
BRAF, MEK, and EGFR Triplet Inhibitors as Salvage Therapy in BRAF-Mutated Metastatic Colorectal Cancer—A Case Series Study Target Therapy of BRAF-Mutated mCRC


 ,
,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. Patient Eligibility
2.2. Analysis of BRAF Mutation, RAS Mutation, and Status of Microsatellite Stability
2.3. Systemic Treatment and Outcome Assessment
2.4. Statistics
3. Results
3.1. Baseline Characteristics of Included Patients
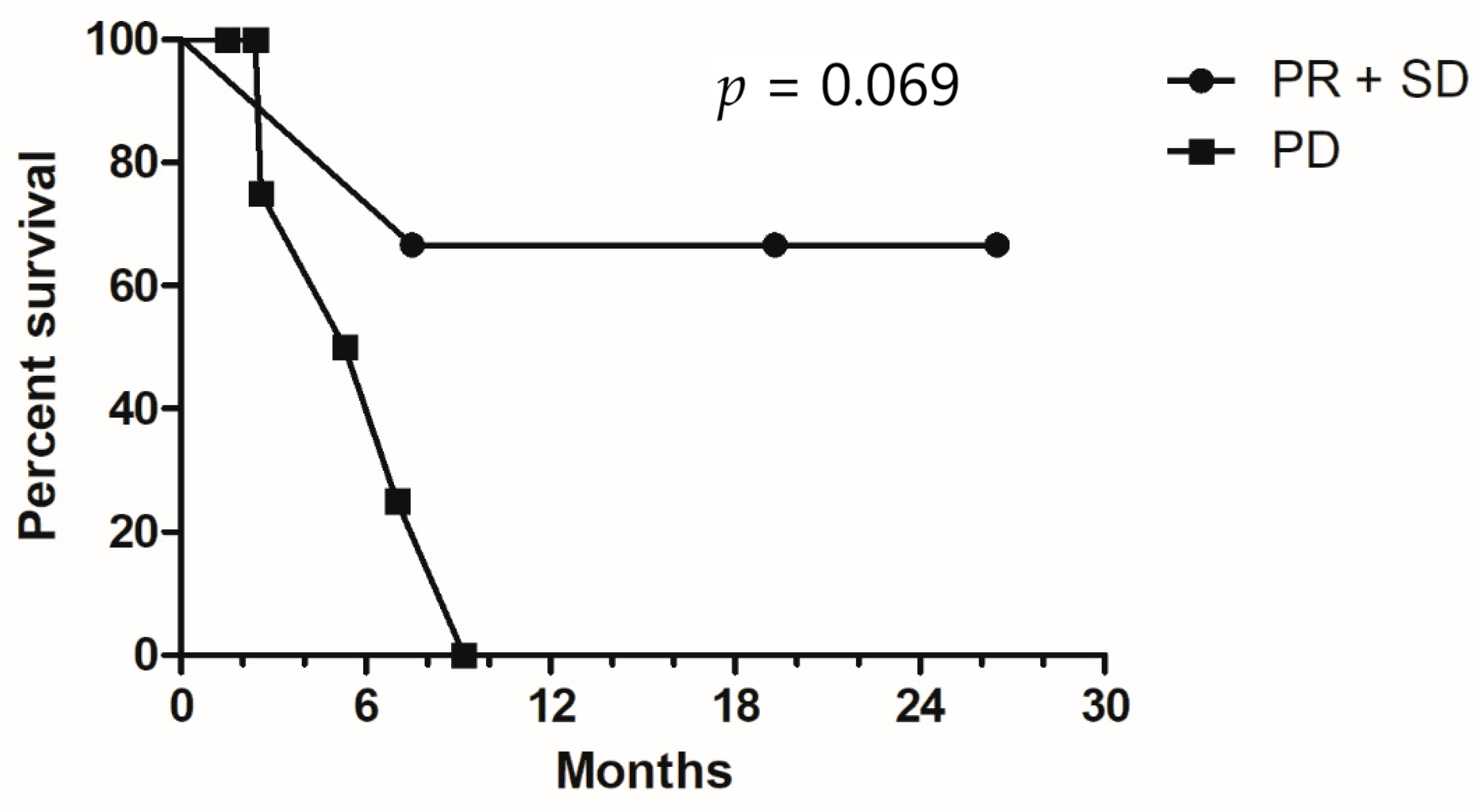
3.2. Response Rate and Survival Analysis
3.3. Adverse Events
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biller, L.H.; Schrag, D. Diagnosis and Treatment of Metastatic Colorectal Cancer: A Review. JAMA 2021, 325, 669–685. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Dahabreh, I.J.; Terasawa, T.; Castaldi, P.J.; Trikalinos, T.A. Systematic review: Anti-epidermal growth factor receptor treatment effect modification by KRAS mutations in advanced colorectal cancer. Ann. Intern. Med. 2011, 154, 37–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tougeron, D.; Lecomte, T.; Pagès, J.C.; Villalva, C.; Collin, C.; Ferru, A.; Tourani, J.M.; Silvain, C.; Levillain, P.; Karayan-Tapon, L. Effect of low-frequency KRAS mutations on the response to anti-EGFR therapy in metastatic colorectal cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2013, 24, 1267–1273. [Google Scholar] [CrossRef] [PubMed]
- André, T.; Shiu, K.-K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N. Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef] [PubMed]
- Nazemalhosseini Mojarad, E.; Kashfi, S.M.; Mirtalebi, H.; Taleghani, M.Y.; Azimzadeh, P.; Savabkar, S.; Pourhoseingholi, M.A.; Jalaeikhoo, H.; Aghdaei, H.A.; Kuppen, P.J.K.; et al. Low Level of Microsatellite Instability Correlates with Poor Clinical Prognosis in Stage II Colorectal Cancer Patients. J. Oncol. 2016, 2016, 2196703. [Google Scholar]
- Yuan, Z.X.; Wang, X.Y.; Qin, Q.Y.; Chen, D.F.; Zhong, Q.H.; Wang, L.; Wang, J.P. The prognostic role of BRAF mutation in metastatic colorectal cancer receiving anti-EGFR monoclonal antibodies: A meta-analysis. PLoS ONE 2013, 8, e65995. [Google Scholar] [CrossRef] [Green Version]
- Chu, J.E.; Johnson, B.; Kugathasan, L.; Morris, V.K.; Raghav, K.; Swanson, L.; Lim, H.J.; Renouf, D.J.; Gill, S.; Wolber, R.; et al. Population-based Screening for BRAF (V600E) in Metastatic Colorectal Cancer Reveals Increased Prevalence and Poor Prognosis. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2020, 26, 4599–4605. [Google Scholar] [CrossRef]
