
Intelligent Diagnosis of Thyroid Ultrasound Imaging Using an Ensemble of Deep Learning Methods

 ,
,  ,
,  ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
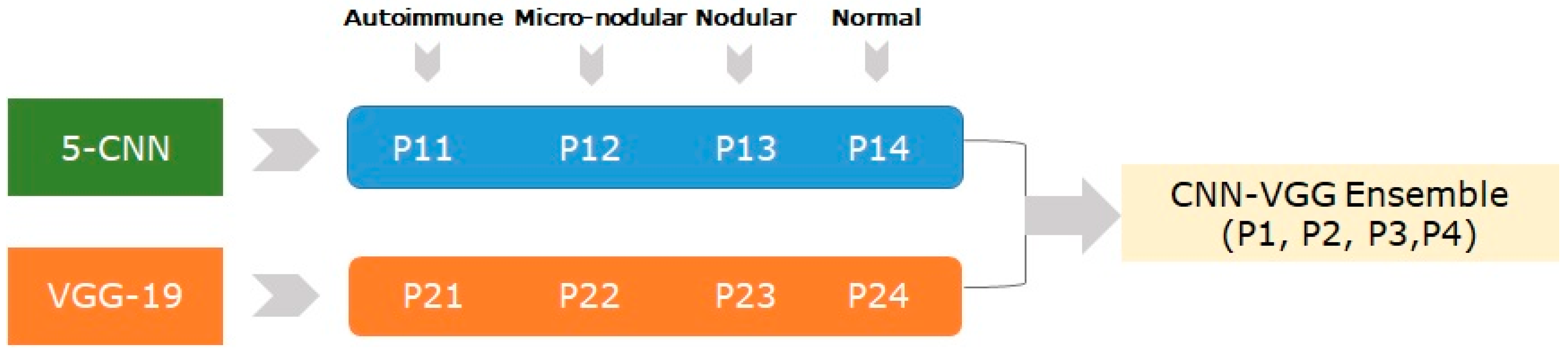
- Designing, developing, training, optimizing, and evaluating a novel fusion method (called CNN-VGG) based on two DL models, in order to increase the classification accuracy.
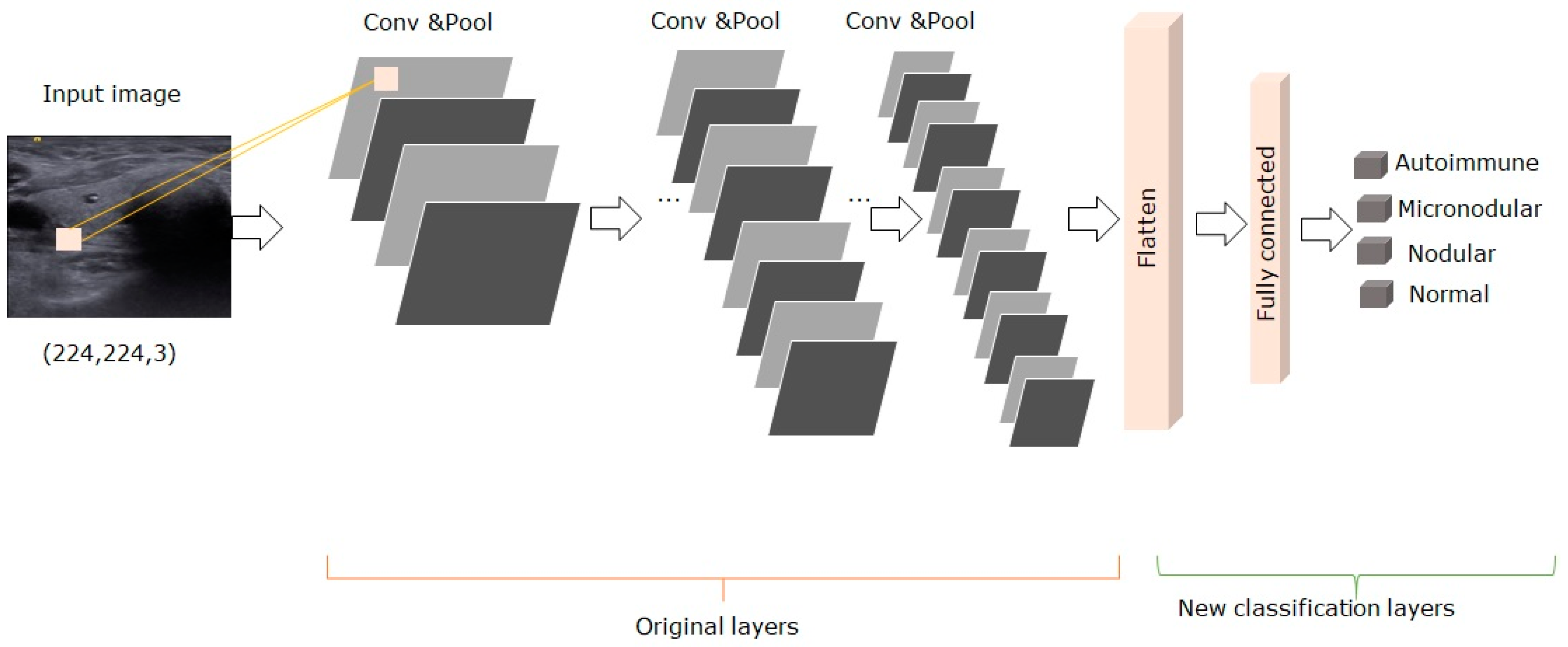
- Fine-tuning of pre-trained models for feature extraction and image classification.
