Outcomes for Patients with Periprosthetic Femoral Fractures—Results from the Registry for Geriatric Trauma of the German Trauma Society

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. ATR-DGU
2.2. Aim of the Study and Outcome Parameters
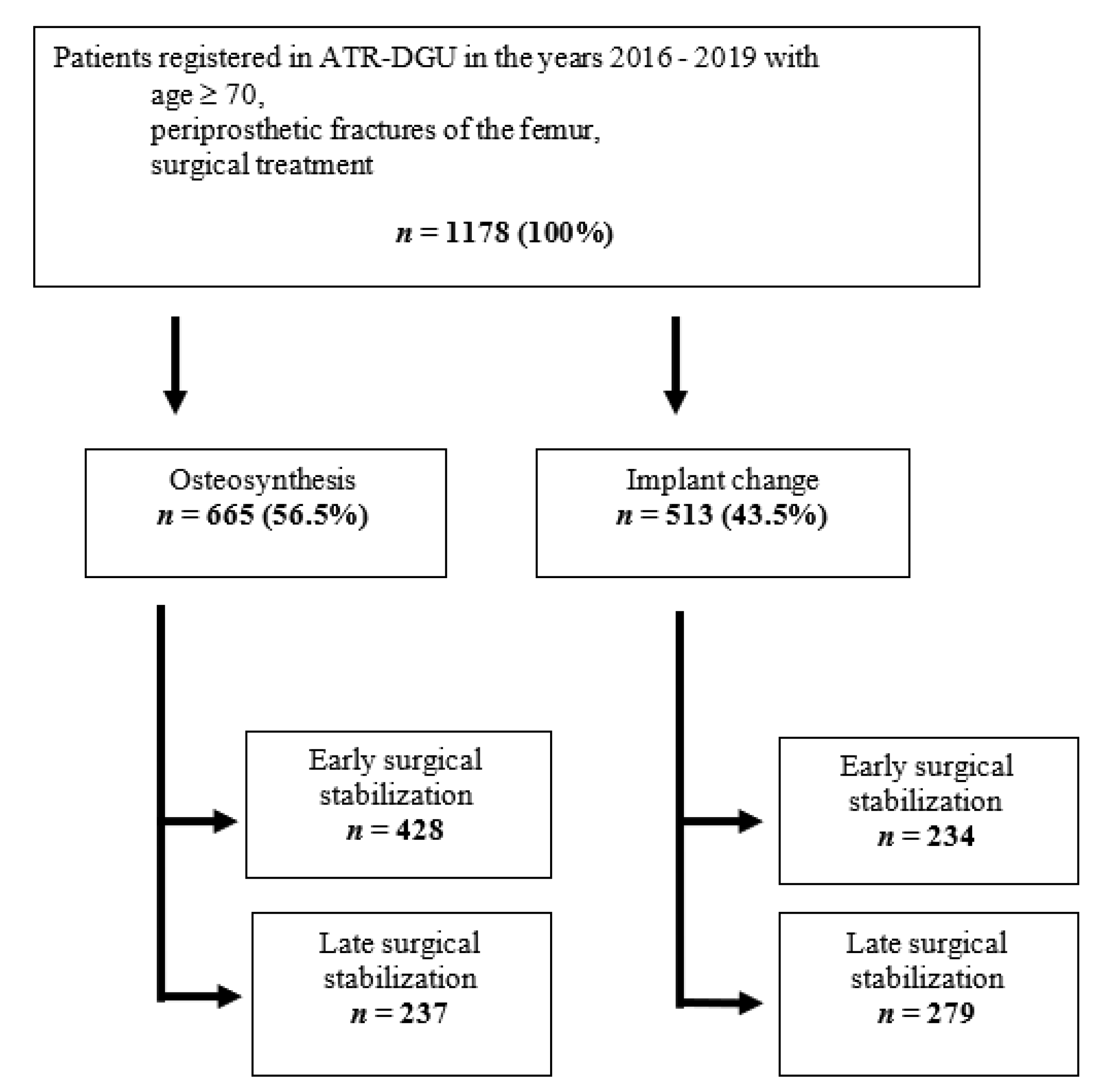
2.3. Inclusion and Exclusion Criteria
2.4. Statistical Analysis
3. Results
3.1. Acute Care Data
3.2. 120 Days Follow-Up Data
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ramavath, A.; Lamb, J.N.; Palan, J.; Pandit, H.G.; Jain, S. Postoperative periprosthetic femoral fracture around total hip replacements: Current concepts and clinical outcomes. EFORT Open Rev. 2020, 5, 558–567. [Google Scholar] [CrossRef] [PubMed]
- Eschbach, D.; Buecking, B.; Kivioja, H.; Fischer, M.; Wiesmann, T.; Zettl, R.; Oberkircher, L.; Barthel, J.; Aigner, R.; Ruchholtz, S.; et al. One year after proximal or distal periprosthetic fracture of the femur-two conditions with divergent outcomes? Injury 2018, 49, 1176–1182. [Google Scholar] [CrossRef]
- Bliemel, C.; Sielski, R.; Doering, B.; Dodel, R.; Balzer-Geldsetzer, M.; Ruchholtz, S.; Buecking, B. Pre-fracture quality of life predicts 1-year survival in elderly patients with hip fracture—development of a new scoring system. Osteoporos. Int. 2016, 27, 1979–1987. [Google Scholar] [CrossRef] [PubMed]
- Bäumlein, M.; Klasan, A.; Klötzer, C.; Bockmann, B.; Eschbach, D.; Knobe, M.; Bücking, B.; Ruchholtz, S.; Bliemel, C. Cement augmentation of an angular stable plate osteosynthesis for supracondylar femoral fractures—Biomechanical investigation of a new fixation device. BMC Musculoskelet. Disord. 2020, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.R.; Halliday, R.; Aquilina, A.L.; Morrison, R.J.; Yip, G.C.; McArthur, J.; Hull, P.; Gray, A.; Kelly, M.B.; Collaborative—Orthopaedic Trauma Society (OTS). Distal femoral fractures: The need to review the standard of care. Injury 2015, 46, 1084–1088. [Google Scholar] [CrossRef] [PubMed]
- Bliemel, C.; Oberkircher, L.; Eschbach, D.A.; Struewer, J.; Ruchholtz, S.; Buecking, B. Surgical treatment of proximal femoral fractures--a training intervention? Z. Orthop. Unfall. 2013, 151, 180–188. [Google Scholar]
- Bliemel, C.; Buecking, B.; Oberkircher, L.; Knobe, M.; Ruchholtz, S.; Eschbach, D. The impact of pre-existing conditions on functional outcome and mortality in geriatric hip fracture patients. Int. Orthop. 2017, 41, 1995–2000. [Google Scholar] [CrossRef]