- Modest, D.P.; Ricard, I.; Heinemann, V.; Hegewisch-Becker, S.; Schmiegel, W.; Porschen, R.; Stintzing, S.; Graeven, U.; Arnold, D.; von Weikersthal, L.F.; et al. Outcome according to KRAS-, NRAS- and BRAF-mutation as well as KRAS mutation variants: Pooled analysis of five randomized trials in metastatic colorectal cancer by the AIO colorectal cancer study group. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 1746–1753. [Google Scholar] [CrossRef]
- Gavin, P.G.; Colangelo, L.H.; Fumagalli, D.; Tanaka, N.; Remillard, M.Y.; Yothers, G.; Kim, C.; Taniyama, Y.; Kim, S.I.; Choi, H.J.; et al. Mutation profiling and microsatellite instability in stage II and III colon cancer: An assessment of their prognostic and oxaliplatin predictive value. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2012, 18, 6531–6541. [Google Scholar] [CrossRef] [Green Version]
- Kopetz, S.; Grothey, A.; Yaeger, R.; Van Cutsem, E.; Desai, J.; Yoshino, T.; Wasan, H.; Ciardiello, F.; Loupakis, F.; Hong, Y.S.; et al. Encorafenib, Binimetinib, and Cetuximab in BRAF V600E-Mutated Colorectal Cancer. N. Engl. J. Med. 2019, 381, 1632–1643. [Google Scholar] [CrossRef] [Green Version]
- Corcoran, R.B.; Atreya, C.E.; Falchook, G.S.; Kwak, E.L.; Ryan, D.P.; Bendell, J.C.; Hamid, O.; Messersmith, W.A.; Daud, A.; Kurzrock, R.; et al. Combined BRAF and MEK Inhibition with Dabrafenib and Trametinib in BRAF V600-Mutant Colorectal Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 4023–4031. [Google Scholar] [CrossRef] [Green Version]
- Yaeger, R.; Cercek, A.; O’Reilly, E.M.; Reidy, D.L.; Kemeny, N.; Wolinsky, T.; Capanu, M.; Gollub, M.J.; Rosen, N.; Berger, M.F.; et al. Pilot trial of combined BRAF and EGFR inhibition in BRAF-mutant metastatic colorectal cancer patients. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2015, 21, 1313–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corcoran, R.B.; André, T.; Atreya, C.E.; Schellens, J.H.M.; Yoshino, T.; Bendell, J.C.; Hollebecque, A.; McRee, A.J.; Siena, S.; Middleton, G.; et al. Combined BRAF, EGFR, and MEK Inhibition in Patients with BRAF(V600E)-Mutant Colorectal Cancer. Cancer Discov. 2018, 8, 428–443. [Google Scholar] [CrossRef] [Green Version]
- Grothey, A.; Tabernero, J.; Taieb, J.; Yaeger, R.; Yoshino, T.; Maiello, E.; Fernandez, E.E.; Casado, A.R.; Ross, P.; André, T.; et al. LBA-5 ANCHOR CRC: A single-arm, phase 2 study of encorafenib, binimetinib plus cetuximab in previously untreated BRAF V600E-mutant metastatic colorectal cancer. Ann. Oncol. 2020, 31, S242–S243. [Google Scholar] [CrossRef]