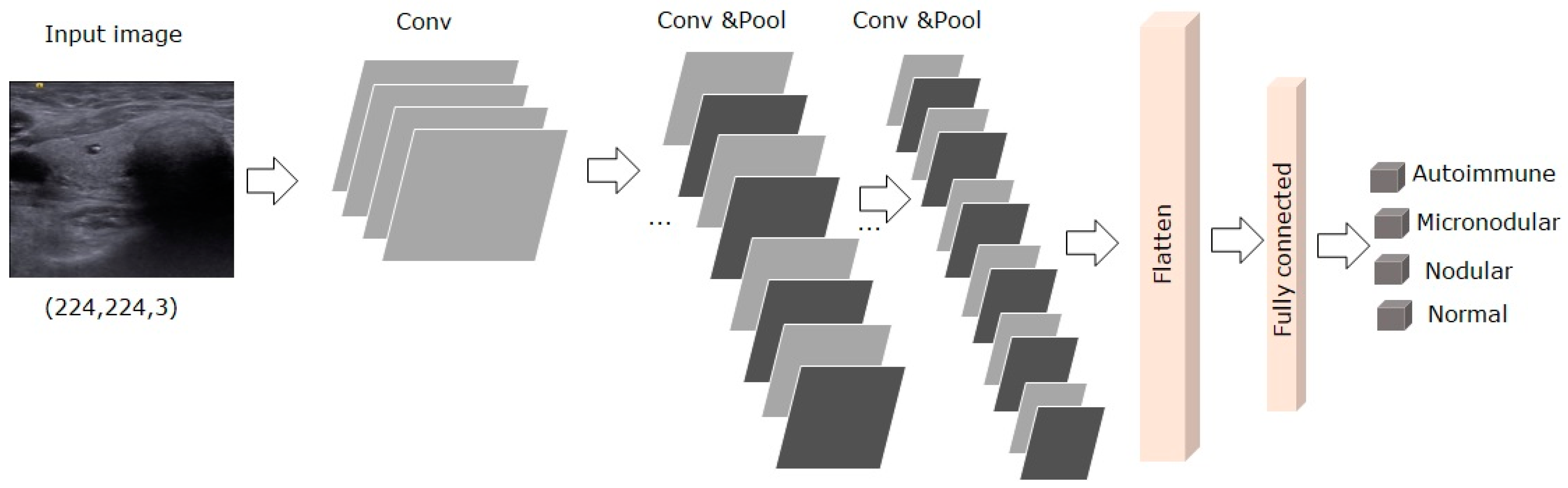
- Designing, developing, evaluating, and optimizing an efficient 5-CNN model with five convolutional layers, in order to analyze its classification abilities.
