Chemically Activated Cooling Vest’s Effect on Cooling Rate Following Exercise-Induced Hyperthermia: A Randomized Counter-Balanced Crossover Study

 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Selection of Participants
2.3. Interventions
2.4. Outcomes
2.5. Analysis
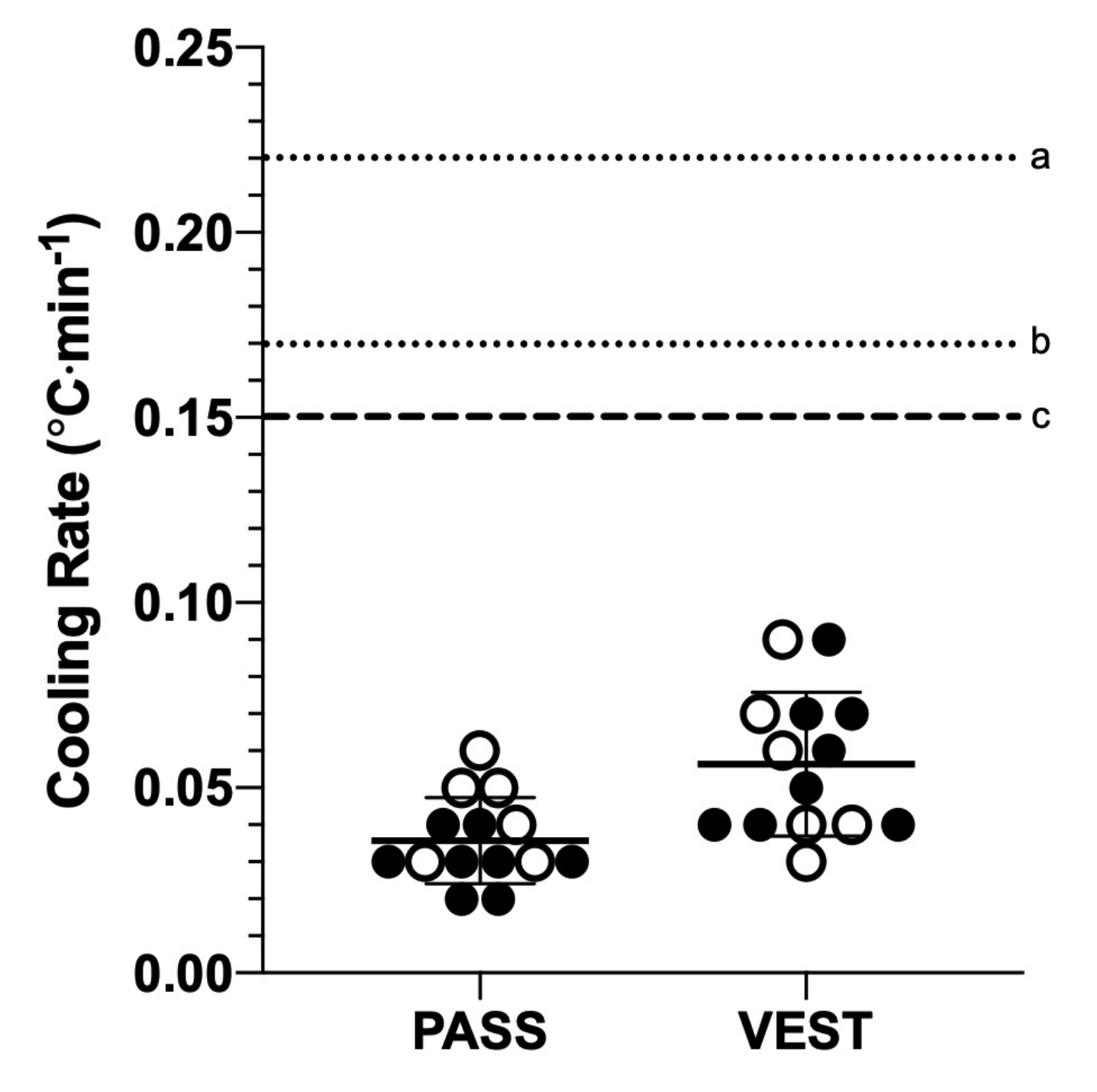
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Casa, D.J.; DeMartini, J.K.; Bergeron, M.F.; Csillan, D.; Eichner, E.R.; Lopez, R.M.; Ferrara, M.S.; Miller, K.C.; O’Connor, F.; Sawka, M.N.; et al. National Athletic Trainers’ Association Position Statement: Exertional Heat Illnesses. J. Athl. Train. 2015, 50, 986–1000. [Google Scholar] [CrossRef] [PubMed]
- Belval, L.N.; Casa, D.J.; Adams, W.M.; Chiampas, G.T.; Holschen, J.C.; Hosokawa, Y.; Jardine, J.; Kane, S.F.; LaBotz, M.; Lemieux, R.S.; et al. Consensus Statement-Prehospital Care of Exertional Heat Stroke. Prehospital Emerg. Care 2018, 22, 392–397. [Google Scholar] [CrossRef]
- McDermott, B.P.; Casa, D.J.; Ganio, M.S.; Lopez, R.M.; Yeargin, S.W.; Armstrong, L.E.; Maresh, C.M. Acute Whole-Body Cooling for Exercise-Induced Hyperthermia: A Systematic Review. J. Athl. Train. 2009, 44, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Poirier, M.P.; Notley, S.R.; Flouris, A.D.; Kenny, G.P. Physical characteristics cannot be used to predict cooling time using cold-water immersion as a treatment for exertional hyperthermia. Appl. Physiol. Nutr. Metab. 2018, 43, 857–860. [Google Scholar] [CrossRef]
- DeMartini, J.K.; Casa, D.J.; Stearns, R.; Belval, L.N.; Crago, A.; Davis, R.; Jardine, J. Effectiveness of Cold Water Immersion in the Treatment of Exertional Heat Stroke at the Falmouth Road Race. Med. Sci. Sports Exerc. 2015, 47, 240–245. [Google Scholar] [CrossRef]
- Adams, W.M.; Hosokawa, Y.; Casa, U.J. Body-Cooling Paradigm in Sport: Maximizing Safety and Performance During Competition. J. Sport Rehabil. 2016, 25, 382–394. [Google Scholar] [CrossRef] [PubMed]
- Douma, M.; Aves, T.; Allan, K.; Bendall, J.C.; Berry, D.C.; Chang, W.-T.; Epstein, J.; Hood, N.; Singletary, E.M.; Zideman, D.; et al. First aid cooling techniques for heat stroke and exertional hyperthermia: A systematic review and meta-analysis. Resuscitation 2020, 148, 173–190. [Google Scholar] [CrossRef]
- Gomm, E.; Grimaldi, R.; Galloway, R.; Sharma, S.; Simpson, W.; Cottingham, R. Successful out-of-hospital therapy for heatstroke in three marathon runners with a novel core body cooling device: CAERvest®. Scand. J. Med. Sci. Sports 2016, 26, 854–855. [Google Scholar] [CrossRef]
