
The Effects of COVID-19 on Healthcare Workers and Non-Healthcare Workers in Mexico: 14 Months into the Pandemic


 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Operational Definition of the Variables
- Infection disease—an illness caused by the transmission of a specific infectious biological agent from an infected person. The transmission can occur directly or indirectly from an infectious patient to a susceptible host [24].
- Suspected case of viral respiratory disease—an individual of any age who has with a presented cough, dyspnea, and fever accompanied by one or more of the following or symptoms: myalgia, arthralgia, odynophagia, chills, chest pain, rhinorrhea, polypnea, anosmia, dysgeusia, or conjunctivitis in the last 10 days.
- Laboratory-confirmed case of COVID-19—all patients that meet the definition of a suspected case of viral respiratory disease and who have received a diagnosis confirmed by an RT-PCR test and/or rapid antigen test performed in any of the National Network of Public Health Laboratories recognized by the Institute of Epidemiological Diagnosis and Reference (In-DRE, acronym in Spanish) of the SSA.
- Case of COVID-19 confirmed by epidemiological association—all patients that meet the definition of a suspected case and who have been shown to have been in close contact (proximity of less than one meter for 15 min or more, continuous or accumulated) with a person with a case confirmed by an RT-PCR test and/or rapid antigen test 2 to 14 days before the onset of symptoms, with the associated confirmed case registered on the SISVER platform.