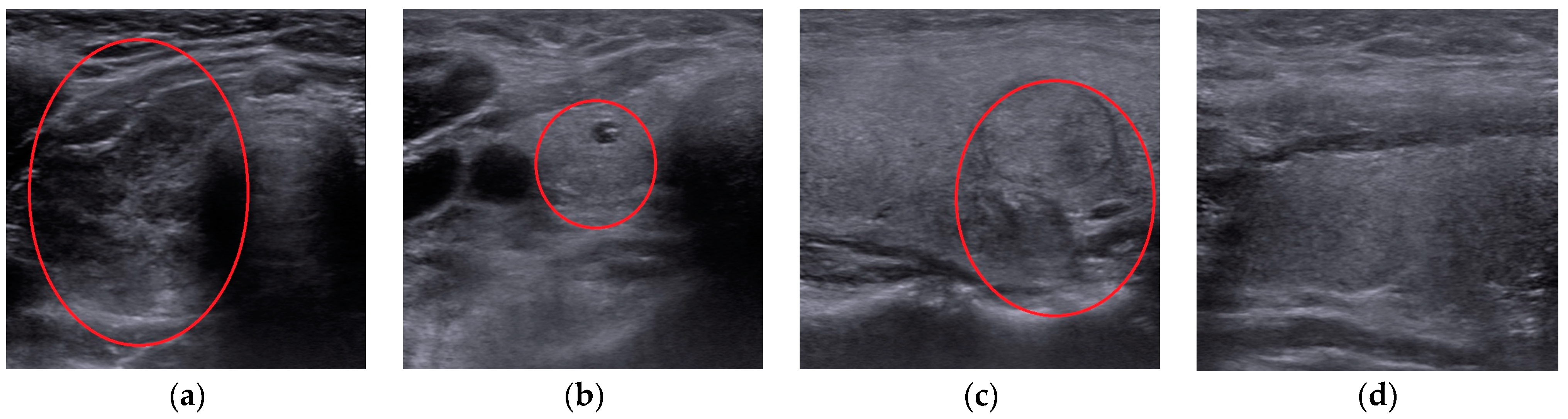
- Collecting and curing a novel dataset of 2797 images, which included thyroidal US images, classified into four diagnoses: autoimmune, micro-nodular, nodular, and normal.
- A detailed experimental and statistical analysis of the proposed models was provided to validate the performance of the proposed methods: accuracy, sensitivity, specificity, positive and negative predictive values, ROC-AUC, and Precision/Recall were taken into consideration.
2. Materials and Methods
2.1. Patients Data
2.2. Image Dataset
2.3. Convolutional Neural Networks
2.4. Transfer Learning with Fine Tuning
2.5. Deep Models Implementation
2.5.1. The 5-CNN Model
| Algorithm 1. The 5-CNN model description |
| Input: thyroidal images of dimension (500 px, 500 px) from the train dataset. |
| Output: CNN model weights |
| 1. for each image in the dataset |
| 2. Resize image to (224 px, 224 px) |
| 3. Normalize the image pixels values between [0, 1]. |
| 4. end |
| 5. Add a first convolutional layer with a RELU activation function. |
| 6. Add a second convolutional layer with a RELU activation function. |
| 7. Apply a max pooling layer for down-sampling feature map from the previous layer. |
| 8. Repeat the steps 4 and 5 for three times. |
| 9. Add a Flatten layer on the output obtained from the last max-pooling layer. |
| 10. Add a fully connected layer with 256 hidden units. |
| 11. Apply a dropout for inactivate neurons in the previous layer. |
| 12. Add a fully connected layer with 4 hidden units and a softmax activation function. |
| 13. Optimize the model with RMSProp optimizer with a learning rate of 0.0001. |
| 14. Train the model for 100 epochs. |
| 15. Save the final model. |
2.5.2. The VGG-19 Model
| Algorithm 2. The VGG-19 model description |
| Input: thyroidal images of dimension (500 px, 500 px) from the train dataset. |
| Output: VGG model weights |
| 1. for each image in the dataset |
| 2. Resize image to (224 px, 224 px) |
| 3. Normalize the image pixels values between [0, 1]. |
| 4. end |
| 5. Load the VGG-19 model pre-trained on ImageNet dataset. |
| 6. Remove the last layer of the model. |
| 7. Make non-trainable all the layers of the model. |
| 8. Add a Flatten layer on the model output to obtain a 1-D array of features. |
| 9. Add a fully connected layer with 256 hidden units. |
| 10. Apply a dropout for inactivate neurons in the previous layer. |
| 11. Add a fully connected layer with 4 hidden units and a softmax activation function. |
| 12. Optimize the model with Adam optimizer. |
| 13. Train the model for 100 epochs. |
| 14. Save the final model. |
2.5.3. The CNN-VGG Ensemble Method
| Algorithm 3. The VGG-CNN ensemble description. |
| Input: thyroidal images of dimension (500 px, 500 px) from the test dataset. |
| Output: prediction probabilities for each diagnosis class (autoimmune, micro-nodular, nodular, normal). |
| 1. for each image in the dataset |
| 2. Resize image to (224 px, 224 px) |
| 3. Normalize the image pixels values between [0, 1]. |
| 4. end |
| 5. Load the trained 5-CNN model. |
| 6. Load the trained VGG-19 model. |
| 7. Predict the images with CNN resulting a list of probabilities (P11, P12, P13, P14) |
