The Impact of Novel Anticoagulants on the Upper Gastrointestinal Tract Mucosa


Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jairath, V.; Desborough, M.J. Modern-day management of upper gastrointestinal haemorrhage. Transfus. Med. 2015, 25, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Raval, J.; Cigarroa, J.E.; Chung, M.K.; Diaz-Sandoval, L.J.; Diercks, D.; Jung, H.S.; Washam, J.B.; Welch, B.G.; Zazulia, A.R.; Collins, S.P. Management of patients on non-vitamin K antagonist oral anticoagulants in acute care and periprocedural setting. Circulation 2017, 135, 604–633. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, K.; Yamamoto, T.; Aoyagi, H.; Isono, A.; Abe, K.; Kodashima, S.; Kita, H.; Watari, Y.; Kozuma, K. Difference between the Upper and the Lower Gastrointestinal Bleeding in Patients Taking Nonvitamin K Oral Anticoagulants. BioMed Res. Int. 2018, 2018, 1–5. [Google Scholar] [CrossRef]
- Majeed, A.; Hwang, H.-G.; Connolly, S.J.; Eikelboom, J.W.; Ezekowitz, M.D.; Wallentin, L.; Brueckmann, M.; Fraessdorf, M.; Yusuf, S.; Schulman, S. Management and Outcomes of Major Bleeding During Treatment With Dabigatran or Warfarin. Circulation 2013, 128, 2325–2332. [Google Scholar] [CrossRef]
- Caldeira, D.; Barra, M.; Ferreira, A.; Rocha, A.; Augusto, A.; Pinto, F.J.; Costa, J.; Ferreira, J.J. Systematic review with meta-analysis: The risk of major gastrointestinal bleeding with non-vitamin K antagonist oral anticoagulants. Aliment. Pharmacol. Ther. 2015, 42, 1239–1249. [Google Scholar] [CrossRef] [PubMed]
- Komen, J.J.; Forslund, T.; Mantel-Teeurwisse, A.K.; Klungel, O.H.; Euler, M.; Braunschweig, F.; Wallén, H.; Hjemdahl, P. Association of preceding antithrombotic therapy in atrial fibrillation patients with ischaemic stroke, intracranial haemorrhage, or gastrointestinal bleed and mortality. Eur. Heart J. 2019, 10, pvz063. [Google Scholar]