- Active case of COVID-19—positive case with symptoms in the last 14 days.
- Death with laboratory-confirmed diagnosis—deceased person who meets the definition of a suspected case of viral respiratory disease confirmed by a laboratory RT-PCR test or by a rapid test (detection of SARS-CoV-2 antigen).
- Death due to COVID-19 confirmed by epidemiological association–deceased person who meets the definition of a suspected case of viral respiratory disease with a negative, nonamplified, or inadequate test or non-available sample, and who had contact with a laboratory-confirmed case (RT-PCR test or rapid antigen test) within 14 days before the date of symptom onset with the associated confirmed case registered on the SISVER platform.
- Healthcare workers—The information for HCWs was obtained by filtering data by “occupation” on the SISVER platform; the data on the platform were gathered from epidemiological reports regarding the COVID-19 situation in Mexico and in the reports on healthcare workers with COVID-19 by the SSA.
- “Occupation” was reported by respondents based on which group of healthcare workers that they belonged to, i.e., “physician”, “nurse”, “laboratory specialist”, “dentist”, and “other healthcare worker”.
- Comorbidities—The following comorbidities that are associated with COVID-19 were included: obesity, systemic arterial hypertension, diabetes mellitus, smoking, asthma, chronic obstructive pulmonary disease, asthma, immunosuppression, chronic renal failure, cardiovascular disease, and human immunodeficiency virus (HIV).