- Bliemel, C.; Oberkircher, L.; Eschbach, D.-A.; Lechler, P.; Balzer-Geldsetzer, M.; Ruchholtz, S.; Buecking, B. Impact of Parkinson’s disease on the acute care treatment and medium-term functional outcome in geriatric hip fracture patients. Arch. Orthop. Trauma Surg. 2015, 135, 1519–1526. [Google Scholar] [CrossRef]
- Bennett, A.; Li, H.; Patel, A.; Kang, K.; Gupta, P.; Choueka, J.; Feierman, D.E. Retrospective Analysis of Geriatric Patients Undergoing Hip Fracture Surgery: Delaying Surgery Is Associated With Increased Morbidity, Mortality, and Length of Stay. Geriatr. Orthop. Surg. Rehabili. 2018, 9. [Google Scholar] [CrossRef]
- Myers, P.; Laboe, P.; Johnson, K.J.; Fredericks, P.D.; Crichlow, R.J.; Maar, D.C.; Weber, T.G. Patient Mortality in Geriatric Distal Femur Fractures. J. Orthop. Trauma 2018, 32, 111–115. [Google Scholar] [CrossRef]
- Schoeneberg, C.; Aigner, R.; Pass, B.; Volland, R.; Eschbach, D.; Peiris, S.E.; Ruchholtz, S.; Lendemans, S. Effect of time-to-surgery on in-house mortality during orthogeriatric treatment following hip fracture: A retrospective analysis of prospectively collected data from 16,236 patients of the AltersTraumaRegister DGU®. Injury 2021, 52, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Liener, U.; Becker, C.; Rapp, K. Weissbuch Alterstraumatologie: W; Kohlhammer Verlag: Stuttgart, Germany, 2018. [Google Scholar]
- Scott, B.L.; King, C.A.; Lee, C.S.; Lee, M.J.; Su, E.P.; Landy, D.C. Periprosthetic Hip Fractures Outside the Initial Postoperative Period: Does Time from Diagnosis to Surgery Matter? Arthroplast. Today 2020, 6, 628–633.e0. [Google Scholar] [CrossRef]
- Jennison, T.; Yarlagadda, R. Mortality in patients sustaining a periprosthetic fracture following a hemiarthroplasty. J. Orthop. 2018, 15, 798–801. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, E.J.; Cash, D.J.; Kalra, S.; Hopgood, P.J. Time to surgery and 30-day morbidity and mortality of periprosthetic hip fractures. Injury 2013, 44, 1949–1952. [Google Scholar] [CrossRef] [PubMed]
- Bovonratwet, P.; Fu, M.C.; Adrados, M.; Ondeck, N.T.; Su, E.P.; Grauer, J.N. Unlike Native Hip Fractures, Delay to Periprosthetic Hip Fracture Stabilization Does Not Significantly Affect Most Short-Term Perioperative Outcomes. J. Arthroplast. 2019, 34, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Boddapati, V.; Grosso, M.J.; Sarpong, N.O.; Geller, J.A.; Cooper, H.J.; Shah, R.P. Early Morbidity but Not Mortality Increases With Surgery Delayed Greater Than 24 Hours in Patients With a Periprosthetic Fracture of the Hip. J. Arthroplast. 2019, 34, 2789–2792.e1. [Google Scholar] [CrossRef]
