
Palliative Surgery or Metallic Stent Positioning for Advanced Gastric Cancer: Differences in QOL

 , ,
, ,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Endoscopic Procedure
2.2. Radio-Chemotherapy
2.3. Karnofsky Performance Scale and Quality of Life (QoL) Assessment
2.4. Follow-Up Evaluation
2.5. Statistical Analysis
3. Results
3.1. Demographics and Clinical Findings
3.2. Early Results
3.3. Long-Term Results
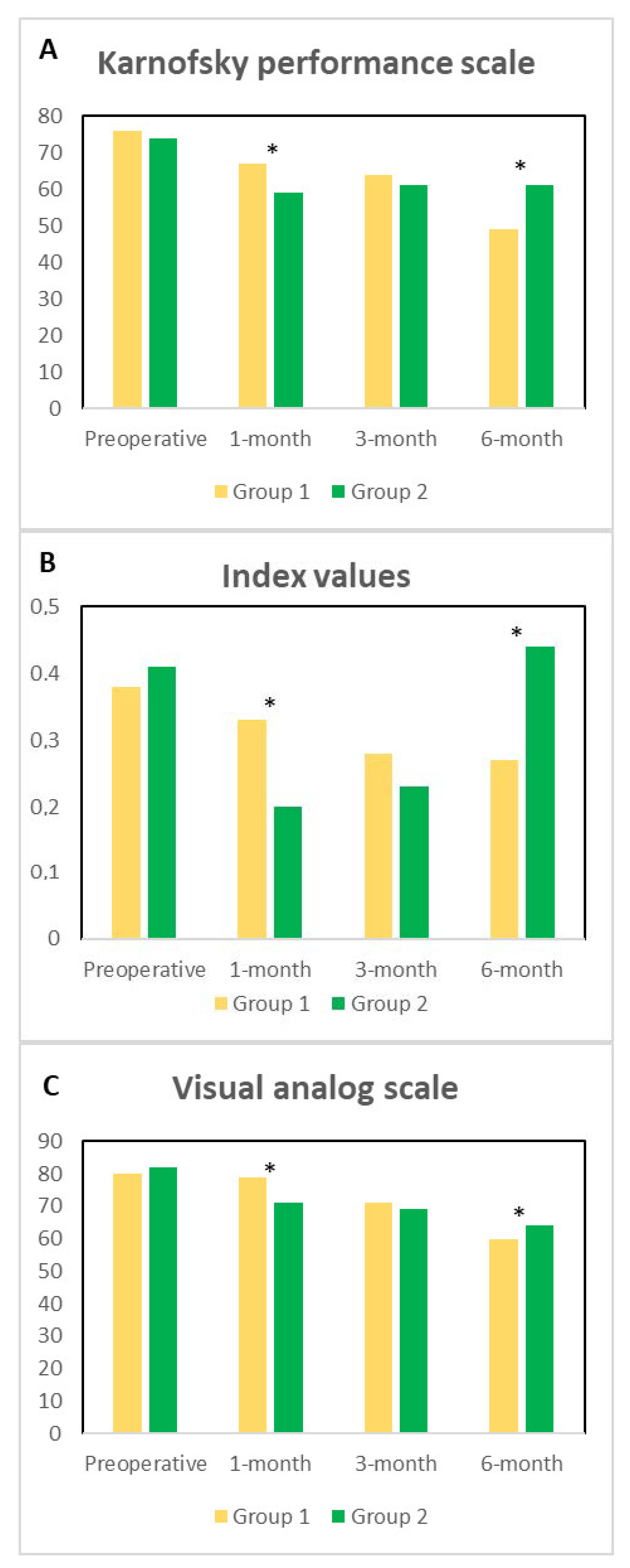
3.4. Karnofsky Performance Scale and Quality of Life (QoL)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sterpetti, A.V.; Fiori, E.; Sapienza, P.; Lamazza, A. Complications after endoscopic stenting for malignant gastric outlet obstruction: A cohort study. Surg. Laparosc. Endosc. Percutaneous Tech. 2019, 29, 169–172. [Google Scholar] [CrossRef]
- Fiori, E.; Lamazza, A.; Demasi, E.; De Cesare, A.; Schillaci, A.; Sterpetti, A.V. Endoscopic stenting for gastric outlet obstruction in patients with unresectable antro pyloric cancer. Systematic review of the literature and final results of a prospective study. The point of view of a surgical group. Am. J. Surg. 2013, 206, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Cisano, C.; Sapienza, P.; Crocetti, D.; De Toma, G. Z-Entry technique reduces the risk of trocar-site hernias in obese patients. Ann. R. Coll. Surg. Engl. 2016, 98, 340–341. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Crocetti, D.; Sapienza, P.; Pedullà, G.; De Toma, G. Reducing the risk of trocar site hernias. Ann. R. Coll. Surg. Engl. 2014, 96, 558. [Google Scholar] [CrossRef]
- Ernberg, A.; Kumagai, K.; Analatos, A.; Rouvelas, I.; Swahn, F.; Lindblad, M.; Lundell, L.; Nilsson, M.; Tsai, J.A. The added value of partial stomach-partitioning to a conventional gastrojejunostomy in the treatment of gastric outlet obstruction. J. Gastrointest. Surg. 2015, 19, 1029–1035. [Google Scholar] [CrossRef]
- Fiori, E.; Lamazza, A.; Volpino, P.; Burza, A.; Paparelli, C.; Cavallaro, G.; Schillaci, A.; Cangemi, V. Palliative management of malignant antro-pyloric strictures. Gastroenterostomy vs. endoscopic stenting. A randomized prospective trial. Anticancer Res. 2004, 24, 269–271. [Google Scholar]
- Kumagai, K.; Rouvelas, I.; Ernberg, A.; Persson, S.; Analatos, A.; Mariosa, D.; Lindblad, M.; Nilsson, M.; Ye, W.; Lundell, L.; et al. A systematic review and meta-analysis comparing partial stomach partitioning gastrojejunostomy versus conventional gastrojejunostomy for malignant gastroduodenal obstruction. Langenbecks Arch. Surg. 2016, 401, 777–785. [Google Scholar] [CrossRef]
