
Fibromuscular Dysplasia/Carotid Web in Angio-CT Imaging: A Rare Cause of Ischemic Stroke


Abstract
:1. Introduction
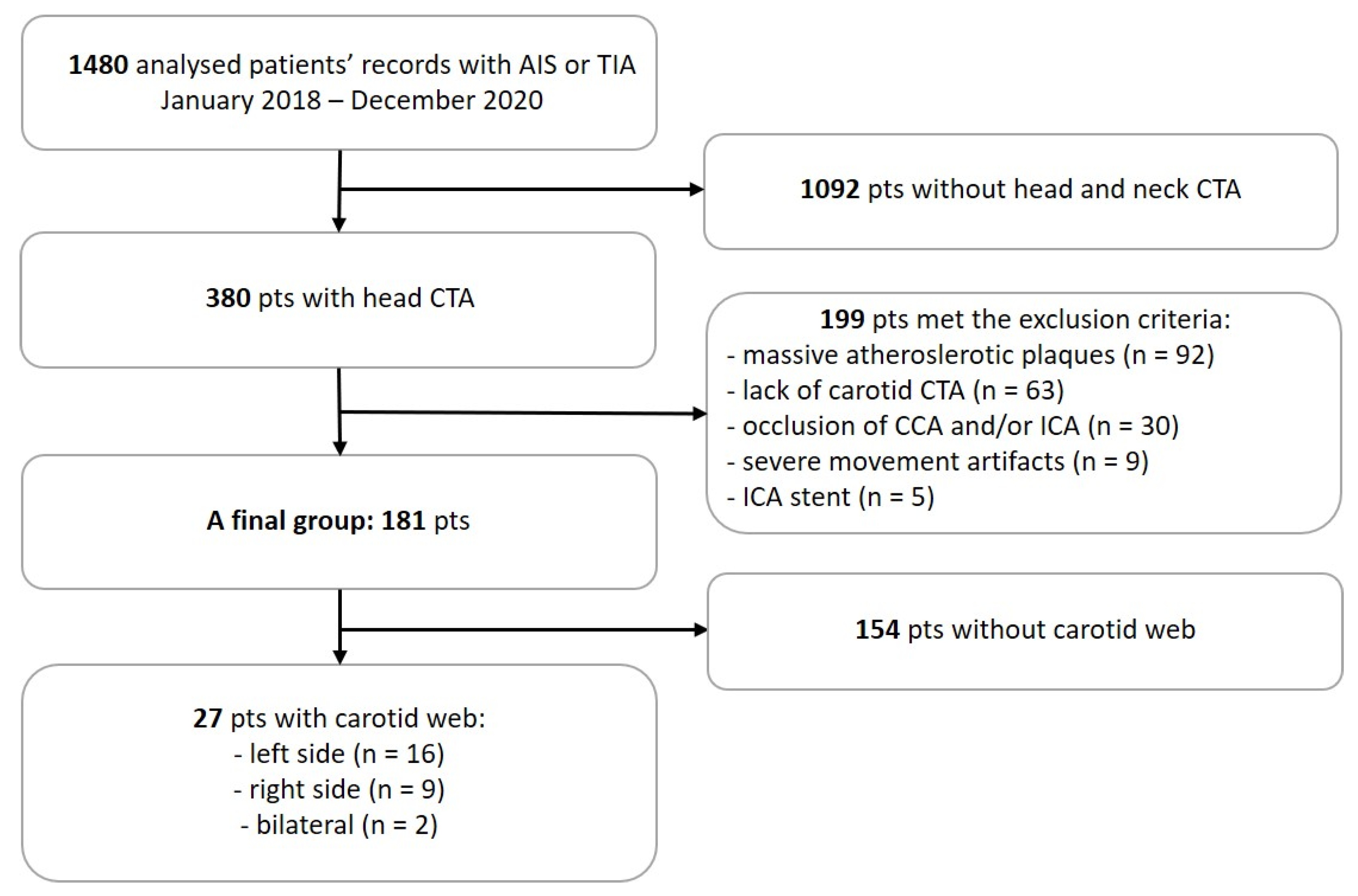
2. Materials and Methods
3. Results
3.1. The Prevalence of CaW
3.2. CaW and Non-CaW Groups
3.3. CaW and Cryptogenic and Recurrent Stroke
3.4. CaW and Risk Factors
3.5. AIS and TIA Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Błażejewska-Hyżorek, B.; Czernuszenko, A.; Członkowska, A.; Ferens, A.; Gąsecki, D.; Kaczorowski, R.; Karaszewski, B.; Karliński, M.; Kaźmierski, R.; Kłysz, B.; et al. Wytyczne postępowania w udarze mózgu. Pol. Przegląd Neurol. 2019, 15, 1–156. [Google Scholar] [CrossRef]
- Kim, J.; Thayabaranathan, T.; Donnan, G.A.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.; Norrving, B.; Owolabi, M.; Pandian, J.; et al. Global Stroke Statistics 2019. Int. J. Stroke 2020, 15, 819–838. [Google Scholar] [CrossRef] [PubMed]
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.; Culebras, A.; Elkind, M.S.V.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An updated definition of stroke for the 21st century: A statement for healthcare professionals from the American heart association/American stroke association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, H.P.; Woolson, R.F.; Biller, J.; Clarke, W. Studies of org 10172 in patients with acute ischemic stroke. Pathophysiol. Haemost. Thromb. 1992, 22, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Ossowska, A.; Chwojnicki, K.; Nyka, W.M. Dysplazja włóknisto-mięśniowa—Rzadka przyczyna udaru mózgu. Varia Med. 2019, 3, 363–366. [Google Scholar]
- Pappaccogli, M.; Di Monaco, S.; Warchoł-Celińska, E.; Lorthioir, A.; Amar, L.; Aparicio, L.S.; Beauloye, C.; Bruno, R.M.; Chenu, P.; de Leeuw, P.; et al. The European/International Fibromuscular Dysplasia Registry and Initiative (FEIRI)—clinical phenotypes and their predictors based on a cohort of 1000 patients. Cardiovasc. Res. 2021, 117, 950–959. [Google Scholar] [CrossRef]
- Shah, K.P.; Peruri, A.; Kanneganti, M.; Gorsch, L.; Ramcharitar, R.; Williams, C.; Clouse, D.; Thomas, M.; Norton, P.T.; Hagspiel, K.D.; et al. Fibromuscular dysplasia: A comprehensive review on evaluation and management and role for multidisciplinary comprehensive care and patient input model. Semin. Vasc. Surg. 2021, 34, 89–96. [Google Scholar] [CrossRef]