- Bhattacharyya, T.; Chang, D.; Meigs, J.B.; Estok, D.M.; Malchau, H. Mortality after Periprosthetic Fracture of the Femur. J. Bone Jt. Surg. Am. 2007, 89, 2658–2662. [Google Scholar] [CrossRef]
- Sellan, M.E.; Lanting, B.A.; Schemitsch, E.H.; MacDonald, S.J.; Vasarhelyi, E.M.; Howard, J.L. Does Time to Surgery Affect Outcomes for Periprosthetic Femur Fractures? J. Arthroplast. 2018, 33, 878–881. [Google Scholar] [CrossRef]
- Lee, S.R.; Shrestha, K.; Staggers, J.; Li, P.; Naranje, S.M.; Shah, A. Impact of time to surgery from injury on postoperative infection and deep vein thrombosis in periprosthetic knee fractures. Chin. J. Traumatol. 2018, 21, 329–332. [Google Scholar] [CrossRef]
- McCusker, J.; Bellavance, F.; Cardin, S.; Trepanier, S.; Verdon, J.; Ardman, O. Detection of Older People at Increased Risk of Adverse Health Outcomes After an Emergency Visit: The ISAR Screening Tool. J. Am. Geriatr. Soc. 1999, 47, 1229–1237. [Google Scholar] [CrossRef]
- Farrow, L.; Ablett, A.D.; Sargeant, H.W.; Smith, T.O.; Johnston, A.T. Does early surgery improve outcomes for periprosthetic fractures of the hip and knee? A systematic review and meta-analysis. Arch. Orthop. Trauma Surg. 2021. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Boddapati, V.; Held, M.B.; Lee, N.J.; Geller, J.A.; Cooper, H.J.; Shah, R.P. Is the time to revision surgery after peri-prosthetic fracture of the knee associated with increased rates of post-operative complications? Arthroplast. Today 2019, 5, 348–351. [Google Scholar] [CrossRef]
- Hoellwarth, J.S.; Fourman, M.S.; Crossett, L.; Goodman, M.; Siska, P.; Moloney, G.B.; Tarkin, I.S. Equivalent mortality and complication rates following periprosthetic distal femur fractures managed with either lateral locked plating or a distal femoral replacement. Injury 2018, 49, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Prestmo, A.; Hagen, G.; Sletvold, O.; Helbostad, J.L.; Thingstad, P.; Taraldsen, K.; Lydersen, S.; Halsteinli, V.; Saltnes, T.; Lamb, S.E.; et al. Comprehensive geriatric care for patients with hip fractures: A prospective, randomised, controlled trial. Lancet 2015, 385, 1623–1633. [Google Scholar] [CrossRef]