- Hsieh, Y.-C.; Chang, T.-K.; Su, W.-C.; Huang, C.-W.; Tsai, H.-L.; Chen, Y.-C.; Li, C.-C.; Chen, P.-J.; Yin, T.-C.; Ma, C.-J.; et al. UGT1A1 Polymorphism for Irinotecan Dose Escalation in Patients with BRAF-Mutated Metastatic Colorectal Cancer Treated with First-Line Bevacizumab and FOLFIRI. J. Oncol. 2021, 2021, 6686517. [Google Scholar] [CrossRef]
- Chuang, S.-C.; Huang, C.-W.; Chen, Y.-T.; Ma, C.-J.; Tsai, H.-L.; Chang, T.-K.; Su, W.-C.; Hsu, W.-H.; Kuo, C.-H.; Wang, J.-Y. Effect of KRAS and NRAS mutations on the prognosis of patients with synchronous metastatic colorectal cancer presenting with liver-only and lung-only metastases. Oncol. Lett. 2020, 20, 2119–2130. [Google Scholar] [CrossRef] [PubMed]
- Weissman, S.M.; Bellcross, C.; Bittner, C.C.; Freivogel, M.E.; Haidle, J.L.; Kaurah, P.; Leininger, A.; Palaniappan, S.; Steenblock, K.; Vu, T.M.; et al. Genetic counseling considerations in the evaluation of families for Lynch syndrome—A review. J. Genet. Couns. 2011, 20, 5–19. [Google Scholar] [CrossRef]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; Van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotani, D.; Bando, H.; Masuishi, T.; Komatsu, Y.; Yamaguchi, K.; Nakajima, T.; Satoh, T.; Nishina, T.; Esaki, T.; Nomura, S.; et al. BIG BANG study: A multicenter phase II study of the MEK inhibitor binimetinib + BRAF inhibitor encorafenib + anti-EGFR antibody cetuximab in patients with BRAF non-V600E mutated metastatic colorectal cancer (EPOC 1703). Ann. Oncol. 2018, 29, viii201–viii202. [Google Scholar] [CrossRef]
- Loupakis, F.; Intini, R.; Cremolini, C.; Orlandi, A.; Sartore-Bianchi, A.; Pietrantonio, F.; Pella, N.; Spallanzani, A.; Dell’Aquila, E.; Scartozzi, M.; et al. A validated prognostic classifier for V600EBRAF-mutated metastatic colorectal cancer: The ‘BRAF BeCool’ study. Eur. J. Cancer 2019, 118, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Brulé, S.; Jonker, D.; Karapetis, C.; O’Callaghan, C.; Moore, M.; Wong, R.; Tebbutt, N.; Underhill, C.; Yip, D.; Zalcberg, J.; et al. Location of colon cancer (right-sided versus left-sided) as a prognostic factor and a predictor of benefit from cetuximab in NCIC CO.17. Eur J. Cancer 2015, 51, 1405–1414. [Google Scholar] [CrossRef]