- Mortality rate—A measure of the frequency of the occurrence of death in a defined population during a specified interval of time [24].
- Excess mortality—the number of observed deaths minus the number of expected deaths and deaths associated with COVID-19 due to excess mortality—obtained by filtering data by “cause of death” on the National Registry of Population and Identity of the Mexican Republic [25].
2.3. Statistical Analysis
3. Results
3.1. Distribution of COVID-19 Cases in Healthcare Workers and Non-Healthcare Workers in Mexico
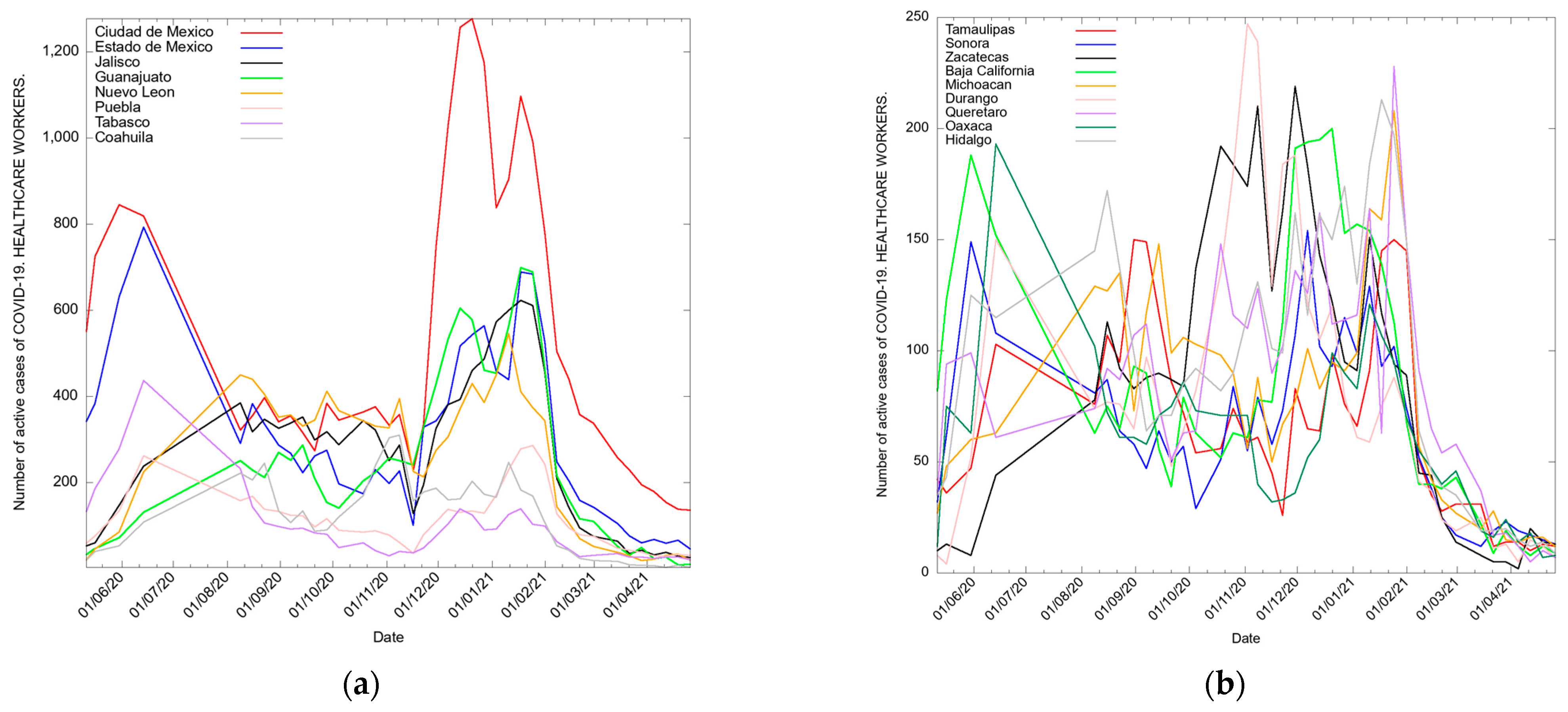
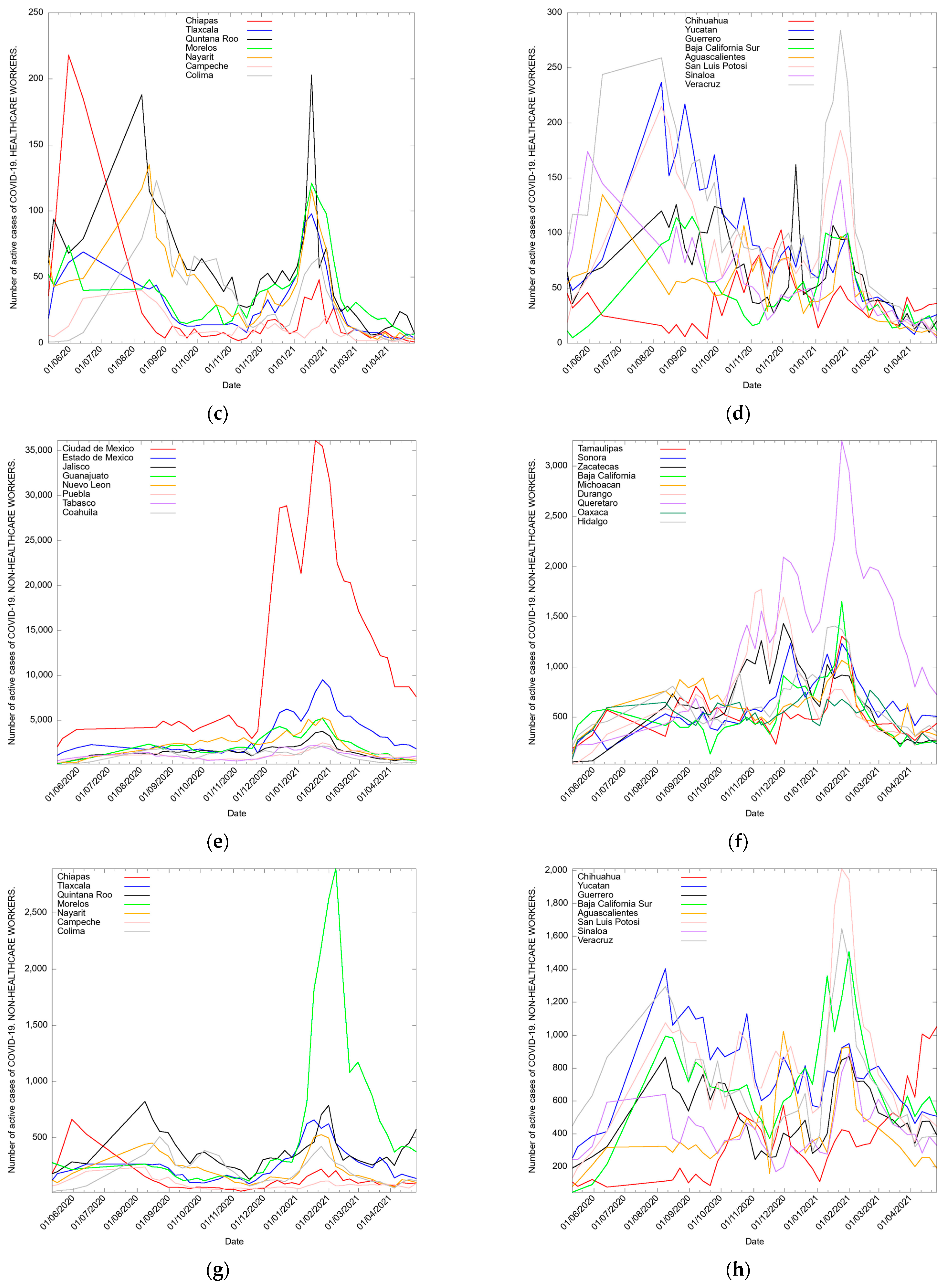
3.2. Active Cases of COVID-19 Cases in Healthcare Workers and Non-Healthcare Workers in Mexico
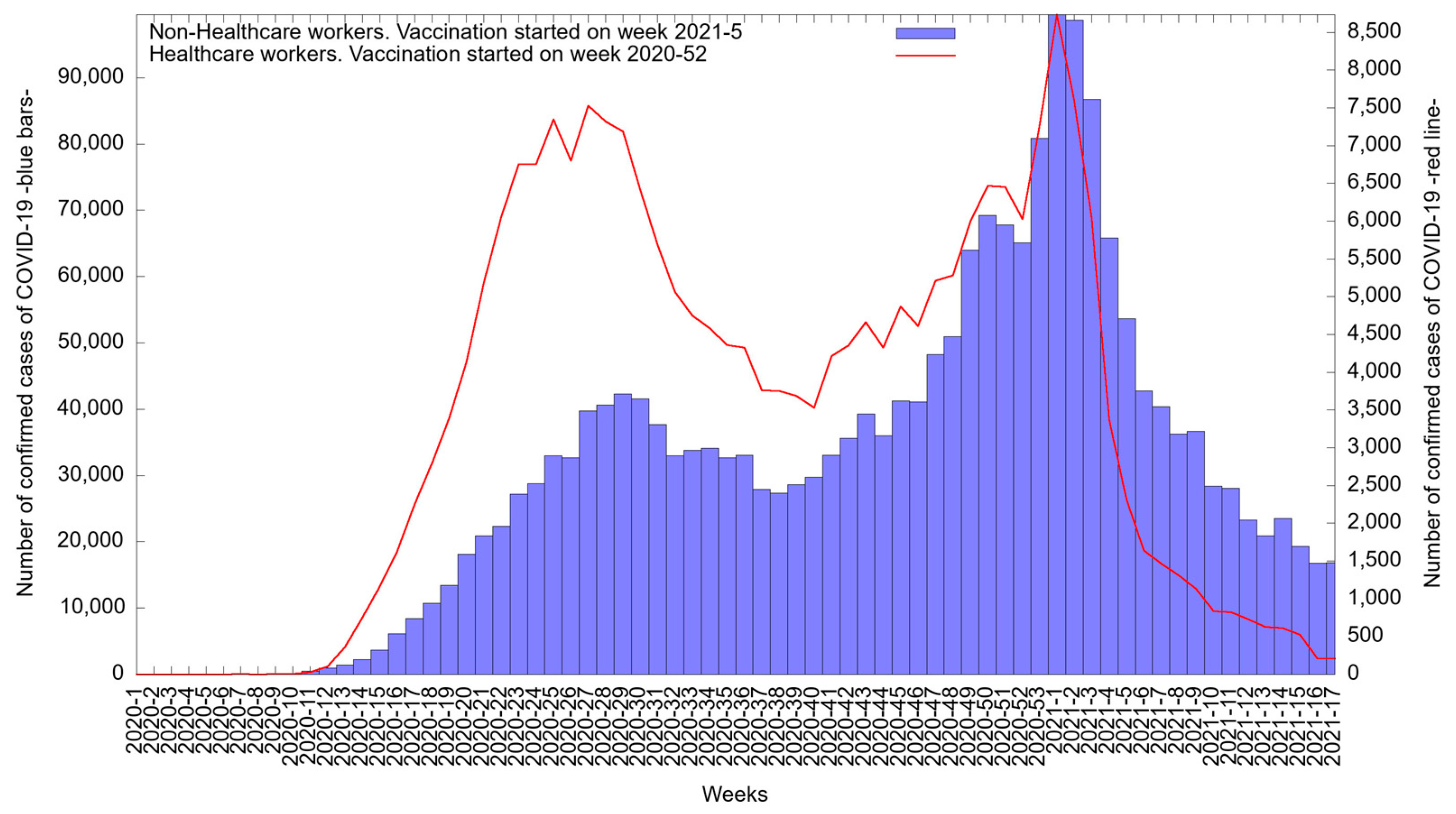
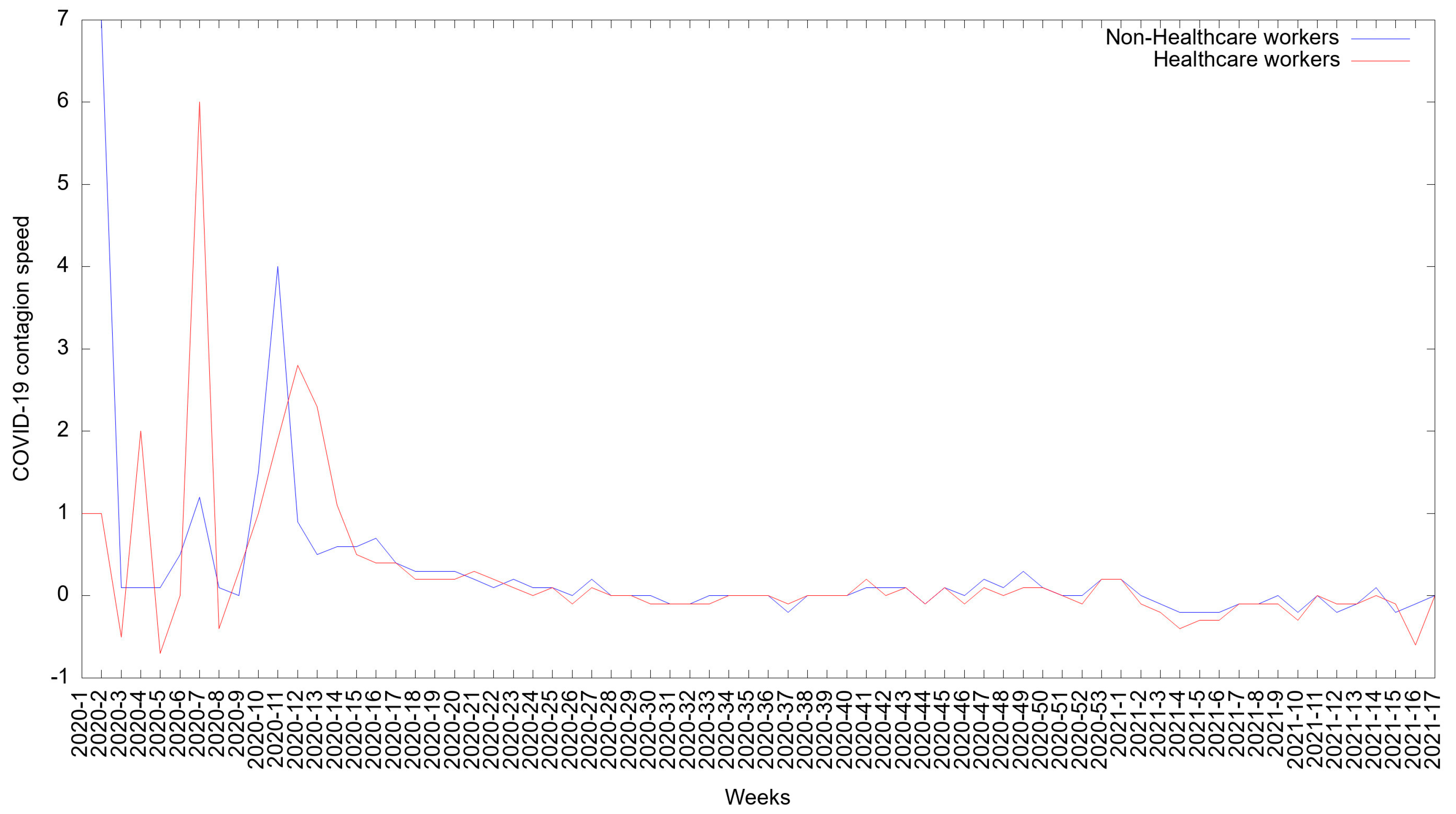
3.3. Epidemic Curve of COVID-19 Cases in Healthcare Workers and Non-Healthcare Workers in Mexico
3.4. COVID-19 Infection Rate in Healthcare Workers and Non-Healthcare Workers in Mexico
3.5. Deaths from COVID-19 in Healthcare Workers and Non-Healthcare Workers in Mexico
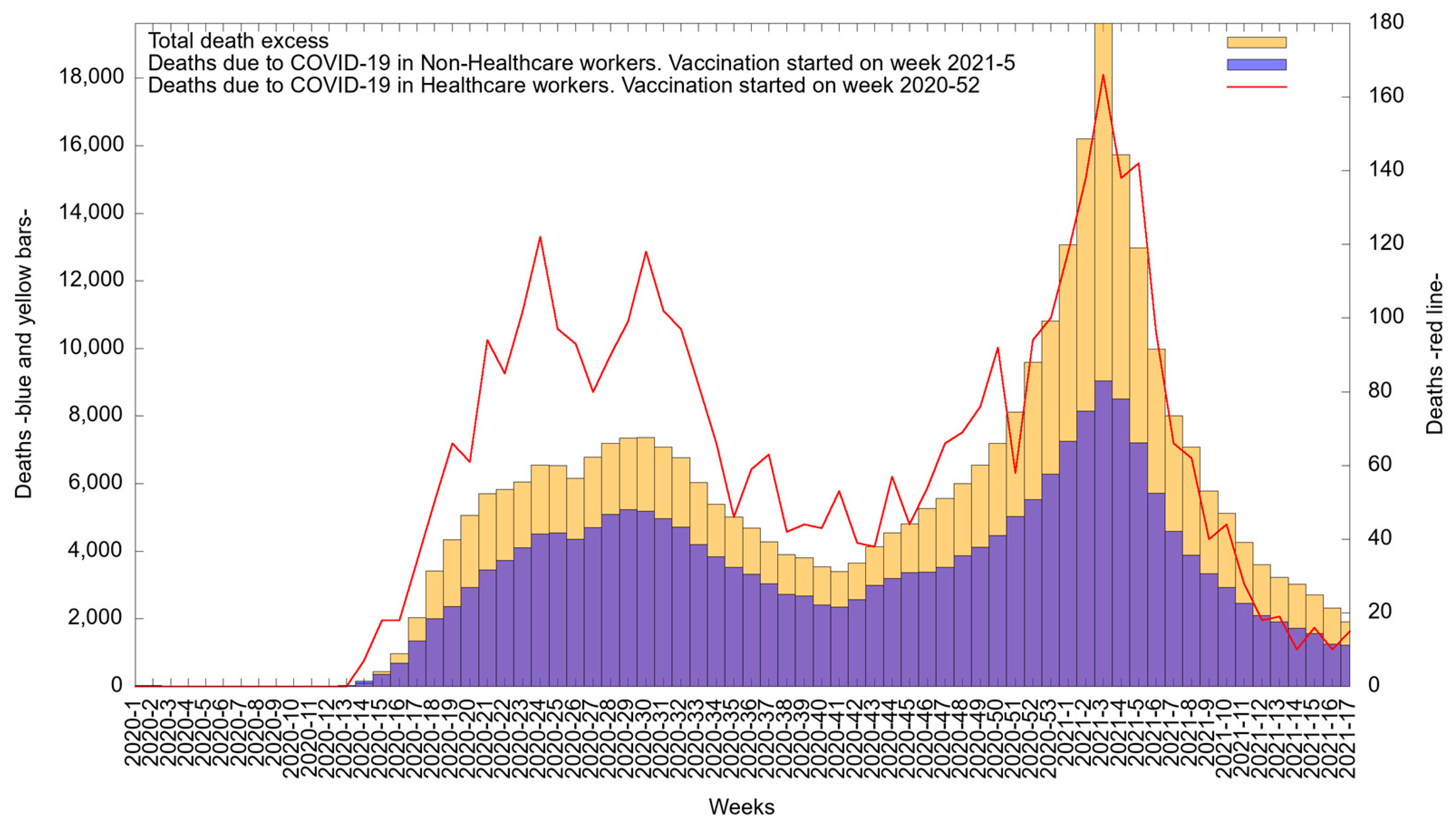
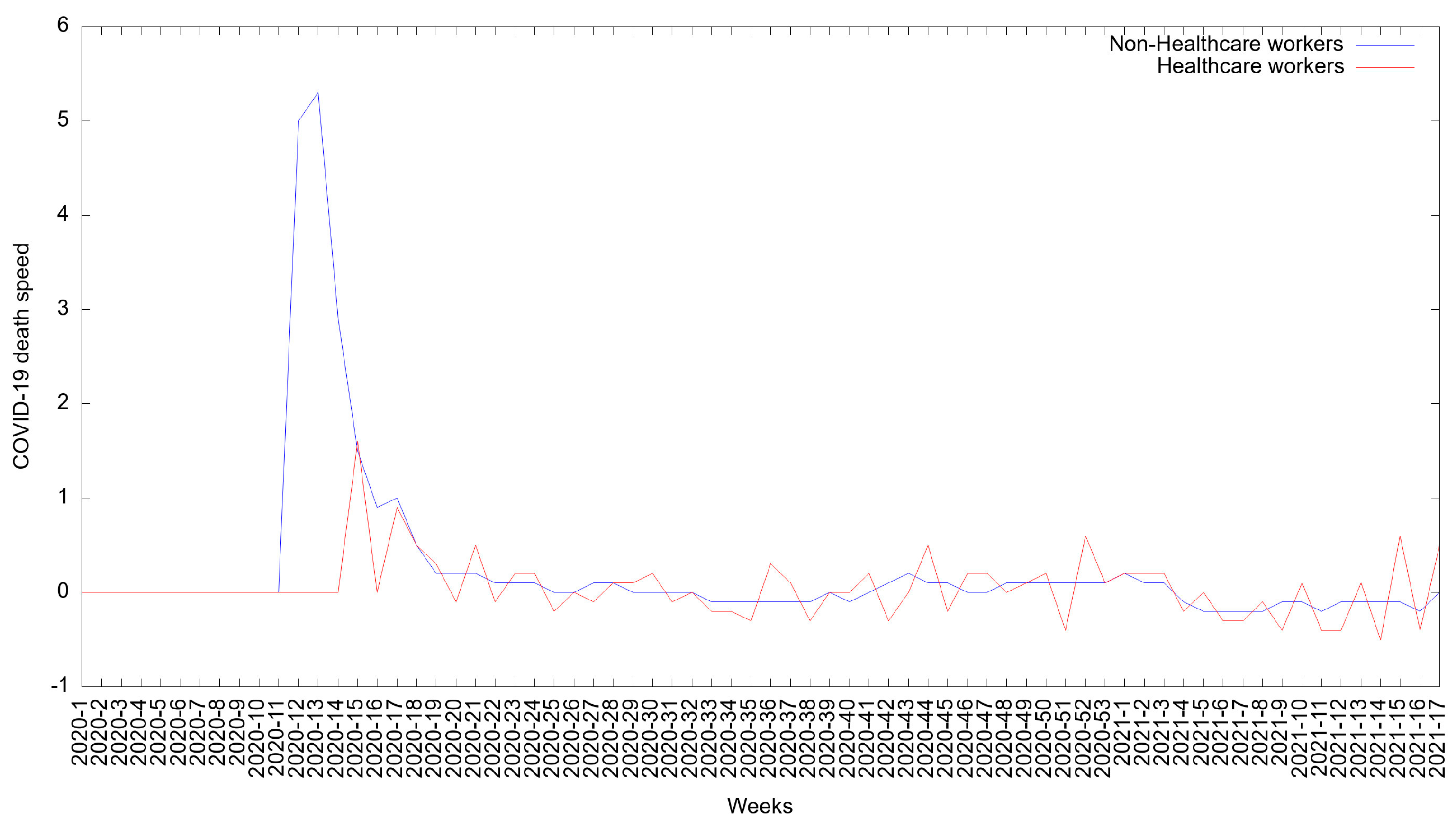
3.6. Epidemic Curve for Deaths Due to COVID-19 in Healthcare Workers and Non-Healthcare Workers in Mexico
3.7. The COVID-19 Death Rate in Healthcare Workers and Non-Healthcare Workers in Mexico
3.8. Cases and Deaths Due to COVID-19 by Age Group in Healthcare Workers and Non-Healthcare Workers in Mexico
3.9. Cases and Deaths Due to COVID-19 and Comorbidities among Healthcare Workers and Non-Healthcare Workers in Mexico