- Bliemel, C.; Bieneck, F.; Riem, S.; Hartwig, E.; Liener, U.C.; Ruchholtz, S.; Buecking, B. Subsequent treatment following proximal femoral fracture—who, when, where? Assessment of the current situation in Germany. Z. Orthop. Unfall. 2012, 150, 210–217. [Google Scholar] [CrossRef]
- Buecking, B.; Timmesfeld, N.; Riem, S.; Bliemel, C.; Hartwig, E.; Friess, T.; Liener, U.; Ruchholtz, S.; Eschbach, D. Early orthogeriatric treatment of trauma in the elderly: A systematic review and metaanalysis. Dtsch. Arztebl. Int. 2013, 110, 255–262. [Google Scholar]


{kind=link}
| Parameter | Subdivision | Osteosynthesis | Implant Change | p-Value |
|---|---|---|---|---|
| Number of patients | 665 | 513 | ||
| Gender | Male | 147 (22.3%) | 159 (31.0%) | 0.001 * |
| Female | 513 (77.7%) | 354 (69.0%) | ||
| Patient age (year) Median | 84 (79; 88) | 83 (79; 87) | 0.002 ** | |
| Time to surgery (h) Median | 27.0 (13.7; 69.7) | 57.1 (24.6; 106) | <0.001 ** | |
| ASA score | Unknown | 15 | 17 | 0.678 * |
| 1 | 4 (0.6%) | 4 (0.8%) | ||
| 2 | 130 (20.0%) | 109 (22.1%) | ||
| 3 | 453 (69.8%) | 331 (67.1%) | ||
| 4 and 5 | 62 (9.6%) | 49 (9.9%) | ||
| ISAR score | 0 | 32 (7.5%) | 24 (7.0%) | 0.012 * |
| 1 | 45 (10.6%) | 47 (13.6%) | ||
| 2 | 102 (24%) | 87 (25.2%) | ||
| 3 | 85 (20%) | 96 (27.8%) | ||
| 4 | 109 (25.6%) | 61 (17.7%) | ||
| 5 | 45 (10.6%) | 22 (6.4%) | ||
| 6 | 7 (1.7%) | 8 (2.3%) | ||
| Anticoagulatory drugs | Yes | 153 (23.3%) | 114 (22.6%) | 0.832 * |
| No | 503 (76.7%) | 390 (77.4%) | ||
| Prefracture residental status | At home | 492 (75.8%) | 408 (81.4%) | 0.040 * |
| Nursing home | 139 (21.4%) | 74 (14.8%) | ||
| Hospital | 12 (1.9%) | 14 (2.8%) | ||
| Other | 6 (0.9%) | 5 (1.0%) | ||
| Cocomitant fractures | Yes | 48 (7.3%) | 41 (8.1%) | 0.714 * |
| No | 609 (92.7%) | 468 (91.9%) | ||
| Prefracture walking ability | Unknown | 47 | 46 | 0.024 * |
| Independent without walking aids | 181 (29.6%) | 165 (35.5%) | ||
| Ability to walk outside with a walking stick or crutch | 100 (16.4%) | 80 (17.1%) | ||
| Ability to walk outside with two crutches or a walker | 213 (34.9%) | 148 (31.7%) | ||
| Certain walking ability in the apartment, but outside only with an assistant | 79 (12.9%) | 62 (13.3%) | ||
| No functional walking ability | 38 (6.2%) | 12 (2.6%) | ||
| Death during stay in the acute hospital | Yes | 21 (3.2%) | 21 (4.1%) | 0.500 |
| No | 639 (96.8%) | 492 (95.9%) | ||
| Ability to walk at the 7th postoperative day | Unknown | 15 | 18 | 0.031 * |
