Prevalence of Adverse Reactions to Glutenand People Going on a Gluten-Free Diet:A Survey Study Conducted in Brazil

 ,
,  , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Survey Tool and Data Collection
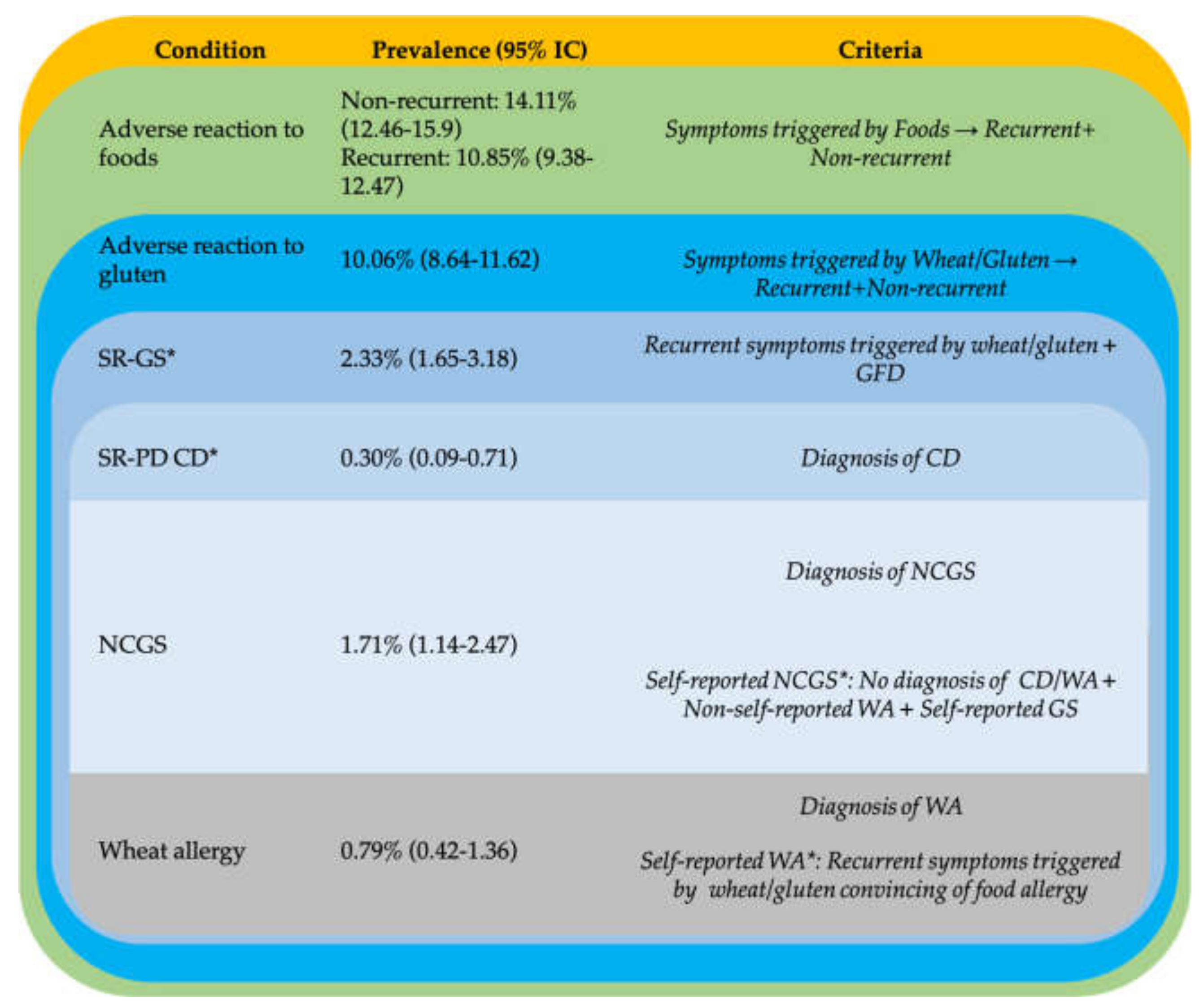
2.2. Criteria Used to Classify Adverse Reactions to Gluten and GRDs
2.3. Ethical and Statistical Aspects
3. Results
3.1. Participation and Interviewees’ Characteristics
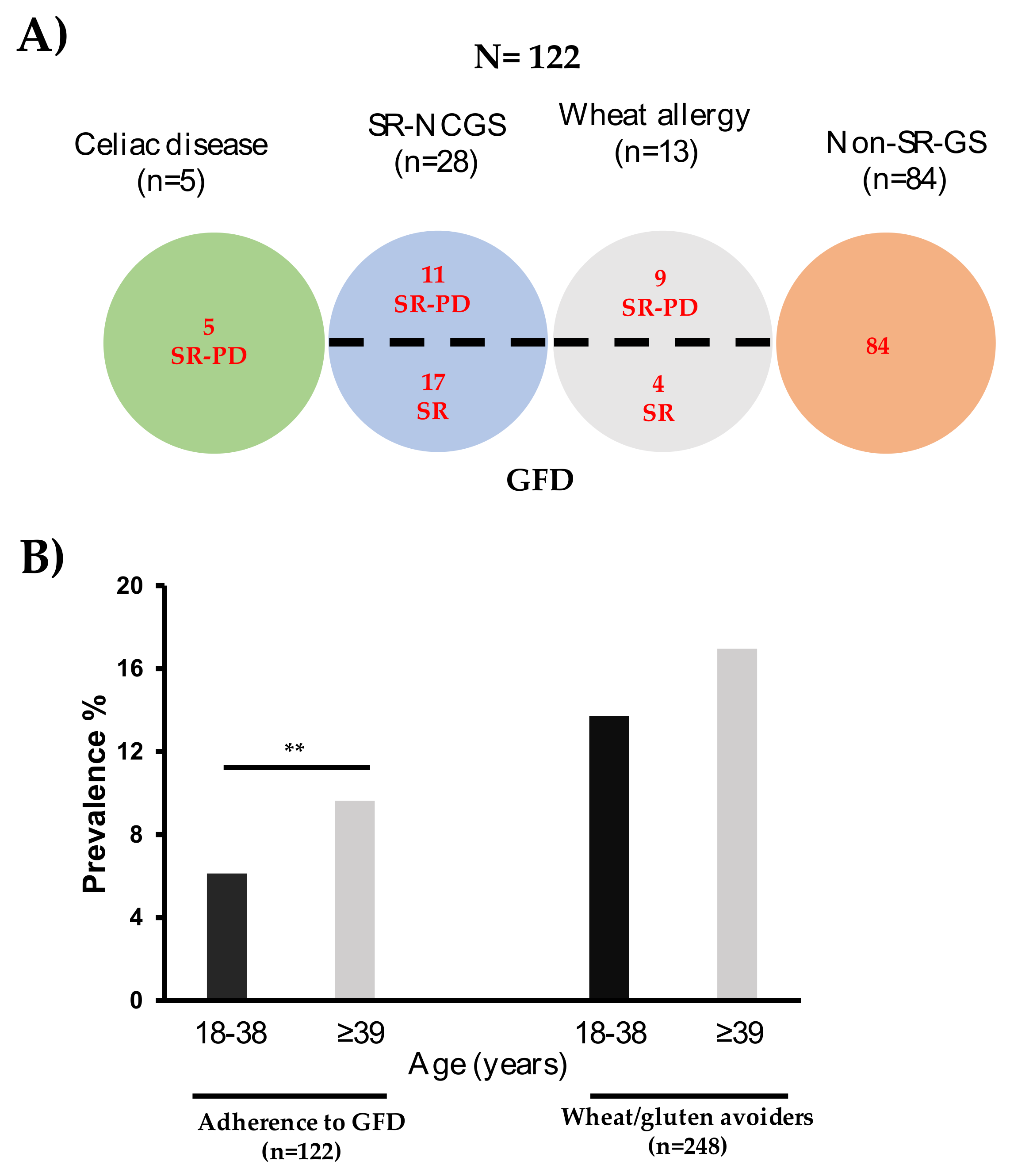
3.2. Proportions Estimations
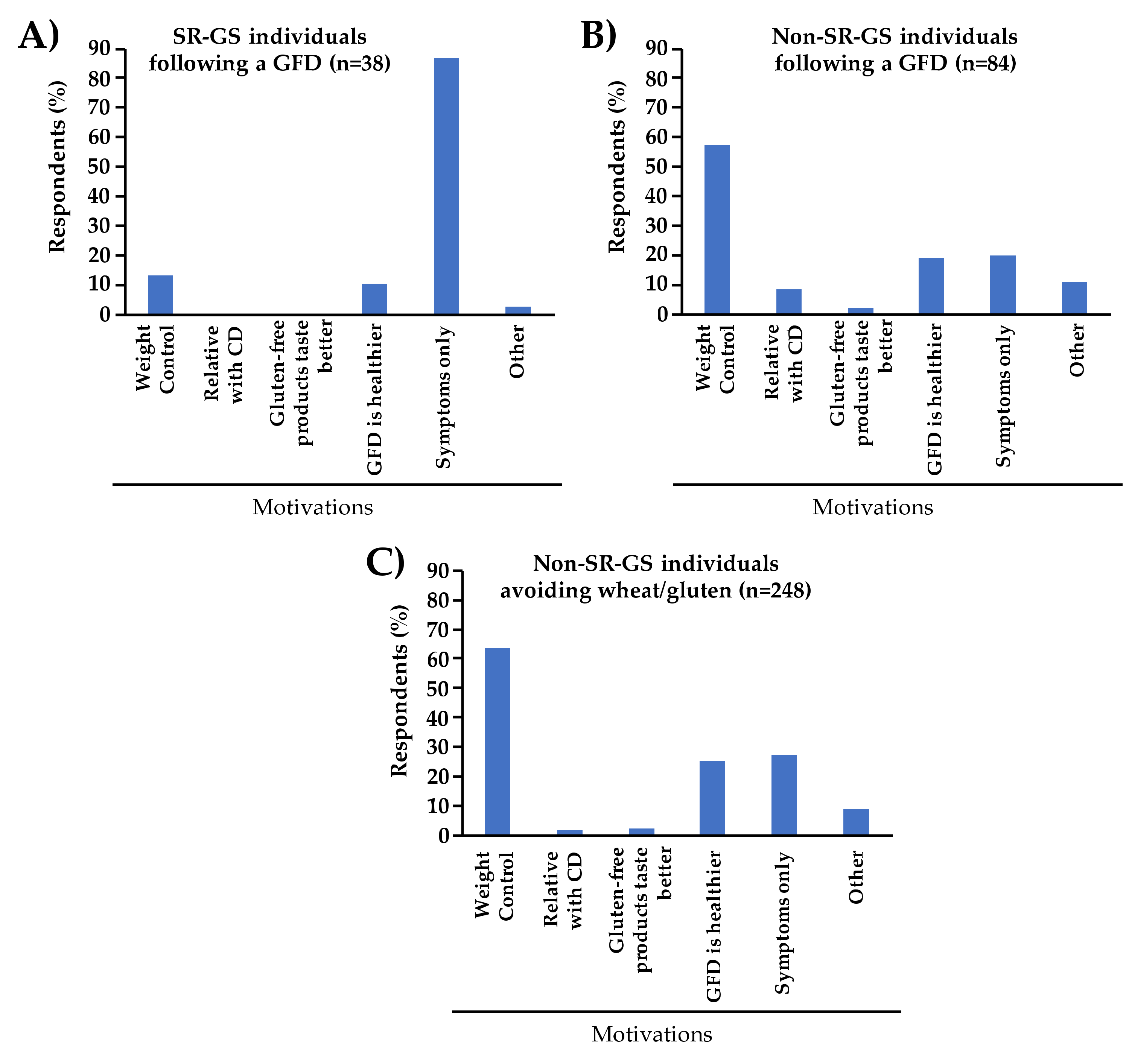
3.3. Reasons for Adhering to a GFD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ontiveros, N.; Flores-Mendoza, L.; Canizalez-Román, V.; Cabrera-Chavez, F. Food allergy: Prevalence and food technology approaches for the control of IgE-mediated food allergy. Austin J. Nutr. Food Sci. 2014, 2, 1029. [Google Scholar]
- Catassi, C.; Alaedini, A.; Bojarski, C.; Bonaz, B.; Bouma, G.; Carroccio, A.; Castillejo, G.; De Magistris, L.; Dieterich, W.; Di Liberto, D. The overlapping area of non-celiac gluten sensitivity (NCGS) and wheat-sensitive irritable bowel syndrome (IBS): An update. Nutrients 2017, 9, 1268. [Google Scholar] [CrossRef] [PubMed]
- Rej, A.; Sanders, D.S. The overlap of irritable bowel syndrome and noncoeliac gluten sensitivity. Curr. Opin. Gastroenterol. 2019, 35, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, M.R.; Cremon, C.; Stanghellini, V.; Barbara, G. Recent advances in understanding non-celiac gluten sensitivity. F1000Research 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Elli, L.; Bonaz, B.; Bouma, G.; Carroccio, A.; Castillejo, G.; Cellier, C.; Cristofori, F.; De Magistris, L.; Dolinsek, J. Diagnosis of non-celiac gluten sensitivity (NCGS): The Salerno experts’ criteria. Nutrients 2015, 7, 4966–4977. [Google Scholar] [CrossRef] [PubMed]
- Figueroa-Salcido, O.G.; Ontiveros, N.; Cabrera-Chavez, F. Gluten vehicle and placebo for non-celiac gluten sensitivity assessment. Medicina 2019, 55, 117. [Google Scholar] [CrossRef]