- Lee, J.Y. Risk Factors of Gastrointestinal Bleeding in Patients Receiving New Oral Anticoagulants. Korean J. Helicobacter Up Gastrointest. Res. 2018, 18, 219–224. [Google Scholar] [CrossRef]
- Rohla, M.; Weiss, T.W.; Pecen, L.; Patti, G.; Siller-Matula, J.M.; Schnabel, R.B.; Schilling, R.; Kotecha, D.; Lucerna, M.; Huber, K.; et al. Risk factors for thromboembolic and bleeding events in anticoagulated patients with atrial fibrillation: The prospective, multicentre observational PREvention oF thromboembolic events—European Registry in Atrial Fibrillation (PREFER in AF). BMJ Open 2019, 9, e022478. [Google Scholar] [CrossRef]
- Holster, I.L.; Valkhoff, V.E.; Kuipers, E.J.; Tjwa, E.T. New oral anticoagulants increase risk for gastrointestinal bleeding: A systematic review and meta-analysis. Gastroenterology 2013, 145, 105–112. [Google Scholar] [CrossRef]
- Cheung, K.S.; Leung, W.K. Gastrointestinal bleeding in patients on novel oral anticoagulants: Risk, prevention and management. World J. Gastroenterol. 2017, 23, 1954–1963. [Google Scholar] [CrossRef]
- Camm, A.J.; Lip, G.Y.; De Caterina, R.; Savelieva, I.; Atar, D.; Hohnloser, S.H.; Hindricks, G.; Bax, J.J.; Baumgartner, H.; Ceconi, C.; et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation. Eur. Heart J. 2012, 33, 2719–2747. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castellá, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the Management of Atrial Fibrillation Developed in Collaboration With EACTS. Rev. Esp. Cardiol. 2017, 70, 50. [Google Scholar] [CrossRef] [PubMed]
- Stiles, S. Risk-score insights on how DOACs vary in upper GI bleeding risk. JAMA 2018, 320, 2221–2230. [Google Scholar]
