
A Seroprevalence Study of Anti-SARS-CoV-2 Antibodies in Patients with Inflammatory Bowel Disease during the Second Wave of the COVID-19 Pandemic in Italy

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
- (a)
- patients treated with a biologic drug, including: infliximab (IFX), adalimumab (ADA), golimumab (GOL), vedolizumab (VDZ), ustekinumab (UST) or any new experimental biologic drug being used in clinical trials;
- (b)
- patients treated with oral and/or topical mesalazine.
- -
- possible onset of COVID-19 related symptoms in the previous 30 days (headache, cough, sneezing, vomiting, ageusia/anosmia, fever, fatigue, dyspnea, arthromyalgia, diarrhea, conjunctivitis);
- -
- results of previous nasopharyngeal swabs (antigen or molecular tests);
- -
- flu vaccination;
- -
- any close contacts with individuals testing positive for SARS-CoV-2;
- -
- protective measures: use and type of personal protective equipment (PPE), average number of people in contact with daily [22].
2.2. Laboratory Analysis
2.3. Statistical Analysis
3. Results
3.1. Baseline Demographic and Disease Characteristics
3.2. COVID-19 Related Questionnaire Analysis
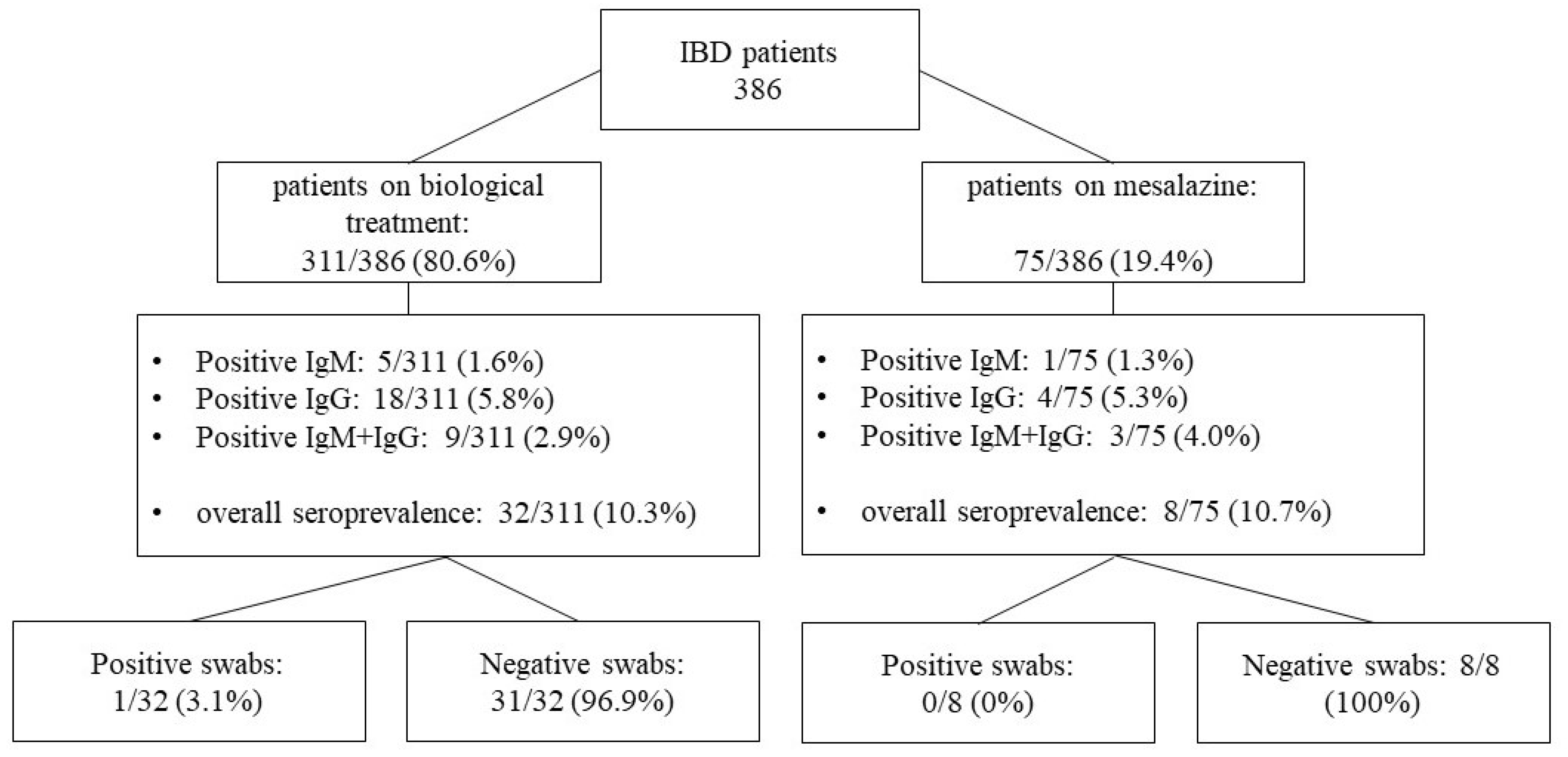
3.3. Anti-SARS-CoV-2 Antibodies Seroprevalence Analysis
3.4. COVID-19 Risk Factors Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ciotti, M.; Ciccozzi, M.; Terrinoni, A.; Jiang, W.C.; Wang, C.B.; Bernardini, S. The COVID-19 pandemic. Crit. Rev. Clin. Lab. Sci. 2020, 57, 365–388. [Google Scholar] [CrossRef] [PubMed]
- Gasmi, A.; Peana, M.; Pivina, L.; Srinath, S.; Benahmed, A.G.; Semenova, Y.; Menzel, A.; Dadar, M.; Bjørklund, G. Interrelations between COVID-19 and other disorders. Clin. Immunol. 2021, 224, 108651. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, K.H.; Papadakis, K.A. Inflammatory bowel disease: Updates on molecular targets for biologics. Gut Liver 2017, 11, 455–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirchgesner, J.; Lemaitre, M.; Carrat, F.; Zureik, M.; Carbonnel, F.; Dray-Spira, R. Risk of serious and opportunistic infections associated with treatment of inflammatory bowel diseases. Gastroenterology 2018, 155, 337–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, N.A.; Jones, G.