- Ulivi, P.; Scarpi, E.; Chiadini, E.; Marisi, G.; Valgiusti, M.; Capelli, L.; Gardini, A.C.; Monti, M.; Ruscelli, S.; Frassineti, G.L.; et al. Right- vs. Left-Sided Metastatic Colorectal Cancer: Differences in Tumor Biology and Bevacizumab Efficacy. Int. J. Mol. Sci. 2017, 18, 1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venook, A.P.; Niedzwiecki, D.; Innocenti, F.; Fruth, B.; Greene, C.; O’Neil, B.H.; Shaw, J.E.; Atkins, J.N.; Horvath, L.E.; Polite, B.N.; et al. Impact of primary (1º) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts) with metastatic colorectal cancer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). J. Clin. Oncol. 2016, 34 (Suppl. 15), 3504. [Google Scholar] [CrossRef]
- Stintzing, S.; Heinrich, K.; Tougeron, D.; Modest, D.P.; Schwaner, I.; Euker, J.; Pihusch, R.; Stauch, M.; Kaiser, F.; Kahl, C.; et al. Randomized study to investigate FOLFOXIRI plus either bevacizumab or cetuximab as first-line treatment of BRAF V600E-mutant mCRC: The phase-II FIRE-4.5 study (AIO KRK-0116). J. Clin. Oncol. 2021, 39 (Suppl. 15), 3502. [Google Scholar] [CrossRef]
- Yaeger, R.; Kotani, D.; Mondaca, S.; Parikh, A.R.; Bando, H.; Van Seventer, E.E.; Taniguchi, H.; Zhao, H.; Thant, C.N.; De Stanchina, E.; et al. Response to Anti-EGFR Therapy in Patients with BRAF non-V600–Mutant Metastatic Colorectal Cancer. Clin. Cancer Res. 2019, 25, 7089–7097. [Google Scholar] [CrossRef] [Green Version]
- Morris, V.; Overman, M.J.; Jiang, Z.-Q.; Garrett, C.; Agarwal, S.; Eng, C.; Kee, B.; Fogelman, D.; Dasari, A.; Wolff, R.; et al. Progression-free survival remains poor over sequential lines of systemic therapy in patients with BRAF-mutated colorectal cancer. Clin. Colorectal Cancer 2014, 13, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Van Cutsem, E.; Huijberts, S.; Grothey, A.; Yaeger, R.; Cuyle, P.J.; Elez, E.; Fakih, M.; Montagut, C.; Peeters, M.; Yoshino, T.; et al. Binimetinib, Encorafenib, and Cetuximab Triplet Therapy for Patients with BRAF V600E-Mutant Metastatic Colorectal Cancer: Safety Lead-in Results from the Phase III BEACON Colorectal Cancer Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 1460–1469. [Google Scholar] [CrossRef]
- Fanelli, G.N.; Pozzo, C.A.D.; Depetris, I.; Schirripa, M.; Brignola, S.; Biason, P.; Balistreri, M.; Santo, L.D.; Lonardi, S.; Munari, G.; et al. The heterogeneous clinical and pathological landscapes of metastatic Braf-mutated colorectal cancer. Cancer Cell Int. 2020, 20, 30. [Google Scholar] [CrossRef]
- Middleton, G.; Yang, Y.; Campbell, C.D.; André, T.; Atreya, C.E.; Schellens, J.H.M.; Yoshino, T.; Bendell, J.C.; Hollebecque, A.; McRee, A.J.; et al. BRAF-Mutant Transcriptional Subtypes Predict Outcome of Combined BRAF, MEK, and EGFR Blockade with Dabrafenib, Trametinib, and Panitumumab in Patients with Colorectal Cancer. Clin. Cancer Res. 2020, 26, 2466. [Google Scholar] [CrossRef] [Green Version]