- Larsen, T.B.; Skjøth, F.; Nielsen, P.B.; Kjældgaard, J.N.; Lip, G.Y.H. Comparative effectiveness and safety of non-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation: Propensity weighted nationwide cohort study. BMJ 2016, 353, 3189. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.S.; Dorreen, A.; Martel, M.; Huynh, T.; Barkun, A.N. Risk of Gastrointestinal Bleeding in Patients Taking Non–Vitamin K Antagonist Oral Anticoagulants: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2017, 15, 1674–1683. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.-Q.; Chen, X.-H.; Tian, X.-Y.; Li, L. Differences In Gastrointestinal Safety Profiles Among Novel Oral Anticoagulants: Evidence From A Network Meta-Analysis. Clin. Epidemiol. 2019, 11, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Young, J.K.; Seonji, K.; Kypunghoon, P.; Bo, R.Y.; Joongyub, L.; Mi-Sook, K.; Byung, J.P. Comparison of bleeding risk among non-vitamin K antagonist oral anticoagulants using the Korea adverse event reporting system database. Ther. Adv. Drug Saf. 2019, 10, 1–11. [Google Scholar]
- Aabakken, L.; Rembacken, B.; Lemoine, O.; Kuznetsov, K.; Rey, J.-F.; Rösch, T.; Eisen, G.; Cotton, P.; Fujino, M. Minimal standard terminology for gastrointestinal endoscopy—MST 3.0. Endoscopy 2009, 41, 727–728. [Google Scholar] [CrossRef]
- Ruff, C.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef]
- Cangemi, D.J.; Krill, T.; Weideman, R.; Cipher, D.J.; Spechler, S.J.; Feagins, L.A. A Comparison of the Rate of Gastrointestinal Bleeding in Patients Taking Non-Vitamin K Antagonist Oral Anticoagulants or Warfarin. Am. J. Gastroenterol. 2017, 112, 734–739. [Google Scholar] [CrossRef]
- Xue, Z.; Zhang, H. Non-Vitamin K Antagonist Oral Anticoagulants Versus Warfarin in Asians With Atrial Fibrillation. Stroke 2019, 50, 2819–2828. [Google Scholar] [CrossRef]