-R.; Lamb, C.A.; Appleby, R.; Arnott, I.; Beattie, R.M.; Bloom, S.; Brooks, A.J.; Cooney, R.; Dart, R.J.; et al. British Society of Gastroenterology guidance for management of inflammatory bowel disease during the COVID-19 pandemic. Gut 2020, 69, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Danese, S.; Cecconi, M.; Spinelli, A. Management of IBD during the COVID-19 outbreak: Resetting clinical priorities. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 253–255. [Google Scholar] [CrossRef] [Green Version]
- Rubin, D.T.; Feuerstein, J.D.; Wang, A.Y.; Cohen, R.D. AGA Clinical practice update on management of inflammatory bowel disease during the COVID-19 pandemic: Expert commentary. Gastroenterology 2020, 159, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Bezzio, C.; Saibeni, S.; Variola, A.; Allocca, M.; Massari, A.; Gerardi, V.; Casini, V.; Ricci, C.; Zingone, F.; Amato, A.; et al. Outcomes of COVID-19 in 79 patients with IBD in Italy: An IG-IBD study. Gut 2020, 69, 1213–1217. [Google Scholar] [CrossRef]
- Brenner, E.J.; Ungaro, R.C.; Gearry, R.B.; Kaplan, G.G.; Kissous-Hunt, M.; Lewis, J.D.; Ng, S.C.; Rahier, J.-F.; Reinisch, W.; Ruemmele, F.M.; et al. Corticosteroids, but Not TNF antagonists, are associated with adverse COVID-19 outcomes in patients with inflammatory bowel diseases: Results from an international registry. Gastroenterology 2020, 159, 481–491. [Google Scholar] [CrossRef]
- Papa, A.; Gasbarrini, A.; Tursi, A. Epidemiology and the impact of therapies on the outcome of COVID-19 in patients with inflammatory bowel disease. Am. J. Gastroenterol. 2020, 115, 1722–1724. [Google Scholar] [CrossRef]
- Dramé, M.; Tabue Teguo, M.; Proye, E.; Hequet, F.; Hentzien, M.; Kanagaratnam, L.; Godaert, L. Should RT-PCR be considered a gold standard in the diagnosis of COVID-19? J. Med. Virol. 2020, 92, 2312–2313. [Google Scholar] [CrossRef]
- Petherick, A. Developing antibody tests for SARS-CoV-2. Lancet 2020, 395, 1101–1102. [Google Scholar] [CrossRef]
- Lee, Y.-L.; Liao, C.-H.; Liu, P.-Y.; Cheng, C.-Y.; Chung, M.-Y.; Liu, C.-E.; Chang, S.-Y.; Hsueh, P.-R. Dynamics of anti-SARS-Cov-2 IgM and IgG antibodies among COVID-19 patients. J. Infect. 2020, 81, 55–58. [Google Scholar] [CrossRef]
- McGregor, C.G.; Adams, A.; Sadler, R.; Arancibia-Cárcamo, C.V.; Palmer, R.; Ambrose, T.; Brain, O.; Walsh, A.; Klenerman, P.; Travis, S.P.; et al. Maintenance therapy with infliximab or vedolizumab in IBD is not associated with increased SARS-CoV-2 seroprevalence: UK experience in the 2020 pandemic. Gut 2021, 2021–324116. [Google Scholar] [CrossRef]