| Without aid | 3 (0.5%) | 0 (0%) | ||
| With walking stick or crutch | 51 (7.9%) | 46 (9.3%) | ||
| With a rollator | 89 (13.8%) | 90 (18.3%) | ||
| With a goat | 86 (13.3%) | 62 (12.6%) | ||
| With a walker | 144 (22.3%) | 125 (25.4%) | ||
| Not possible | 274 (42.3%) | 170 (34.5%) | ||
| Reoperation within initial acute hospital stay (several surgical procedures per patient possible) | Reposition | 1 (3.3%) | 6 (12.5%) | 0.024 * |
| Lavage/debridement | 10 (33.3%) | 22 (45.8%) | ||
| Implant removal | 1 (3.3%) | 3 (6.3%) | ||
| Periprosthetic fracture | 4 (13.3%) | 1 (2.1%) | ||
| Other | 14 (46.7%) | 16 (33.3%) | ||
| Discharge from hospital | At home | 153 (23.4%) | 108 (21.2%) | 0.001 * |
| Nursing home | 238 (36.3%) | 136 (26.7%) | ||
| Inpatient stay/other | 243 (37.1%) | 245 (48.0%) | ||
| Death | 21 (3.2%) | 21 (4.1%) |
| Parameter | Subdivision | Osteosynthesis | Implant Change | ||||
|---|---|---|---|---|---|---|---|
| Early Surgical Stabilisation | Late Surgical Stabilisation | p-Value | Early Surgical Stabilisation | Late Surgical Stabilisation | p-Value | ||
| Number of patients | 428 (75.8%) | 237 (24.2%) | 234 (46.6%) | 279 (54.4%) | |||
| Gender | Male | 76 (18.0%) | 71 (30.0%) | 0.001 * | 70 (29.9%) | 89 (31.9%) | 0.698 * |
| Female | 347 (82.0%) | 166 (70.0%) | 164 (70.1%) | 190 (68.1%) | |||
| Patient age (year) Median | 85(80; 89) | 84 (79; 87) | 0.027 ** | 83 (79; 87) | 83 (79; 87) | 0.663 ** | |
| Time to surgery (h) Median | 18.6 | 89.6 | 24 | 103 | |||
| ASA score | Unknown | 13 | 2 | 0.393 * | 4 | 13 | 0.212 * |
| 1 | 2 (0.4%) | 2 (0.9%) | 0 (0.0%) | 4 (1.51%) | |||
| 2 | 89 (21.4%) | 41 (17.5%) | 54 (23.7%) | 55 (20.8%) | |||
| 3 | 281 (67.7%) | 172 (73.5%) | 154 (67.5%) | 177 (66.8%) | |||
| 4 and 5 | 43 (10.4%) | 19 (8.1%) | 20 (8.77%) | 29 (10.9%) | |||
| ISAR score | 0 | 25 (9.3%) | 7 (4.5%) | 0.129 * | 15 (9.4%) | 9 (4.9%) | 0.102 * |
| 1 | 30 (11.2%) | 15 (9.6%) | 25 (15.6%) | 22 (11.9%) | |||
| 2 | 57 (21.2%) | 45 (28.8%) | 38 (23.8%) | 49 (26.5%) | |||
| 3 | 50 (18.6%) | 35 (22.4%) | 38 (23.8%) | 58 (31.4%) | |||
| 4 | 98 (25.3%) | 41 (26.3%) | 33 (20.6%) | 28 (15.1%) | |||
| 5 | 33 (12.3%) | 12 (7.7%) | 10 (6.3%) | 12 (6.5%) | |||
| 6 | 6 (2.2%) | 1 (0.6%) | 1 (0.6%) | 7 (3.8%) | |||
| Anticoagulatory drugs | Yes | 90 (21.2%) | 63 (27.3%) | 0.096 * | 43 (18.8%) | 71 (25.8%) | 0.076 * |
| No | 335 (78.8%) | 168 (72.7%) | 186 (81.2%) | 204 (74.2%) | |||