- Cabrera-Chávez, F.; Salcido-Figueroa, O.G.; Noé, O. The indistinguishable gluten vehicle and placebo in the diagnosis of NCGS. Am. J. Gastroenterol. 2018, 113, 1559–1560. [Google Scholar]
- Pietzak, M.; Kerner Jr, J.A. Celiac disease, wheat allergy, and gluten sensitivity: When gluten free is not a fad. J. Parenter. Enter. Nutr. 2012, 36, 68–75. [Google Scholar] [CrossRef]
- Cabrera-Chávez, F.; Dezar, G.V.; Islas-Zamorano, A.P.; Espinoza-Alderete, J.G.; Vergara-Jiménez, M.J.; Magaña-Ordorica, D.; Ontiveros, N. Prevalence of self-reported gluten sensitivity and adherence to a gluten-free diet in argentinian adult population. Nutrients 2017, 9, 81. [Google Scholar] [CrossRef]
- Ontiveros, N.; Rodríguez-Bellegarrigue, C.I.; Galicia-Rodríguez, G.; Vergara-Jiménez, M.D.J.; Zepeda-Gómez, E.M.; Arámburo-Galvez, J.G.; Gracia-Valenzuela, M.H.; Cabrera-Chávez, F. Prevalence of self-reported gluten-related disorders and adherence to a gluten-free diet in Salvadoran adult population. Int. J. Environ. Res. Public Health 2018, 15, 786. [Google Scholar] [CrossRef]
- Wünsche, J.; Lambert, C.; Gola, U.; Biesalski, H.K. Consumption of gluten free products increases heavy metal intake. NFS J. 2018, 12, 11–15. [Google Scholar] [CrossRef]
- Cartee, A.; Murray, J.A. The gluten-free diet: An historical perspective and its use by people without coeliac disease. Med J. Aust. 2020, 212, 111–112. [Google Scholar] [CrossRef] [PubMed]
- Ontiveros, N.; López-Gallardo, J.A.; Vergara-Jiménez, M.J.; Cabrera-Chávez, F. Self-reported prevalence of symptomatic adverse reactions to gluten and adherence to gluten-free diet in an adult Mexican population. Nutrients 2015, 7, 6000–6015. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Chávez, F.; Granda-Restrepo, D.M.; Arámburo-Gálvez, J.G.; Franco-Aguilar, A.; Magaña-Ordorica, D.; Vergara-Jiménez, M.d.J.; Ontiveros, N. Self-reported prevalence of gluten-related disorders and adherence to gluten-free diet in Colombian adult population. Gastroenterol. Res. Pract. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Arámburo-Gálvez, J.G.; Carvalho Gomes, I.; André, T.G.; Beltrán-Cárdenas, C.E.; Macêdo-Callou, M.A.; Braga Rocha, É.M.; Mye-Takamatu-Watanabe, E.A.; Rahmeier-Fietz, V.; Figueroa-Salcido, O.G.; Cárdenas-Torres, F.I. Translation, cultural adaptation, and evaluation of a brazilian portuguese questionnaire to estimate the self-reported prevalence of gluten-related disorders and adherence to gluten-free diet. Medicina 2019, 55, 593. [Google Scholar] [CrossRef] [PubMed]
- DiGiacomo, D.V.; Tennyson, C.A.; Green, P.H.; Demmer, R.T. Prevalence of gluten-free diet adherence among individuals without celiac disease in the USA: Results from the Continuous National Health and Nutrition Examination Survey 2009–2010. Scand. J. Gastroenterol. 2013, 48, 921–925. [Google Scholar] [CrossRef] [PubMed]
- Carroccio, A.; Giambalvo, O.; Blasca, F.L.; Iacobucci, R.; D’Alcamo, A.; Mansueto, P. Self-reported non-celiac wheat sensitivity in high school students: Demographic and clinical characteristics. Nutrients 2017, 9, 771. [Google Scholar] [CrossRef]
- Aziz, I.; Lewis, N.R.; Hadjivassiliou, M.; Winfield, S.N.; Rugg, N.; Kelsall, A.; Newrick, L.; Sanders, D.S. A UK study assessing the population prevalence of self-reported gluten sensitivity and referral characteristics to secondary care. Eur. J. Gastroenterol. Hepatol. 2014, 26, 33–39. [Google Scholar] [CrossRef]
- Van Gils, T.; Nijeboer, P.; IJssennagger, C.E.; Sanders, D.S.; Mulder, C.J.; Bouma, G. Prevalence and characterization of self-reported gluten sensitivity in The Netherlands. Nutrients 2016, 8, 714. [Google Scholar] [CrossRef]
- Volta, U.; Bardella, M.T.; Calabrò, A.; Troncone, R.; Corazza, G.R. An Italian prospective multicenter survey on patients suspected of having non-celiac gluten sensitivity. BMC Med. 2014, 12, 85. [Google Scholar] [CrossRef]