- Berte’, R.; Mazza, S.; Stefanucci, M.R.; Noviello, D.; Costa, S.; Ciafardini, C.; Mileti, E.; Mapelli, M.; Pasqualato, S.; Pinto, S.; et al. Seroprevalence of SARS-CoV2 in IBD patients treated with biological therapy. J. Crohn’s Colitis 2021, 15, 864–868. [Google Scholar] [CrossRef] [PubMed]
- Bossa, F.; Carparelli, S.; Latiano, A.; Palmieri, O.; Tavano, F.; Panza, A.; Pastore, M.; Marseglia, A.; D’Altilia, M.; Latiano, T.; et al. Impact of the COVID-19 outbreak and the serum prevalence of SARS-CoV-2 antibodies in patients with inflammatory bowel disease treated with biologic drugs. Dig. Liver Dis. 2021, 53, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Scucchi, L.; Neri, B.; Sarmati, L.; Mossa, M.; Sena, G.; Massoud, R.; Petruzziello, C.; Musumeci, M.; Marafini, I.; Calabrese, E.; et al. Low prevalence of SARS-CoV-2 infection in inflammatory bowel disease. Eur. Rev. Med. Pharm. Sci. 2021, 25, 2418–2424. [Google Scholar]
- Norsa, L.; Cosimo, P.; Indriolo, A.; Sansotta, N.; D’Antiga, L.; Callegaro, A. Asymptomatic Severe acute respiratory syndrome Coronavirus 2 infection in patients with inflammatory bowel disease under biologic treatment. Gastroenterology 2020, 159, 2229–2231. [Google Scholar] [CrossRef] [PubMed]
- Łodyga, M.; Maciejewska, K.; Eder, P.; Waszak, K.; Stawczyk-Eder, K.; Michalak, M.; Dobrowolska, A.; Wiśniewska-Jarosińska, M.; Gąsiorowska, A.; Cicha, M.; et al. Inflammatory bowel disease is associated with higher seroprevalence rates of antibodies against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Pol. Arch. Intern. Med. 2021, 131, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Ordás, I.; Eckmann, L.; Talamini, M.; Baumgart, D.C.; Sandborn, W.J. Ulcerative colitis. Lancet 2012, 380, 1606–1619. [Google Scholar] [CrossRef] [Green Version]
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Umakanthan, S.; Sahu, P.; Ranade, A.V.; Bukelo, M.M.; Rao, J.S.; Abrahao-Machado, L.F.; Dahal, S.; Kumar, H.; Kv, D. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad. Med. J. 2020, 96, 753–758. [Google Scholar] [CrossRef] [PubMed]
- The Combined Testing Solutions for the Detection of Antibodies to SARS-CoV-2. Available online: https://www.diasorin.com/en/immunodiagnostic-solutions/clinical-areas/infectious-diseases/covid-19. (accessed on 28 September 2021).