- Choi, P.M.C.; Singh, D.; Trivedi, A.; Qazi, E.; George, D.; Wong, J.; Demchuk, A.M.; Goyal, M.; Hill, M.D.; Menon, B.K. Carotid webs and recurrent ischemic strokes in the Era of CT angiography. Am. J. Neuroradiol. 2015, 36, 2134–2139. [Google Scholar] [CrossRef] [Green Version]
- Palubinskas, A.J.; Ripley, H.R. Fibromuscular Hyperplasia in Extrarenal Arteries. Radiology 1964, 82, 451–455. [Google Scholar] [CrossRef]
- Kim, S.J.; Nogueira, R.G.; Haussen, D.C. Current Understanding and Gaps in Research of Carotid Webs in Ischemic Strokes: A Review. JAMA Neurol. 2019, 76, 355–361. [Google Scholar] [CrossRef]
- Brott, T.; Adams, H.P.; Olinger, C.P.; Marle, J.R.; Barsan, W.G.; Biller, J.; Spilker, J.; Holleran, R.; Eberle, R.; Hertzberg, V.; et al. Measurements of acute cerebral infarction: A clinical examination scale. Stroke 1989, 20, 864–870. [Google Scholar] [CrossRef] [Green Version]
- Quinn, T.J.; Dawson, J.; Walters, M.R.; Lees, K.R. Reliability of the modified rankin scale: A systematic review. Stroke 2009, 40, 3393–3395. [Google Scholar] [CrossRef] [Green Version]
- Varennes, L.; Tahon, F.; Kastler, A.; Grand, S.; Thony, F.; Baguet, J.P.; Detante, O.; Touzé, E.; Krainik, A. Fibromuscular dysplasia: What the radiologist should know: A pictorial review. Insights Imaging 2015, 6, 295–307. [Google Scholar] [CrossRef] [Green Version]
- Wojcik, K.; Milburn, J.; Vidal, G.; Tarsia, J.; Steven, A. Survey of current management practices for carotid webs. Ochsner J. 2019, 19, 296–302. [Google Scholar] [CrossRef] [Green Version]
- Mei, J.; Chen, D.; Esenwa, C.; Gold, M.; Burns, J.; Zampolin, R.; Slasky, S.E. Carotid web prevalence in a large hospital-based cohort and its association with ischemic stroke. Clin. Anat. 2021, 34, 867–871. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Wang, B.; Zheng, S.; Kou, J.; Gu, X.; Liu, T. Carotid web and ischemic stroke: A CT angiography study. Clin. Imaging 2020, 67, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Olindo, S.; Marnat, G.; Chausson, N.; Turpinat, C.; Smadja, D.; Gaillard, N. Carotid webs associated with ischemic stroke. Updated general review and research directions. Rev. Neurol. 2021, 177, 627–638. [Google Scholar] [CrossRef]