- Booth, A.E.C.; Hopkins, A.M.; Rowland, A.; Kichenadasse, G.; Smith, J.R.; Sorich, M.J. Risk factors for MEK-associated retinopathy in patients with advanced melanoma treated with combination BRAF and MEK inhibitor therapy. Ther. Adv. Med. Oncol. 2020, 12, 1758835920944359. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristic | All Patients (N = 9) | Right Side Tumor (N = 4) | Left Side Tumor (N = 5) | p Value |
|---|---|---|---|---|
| Gender (Male: Female) | 4:5 | 3:1 | 1:4 | 0.099 |
| Age (years) Median ± SD (range) | 51 ± 14.4 (35–81) | 52.5 ± 5.8 (45–59) | 45 ± 19.7 (35–81) | 0.730 |
| BMI kg/m2 Mean ± SD | 22.7 ± 6.4 | 22.8 ± 3.5 | 22.6 ± 8.5 | 1.000 |
| Histology Moderately differentiated Poorly differentiated | 7 (77.7%) 2 (22.2%) | 3 (75%) 1 (25%) | 4 (80%) 1 (20%) | 0.858 |
| Stage at triplet therapy 4A 4B 4C | 4 (44.4%) 3 (33.3%) 2 (22.2%) | 2 (50%) 1 (25%) 1 (25%) | 2 (40%) 2 (40%) 1 (20%) | 0.894 |
| Involvement of ≥3 organs | 4 (44.4%) | 2 (50%) | 2 (40%) | 0.764 |
| Liver metastasis | 7 (77.7%) | 3 (75%) | 4 (75%) | 0.858 |
| Primary tumor resection Complete resection Partial or no resection | 5 (55.5%) 4 (44.4%) | 2 (50%) 2 (50%) | 3 (60%) 2 (40%) | 0.764 |
| Baseline CEA > 5 μg/L | 8 (88.8%) | 3 (75%) | 5 (100%) | 0.236 |
| Response Partial response Stable disease Progressive disease | 1 (11.1%) 2 (22.2%) 6 (66.6%) | 0 1 (25%) 3 (75%) | 1 (20%) 1 (20%) 3 (60%) | 0.638 |
| Responder Non-responder | 1 (11.1%) 8 (88.8%) | 0 4 (100%) | 1 (20%) 4 (80%) | 0.343 |
| Disease control rate | 3 (33.3%) | 1 (25%) | 2 (40%) | 0.635 |
| Age (Year) /Sex | Tumor Location | Primary Surgery | Metastasis Foci | dMMR | Best Response | PFS (Months) | OS (Months) | |
|---|---|---|---|---|---|---|---|---|
| Patient 1 | 51, female | Right colon | No | Liver, lung, pancreas | ND | SD | 6.9 | 7.5 |
| Patient 2 | 45, female | Left colon | No | Liver, lung | No | PD | 2.3 | 5.3 |
| Patient 3 | 81, female | Left colon | R0 resection | Liver, lung | Yes | SD | 19.3 | 19.3 |
| Patient 4 | 41, male | Left colon | R0 resection | Liver, lung, adrenal gland, pancreas | No | PR | 5.4 | 26.5 |
| Patient 5 | 59, male | Right colon | R0 resection | Liver, peritoneum, pancreas | ND | PD | 3.1 | 7.0 |
| Patient 6 | 45, male | Right colon | R0 resection | Liver, peritoneum, | No | PD | 1.5 | 1.5 |