- Huyghe, E.; Jansens, H.; Matheeussen, V.; Hoffbauer, I.; Goossens, H.; Peeters, B. Performance of three automated SARS-CoV-2 antibody assays and relevance of orthogonal testing algorithms. Clin. Chem. Lab. Med. 2020, 59, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Carletti, M.; Pancrazi, R. Geographic negative correlation of estimated incidence between first and second waves of Coronavirus disease 2019 (COVID-19) in Italy. Mathematics 2021, 9, 133. [Google Scholar] [CrossRef]
- Ungaro, R.C.; Brenner, E.J.; Gearry, R.B.; Kaplan, G.G.; Kissous-Hunt, M.; Lewis, J.D.; Ng, S.C.; Rahier, J.-F.; Reinisch, W.; Steinwurz, F.; et al. Effect of IBD medications on COVID-19 outcomes: Results from an international registry. Gut 2021, 70, 725–732. [Google Scholar] [CrossRef] [PubMed]
- JM, A.A.; Vicente-Guijarro, J.; Peribáñez, B.; Haro, G.; Valencia-Martín, J.L.; Valdés, B. Masks as personal protective equipment in the COVID-19 pandemic: How, when and which should be used. J. Healthc. Qual. Res. 2020, 35, 245–252. [Google Scholar]


{kind=link}
| Characteristic | Patients on Biologic | Patients on Mesalazine | p Value | Overall IBD Patients | Control Group |
|---|---|---|---|---|---|
| Number of patients, n | 311 | 75 | 386 | 2209 | |
| Male (%) | 177 (56.9%) | 34 (45.3%) | 0.071 | 211 (54.7%) | 832 (37.7%) |
| Mean age, years ± SD | 45.4 ± 15.5 | 46.2 ± 14.2 | 0.652 | 45.8 ± 14.9 | 43.7 ± 12.5 |
| Mean BMI, ± SD | 24.8 ± 4.55 | 24.0 ± 4.48 | 0.143 | ||
| Residence: | 0.911 | ||||
| Veneto, n (%) | 259 (83.3%) | 62 (82.7%) | |||
| other regions, n (%) | 52 (16.7%) | 13 (17.3%) | |||
| Smoking habit: | 0.781 | ||||
| non smokers, n (%) | 236 (75.9%) | 59 (78.7%) | |||
| ex smokers, n (%) | 37 (11.9%) | 9 (12%) | |||
| current smokers, n (%) | 38 (12.2%) | 7 (9.3%) | |||
| Comorbities: | 0.248 | ||||
| no, n (%) | 154 (49.5%) | 43 (57.3%) | |||
| yes, n (%) | 157 (50.5%) | 32 (42.7%) | |||
| Disease: | 0.397 | ||||
| UC, n (%) | 139 (44.7%) | 40 (53.3%) | |||
| CD, n (%) | 166 (53.4%) | 34 (45.3%) | |||
| IBD-U, n (%) | 6 (1.9%) | 1 (1.3%) | |||
| Disease activity: | 0.500 | ||||
| quiescent, n (%) | 216 (69.5%) | 50 (66.7%) | |||
| mild, n (%) | 72 (23.2%) | 17 (22,7%) | |||
| moderate, n (%) | 22 (7.1%) | 7 (9.3%) | |||
| severe, n (%) | 1 (0.3%) | 1 (1.3%) | |||
| UC extension: | 0.001 | ||||
| E1, n (%) | 11 (7.9%) | 13 (32.5%) | |||
| E2, n (%) | 75 (54%) | 18 (45%) | |||
| E3, n (%) | 53 (38.1%) | 9 (22.5%) | |||
| CD location: | 0.223 | ||||
| L1, n (%) | 67 (40.4%) | 19 (55.9%) | |||
| L2, n (%) | 32 (19.3%) | 6 (17.6%) | |||
| L3, n (%) | 66 (39.8%) | 9 (26.5%) | |||
| L4 (upper), n (%) | 9 (5.4%) | 0 (0%) | |||
| CD phenotype: | 0.009 | ||||
| B1, n (%) | 108 (65.0%) | 29 (85.3%) | |||
| B2, n (%) | 35 (21.1%) | 4 (11.7%) | |||
| B3, n (%) | 22 (13.3%) | 0 (0%) | |||
| perianal disease, n (%) | 24 (14.5%) | 1 (3%) | |||
| Biological therapy: | 0.001 | ||||
| IFX, n (%) | 95 (30.5%) | 0 (0%) | |||
| ADA, n (%) | 42 (13.5%) | 0 (0%) | |||
| GOL, n (%) | 4 (1.3%) | 0 (0%) | |||
| VDZ, n (%) | 99 (31.8%) | 0 (0%) | |||
| UST, n (%) | 57(18.3%) | 0 (0%) | |||
| Others (experimental), n (%) | 14 (4.5%) | 0 (0%) | |||
| Biological standard maintenance treatment, n (%) | 239 (62%) | 0 (0%) | |||
| Biological optimized maintenance treament, n (%) | 93 (24.1%) | 0 (0%) | |||
| Concomitant corticosteroid, n (%) | 43 (13.8%) | 26 (34.7%) | 0.001 |
| Characteristic | Patients on Biologic | Patients on Mesalazine | p Value |
|---|---|---|---|