- Fu, W.; Crockett, A.; Low, G.; Patel, V. Internal carotid artery web: Doppler ultrasound with CT angiography correlation. J. Radiol. Case Rep. 2015, 9, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Berge, E.; Whiteley, W.; Audebert, H.; De Marchis, G.M.; Fonseca, A.C.; Padiglioni, C.; de la Ossa, N.P.; Strbian, D.; Tsivgoulis, G.; Turc, G. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur. Stroke J. 2021, 6, I–LXII. [Google Scholar] [CrossRef]
- Mayer, S.A.; Viarasilpa, T.; Panyavachiraporn, N.; Brady, M.; Scozzari, D.; Van Harn, M.; Miller, D.; Katramados, A.; Hefzy, H.; Malik, S.; et al. CTA-for-All: Impact of Emergency Computed Tomographic Angiography for All Patients With Stroke Presenting Within 24 Hours of Onset. Stroke 2020, 51, 331–334. [Google Scholar] [CrossRef]
- Madaelil, T.P.; Grossberg, J.A.; Nogueira, R.G.; Anderson, A.; Barreira, C.; Frankel, M.; Haussen, D.C. Multimodality Imaging in Carotid Web. Front. Neurol. 2019, 10, 3–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haussen, D.C.; Grossberg, J.A.; Bouslama, M.; Pradilla, G.; Belagaje, S.; Bianchi, N.; Allen, J.W.; Frankel, M.; Nogueira, R.G. Carotid web (intimal Fibromuscular Dysplasia) has high stroke recurrence risk and is amenable to stenting. Stroke 2017, 48, 3134–3137. [Google Scholar] [CrossRef] [PubMed]
- Sajedi, P.; Chelala, L.; Nunez-Gonalez, J.; Cronin, C.; Kittner, S.; Zhuo, J.; Zhang, Y.; Gandhi, D.; Raghavan, P. Carotid webs and ischemic stroke: Experiences in a comprehensive stroke center. J. Neuroradiol. 2019, 46, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Compagne, K.C.J.; van Es, A.C.G.M.; Berkhemer, O.A.; Borst, J.; Roos, Y.B.W.E.; van Oostenbrugge, R.J.; van Zwam, W.H.; Majoie, C.B.L.M.; Marquering, H.A.; Dippel, D.W.J.; et al. Prevalence of carotid web in patients with acute intracranial stroke due to intracranial large vessel occlusion. Radiology 2018, 286, 1000–1007. [Google Scholar] [CrossRef] [Green Version]
- Phair, J.; Trestman, E.B.; Yean, C.; Lipsitz, E.C. Endarterectomy for a symptomatic carotid web. Vascular 2017, 25, 553–556. [Google Scholar] [CrossRef]
- Warchol-Celinska, E.; Prejbisz, A.; Dobrowolski, P.; Klisiewicz, A.; Kadziela, J.; Florczak, E.; Michalowska, I.; Jozwik-Plebanek, K.; Kabat, M.; Kwiatek, P.; et al. Systematic and multidisciplinary evaluation of fibromuscular dysplasia patients reveals high prevalence of previously undetected fibromuscular dysplasia lesions and affects clinical decisions: The ARCADIA-POL Study. Hypertension 2020, 75, 1102–1109. [Google Scholar] [CrossRef]