3.10. Comorbidities Related with COVID-19 Cases in Healthcare Workers and Non-Healthcare Workers in Mexico
3.11. Cases and Deaths Due to COVID-19 by Occupation in Healthcare Workers and Non-Healthcare Workers in Mexico
3.12. New Cases of and Deaths Due to COVID-19 by Period among Healthcare Workers in Mexico
3.13. Health System Personnel Combatting the Pandemic in Mexico
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Novel Coronavirus (2019-nCoV) Situation Report-1. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200121-sitrep-1-2019-ncov.pdf (accessed on 26 April 2021).
- Sharma, A.; Tiwari, S.; Deb, M.K.; Marty, J.L. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): A global pandemic and treatment strategies. Int. J. Antimicrob. Agents 2020, 56, 106054. [Google Scholar] [CrossRef] [PubMed]
- Health Workers and Administrator. Available online: https://www.who.int/teams/risk-communication/health-workers-and-administrators (accessed on 26 April 2021).
- Atención a Personas sin Seguridad Social se Garantiza en los Centros Públicos de Salud: Insabi. Available online: https://www.gob.mx/salud/prensa/002-atencion-a-personas-sin-seguridad-social-se-garantiza-en-los-centros-publicos-de-salud-insabi?idiom=es (accessed on 26 November 2021). (In Spanish).
- Lineamientos de Reconversión Hospitalaria en México. Available online: https://coronavirus.gob.mx/wp-content/uploads/2020/04/Documentos-Lineamientos-Reconversion-Hospitalaria.pdf (accessed on 26 November 2021). (In Spanish).