| Prefracture residental status | At home | 310 (74.7%) | 182 (77.8%) | 0.280 * | 188 (81.7%) | 220 (81.2%) | 0.802 * |
| Nursing home | 95 (22.9%) | 44 (18.8%) | 32 (13.9%) | 42 (15.5%) | |||
| Hospital | 8 (1.9%) | 4 (1.7%) | 8 (3.5%) | 6 (2.2%) | |||
| Other | 2 (0.5%) | 4 (1.7%) | 2 (0.9%) | 3 (1.1%) | |||
| Cocomitant fractures | Yes | 27 (6.4%) | 21 (8.9%) | 0.298 * | 18 (7.7%) | 23 (8.3%) | 0.930 * |
| No | 395 (93.6%) | 214 (91.1%) | 215 (92.3%) | 253 (91.7%) | |||
| Prefracture walking ability | Unknown | 36 | 11 | 0.412 * | 24 | 22 | 0.189 * |
| Independent without walking aids | 113 (29.2%) | 68 (30.4%) | 82 (39.0%) | 83 (32.3%) | |||
| Ability to walk outside with a walking stick or crutch | 59 (15.2%) | 41 (18.3%) | 37 (17.6%) | 43 (16.7%) | |||
| Ability to walk outside with two crutches or a walker | 132 (34.1%) | 81 (36.2%) | 64 (30.5%) | 84 (32.7%) | |||
| Certain walking ability in the apartment, but outside only with an assistant | 56 (14.5%) | 23 (10.3%) | 25 (11.9%) | 37 (14.4%) | |||
| No functional walking ability | 27 (7.0%) | 11 (4.9%) | 2 (1.0%) | 10 (3.9%) | |||
| Death during stay in the acute hospital | Yes | 13 (3.1%) | 8 (3.4%) | 1.000 * | 13 (5.5%) | 8 (2.9%) | 0.191 * |
| No | 411 (96.9%) | 228 (96.6%) | 221 (94.4%) | 271 (97.1%) | |||
| Ability to walk at the 7th postoperative day | Unknown | 11 | 4 | <0.001 * | 6 | 12 | 0.167 * |
| Without aid | 0 | 3 (1.3%) | 0 (0%) | 0 (0%) | |||
| With walking stick or crutch | 34 (8.2%) | 17 (7.3%) | 25 (11.1%) | 21 (7.9%) | |||
| With a rollator | 56 (13.5%) | 33 (14.2%) | 39 (17.3%) | 51 (19.1%) | |||
| With a goat | 198 (47.8%) | 76 (32.6%) | 67 (29.6%) | 103 (38.6%) | |||
| With a walker | 49 (11.8%) | 37 (15.9%) | 33 (14.6%) | 29 (10.9%) | |||
| Not possible | 77 (18.6%) | 67 (28.8%) | 62 (27.4%) | 63 (23.6%) | |||
| Reoperation within initial acute hospital stay (several surgical procedures per patient possible) | Reposition | 1 (4.4%) | 0 (0%) | 0.150 * | 2 (11.8%) | 4 (12.9%) | 0.212 * |
| Lavage/debridement | 8 (34.8%) | 2 (28.6%) | 7 (41.2%) | 15 (48.4%) | |||
| Implant removal | 0 (0%) | 1 (14.3%) | 2 (11.8%) | 1 (3.2%) | |||
| Periprosthetic fracture | 3 (13.0%) | 1 (14.3%) | 0 (0.0%) | 1 (3.2%) | |||
| Other | 11 (47.8%) | 3 (42.9%) | 6 (35.3%) | 10 (32.3%) | |||
| Discharge from hospital | At home | 101 (23.9%) | 52 (22.3%) | 0.795 * | 57 (24.6%) | 51 (18.3%) | 0.053 * |