{kind=link}
| Study Group (n = 181) | |||
|---|---|---|---|
| Variable | CaW (n = 27) | no-CaW (n = 154) | p Value |
| Gender [n (%)] | 0.39 | ||
| Females | 16 (59%) | 78 (51%) | |
| Males | 11 (41%) | 76 (49%) | |
| Age [years] [n ± SD] | 66.70 ± 14.34 | 68.01 ± 13.40 | 0.73 |
| Pathology [n (%)] | |||
| Transient ischemic attack | 3 (11%) | 17 (11%) | - |
| Acute supratentorial ischemic stroke | 20 (74%) | 122 (79%) | - |
| Acute infratentorial ischemic stroke | 4 (15%) | 15 (10%) | - |
| NIHSS—admission [n ± SD] | 5.76 ± 4.05 | 7.51 ± 5.83 | 0.27 |
| NIHSS—discharge [n ± SD] | 2.88 ± 3.38 | 5.14 ± 6.14 | 0.13 |
| rtPA [n (%)] | 17 (63%) | 74 (48%) | 0.12 |
| Thrombectomy [n (%)] | 3 (11%) | 19 (12%) | 0.94 |
| Stroke side (supratentorial) [n (%)] 1,2 | 0.89 | ||
| Right | 10 (37%) | 59 (38%) | |
| Left | 10 (37%) | 63 (41%) | |
| Recurrent stroke [n (%)] | 7 (26%) | 28 (18%) | 0.38 |
| Cryptogenic stroke [n (%)] | 3 (11%) | 20 (13%) | 0.99 |
| Risk factors [n (%)] | |||
| Hypertension | 23 (85%) | 129 (84%) | 0.97 |
| Dyslipidemia | 14 (52%) | 80 (52%) | 0.71 |
| Atrial fibrillation | 5 (19%) | 25 (16%) | 0.64 |
| Diabetes mellitus | 4 (15%) | 48 (31%) | 0.12 |
| Smoking | 5 (19%) | 33 (21%) | 0.87 |
| Myocardial infarction | 3 (11%) | 27 (18%) | 0.49 |
| Ischemic heart disease | 8 (30%) | 62 (40%) | 0.43 |
| Arterial narrowing | 8 (30%) | 32 (21%) | 0.22 |
| Bloodwork results [n ± SD] | |||
| LDL cholesterol [mg/dL] | 130.08 ± 46.49 | 112.97 ± 49.38 | 0.06 |
| HDL cholesterol [mg/dL] | 52.96 ± 12.43 | 47.64 ± 15.60 | 0.02 |
| Total cholesterol [mg/dL] | 209.04 ± 50.33 | 183.65 ± 57.36 | 0.02 |
| Triglycerides [mg/dL] | 125.59 ± 65.05 | 124.88 ± 59.53 | 0.65 |
| Hb A1c [%] | 6.50 ± 0.43 | 7.27 ± 1.99 | - |
| Study Final Group (n = 181) | |||
|---|---|---|---|
| Variable | Females n = 94 (52%) | Males n = 87 (48%) | p * Value |
| Age [years] [n ± SD] | 72.00 ± 13.30 | 63.30 ± 12.29 | <0.01 |
| Pathology [n (%)] | |||
| Transient Ischemic Attack | 12 (13%) | 8 (9%) | 0.24 |
| Acute supratentorial ischemic stroke | 74 (79%) | 68 (78%) | 0.96 |
| Acute infratentorial ischemic stroke | 8 (8%) | 11 (13%) | 0.39 |