| 8. Predict the images with VGG resulting a list of probabilities (P21, P22, P23, P24) |
| 9. Average the two lists of predictions of the two models. |
| 10. for each class in the set of diagnosis |
| 11.Output prediction probabilities for the diagnosis class. |
| 12. end |
2.6. Evaluation Metrics
3. Results
3.1. Experimental Setup
3.2. Deep Models Evaluation and Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AITD | Autoimmune thyroid disease |
| HT | Hashimoto’s thyroiditis |
| GD | Graves Disease |
| TSH | Thyroid-Stimulating Hormone |
| FT4 | Free T4 (thyroxine) |
| ATPO | Thyroid Peroxidase Antibodies |
| ATG | Thyroglobulin Antibodies |
| TRAb | Thyrotropin Receptor Antibodies |
| TSAb | Thyroid-stimulating antibodies |
| US | Ultrasound |
| CAD | Computer-Aided Diagnosis |
| ML | Machine Learning |
| DL | Deep Learning |
| CNN | Convolutional Neural Network |
| PPV | Predictive Positive Value |
| NPV | Negative Predictive Value |
| AUC | Area under the Curve |
References
- Gardner, D.G.; Shoback, D.M.; Greenspan, F.S. The Thyroid Gland. In Greenspan’s Basic & Clinical Endocrinology, 10th ed.; McGraw-Hill Medical: New York, NY, USA, 2018. [Google Scholar]
- Cappa, M.; Bizzarri, C.; Crea, F. Autoimmune thyroid diseases in children. J. Thyroid Res. 2011, 675703, 2010. [Google Scholar] [CrossRef]
- Stanciu, M.; Bera, L.G.; Popescu, M.; Grosu, F.; Popa, F.L. Hashimoto’s thyroiditis associated with thyroid adenoma with Hurthle cells-case report. Rom. J. Morphol. Embryol. 2017, 58, 241–248. [Google Scholar]
- Pedersen, O.M.; Aardal, N.P.; Larssen, T.B.; Varhaug, J.E.; Myking, O.; Vik-Mo, H. The value of ultrasonography in predicting autoimmune thyroid disease. Thyroid 2000, 10, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Dorte, H.; Bennedbaek, F.; Høier-Madsen, M.; Hegedüs, L.; Jacobsen, B. A prospective study of thyroid function, morphology and autoimmunity in young patients with type 1 diabetes. Eur. J. Endocrinol. 2003, 148, 245–251. [Google Scholar]
- Marqusee, E.; Benson, C.B.; Frates, M.C.; Doubilet, P.M.; Larsen, P.R.; Cibas, E.S.; Mandel, S.J. Usefulness of ultrasonography in the management of nodular thyroid disease. Ann. Internal. Med. 2000, 133, 696–700. [Google Scholar] [CrossRef]
- Yildirim, D.; Gurses, B.; Gurpinar, B.; Ekci, B.; Colakoglu, B.; Kaur, A. Nodule or pseudonodule? Differentiation in Hashimoto’s thyroiditis with sonoelastography. J. Int. Med. Res. 2011, 39, 2360–2369. [Google Scholar] [CrossRef]
- Nguyen, D.T.; Pham, T.D.; Batchuluun, G.; Yoon, H.J.; Park, K.R. Artificial Intelligence-Based Thyroid Nodule Classification Using Information from Spatial and Frequency Domains. J. Clin. Med. 2019, 8, 1976. [Google Scholar] [CrossRef] [PubMed]
- Park, V.Y.; Han, K.; Seong, Y.K.; Park, M.H.; Kim, E.K.; Moon, H.J.; Yoon, J.H.; Kwak, J.Y. Diagnosis of Thyroid Nodules: Performance of a Deep Learning Convolutional Neural Network Model vs. Radiologists. Sci. Rep. 2019, 9, 17843. [Google Scholar] [CrossRef]
- Cazacu, I.; Udristoiu, A.; Gruionu, L.; Iacob, A.; Gruionu, G.; Saftoiu, A. Artificial intelligence in pancreatic cancer: Toward precision diagnosis. Endosc. Ultrasound 2019, 8, 357–359. [Google Scholar]