- Keen, M.L.; Miller, K.C. Should Cooling Vests be Used to Treat Exertional Heatstroke? A Critically-Appraised Topic. J. Sport Rehabil. 2015, 26, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Willmott, A.G.; Bliss, A.; Simpson, W.H.; Tocker, S.M.; Cottingham, R.; Maxwell, N.S. CAERvest®—A novel endothermic hypothermic device for core temperature cooling: Safety and efficacy testing. Int. J. Occup. Saf. Ergon. 2017, 24, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Cramer, M.N.; Jay, O. Biophysical aspects of human thermoregulation during heat stress. Auton. Neurosci. 2016, 196, 3–13. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, X.J.; Thompson, B.; Han, A. Methodological Recommendations for Menstrual Cycle Research in Sports and Exercise. Med. Sci. Sports Exerc. 2019, 51, 2610–2617. [Google Scholar] [CrossRef]
- Jackson, A.S.; Pollock, M.L. Generalized equations for predicting body density of men. Br. J. Nutr. 1978, 40, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.S.; Pollock, M.L.; Ward, A. Generalized equations for predicting body density of women. Med. Sci. Sports Exerc. 1980, 12, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.N.; Burke, L.M.; Eichner, E.R.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. American College of Sports Medicine position stand. Exercise and fluid replacement. Med. Sci. Sports Exerc. 2007, 39, 377–390. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Wuensch, K.L.; Evans, J.D. Straightforward Statistics for the Behavioral Sciences. J. Am. Stat. Assoc. 1996, 91, 1750. [Google Scholar] [CrossRef]
- Hosokawa, Y.; Adams, W.M.; Belval, L.N.; Vandermark, L.W.; Casa, D.J. Tarp-Assisted Cooling as a Method of Whole-Body Cooling in Hyperthermic Individuals. Ann. Emerg. Med. 2017, 69, 347–352. [Google Scholar] [CrossRef]
- Morrison, K.E.; Desai, N.; McGuigan, C.; Lennon, M.; Godek, S.F. Effects of Intravenous Cold Saline on Hyperthermic Athletes Representative of Large Football Players and Small Endurance Runners. Clin. J. Sport Med. 2018, 28, 493–499. [Google Scholar] [CrossRef]
- DeMartini, J.K.; Ranalli, G.F.; Casa, D.J.; Lopez, R.M.; Ganio, M.S.; Stearns, R.L.; McDermott, B.P.; Armstrong, L.E.; Maresh, C.M. Comparison of Body Cooling Methods on Physiological and Perceptual Measures of Mildly Hyperthermic Athletes. J. Strength Cond. Res. 2011, 25, 2065–2074. [Google Scholar] [CrossRef]
- Stearns, R.L.; Casa, D.J.; O’Connor, F.G.; Lopez, R.M. A Tale of Two Heat Strokes: A Comparative Case Study. Curr. Sports Med. Rep. 2016, 15, 94–97. [Google Scholar] [CrossRef]
- Yoshizawa, T.; Omori, K.; Takeuchi, I.; Miyoshi, Y.; Kido, H.; Takahashi, E.; Jitsuiki, K.; Ishikawa, K.; Ohsaka, H.; Sugita, M.; et al. Heat stroke with bimodal rhabdomyolysis: A case report and review of the literature. J. Intensiv. Care 2016, 4, 71. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.S.; Rodeia, S.C.; Silvestre, J.; Póvoa, P. Exertional heat stroke and acute liver failure: A late dysfunction. BMJ Case Rep. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Hadad, E.; Ben-Ari, Z.; Heled, Y.; Moran, D.S.; Shani, Y.; Epstein, Y. Liver transplantation in exertional heat stroke: A medical dilemma. Intensive Care Med. 2004, 30, 1474–1478. [Google Scholar] [CrossRef] [PubMed]