- COVID-19 Strategy Update. Available online: https://www.who.int/publications/i/item/covid-19-strategy-update---14-april-2020 (accessed on 26 April 2021).
- Salazar, M.Á.; Chavez-Galan, L.; Castorena-Maldonado, A.; Mateo-Alonso, M.; Diaz-Vazquez, N.O.; Vega-Martínez, A.M.; Martínez-Orozco, J.A.; Becerril-Vargas, E.; Sosa-Gómez, F.M.; Patiño-Gallegos, H.; et al. Low Incidence and Mortality by SARS-CoV-2 Infection Among Healthcare Workers in a Health National Center in Mexico: Successful Establishment of an Occupational Medicine Program. Front. Public Health 2021, 9, 311. [Google Scholar] [CrossRef] [PubMed]
- Caldera-Villalobos, C.; Garza-Veloz, I.; Martínez-Avila, N.; Delgado-Enciso, I.; Ortiz-Castro, Y.; Cabral-Pacheco, G.A.; Martinez-Fierro, M.L. The Coronavirus Disease (COVID-19) Challenge in Mexico: A Critical and Forced Reflection as Individuals and Society. Front. Public Health 2020, 8, 337. [Google Scholar] [CrossRef] [PubMed]
- Health Workers: A Global Profile. In The World Health Report 2006: Working Together for Health; World Health Organization: Geneva, Switzerland, 2006.
- Mutambudzi, M.; Niedzwiedz, C.; Macdonald, E.B.; Leyland, A.; Mair, F.; Anderson, J.; Celis-Morales, C.; Cleland, J.; Forbes, J.; Gill, J.; et al. Occupation and risk of severe COVID-19: Prospective cohort study of 120 075 UK Biobank participants. Occup. Environ. Med. 2021, 78, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Programa Nacional de Vacunación. Available online: http://vacunacovid.gob.mx/wordpress/priorizacion-de-personas-a-vacunar/ (accessed on 26 November 2021). (In Spanish).