- Dhaka, V.S.; Rani, G.; Oza, M.G.; Sharma, T.; Misra, A. A deep learning model for mass screening of COVID-19. Int. J. Imaging Syst. Technol. 2021, 1–16, status manuscript in preparation. [Google Scholar]
- Liu, S.; Wang, Y.; Yang, X.; Lei, B.; Liu, L.; Li, S.X.; Ni, D.; Wang, T. Deep Learning in Medical Ultrasound Analysis: A Review. Engineering 2019, 5, 261–275. [Google Scholar] [CrossRef]
- Yin, S.; Peng, Q.; Li, H.; Zhang, Z.; You, X.; Liu, H.; Fischer, K.; Furth, S.L.; Tasian, G.E.; Fan, Y. Multi-instance Deep Learning with Graph Convolutional Neural Networks for Diagnosis of Kidney Diseases Using Ultrasound Imaging. In Uncertainty for Safe Utilization of Machine Learning in Medical Imaging and Clinical Image-Based Procedures; Springer: Cham, Switzerland, 2019; Volume 11840, pp. 146–154. [Google Scholar]
- Koh, J.; Lee, E.; Han, K.; Kim, E.K.; Son, E.J.; Sohn, Y.M.; Seo, M.; Kwon, M.R.; Yoon, J.H.; Lee, J.H.; et al. Diagnosis of thyroid nodules on ultrasonography by a deep convolutional neural network. Sci. Rep. 2020, 10, 15245. [Google Scholar] [CrossRef]
- Ma, J.; Wu, F.; Zhu, J.; Xu, D.; Kong, D. A pre-trained convolutional neural network based method for thyroid nodule diagnosis. Ultrasonics 2017, 73, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Xie, S.; Yu, J.; Niu, L.; Sun, W.D. Classification of thyroid nodules in ultrasound images using deep model based transfer learning and hybrid features. In Proceedings of the 2017 IEEE International Conference on Acoustics, Speech and Signal Processing, New Orleans, LA, USA, 5–9 March 2017; pp. 919–923. [Google Scholar]
- Liu, T.; Xie, S.; Zhang, Y.; Yu, J.; Niu, L.; Sun, W.D. Feature selection and thyroid nodule classification using transfer learning. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging, Melbourne, Australia, 18–21 April 2017; pp. 1096–1099. [Google Scholar]
- Nguyen, D.; Kang, J.; Pham, T.; Batchuluun, G.; Park, K. Ultrasound Image-Based Diagnosis of Malignant Thyroid Nodule Using Artificial Intelligence. Sensors 2020, 20, 1822. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhang, S.; Zhang, Q.; Wei, X.; Pan, Y.; Zhao, J.; Xin, X.; Qin, C.; Wang, X.; Li, J.; et al. Diagnosis of thyroid cancer using deep convolutional neural network models applied to sonographic images: A retrospective, multicohort, diagnostic study. Lancet Oncol. 2019, 20, 193–201. [Google Scholar] [CrossRef]
- Pan, S.J.; Yang, Q. A survey on transfer learning. IEEE Trans. Knowl. Data Eng. 2009, 22, 1345–1359. [Google Scholar] [CrossRef]
- Abadi, M. TensorFlow: Learning functions at scale. In Proceedings of the 21st ACM SIGPLAN International Conference on Functional Programming, Nara, Japan, 19–21 September 2016; Volume 51, p. 1. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. In Proceedings of the 3rd International Conference on Learning Representations, ICLR 2015, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Tan, M.; Le, Q. Efficient Net: Rethinking Model Scaling for Convolutional Neural Networks. In Proceedings of the 36th International Conference on Machine Learning, PMLR, Long Beach, CA, USA, 9–15 June 2019; Volume 97, pp. 6105–6114. [Google Scholar]
- Keras. Available online: https://github.com/keras-team/keras (accessed on 1 June 2020).