- Kaminishi, M.; Yamaguchi, H.; Shimizu, N.; Nomura, S.; Yoshikawa, A.; Hashimoto, M.; Sakai, S.; Oohara, T. Stomach-Partitioning gastrojejunostomy for unresectable gastric carcinoma. Arch. Surg. 1997, 132, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Fiori, E.; Sterpetti, A.V.; De Cesare, A.; Lamazza, A. Factors leading to improved results for endoscopic stenting for metastatic antropyloric adenocarcinoma. A comparison with gastrojejunostomy. J. Gastrointest. Surg. 2016, 20, 1802–1806. [Google Scholar] [CrossRef]
- Schag, C.C.; Heinrich, R.L.; Ganz, P.A. Karnofsky performance status revisited: Reliability, validity, and guidelines. J. Clin. Oncol. 1984, 2, 187–193. [Google Scholar] [CrossRef]
- Faiz, K.W. VAS-Visuell analog skala [VAS-Visual analog scale]. Tidsskr. Nor. Laegeforening 2014, 134, 323. [Google Scholar] [CrossRef] [PubMed]
- Scalone, L.; Cortesi, P.A.; Ciampichini, R.; Belisari, A.; D’Angiolella, L.S.; Cesana, G.; Mantovani, L.G. Italian population-based values of EQ-5D health states. Value Health 2013, 16, 814–822. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Whitley, E.; Ball, J. Statistics review 1: Presenting and summarizing data. Crit. Care 2002, 6, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Lye, T.J.; Goh, Y.C.; Eng, A.K.; Ong, H.S.; Wong, W.K.; Chan, W.H. Endoscopic self-expandable metallic stenting for palliation of malignant gastric outlet obstruction in Southeast Asia. ANZ J. Surg. 2016, 86, 464–468. [Google Scholar] [CrossRef]
- Hori, Y.; Naitoh, I.; Hayashi, K.; Ban, T.; Natsume, M.; Okumura, F.; Nakazawa, T.; Takada, H.; Hirano, A.; Jinno, N.; et al. Predictors of stent dysfunction after self-expandable metal stent placement for malignant gastric outlet obstruction: Tumor ingrowth in uncovered stents and migration of covered stents. Surg. Endosc. 2017, 31, 4165–4173. [Google Scholar] [CrossRef] [PubMed]
- Takahara, N.; Isayama, H.; Nakai, Y.; Yoshida, S.; Saito, T.; Mizuno, S.; Yagioka, H.; Kogure, H.; Togawa, O.; Matsubara, S.; et al. A novel partially covered self-expandable metallic stent with proximal flare in patients with malignant gastric outlet obstruction. Gut Liver 2017, 11, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Boškoski, I.; Tringali, A.; Familiari, P.; Mutignani, M.; Costamagna, G. Self-Expandable metallic stents for malignant gastric outlet obstruction. Adv. Ther. 2010, 27, 691–703. [Google Scholar] [CrossRef]