- Coronavirus COVID19 Comunicados Técnicos Diarios Históricos. 2021. Available online: https://www.gob.mx/cms/uploads/attachment/file/632693/Comunicado_Tecnico_Diario_COVID-19_2021.04.26.pdf (accessed on 26 April 2021). (In Spanish).
- Epidemiological Update: Coronavirus Disease (COVID-19). Available online: https://www.paho.org/es/documentos/actualizacion-epidemiologica-enfermedad-por-coronavirus-covid-19-14-abril-2021 (accessed on 26 April 2021). (In Spanish).
- Kammar-García, A.; Vidal-Mayo, J.J.; Vera-Zertuche, J.M.; Lazcano-Hernández, M.; Vera-López, O.; Segura-Badilla, O.; Aguilar-Alonso, P.; Navarro-Cruz, A.R. Impact of Comorbidities In Mexican Sars-Cov-2-Positive Patients: A Retrospective Analysis In A National Cohort. Rev. Investig. Clin. 2020, 72, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Antonio-Villa, N.E.; Bello-Chavolla, O.Y.; Vargas-Vázquez, A.; Fermín-Martínez, C.A.; Márquez-Salinas, A.; Bahena-López, J.P. Health-care workers with COVID-19 living in Mexico City: Clinical characterization and related outcomes. Clin. Infect. Dis. 2020, 73, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus COVID19 Comunicados Técnicos Diarios Históricos. 2020. Available online: https://www.gob.mx/salud/acciones-y-programas/coronavirus-covid-19-comunicados-tecnicos-diarios-historicos-2020 (accessed on 26 April 2021). (In Spanish).
- Coronavirus COVID19 Comunicados Técnicos Diarios Históricos 2021. Available online: https://www.gob.mx/salud/documentos/informes-epidemiologicos-de-la-situacion-de-covid19-en-mexico-2021 (accessed on 26 April 2021). (In Spanish).
- Informes Epidemiológicos de la Situación de COVID-19 en México. Available online: https://www.gob.mx/salud/documentos/informes-epidemiologicos-de-la-situacion-de-covid19-en-mexico (accessed on 22 April 2021). (In Spanish).
- Informes sobre el Personal de Salud COVID-19 en México. Available online: https://www.gob.mx/salud/documentos/informes-sobre-el-personal-de-salud-covid-19-en-mexico (accessed on 27 April 2021). (In Spanish).
- Tablero de Seguimiento de Covid-19. Available online: https://covid19.sinave.gob.mx/ (accessed on 4 May 2021).
- Tablero Sobre Exceso de Mortalidad en México COVID-19. Available online: https://www.insp.mx/recomendaciones/tablero-sobre-exceso-de-mortalidad-en-mexico-covid-19 (accessed on 28 April 2021). (In Spanish).
- Lineamiento Estandarizado para la Vigilancia Epidemiológica y por Laboratorio de la Enfermedad Respiratoria Viral. Available online: https://www.gob.mx/cms/uploads/attachment/file/672708/Lineamiento_VE_y_Lab_Enf_Viral_20211008.pdf (accessed on 26 August 2021). (In Spanish).
- Lesson 1: Introduction to Epidemiology. In Principles of Epidemiology in Public Health Practice; CDC Center for Disease Control and Prevention: Atlanta, GA, USA, 2006; pp. 1–20.
- Actualizaciones en la Presentación de Información de la Base de Datos del Boletín Estadístico Sobre el Exceso de Mortalidad en México. Available online: http://www.dgis.salud.gob.mx/descargas/datosabiertos/excesoMortalidad/210329_Nota_Actualizacion_en_presentacion_de_informacion_del_boletin_estadistico_sobre_exceso_de_mortalidad_en_Mexico.pdf?v=1.1 (accessed on 30 April 2021). (In Spanish).
- Informe Epidemiológico de la Situación de COVID-19 en México Febrero a 28 de Abril 2020. Available online: https://www.gob.mx/cms/uploads/attachment/file/637171/Informe_COVID-19_2020.04.28.pdf (accessed on 27 April 2021). (In Spanish).
- Décimo Informe Epidemiológico de la Situación de COVID-19. Available online: https://www.gob.mx/cms/uploads/attachment/file/637172/Informe_COVID-19_2020.06.29.pdf (accessed on 30 July 2021). (In Spanish).
- 13° Informe Epidemiológico de la Situación de COVID-19. Available online: https://www.gob.mx/cms/uploads/attachment/file/637183/Informe_COVID-19_2020.07.20.pdf (accessed on 30 September 2021). (In Spanish).
- 14° Informe Epidemiológico de la Situación de COVID-19. Available online: https://www.gob.mx/cms/uploads/attachment/file/637184/Informe_COVID-19_2020.07.27.pdf (accessed on 30 September 2021). (In Spanish).
- Sadeghi Dousari, A.; Taati Moghadam, M.; Satarzadeh, N. COVID-19 (Coronavirus Disease 2019): A New Coronavirus Disease. Infect. Drug Resist. 2020, 13, 2819–2828. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Garduño, E.; Mendoza-Damián, F.; Garduño-Alanís, A.; Ayón-Garibaldo, S. Tuberculosis in Mexico and the USA, Comparison of Trends Over Time 1990–2010. Tuberc. Respir. Dis. 2015, 78, 246–252. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Macías, A.E.; Puentes-Rosas, E.; Velandia, D.; Morley, D.; Coudeville, L.; Baurin, N. Real-World Evidence of Dengue Burden on Hospitals in Mexico: Insights From the Automated Subsystem of Hospital Discharges (Saeh) Database. Rev. Investig. Clín. 2019, 71, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Sistema de Información Legislativa del Gobierno de México. Comparecencia del Secretario de Salud: Dr. Jorge Alcocer. Available online: http://sil.gobernacion.gob.mx/Archivos/Documentos/2020/09/asun_4080276_20200930_1601570367.pdf (accessed on 30 September 2021). (In Spanish).