- Potter, M.D.; Walker, M.M.; Jones, M.P.; Koloski, N.A.; Keely, S.; Talley, N.J. Wheat intolerance and chronic gastrointestinal symptoms in an Australian population-based study: Association between wheat sensitivity, celiac disease and functional gastrointestinal disorders. Am. J. Gastroenterol. 2018, 113, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- Abadie, V.; Sollid, L.M.; Barreiro, L.B.; Jabri, B. Integration of genetic and immunological insights into a model of celiac disease pathogenesis. Annu. Rev. Immunol. 2011, 29, 493–525. [Google Scholar] [CrossRef] [PubMed]
- Brazil: Grain and Feed Update. United States Department of Agriculture. 2019. Available online: https://www.fas.usda.gov/data/brazil-grain-and-feed-update-12 (accessed on 17 February 2020).
- Mexico: Grain and Feed Update. United States Department of Agriculture. 2019. Available online: https://www.fas.usda.gov/data/mexico-grain-and-feed-update-12 (accessed on 17 February 2020).
- Colombia: Grain and Feed Update. United States Department of Agriculture. 2018. Available online: https://www.fas.usda.gov/data/colombia-grain-and-feed-update (accessed on 17 February 2020).
- El Salvador: Exporter Guide. United States Department of Agriculture. 2018. Available online: https://www.fas.usda.gov/data/el-salvador-exporter-guide-2 (accessed on 17 February 2020).
- Gadelha de Mattos, Y.A.; Puppin Zandonadi, R.; Gandolfi, L.; Pratesi, R.; Yoshio Nakano, E.; Pratesi, C.B. Self-reported non-celiac gluten sensitivity in Brazil: Translation, cultural adaptation, and validation of Italian questionnaire. Nutrients 2019, 11, 781. [Google Scholar] [CrossRef] [PubMed]
- Melo, S.B.C.; Fernandes, M.I.M.; Peres, L.C.; Troncon, L.E.A.; Galvão, L.C. Prevalence and demographic characteristics of celiac disease among blood donors in Ribeirão Preto, State of São Paulo, Brazil. Dig. Dis. Sci. 2006, 51, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, L.; Guimarães, T.; Silva, R.; Cheik, M.; de Ramos Nápolis, A.; E Silva, G.B.; Segundo, G. Prevalence of food allergy in infants and pre-schoolers in Brazil. Allergol. Immunopathol. 