- Abraham, N.S.; Noseworthy, P.A.; Yao, X.; Sangaralingham, L.R.; Shah, N.D. Gastrointestinal Safety of Direct Oral Anticoagulants: A Large Population-Based Study. Gastroenterology 2017, 152, 1014–1022. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.W.; Lau, W.C.Y.; Leung, W.K.; Mok, M.; He, Y.; Tong, T.S.; Wong, I.C. Prevention of Dabigatran-Related Gastrointestinal Bleeding With Gastroprotective Agents: A Population-Based Study. Gastroenterology 2015, 149, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Bolek, T.; Samoš, M.; Škorňová, I.; Galajda, P.; Staško, J.; Kubisz, P.; Mokáň, M. Proton Pump Inhibitors and Dabigatran Therapy: Impact on Gastric Bleeding and Dabigatran Plasma Levels. Semin. Thromb. Hemost. 2019, 45, 846–850. [Google Scholar] [CrossRef]
- Desai, J.; Kob, J.M.; Weitz, J.I.; Aisenberg, J. Gastrointestinal bleeding with new oral anticoagulants—Ddefining the issues and the management strategies. Thromb. Haemost. 2013, 110, 205–222. [Google Scholar] [CrossRef] [PubMed]
- Veitch, A.M.; Vanbiervliet, G.; Gershlick, A.H.; Boustiere, C.H.; Baglin, T.P.; Smith, L.A.; Radaelli, F.; Knight, E.; Gralnek, L.M.; Hassan, C.; et al. Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guidelines. Endoscopy 2016, 48, 1–18. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Sex | UV | HP | NSAID-SA | PPI | DM | MI | NYHA | AH | TIA, Stroke, PAE | PAO | CHA2DS2-VASC | HAS-BLED | Indication | Bleeding into GIT/all | Biopsy | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
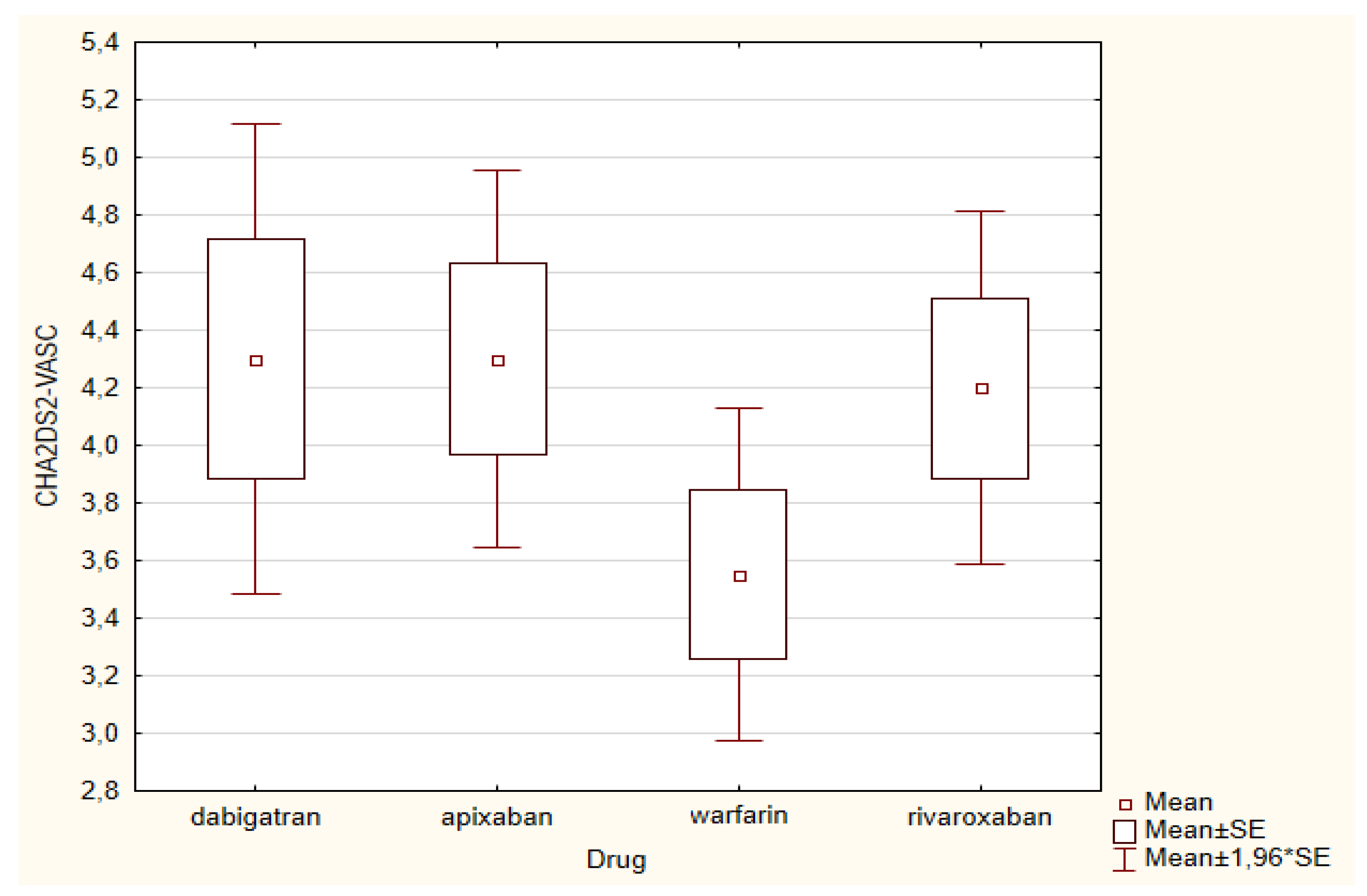
| Warfarin | 72.4 (60–86) | F 9/M 11 | 6 | 2/15 | 0 | GERD 5/UV 2 | 3 | 3 | 2.1 ± 0.31 | 20 | 4 | 3 | 3.55 ± 1.32 | 2.05 ± 0.60 | DVT 4 /FA 16 | 4 GIT/6 all | 12 |
| Dabigatran | 73.15 (60–89) | F 7/M 13 | 7 | 2/15 | 0 | GERD 2/UV 3 | 6 | 3 | 2.2 ± 0.41 | 20 | 7 | 1 | 4.30 ± 1.87 | 2.7 ± 0.98 | DVT 4 /FA 16 | 4 GIT/4 all | 13 |
| Rixaroxaban | 77.25 (67–93) | F 15/M 5 | 10 | 2/17 | 2 | GERD 8/UV 6 | 2 | 4 | 2.15 ± 0.37 | 20 | 5 | 0 | 4.20 ± 1.39 | 2.45 ± 0.51 | DVT 4 /FA 16 | 2 GIT/4 all | 12 |
| Apixaban | 76.35 (66–88) | F 11/M9 | 3 | 3/15 | 0 | GERD 6/UV 3 | 10 | 3 | 2.1 ± 0.31 | 20 | 5 | 4 | 4.30 ± 1.49 | 2.25 ± 0.72 | DVT 0 /20 FA | 1 GIT/3 all | 16 |