- Actualización Epidemiológica: Enfermedad por Coronavirus (COVID-19)—22 de Julio de 2021. Available online: https://www.paho.org/es/documentos/actualizacion-epidemiologica-enfermedad-por-coronavirus-covid-19-22-julio-2021 (accessed on 20 August 2021). (In Spanish).
- Van der Plaat, D.A.; Madan, I.; Coggon, D.; van Tongeren, M.; Edge, R.; Muiry, R.; Parsons, V.; Cullinan, P. Risks of COVID-19 by occupation in NHS workers in England. Occup. Environ. Med. 2021. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Atlas de la Diabetes de la Federación Internacional de Diabetes (FID) Novena Edición 2019. Available online: https://www.diabetesatlas.org/upload/resources/material/20200302_133352_2406-IDF-ATLAS-SPAN-BOOK.pdf (accessed on 30 September 2021). (In Spanish).
- Hipertensión Arterial un Problema de Salud Pública en México Secretaria de Salud de México. Available online: https://www.insp.mx/avisos/5398-hipertension-arterial-problema-salud-publica.html#:~:text=De%20acuerdo%20con%20la%20Encuesta,cuales%20aproximadamente%20el%2040%20por (accessed on 30 June 2021).
- Launch of the Study: “The Heavy Burden of Obesity: The Economics of Prevention”. Available online: https://www.oecd.org/about/secretary-general/heavy-burden-of-obesity-mexico-january-2020.htm (accessed on 30 May 2021). (In Spanish).
- Guerrero-Torres, L.; Caro-Vega, Y.; Crabtree-Ramírez, B.; Sierra-Madero, J.G. Clinical Characteristics and Mortality of Health-Care Workers With Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Mexico City. Clin. Infect. Dis. 2020, 73, e199–e205. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Prather, K.A.; Sznitman, J.; Jimenez, J.L.; Lakdawala, S.S.; Tufekci, Z.; Marr, L.C. Airborne transmission of respiratory viruses. Science 2021, 373, eabd9149. [Google Scholar] [CrossRef] [PubMed]
- Senpuku, H.; Fukumoto, M.; Uchiyama, T.; Taguchi, C.; Suzuki, I.; Arikawa, K. Effects of Extraoral Suction on Droplets and Aerosols for Infection Control Practices. Dent. J. 2021, 9, 80. [Google Scholar] [CrossRef] [PubMed]
- Plan Nacional de Vacunación para COVID-19 en México. Available online: https://www.gob.mx/sre/articulos/el-plan-nacional-de-vacunacion-se-llevara-a-cabo-en-tiempo-y-forma-de-acuerdo-a-los-periodos-programados-ebrard-260227?idiom=es (accessed on 26 November 2021). (In Spanish).
- Comunicado Técnico Diario: Avances de la Vacunación en México, 26 de Abril del 2021. Available online: https://coronavirus.gob.mx/2021/04/26/conferencia-26-de-abril-3/ (accessed on 26 November 2021). (In Spanish).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cases HCWs | % | Cases Non-HCWs | % | Deaths HCWs | % | Deaths Non-HCWs | % | |
|---|---|---|---|---|---|---|---|---|
| Gender | ||||||||
| Female | 145,913 | 62 | 1,017,792 | 50 | 1187 | 31 | 80,679 | 37.50 |
| Male | 89,430 | 38 | 1,076,399 | 50 | 2642 | 69 | 134,434 | 62.50 |
| Age groups | ||||||||
| <25 | 9386 | 3.99 | 283,650 | 12.18 | 5 | 0.13 | 1455 | 0.68 |
| 25–29 | 36,569 | 15.54 | 244,530 | 10.50 | 39 | 1.02 | 1603 | 0.75 |
| 30–34 | 42,090 | 17.88 | 253,137 | 10.87 | 104 | 2.72 | 3077 | 1.43 |
| 35–39 | 39,531 | 16.80 | 244,772 | 10.51 | 164 | 4.28 | 5104 | 2.37 |
| 40–44 | 33,174 | 14.10 | 232,282 | 9.97 | 275 | 7.18 | 8522 | 3.96 |
| 45–49 | 27,492 | 11.68 | 241,293 | 10.36 | 416 | 10.86 | 14,224 | 6.61 |
| 50–54 | 20,683 | 8.79 | 213,915 | 9.18 | 492 | 12.85 | 19,204 | 8.93 |
| 55–59 | 13,474 | 5.73 | 181,431 | 7.79 | 613 | 16.01 | 25,206 | 11.72 |
| 60–64 | 7524 | 3.20 | 139,753 | 6.00 | 647 | 16.90 | 29,720 | 13.82 |
| 65–69 | 3432 | 1.46 | 105,802 | 4.54 | 566 | 14.78 | 30,443 | 14.15 |
| 70–74 | 1214 | 0.52 | 77,002 | 3.31 | 286 | 7.47 | 27,609 | 12.83 |
| 75–79 | 456 | 0.19 | 53,345 | 2.29 | 125 | 3.26 | 21,931 | 10.20 |
| 80–84 | 187 | 0.08 | 32,785 | 1.41 | 62 | 1.62 | 14,877 | 6.92 |
| 85–89 | 86 | 0.04 | 17,296 | 0.74 | 28 | 0.73 | 8327 | 3.87 |
| 90–94 | 30 | 0.01 | 6356 | 0.27 | 7 | 0.18 | 2975 | 1.38 |
| >94 | 15 | 0.01 | 2185 | 0.09 | 0 | 0.00 | 836 | 0.39 |
| TOTAL | 235,343 | 100 | 2,094,191 | 100 | 3829 | 100 | 211,284 | 100 |
| HCWs | Non-HCWs | |||||
|---|---|---|---|---|---|---|
| Variable | May 2020–1st Half November 2020 (Mean) | 2nd Half November 2020–April 2021 (Mean) | p-Value | May 2020–1st Half November 2020 (Mean) | 2nd Half November 2020–April 2021 (Mean) | p-Value |
| Total new cases COVID-19 | 7909 | 3857 | 0.105 | 40,507 | 72,426 | 0.103 |
| Female new cases | 4817 | 2479 | 0.189 | 19,891 | 36,512 | 0.076 |