| NIHSS—admission [n ± SD] | 8.04 ± 6.32 | 6.38 ± 4.64 | 0.09 |
| NIHSS—discharge [n ± SD] | 5.77 ± 6.75 | 3.77 ± 4.54 | 0.09 |
| mRS [n ± SD] | 2.59 ± 2.05 | 1.86 ± 1.80 | 0.02 |
| rtPA [n (%)] | 48 (51%) | 43 (49%) | 0.54 |
| Thrombectomy [n (%)] | 12 (13%) | 10 (12%) | 0.69 |
| Supratentorial stroke site [n (%)] | 0.10 | ||
| Right | 31 (33%) | 38 (44%) | |
| Left | 43 (46%) | 30 (35%) | |
| Recurrent stroke [n (%)] | 18 (19%) | 17 (20%) | 0.93 |
| Cryptogenic stroke [n (%)] | 9 (10%) | 14 (16%) | 0.23 |
| Risk factors [n (%)] | |||
| Hypertension | 79 (84%) | 73 (84%) | 0.98 |
| Dyslipidemia | 49 (52%) | 45 (52%) | 0.96 |
| Atrial fibrillation | 24 (26%) | 6 (7%) | <0.01 * |
| Diabetes mellitus | 26 (28%) | 26 (30%) | 0.74 |
| Smoking | 14 (15%) | 24 (28%) | 0.04 |
| Myocardial infarction | 13 (14%) | 17 (20%) | 0.30 |
| Ischemic heart disease | 38 (40%) | 32 (37%) | 0.62 |
| Arterial narrowing | 17 (18%) | 23 (26%) | 0.18 |
| Bloodwork results [n ± SD] | |||
| LDL cholesterol [mg/dL] | 120.09 ± 51.67 | 110.86 ± 46.20 | 0.29 |
| HDL cholesterol [mg/dL] | 51.15 ± 12.30 | 45.51 ± 17.52 | <0.01 |
| Total cholesterol [mg/dL] | 196.08 ± 58.36 | 178.46 ± 54.17 | 0.05 |
| Triglycerides [mg/dL] | 120.28 ± 59.71 | 130.17 ± 60.75 | 0.26 |
| Hb A1c [%] | 7.40 ± 2.05 | 6.6 ± 1.14 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rzepka, M.; Chmiela, T.; Bosowska, J.; Cebula, M.; Krzystanek, E. Fibromuscular Dysplasia/Carotid Web in Angio-CT Imaging: A Rare Cause of Ischemic Stroke. Medicina 2021, 57, 1112. https://doi.org/10.3390/medicina57101112
Rzepka M, Chmiela T, Bosowska J, Cebula M, Krzystanek E. Fibromuscular Dysplasia/Carotid Web in Angio-CT Imaging: A Rare Cause of Ischemic Stroke. Medicina. 2021; 57(10):1112. https://doi.org/10.3390/medicina57101112
Chicago/Turabian StyleRzepka, Michalina, Tomasz Chmiela, Joanna Bosowska, Maciej Cebula, and Ewa Krzystanek. 2021. "Fibromuscular Dysplasia/Carotid Web in Angio-CT Imaging: A Rare Cause of Ischemic Stroke" Medicina 57, no. 10: 1112. https://doi.org/10.3390/medicina57101112
APA StyleRzepka, M., Chmiela, T., Bosowska, J., Cebula, M., & Krzystanek, E. (2021). Fibromuscular Dysplasia/Carotid Web in Angio-CT Imaging: A Rare Cause of Ischemic Stroke. Medicina, 57(10), 1112. https://doi.org/10.3390/medicina57101112