2016, 44, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Machado, J.; Gandolfi, L.; Coutinho De Almeida, F.; Malta Almeida, L.; Puppin Zandonadi, R.; Pratesi, R. Gluten-free dietary compliance in Brazilian celiac patients: Questionnaire versus serological test. Nutr. Clín. Diet. Hosp. 2013, 33, 46–49. [Google Scholar]
- Kotze, L. Gynecologic and obstetric findings related to nutritional status and adherence to a gluten-free diet in Brazilian patients with celiac disease. J. Clin. Gastroenterol. 2004, 38, 567–574. [Google Scholar] [CrossRef]
- do Nascimento, A.B.; Fiates, G.M.R.; dos Anjos, A.; Teixeira, E. Gluten-free is not enough–perception and suggestions of celiac consumers. Int. J. Food Sci. Nutr. 2014, 65, 394–398. [Google Scholar] [CrossRef]
- Arias-Gastelum, M.; Cabrera-Chávez, F.; de Jesús Vergara-Jiménez, M.; Ontiveros, N. The gluten-free diet: Access and economic aspects and impact on lifestyle. Nutr. Diet. Suppl. 2018, 10, 27. [Google Scholar] [CrossRef]
- Dana, Z.Y.; Vered, R.; Haim, S.; Efrat, B. Factors associated with non adherence to a gluten free diet in adult with celiac disease: A survey assessed by BIAGI score. Clin. Research Hepatol. Gastroenterol. 2020. [Google Scholar] [CrossRef]
- Pember, S.E.; Rush, S.E. Motivation for gluten-free diet adherence among adults with and without a clinically diagnosed gluten-related illness. Calif. J. Health Promot. 2016, 14, 68–73. [Google Scholar] [CrossRef]
- Golley, S.; Corsini, N.; Topping, D.; Morell, M.; Mohr, P. Motivations for avoiding wheat consumption in Australia: Results from a population survey. Public Health Nutr. 2015, 18, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.H.; Neal, B.; Trevena, H.; Crino, M.; Stuart-Smith, W.; Faulkner-Hogg, K.; Louie, J.C.Y.; Dunford, E. Are gluten-free foods healthier than non-gluten-free foods? An