| Male new cases | 3093 | 1379 | * 0.040 | 20,616 | 35,911 | 0.168 |
| New cases with at least 1 comorbidity | 2689 | 1249 | 0.177 | 17,776 | 31,866 | 0.089 |
| New cases with no comorbidity | 5220 | 2608 | 0.294 | 22,731 | 40,557 | 0.119 |
| Total new deaths | 105 | 86 | 0.380 | 4549 | 5117 | 0.432 |
| Female new deaths | 32 | 28 | 0.218 | 1733 | 1825 | 0.892 |
| Male new deaths | 74 | 58 | 0.387 | 2816 | 3233 | 0.321 |
| Cases HCWs | % | Cases Non-HCWs | % | |
|---|---|---|---|---|
| Comorbidities | ||||
| None | 156,597 | 66.54 | 1,172,747 | 56 |
| Cases with at least 1 or more | 78,746 | 33.46 | 921,444 | 44 |
| Obesity | 35,960 | 15.28 | 299,469 | 14.3 |
| Hypertension | 25,817 | 10.97 | 360,201 | 17.2 |
| Diabetes | 16,097 | 6.84 | 278,527 | 13.3 |
| Smoking | 15,250 | 6.48 | 152,876 | 7.3 |
| Asthma | 8543 | 3.63 | 46,072 | 2.2 |
| COPD | 2524 | 1.08 | 31,413 | 1.5 |
| Immunosuppression | 1506 | 0.64 | 16,754 | 0.8 |
| Chronic kidney disease | 1153 | 0.49 | 31,413 | 1.5 |
| Cardiovascular disease | 871 | 0.37 | 23,036 | 1.1 |
| HIV/AIDS | 541 | 0.23 | 6238 | 0.3 |
| Occupation | Cases HCWs | % | Deaths HCWs | % |
|---|---|---|---|---|
| Nurses | 93,432 | 39.7 | 728 | 19 |
| Physicians | 61,189 | 26 | 1761 | 46 |
| Laboratory personnel | 4942 | 2.1 | 77 | 2 |
| Dentist | 3765 | 1.6 | 114 | 3 |
| Others | 72,015 | 30.6 | 1149 | 30 |
| Total | 235,343 | 100 | 3829 | 100 |
| Healthcare Workers by Occupation | |||
|---|---|---|---|
| Variable | May 2020–1st Half November 2020 (Mean) | 2nd Half November 2020–Apr 2021 (Mean) | p-Value |
| Physicians total new cases | 2057 | 1003 | 0.097 |
| Dentists total new cases | 79 | 109 | 0.576 |
| Nurses total new cases | 3243 | 1429 | 0.067 |
| Others total new cases | 2373 | 1228 | 0.189 |
| Physicians total new deaths | 52 | 36 | 0.852 |
| Dentists total new deaths | 2 | 2 | 0.363 |
| Nurses total new deaths | 19 | 17 | 0.478 |
| Others total new deaths | 31 | 27 | 0.575 |
| Type Personnel | SINERHIAS IMSS, ISSSTE March 2020 | INSABI * April 2020 | SEMAR September 2020 | ISSSTE September 2020 | Operation Chapultepec-IMSS December 2020 |
|---|---|---|---|---|---|
| Physicians | 37,596 | -- | -- | -- | -- |
| Nurses in contact | 112,042 | -- | -- | -- | -- |
| Urgenciologists | 1284 | -- | -- | -- | -- |
| Pulmonologists | 207 | -- | -- | -- | -- |
| Infectologists | 174 | -- | -- | -- | -- |
| Epidemiologists | 440 | -- | -- | -- | -- |
| Supportive healthcare workers | -- | 17,563 | -- | -- | 620 |
| Hiring healthcare workers in hospitals | -- | 4039 | 500 | 4331 | -- |
| Total | 151,743 | 21,602 | 500 | 4331 | * 620 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esquivel-Chirino, C.; Valero-Princet, Y.; Gaitán-Cepeda, L.A.; Hernández-Hernández, C.; Hernández, A.M.; Laparra-Escareño, H.; Ventura-Gallegos, J.L.; Montes-Sánchez, D.; Lopéz-Macay, A.; Hernández-Sánchez, F.; et al. The Effects of COVID-19 on Healthcare Workers and Non-Healthcare Workers in Mexico: 14 Months into the Pandemic. Medicina 2021, 57, 1353. https://doi.org/10.3390/medicina57121353
Esquivel-Chirino C, Valero-Princet Y, Gaitán-Cepeda LA, Hernández-Hernández C, Hernández AM, Laparra-Escareño H, Ventura-Gallegos JL, Montes-Sánchez D, Lopéz-Macay A, Hernández-Sánchez F, et al. The Effects of COVID-19 on Healthcare Workers and Non-Healthcare Workers in Mexico: 14 Months into the Pandemic. Medicina. 2021; 57(12):1353. https://doi.org/10.3390/medicina57121353
Chicago/Turabian StyleEsquivel-Chirino, César, Yolanda Valero-Princet, Luis Alberto Gaitán-Cepeda, Carlos Hernández-Hernández, Alejandro Macías Hernández, Hugo Laparra-Escareño, José Luis Ventura-Gallegos, Delina Montes-Sánchez, Ambar Lopéz-Macay, Fernando Hernández-Sánchez, and et al. 2021. "The Effects of COVID-19 on Healthcare Workers and Non-Healthcare Workers in Mexico: 14 Months into the Pandemic" Medicina 57, no. 12: 1353. https://doi.org/10.3390/medicina57121353
APA StyleEsquivel-Chirino, C., Valero-Princet, Y., Gaitán-Cepeda, L. A., Hernández-Hernández, C., Hernández, A. M., Laparra-Escareño, H., Ventura-Gallegos, J. L., Montes-Sánchez, D., Lopéz-Macay, A., Hernández-Sánchez, F., Oliveira, W. A. d., Morales-González, J. A., Carmona-Ruiz, D., Rosen-Esquivel, K., & Zentella-Dehesa, A. (2021). The Effects of COVID-19 on Healthcare Workers and Non-Healthcare Workers in Mexico: 14 Months into the Pandemic. Medicina, 57(12), 1353. https://doi.org/10.3390/medicina57121353