| Warfarin | Dabigatran | Rivaroxaban | Apixaban | |
|---|---|---|---|---|
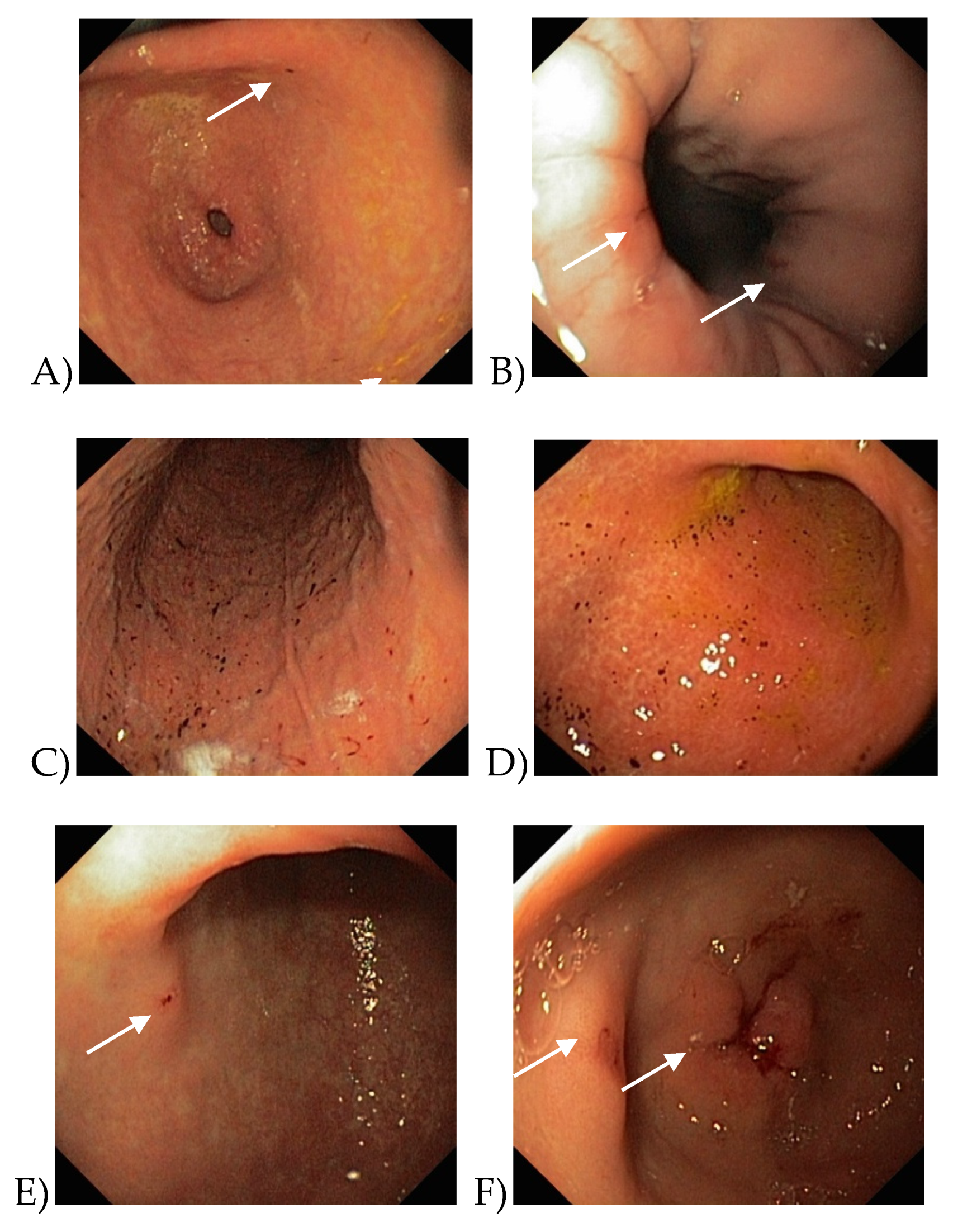
| Upper gastrointestinal Tract | Petechiae in stomach antrum, HP negative | Petechiae in stomach antrum, HP positive | Erosions in stomach antrum with bleeding signs, HP positive | Ulcus ventriculi, petechiae in stomach antrum, HP positive |
| Petechiae in stomach antrum, HP negative | Petechiae in stomach antrum, HP negative | Erosions in stomach antrum with bleeding signs, HP positive | ||
| Haemorrhagic gastropathy, HP positive | Cameron’s lesions with bleeding signs in hiatus hernia | |||
| Haemorrhagic gastropathy, HP negative | Erosions in stomach antrum with bleeding signs, HP positive | |||
| Location other than the upper gastrointestinal tract | Positive FOBT–EGD and colonoscopy negative | Epistaxis | Enterorrhagia from haemorrhoids | |
| Positive FOBT–EGD and colonoscopy negative | Positive FOBT–EGD and colonoscopy negative | Ppositive FOBT–EGD and colonoscopy negative |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihalkanin, L.; Stancak, B. The Impact of Novel Anticoagulants on the Upper Gastrointestinal Tract Mucosa. Medicina 2020, 56, 363. https://doi.org/10.3390/medicina56070363
Mihalkanin L, Stancak B. The Impact of Novel Anticoagulants on the Upper Gastrointestinal Tract Mucosa. Medicina. 2020; 56(7):363. https://doi.org/10.3390/medicina56070363
Chicago/Turabian StyleMihalkanin, Lubomir, and Branislav Stancak. 2020. "The Impact of Novel Anticoagulants on the Upper Gastrointestinal Tract Mucosa" Medicina 56, no. 7: 363. https://doi.org/10.3390/medicina56070363
APA StyleMihalkanin, L., & Stancak, B. (2020). The Impact of Novel Anticoagulants on the Upper Gastrointestinal Tract Mucosa. Medicina, 56(7), 363. https://doi.org/10.3390/medicina56070363