| Nursing home | 157 (37.2%) | 81 (34.8%) | 64 (27.6%) | 72 (25.9%) | |||
| Inpatient stay/other | 151 (35.8%) | 92 (39.5%) | 98 (42.2%) | 147 (52.9%) | |||
| Death | 13 (3.1%) | 8 (3.4%) | 13 (5.6%) | 8 (2.9%) | |||
| Influence of Time to Surgery on… | N | OR | 95% CI and OR | p-Value | |
| Acute phase | |||||
| <48 h | ≥48 h | ||||
| Death during stay in the acute hospital * Yes vs. no | 642 | 504 | 0.70 | (0.35; 1.38) | 0.310 |
| Walking ability after 7 days * Unable to walk, e.g., just in the room/flat vs. able to walk | 624 | 489 | 0.86 | (0.66; 1.11) | 0.239 |
| N | ẞ | 95% CI and ẞ | p-Value | ||
| EQ5D index after 7 days ~ | 446 | 351 | −0.005 | (−0.05; 0.04) | 0.812 |
| 120 days follow-up | |||||
| <48 h | ≥48 h | ||||
| Mortality * | 258 | 144 | 0.92 | (0.49; 1.70) | 0.803 |
| Walking ability * Unable to walk, e.g., just in the room/flat vs. able to walk | 232 | 128 | 0.77 | (0.47; 1.27) | 0.307 |
| Reoperation within the first 120 days postoperative | 318 | 215 | 1.86 | (1.23; 2.83) | 0.003 |
| N | ẞ | 95% CI and ẞ | p-Value | ||
| EQ5D index ~ | 191 | 101 | −0.07 | (−0.14; 0.01) | 0.082 |
| Parameter | Subdivision | Osteosynthesis | Implant Change | ||||
|---|---|---|---|---|---|---|---|
| Early Surgical Stabilisation | Late Surgical Stabilisation | p-Value | Early Surgical Stabilisation | Late Surgical Stabilisation | p-Value | ||
| Number of patients | 226 (67.5%) | 109 (32.5%) | 114 (48.7%) | 120 (51.3%) | |||
| Readmission to hospital | Yes | 11 (5.8%) | 7 (7.7%) | 0.727 * | 10 (10.1%) | 12 (12.9%) | 0.702 * |
| No | 179 (94.2%) | 84 (92.3%) | 89 (89.9%) | 81 (87.1%) | |||
| Reoperation within the first 120 days postoperative (several surgical procedures per patient possible) | Reposition | 0 (0%) | 0 (0%) | 0.320 * | 6 (60%) | 3 (37.5%) | 0.538 * |
| Lavage/debridement | 0 (0%) | 3 (37.5%) | 2 (20%) | 3 (37.5%) | |||
| Implant removal | 0 (0%) | 2 (25%) | 1 (10%) | 0 (0%) | |||
| Conversion in total arthroplasty | 0 (0%) | 2 (25%) | 0 (0%) | 1 (12.5%) | |||
| Periprosthetic fracture | 5 (55.6%) | 1 (12.5%) | 0 (0%) | 0 (0%) | |||
| Other | 4 (44.4%) | 0 (0%) | 1 (10%) | 1 (12.5%) | |||
| Walking ability at the time of the 120 days follow-up | Unknown | 59 | 38 | 0.449 * | 29 | 52 | 0.498 ** |
| Independent without walking aids | 8 (5.1%) | 4 (6.0%) | 6 (7.2%) | 2 (3.1%) | |||
| Ability to walk outside with a walking stick or crutch | 22 (14.1%) | 7 (10.4%) | 16 (19.3%) | 10 (15.4%) | |||