- Song, G.A.; Kang, D.H.; Kim, T.O.; Heo, J.; Kim, G.H.; Cho, M.; Heo, J.H.; Kim, J.Y.; Lee, J.S.; Jeoung, Y.J.; et al. Endoscopic stenting in patients with recurrent malignant obstruction after gastric surgery: Uncovered versus simultaneously deployed uncovered and covered (double) self-expandable metal stents. Gastrointest. Endosc. 2007, 65, 782–787. [Google Scholar] [CrossRef]
- Lamazza, A.; Fiori, E.; Schillaci, A.; Sterpetti, A.V.; Lezoche, E. Treatment of anastomotic stenosis and leakage after colorectal resection for cancer with self-expandable metal stents. Am. J. Surg. 2014, 208, 465–469. [Google Scholar] [CrossRef]
- Bocca, B.; Lamazza, A.; Pino, A.; De Masi, E.; Iacomino, M.; Mattei, D.; Rahimi, S.; Fiori, E.; Schillaci, A.; Alimonti, A.; et al. Determination of 30 elements in colorectal biopsies by sector field inductively coupled plasma mass spectrometry: Method development and preliminary baseline levels. Rapid Commun. Mass Spectrom. 2007, 21, 1776–1782. [Google Scholar] [CrossRef]
- Lamazza, A.; Fiori, E.; Schillaci, A.; Sterpetti, A.V. A new technique for placement of a self-expanding metallic stent (SEMS) in patients with colon rectal obstruction: A prospective study of 43 patients. Surg. Endosc. 2013, 27, 1045–1048. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Kang, D.H.; Kim, G.H.; Park, W.I.; Kim, H.W.; Park, J.H. Self-Expanding metallic stents for gastric outlet obstruction resulting from stomach cancer: A preliminary study with a newly designed double-layered pyloric stent. Gastrointest. Endosc. 2007, 66, 1206–1210. [Google Scholar] [CrossRef] [PubMed]
- Lamazza, A.; Fiori, E.; De Masi, E.; Scoglio, D.; Sterpetti, A.V.; Lezoche, E. Self-Expanding metal stents for treatment of anastomotic complications after colorectal resection. Endoscopy 2013, 45, 493–495. [Google Scholar] [CrossRef]
- Venu, R.P.; Pastika, B.J.; Kini, M.; Chua, D.; Christian, R.; Schlais, J.; Brown, R.D. Self-Expandable metal stents for malignant gastric outlet obstruction: A modified technique. Endoscopy 1998, 30, 553–558. [Google Scholar] [CrossRef]
- Lamazza, A.; Fiori, E.; Sterpetti, A.V.; Schillaci, A.; De Cesare, A.; Lezoche, E. Endoscopic placement of self-expandable metallic stents for rectovaginal fistula after colorectal resection: A comparison with proximal diverting ileostomy alone. Surg. Endosc. 2016, 30, 797–801. [Google Scholar] [CrossRef]
- Nassif, T.; Prat, F.; Meduri, B.; Fritsch, J.; Choury, A.D.; Dumont, J.L.; Auroux, J.; Desaint, B.; Boboc, B.; Ponsot, P.; et al. Endoscopic palliation of malignant gastric outlet obstruction using self-expandable metallic stents: Results of a multicenter study. Endoscopy 2003, 35, 483–489. [Google Scholar]