- Gatwick Airport, United Kingdom Weather History|Weather Underground n.d. Available online: https://www.wunderground.com/history/daily/gb/gatwick-airport/EGKK/date/2015-4-11 (accessed on 19 March 2020).
- London, United Kingdom Weather History|Weather Underground. Available online: https://www.wunderground.com/history/daily/gb/london/EGLC/date/2015-4-25 (accessed on 19 March 2020).



{kind=link}
{kind=link}
| Patient | Mechanism of Injury | Cooling Modality | Outcome | |
|---|---|---|---|---|
| Type | Location | |||
| Patient 1 | Collapsed at the finish line of the 2015 Brighton Marathon | Ice packs | Groin | Discharged home the same day |
| CAERvest® | Torso | |||
| Cooled intravenous solution | Intravenous infusion | |||
| Patent 2 | Collapsed at the 2015 London Marathon | Ice packs | Unspecified | Discharged home the same day |
| CAERvest® | Torso | |||
| Patient 3 | Collapsed at the finish line of the 2015 London Marathon | CAERvest® | Torso | Rhabdomyolysis, intestinal ischemia, and bilateral compartment syndrome |
| Cooling Modality | Sex | ||
|---|---|---|---|
| Male | Female | ||
| Post-exercise TRE (°C) | PASS | 39.73 ± 0.41 | 39.49 ± 0.39 |
| VEST | 39.76 ± 0.27 | 39.29 ± 0.30 | |
| Cooling rate (°C·min−1) | PASS | 0.03 ± 0.01 | 0.04 ± 0.01 |
| VEST | 0.06 ± 0.02 | 0.06 ± 0.02 | |
| Cooling time (min) | PASS | 53.1 ± 23.4 | 29.0 ± 9.5 |
| VEST | 31.2 ± 12.7 | 24.7 ± 14.4 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosokawa, Y.; Belval, L.N.; Adams, W.M.; Vandermark, L.W.; Casa, D.J. Chemically Activated Cooling Vest’s Effect on Cooling Rate Following Exercise-Induced Hyperthermia: A Randomized Counter-Balanced Crossover Study. Medicina 2020, 56, 539. https://doi.org/10.3390/medicina56100539
Hosokawa Y, Belval LN, Adams WM, Vandermark LW, Casa DJ. Chemically Activated Cooling Vest’s Effect on Cooling Rate Following Exercise-Induced Hyperthermia: A Randomized Counter-Balanced Crossover Study. Medicina. 2020; 56(10):539. https://doi.org/10.3390/medicina56100539
Chicago/Turabian StyleHosokawa, Yuri, Luke N. Belval, William M. Adams, Lesley W. Vandermark, and Douglas J. Casa. 2020. "Chemically Activated Cooling Vest’s Effect on Cooling Rate Following Exercise-Induced Hyperthermia: A Randomized Counter-Balanced Crossover Study" Medicina 56, no. 10: 539. https://doi.org/10.3390/medicina56100539
APA StyleHosokawa, Y., Belval, L. N., Adams, W. M., Vandermark, L. W., & Casa, D. J. (2020). Chemically Activated Cooling Vest’s Effect on Cooling Rate Following Exercise-Induced Hyperthermia: A Randomized Counter-Balanced Crossover Study. Medicina, 56(10), 539. https://doi.org/10.3390/medicina56100539