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:14126980. [Google Scholar]
- Dietterich, T.G. Ensemble Methods in Machine Learning. In Proceedings of the First International Workshop on Multiple Classifier Systems, MCS ’00, London, UK, 21–23 June 2000; Springer: London, UK, 2000; pp. 1–15. [Google Scholar]
- Saito, T.; Rehmsmeier, M. The precision-recall plot is more informative than the ROC plot when evaluating binary classifiers on imbalanced datasets. PLoS ONE 2015, 10, e0118432. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; The MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet classification with deep convolutional neural networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Zhu, Y.; Fu, Z.; Fei, J. An image augmentation method using convolutional network for thyroid nodule classification by transfer learning. In Proceedings of the 3rd IEEE International Conference on Computer and Communication, Chengdu, China, 13–16 December 2017; pp. 1819–1823. [Google Scholar]
- Chi, J.; Walia, E.; Babyn, P.; Wang, J.; Groot, G.; Eramian, M. Thyroid nodule classification in ultrasound images by fine-tuning deep convolutional neural network. J. Digit. Imaging 2017, 30, 477–486. [Google Scholar] [CrossRef]
- Song, J.; Chai, Y.J.; Masuoka, H.; Park, S.W.; Kim, S.J.; Choi, J.Y.; Kong, H.J.; Lee, K.E.; Lee, J.; Kwak, N.; et al. Ultrasound image analysis using deep learning algorithm for the diagnosis of thyroid nodules. Medicine 2019, 98, e15133. [Google Scholar] [CrossRef] [PubMed]
- Koundal, D.; Gupta, S.; Signh, S. Computer aided thyroid nodule detection system using medical ultrasound images. Biomed. Signal. Process. Control 2018, 40, 117–130. [Google Scholar] [CrossRef]