| Number of patients, n (%) | 311 | 75 | |
| COVID-19 related symptoms: | 0.561 | ||
| none, n (%) | 228 (73.3%) | 51 (68.0%) | |
| <3 simptoms, n (%) | 60 (19.3%) | 18 (24.0%) | |
| 3–5 symptoms, n (%) | 21 (6.8%) | 5 (6.7%) | |
| >5 symptoms, n (%) | 2 (0.6%) | 1 (1.3%) | |
| Rapid antigenic tests: | 0.001 | ||
| positive, n (%) | 7 (2.3%) | 2 (2.7%) | |
| negative, n (%) | 218 (70.1%) | 7 (9.3%) | |
| Rt-PCR nasopharingeal swabs: | 0.556 | ||
| positive, n (%) | 14 (4.5%) | 5 (6.7%) | |
| negative, n (%) | 30 (9.6%) | 5 (6.7%) | |
| PPE: | 0.495 | ||
| surgical mask, n (%) | 162 (52.1%) | 43 (57.3%) | |
| FFP2 mask, n (%) | 126 (40.5%) | 25 (33.3%) | |
| fabric mask, n (%) | 21 (6.8%) | 6 (8.0%) | |
| gloves, n (%) | 21 (6.8%) | 7 (9.3%) | 0.458 |
| COVID-19 positive close contact, n (%) | 60 (19.3%) | 18 (24.0%) | 0.423 |
| Daily contacts: | 0.257 | ||
| only cohabitants, n (%): | 124 (39.9%) | 32 (42.7%) | |
| <10 individuals, n (%) | 106 (34.1%) | 18 (24%) | |
| >10 individuals, n (%) | 43 (13.8%) | 11 (14.7%) | |
| Flu vaccine taken, n (%) | 113 (36.3%) | 26 (34.7%) | 0.787 |
| Variable | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Age ( ≥46 vs. <46) | 1.388 (0.719–2.679) | 0.328 | ||
| Gender | 0.879 (0.454–1.704) | 0.704 | ||
| BMI (≥30 vs. <30) | 1.826 (0.753–4.428) | 0.182 | ||
| Smoking habit | 0.370 (0.086–1.592) | 0.182 | ||
| Comorbidities | 1.047 (0.544–2.015) | 0.890 | ||
| Disease type | 0.589 (0.300–1.155) | 0.124 | ||
| Disease activity | 1.075 (0.534–2.165) | 0.839 | ||
| Anti-TNFs | 1.072 (0.436–2.634) | 0.880 | ||
| VDZ | 0.637 (0.220–1.843) | 0.406 | ||
| UST | 0.805 (0.248–2.606) | 0.718 | ||
| Experimental drug | 3.35 (0.849–13.208) | 0.085 | ||
| Concomitant corticosteroid | 0.480 (0.165–1.397) | 0.178 | ||
| COVID-19 positive close contact | 15.979 (7.495–34.065) | 0.001 | 20.011 (8.746–45.784) | 0.001 |
| No-FFP2 mask | 0.484 (0.229–1.023) | 0.047 | 0.417 (0.175-0.991) | 0.048 |
| Daily risk exposure (>10 individuals) | 0.866 (0.323–2.317) | 0.774 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Ruscio, M.; Lunardi, G.; Buonfrate, D.; Gobbi, F.; Bertoli, G.; Piccoli, D.; Conti, A.; Geccherle, A.; Variola, A. A Seroprevalence Study of Anti-SARS-CoV-2 Antibodies in Patients with Inflammatory Bowel Disease during the Second Wave of the COVID-19 Pandemic in Italy. Medicina 2021, 57, 1048. https://doi.org/10.3390/medicina57101048
Di Ruscio M, Lunardi G, Buonfrate D, Gobbi F, Bertoli G, Piccoli D, Conti A, Geccherle A, Variola A. A Seroprevalence Study of Anti-SARS-CoV-2 Antibodies in Patients with Inflammatory Bowel Disease during the Second Wave of the COVID-19 Pandemic in Italy. Medicina. 2021; 57(10):1048. https://doi.org/10.3390/medicina57101048
Chicago/Turabian StyleDi Ruscio, Mirko, Gianluigi Lunardi, Dora Buonfrate, Federico Gobbi, Giulia Bertoli, Donatella Piccoli, Antonio Conti, Andrea Geccherle, and Angela Variola. 2021. "A Seroprevalence Study of Anti-SARS-CoV-2 Antibodies in Patients with Inflammatory Bowel Disease during the Second Wave of the COVID-19 Pandemic in Italy" Medicina 57, no. 10: 1048. https://doi.org/10.3390/medicina57101048
APA StyleDi Ruscio, M., Lunardi, G., Buonfrate, D., Gobbi, F., Bertoli, G., Piccoli, D., Conti, A., Geccherle, A., & Variola, A. (2021). A Seroprevalence Study of Anti-SARS-CoV-2 Antibodies in Patients with Inflammatory Bowel Disease during the Second Wave of the COVID-19 Pandemic in Italy. Medicina, 57(10), 1048. https://doi.org/10.3390/medicina57101048