evaluation of supermarket products in Australia. Br. J. Nutr. 2015, 114, 448–454. [Google Scholar] [CrossRef] [PubMed]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arámburo-Gálvez, J.G.; Beltrán-Cárdenas, C.E.; Geralda André, T.; Carvalho Gomes, I.; Macêdo-Callou, M.A.; Braga-Rocha, É.M.; Mye-Takamatu-Watanabe, E.A.; Rahmeier-Fietz, V.; Figueroa-Salcido, O.G.; Vergara-Jiménez, M.d.J.; et al. Prevalence of Adverse Reactions to Glutenand People Going on a Gluten-Free Diet:A Survey Study Conducted in Brazil. Medicina 2020, 56, 163. https://doi.org/10.3390/medicina56040163
Arámburo-Gálvez JG, Beltrán-Cárdenas CE, Geralda André T, Carvalho Gomes I, Macêdo-Callou MA, Braga-Rocha ÉM, Mye-Takamatu-Watanabe EA, Rahmeier-Fietz V, Figueroa-Salcido OG, Vergara-Jiménez MdJ, et al. Prevalence of Adverse Reactions to Glutenand People Going on a Gluten-Free Diet:A Survey Study Conducted in Brazil. Medicina. 2020; 56(4):163. https://doi.org/10.3390/medicina56040163
Chicago/Turabian StyleArámburo-Gálvez, Jesús Gilberto, Carlos Eduardo Beltrán-Cárdenas, Tatiane Geralda André, Itallo Carvalho Gomes, María Auxiliadora Macêdo-Callou, Élida Mara Braga-Rocha, Elaine Aparecida Mye-Takamatu-Watanabe, Vivian Rahmeier-Fietz, Oscar Gerardo Figueroa-Salcido, Marcela de Jesus Vergara-Jiménez, and et al. 2020. "Prevalence of Adverse Reactions to Glutenand People Going on a Gluten-Free Diet:A Survey Study Conducted in Brazil" Medicina 56, no. 4: 163. https://doi.org/10.3390/medicina56040163
APA StyleArámburo-Gálvez, J. G., Beltrán-Cárdenas, C. E., Geralda André, T., Carvalho Gomes, I., Macêdo-Callou, M. A., Braga-Rocha, É. M., Mye-Takamatu-Watanabe, E. A., Rahmeier-Fietz, V., Figueroa-Salcido, O. G., Vergara-Jiménez, M. d. J., Flores-Mendoza, L. K., Ontiveros, N., & Cabrera-Chávez, F. (2020). Prevalence of Adverse Reactions to Glutenand People Going on a Gluten-Free Diet:A Survey Study Conducted in Brazil. Medicina, 56(4), 163. https://doi.org/10.3390/medicina56040163