- Lamazza, A.; Fiori, E.; Schillaci, A.; Sterpetti, A.V.; Lezoche, E. Treatment of rectovaginal fistula after colorectal resection with endoscopic stenting: Long-Term results. Colorectal Dis. 2015, 17, 356–360. [Google Scholar] [CrossRef]
- Ly, J.; O’Grady, G.; Mittal, A.; Plank, L.; Windsor, J.A. A systematic review of methods to palliate malignant gastric outlet obstruction. Surg. Endosc. 2010, 24, 290–297. [Google Scholar] [CrossRef]
- Fiori, E.; Lamazza, A.; Sterpetti, A.V.; Crocetti, D.; De Felice, F.; Di Muzio, M.; Mingoli, A.; Sapienza, P.; De Toma, G. Quality of life for patients with incurable stage IV colorectal cancer: Randomized controlled trial comparing resection versus endoscopic stenting. In Vivo 2019, 33, 2065–2070. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group 1 | Group 2 | Significance | |
|---|---|---|---|
| Number | 13 | 14 | |
| Median age (Mode; IQR) | 77 (80; 8) | 73 (81; 10) | 0.201 |
| Sex (M/F) | 8/5 | 9/5 | 0.598 |
| Total bilirubin (μmol/L) | 13 (4) | 11 (3) | 0.439 |
| AST (U/L) | 27 (7) | 31 (9) | 0.829 |
| ALT (U/L) | 45 (9) | 41 (10) | 0.377 |
| PT-INR | 0.9 (0.8) | 1.1 (0.7) | 0.568 |
| Ascites | 2 | 2 | 0.875 |
| Liver metastasis | 11 | 13 | 0.773 |
| Pulmonary metastases | 4 | 3 | 0.263 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiori, E.; Crocetti, D.; Sapienza, P.; Cirocchi, R.; Sterpetti, A.V.; Miccini, M.; Accordino, M.; Costi, S.; Lapolla, P.; Mingoli, A.; et al. Palliative Surgery or Metallic Stent Positioning for Advanced Gastric Cancer: Differences in QOL. Medicina 2021, 57, 428. https://doi.org/10.3390/medicina57050428
Fiori E, Crocetti D, Sapienza P, Cirocchi R, Sterpetti AV, Miccini M, Accordino M, Costi S, Lapolla P, Mingoli A, et al. Palliative Surgery or Metallic Stent Positioning for Advanced Gastric Cancer: Differences in QOL. Medicina. 2021; 57(5):428. https://doi.org/10.3390/medicina57050428
Chicago/Turabian StyleFiori, Enrico, Daniele Crocetti, Paolo Sapienza, Roberto Cirocchi, Antonio V. Sterpetti, Michelangelo Miccini, Marcello Accordino, Silvano Costi, Pierfrancesco Lapolla, Andrea Mingoli, and et al. 2021. "Palliative Surgery or Metallic Stent Positioning for Advanced Gastric Cancer: Differences in QOL" Medicina 57, no. 5: 428. https://doi.org/10.3390/medicina57050428
APA StyleFiori, E., Crocetti, D., Sapienza, P., Cirocchi, R., Sterpetti, A. V., Miccini, M., Accordino, M., Costi, S., Lapolla, P., Mingoli, A., De Toma, G., & Lamazza, A. (2021). Palliative Surgery or Metallic Stent Positioning for Advanced Gastric Cancer: Differences in QOL. Medicina, 57(5), 428. https://doi.org/10.3390/medicina57050428