- Nasser, M.A.; Melendez, J.; Moreno, A.; Omer, O.A.; Puig, D. Breast tumor classification in ultrasound images using texture analysis and super-resolution methods. Eng. Appl. Artif. Intell. 2017, 59, 84–92. [Google Scholar] [CrossRef]
- Jebadurai, J.; Peter, J.D. Super-resolution of retinal images using multi-kernel SVR for IoT healthcare applications. Future Gener. Comput. Syst. 2018, 83, 338–346. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis | Training | Testing | Totals |
|---|---|---|---|
| Autoimmune | 619/67 | 148/16 | 767/83 |
| Micro-nodular | 552/37 | 120/9 | 672/46 |
| Nodular | 590/49 | 130/12 | 720/61 |
| Normal | 536/32 | 102/8 | 638/40 |
| Total | 2297/185 | 500/45 | 2797/230 |
| Diagnostic Class | Accuracy (%) | ROC-AUC | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| Autoimmune | 97.57 | 0.95 | 95.2 | 98.53 | 96.36 | 98.05 |
| Micro-nodular | 92.89 | 0.92 | 91.05 | 94.74 | 93.02 | 95.84 |
| Nodular | 92.2 | 0.92 | 91.93 | 92.99 | 91.70 | 96.36 |
| Normal | 96.88 | 0.93 | 95.24 | 100 | 100 | 96.19 |
| Average | 94.88 | 0.93 | 93.35 | 96.56 | 95.27 | 96.61 |
| Diagnostic Class | Accuracy (%) | ROCAUC | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| Autoimmune | 97.2 | 0.95 | 90.5 | 98.71 | 99.3 | 96.17 |
| Micro-nodular | 95.8 | 0.97 | 91.16 | 94.47 | 89 | 99.73 |
| Nodular | 95.8 | 0.94 | 91.53 | 97.29 | 92.24 | 97.03 |
| Normal | 98 | 0.95 | 90.19 | 99.7 | 98.92 | 97.54 |
| Average | 96.7 | 0.95 | 90.84 | 97.54 | 94.86 | 97.62 |
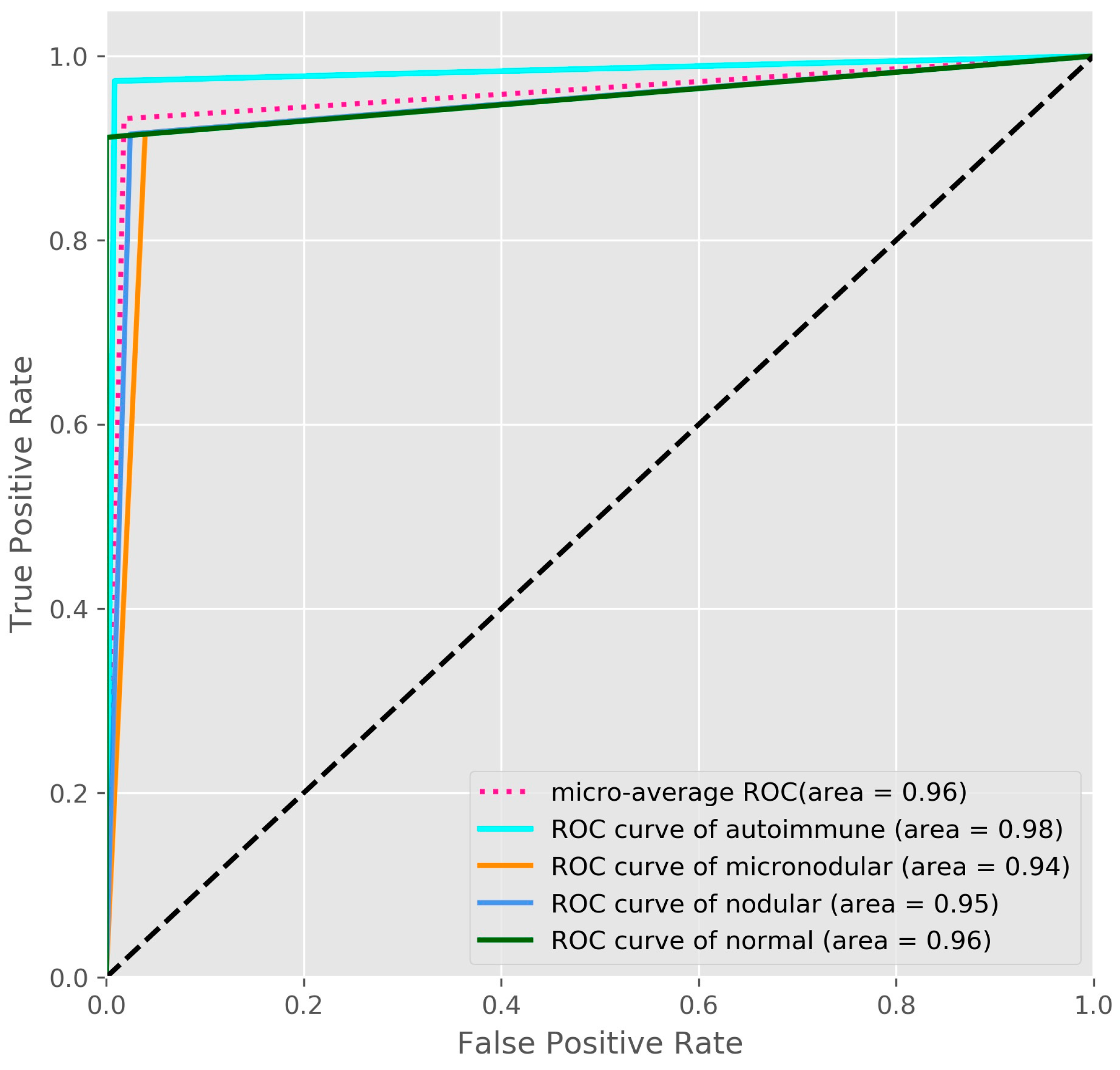
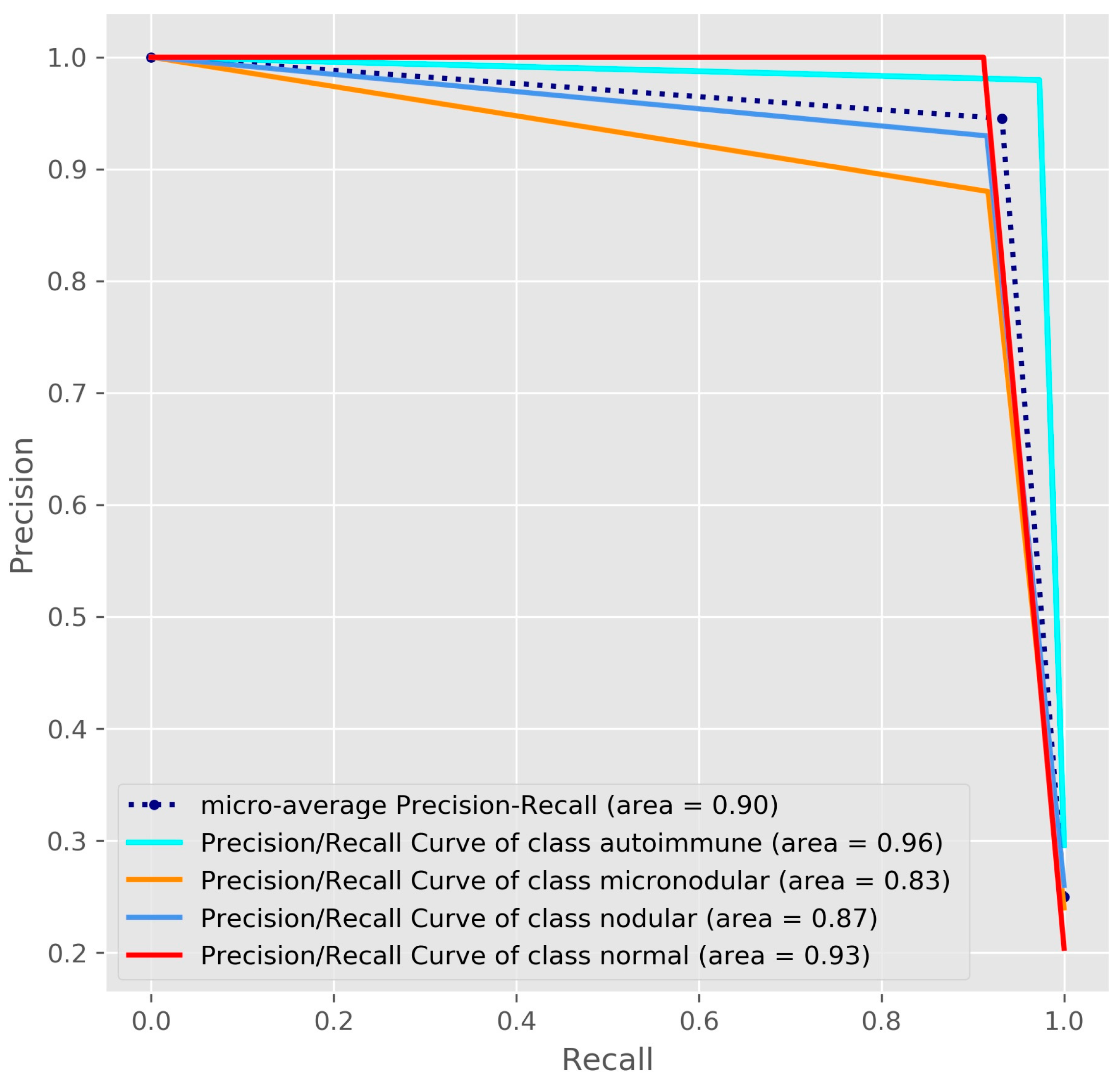
| Diagnostic Class | Accuracy (%) | ROC-AUC | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| Autoimmune | 98.78 | 0.98 | 97.6 | 99.26 | 98.19 | 99.02 |