| Patient 7 | 54, male | Right colon | R1 resection | Peritoneum, Paraaortic lymph nodes | No | PD | 2.6 | 2.6 |
| Patient 8 | 35, female | Left colon | R0 resection | Peritoneum | Yes | PD | 2.4 | 2.4 |
| Patient 9 | 69, female | Left colon | No | Liver, lung, peritoneum, bone | ND | PD | 3.0 | 9.2 |
| Adverse Events | Grade 1–2 (%) | Grade 3 (%) † | Any Grade (%) |
|---|---|---|---|
| Anemia | 1 (11.1) | 0 (0) | 1 (11.1) |
| Neutropenia | 0 (0) | 0 (0) | 0 (0) |
| Thrombocytopenia | 0 (0) | 0 (0) | 0 (0) |
| Fatigue | 0 (0) | 0 (0) | 0 (0) |
| Nausea | 2 (22.2) | 2 (22.2) | 4 (44.4) |
| Vomiting | 3 (33.3) | 0 (0) | 3 (33.3) |
| Hair loss | 1 (11.1) | 0 (0) | 1 (11.1) |
| Abnormal liver function | 6 (66.6) | 0 (0) | 6 (66.6) |
| Acute kidney injury | 2 (22.2) | 0 (0) | 2 (22.2) |
| Hypertension | 4 (44.4) | 2 (22.2) | 6 (66.6) |
| Diarrhea | 1 (11.1) | 1 (11.1) | 2 (22.2) |
| Paresthesia | 2 (22.2) | 0 (0) | 2 (22.2) |
| Skin rash | 4 (44.4) | 0 (0) | 4 (44.4) |
| Dermatitis | 4 (44.4) | 2 (22.2) | 6 (66.6) |
| Blurred vision | 1 (11.1) | 0 (0) | 1 (11.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, J.-H.; Tsai, H.-L.; Chen, Y.-C.; Li, C.-C.; Huang, C.-W.; Chang, T.-K.; Su, W.-C.; Chen, P.-J.; Liu, Y.-P.; Wang, J.-Y. BRAF, MEK, and EGFR Triplet Inhibitors as Salvage Therapy in BRAF-Mutated Metastatic Colorectal Cancer—A Case Series Study Target Therapy of BRAF-Mutated mCRC. Medicina 2021, 57, 1339. https://doi.org/10.3390/medicina57121339
Yeh J-H, Tsai H-L, Chen Y-C, Li C-C, Huang C-W, Chang T-K, Su W-C, Chen P-J, Liu Y-P, Wang J-Y. BRAF, MEK, and EGFR Triplet Inhibitors as Salvage Therapy in BRAF-Mutated Metastatic Colorectal Cancer—A Case Series Study Target Therapy of BRAF-Mutated mCRC. Medicina. 2021; 57(12):1339. https://doi.org/10.3390/medicina57121339
Chicago/Turabian StyleYeh, Jen-Hao, Hsiang-Lin Tsai, Yen-Cheng Chen, Ching-Chun Li, Ching-Wen Huang, Tsung-Kun Chang, Wei-Chih Su, Po-Jung Chen, Yu-Peng Liu, and Jaw-Yuan Wang. 2021. "BRAF, MEK, and EGFR Triplet Inhibitors as Salvage Therapy in BRAF-Mutated Metastatic Colorectal Cancer—A Case Series Study Target Therapy of BRAF-Mutated mCRC" Medicina 57, no. 12: 1339. https://doi.org/10.3390/medicina57121339
APA StyleYeh, J.-H., Tsai, H.-L., Chen, Y.-C., Li, C.-C., Huang, C.-W., Chang, T.-K., Su, W.-C., Chen, P.-J., Liu, Y.-P., & Wang, J.-Y. (2021). BRAF, MEK, and EGFR Triplet Inhibitors as Salvage Therapy in BRAF-Mutated Metastatic Colorectal Cancer—A Case Series Study Target Therapy of BRAF-Mutated mCRC. Medicina, 57(12), 1339. https://doi.org/10.3390/medicina57121339