| Ability to walk outside with two crutches or a walker | 67 (42.9%) | 34 (50.7%) | 32 (38.6%) | 32 (49.2%) | |||
| Certain walking ability in the apartment, but outside only with an assistant | 29 (18.6%) | 15 (22.4%) | 12 (14.5%) | 6 (9.2%) | |||
| No functional walking ability | 30 (19.2%) | 7 (10.4%) | 17 (20.5%) | 15 (23.1%) | |||
| Residence at the time of the 120 days follow-up | At home | 92 (52%) | 39 (53.4%) | 0.996 | 60 (65.9%) | 47 (63.5%) | 0.605 * |
| Nursing home | 52 (29.4%) | 21 (28.8%) | 16 (17.6%) | 12 (16.2%) | |||
| Inpatient stay/other | 7 (4.0%) | 3 (4.1%) | 3 (3.3%) | 6 (8.1%) | |||
| Death | 26 (14.7%) | 10 (13.7%) | 12 (13.2%) | 9 (12.2%) | |||
| Death within the first 120 days postoperative | Yes | 26 (14.7%) | 10 (13.7%) | 0.996 * | 12 (13.2%) | 9 (12.2%) | 1000 * |
| No | 151 (85.3%) | 63 (86.3%) | 79 (86.8%) | 65 (87.8%) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bliemel, C.; Rascher, K.; Knauf, T.; Hack, J.; Eschbach, D.A.; Aigner, R.; Oberkircher, L.; on behalf of the AltersTraumaRegister DGU. Early Surgery Does Not Improve Outcomes for Patients with Periprosthetic Femoral Fractures—Results from the Registry for Geriatric Trauma of the German Trauma Society. Medicina 2021, 57, 517. https://doi.org/10.3390/medicina57060517
Bliemel C, Rascher K, Knauf T, Hack J, Eschbach DA, Aigner R, Oberkircher L, on behalf of the AltersTraumaRegister DGU. Early Surgery Does Not Improve Outcomes for Patients with Periprosthetic Femoral Fractures—Results from the Registry for Geriatric Trauma of the German Trauma Society. Medicina. 2021; 57(6):517. https://doi.org/10.3390/medicina57060517
Chicago/Turabian StyleBliemel, Christopher, Katherine Rascher, Tom Knauf, Juliana Hack, Daphne Asimenia Eschbach, Rene Aigner, Ludwig Oberkircher, and on behalf of the AltersTraumaRegister DGU. 2021. "Early Surgery Does Not Improve Outcomes for Patients with Periprosthetic Femoral Fractures—Results from the Registry for Geriatric Trauma of the German Trauma Society" Medicina 57, no. 6: 517. https://doi.org/10.3390/medicina57060517
APA StyleBliemel, C., Rascher, K., Knauf, T., Hack, J., Eschbach, D. A., Aigner, R., Oberkircher, L., & on behalf of the AltersTraumaRegister DGU. (2021). Early Surgery Does Not Improve Outcomes for Patients with Periprosthetic Femoral Fractures—Results from the Registry for Geriatric Trauma of the German Trauma Society. Medicina, 57(6), 517. https://doi.org/10.3390/medicina57060517