| Micro-nodular | 95.66 | 0.95 | 92.8 | 96.57 | 89.58 | 97.69 |
| Nodular | 96.53 | 0.95 | 92.61 | 97.89 | 93.87 | 97.44 |
| Normal | 98.44 | 0.96 | 100 | 100 | 100 | 98.06 |
| Average | 97.35 | 0.96 | 95.75 | 98.43 | 95.41 | 98.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasile, C.M.; Udriștoiu, A.L.; Ghenea, A.E.; Popescu, M.; Gheonea, C.; Niculescu, C.E.; Ungureanu, A.M.; Udriștoiu, Ș.; Drocaş, A.I.; Gruionu, L.G.; et al. Intelligent Diagnosis of Thyroid Ultrasound Imaging Using an Ensemble of Deep Learning Methods. Medicina 2021, 57, 395. https://doi.org/10.3390/medicina57040395
Vasile CM, Udriștoiu AL, Ghenea AE, Popescu M, Gheonea C, Niculescu CE, Ungureanu AM, Udriștoiu Ș, Drocaş AI, Gruionu LG, et al. Intelligent Diagnosis of Thyroid Ultrasound Imaging Using an Ensemble of Deep Learning Methods. Medicina. 2021; 57(4):395. https://doi.org/10.3390/medicina57040395
Chicago/Turabian StyleVasile, Corina Maria, Anca Loredana Udriștoiu, Alice Elena Ghenea, Mihaela Popescu, Cristian Gheonea, Carmen Elena Niculescu, Anca Marilena Ungureanu, Ștefan Udriștoiu, Andrei Ioan Drocaş, Lucian Gheorghe Gruionu, and et al. 2021. "Intelligent Diagnosis of Thyroid Ultrasound Imaging Using an Ensemble of Deep Learning Methods" Medicina 57, no. 4: 395. https://doi.org/10.3390/medicina57040395
APA StyleVasile, C. M., Udriștoiu, A. L., Ghenea, A. E., Popescu, M., Gheonea, C., Niculescu, C. E., Ungureanu, A. M., Udriștoiu, Ș., Drocaş, A. I., Gruionu, L. G., Gruionu, G., Iacob, A. V., & Alexandru, D. O. (2021). Intelligent Diagnosis of Thyroid Ultrasound Imaging Using an Ensemble of Deep Learning Methods. Medicina, 57(4), 395. https://doi.org/10.3390/medicina57040395