Music Therapy in Pain and Anxiety Management during Labor: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
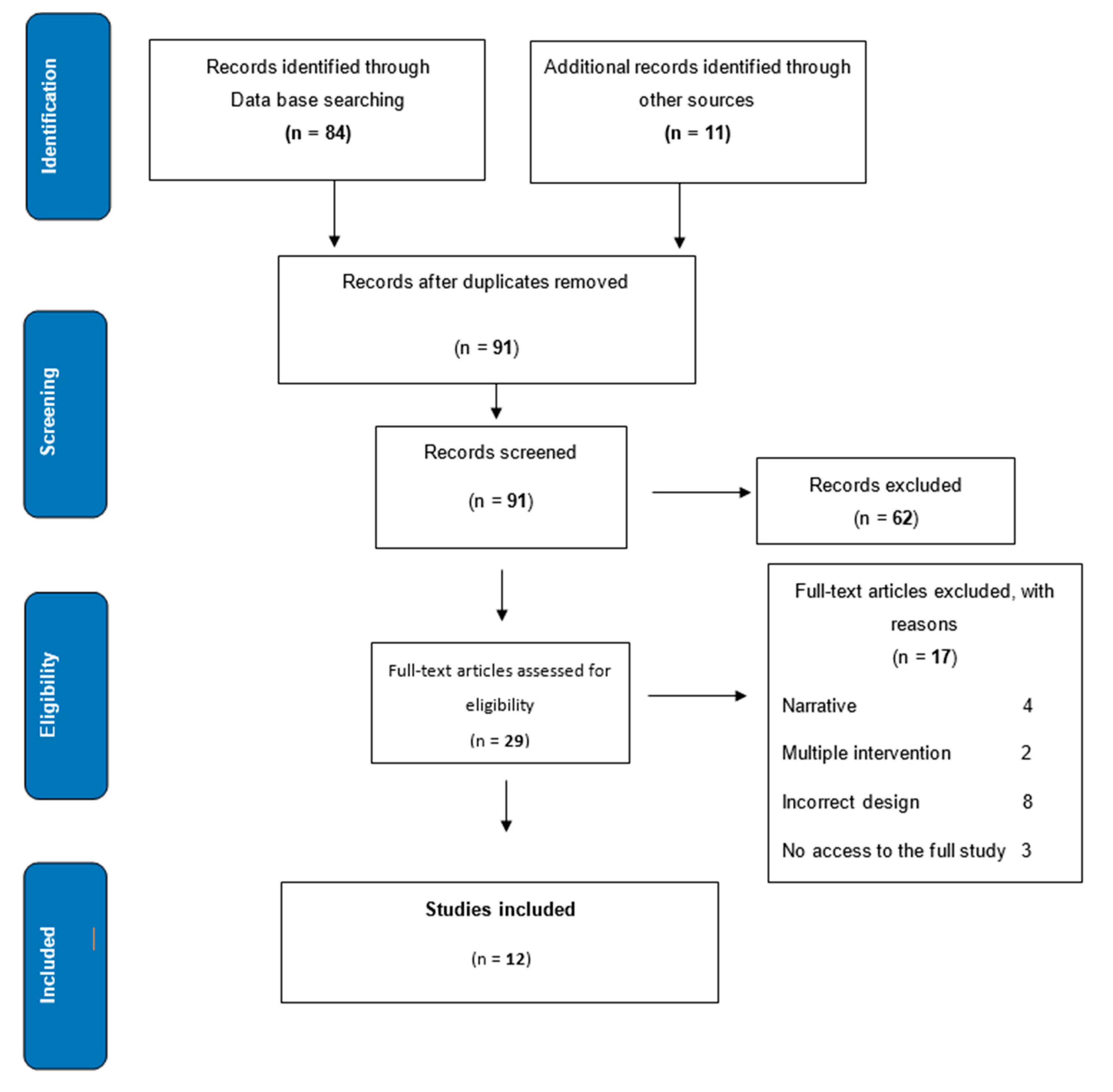
2. Materials and Methods
3. Results
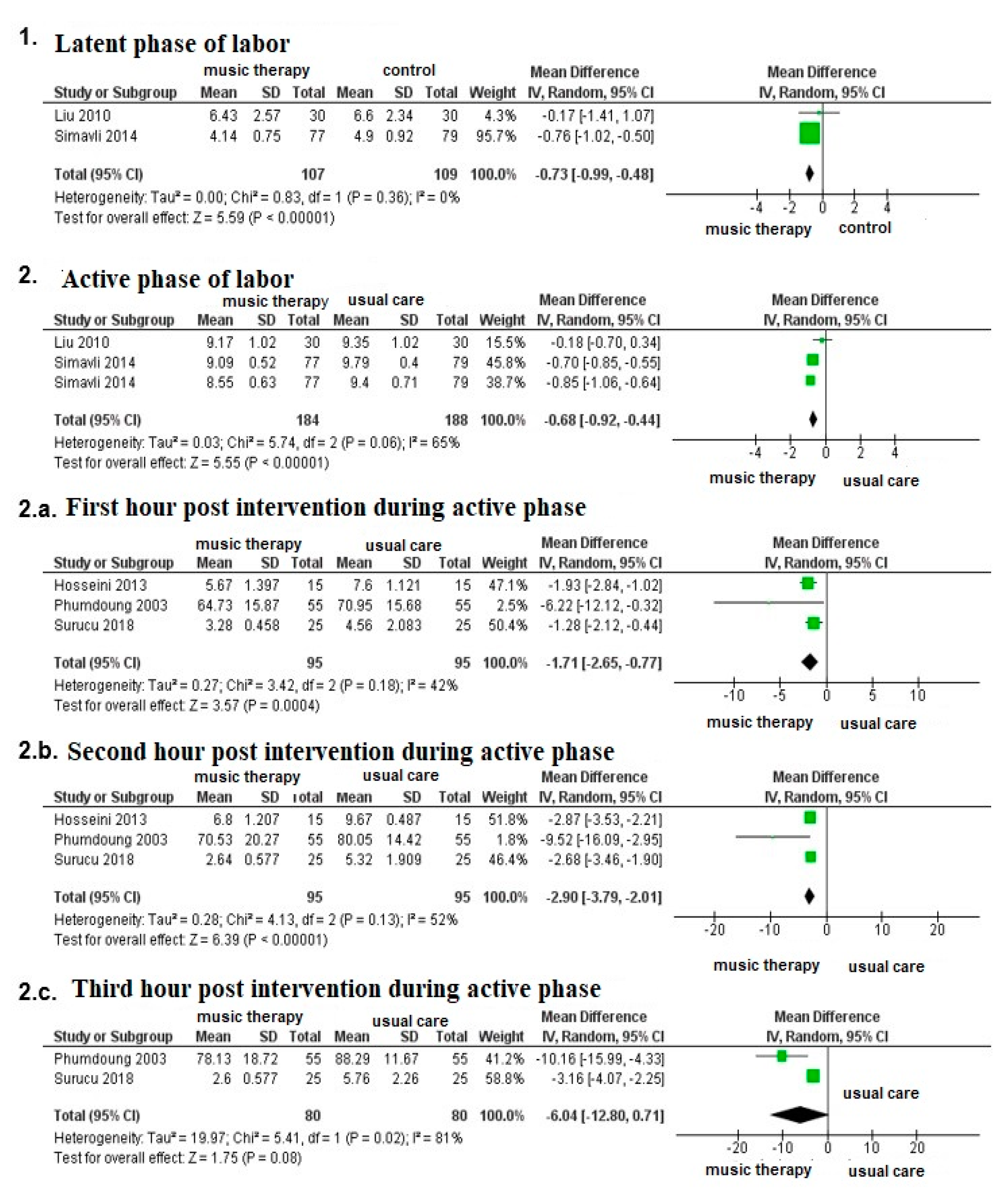
3.1. Effect of Music Therapy on Labor Pain
3.2. Effect of Music Therapy on Anxiety during Labor
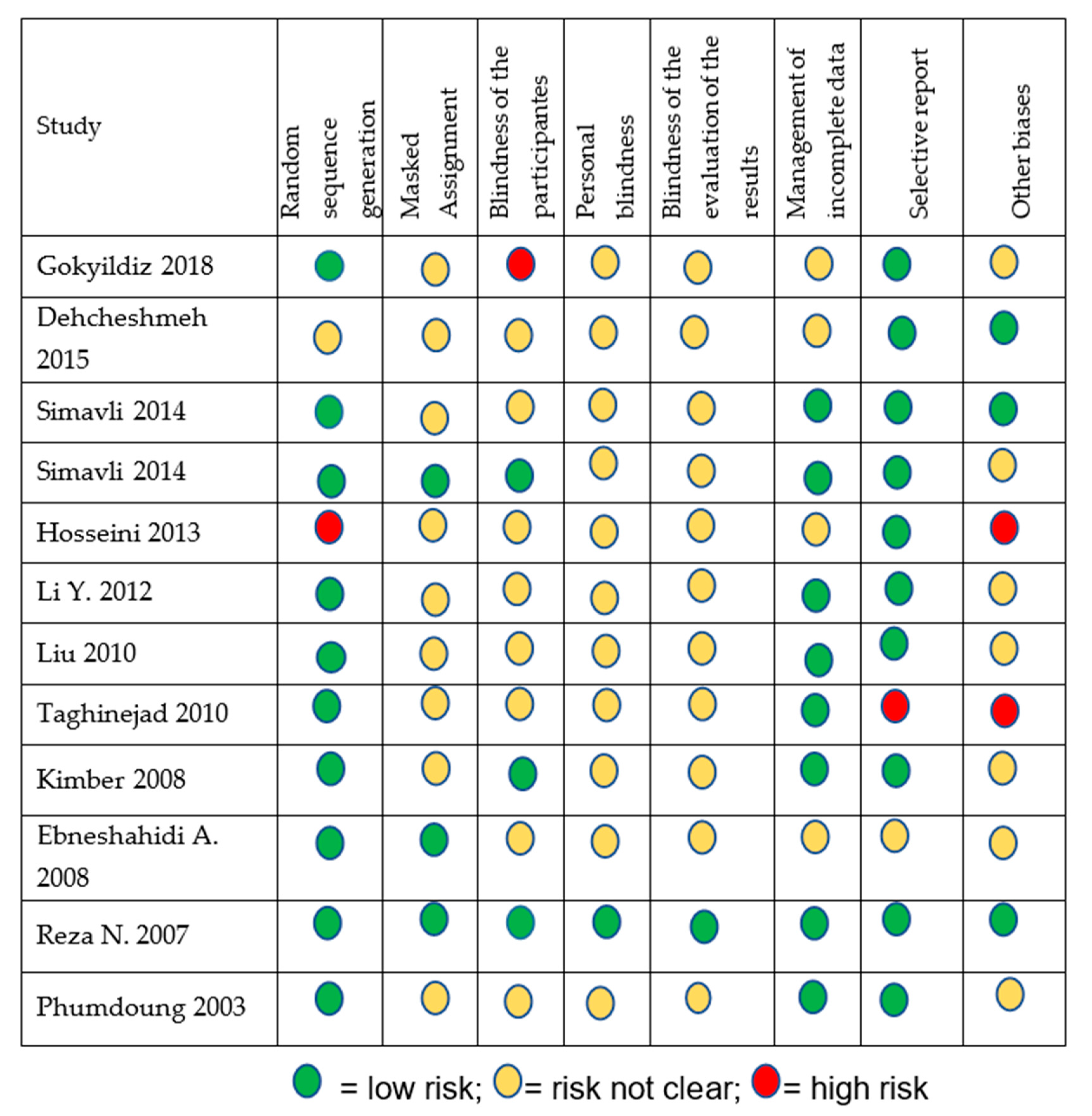
3.3. Quality of Evidence Found
3.4. Other Secondary Outcomes
3.5. Safety and Adverse Effects of Music Therapy
4. Discussion
5. Conclusions
Authors Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vink, A.; Hanser, S. Music-Based Therapeutic Interventions for People with Dementia: A Mini-Review. Medicina 2018, 5, 109. [Google Scholar] [CrossRef] [PubMed]
- Miranda Marcelo, C.; Hazard Sergio, O.; Miranda Pablo, V. La música como una herramienta terapéutica en medicina. Rev. Chil. Neuro-Psiquiatr. 2017, 55, 266–277. [Google Scholar] [CrossRef][Green Version]
- Kamioka, H.; Tsutani, K.; Yamada, M.; Park, H.; Okuizumi, H.; Tsuruoka, K.; Honda, T.; Okada, S.; Park, S.-J.; Kitayuguchi, J.; et al. Effectiveness of music therapy: A summary of systematic reviews based on randomized controlled trials of music interventions. Patient Prefer. Adherence 2014, 8, 727–754. [Google Scholar] [CrossRef] [PubMed]
- Benenzon, R. Musicoterapia De la Teoría a la Práctica; Paidos: Barcelona, Spain, 2000. [Google Scholar]
- González, J.G.; Miranda, M.I.V.; Mullor, M.R.; Carreño, T.P.; Rodriguez, R.A. Effects of prenatal music stimulation on state/trait anxiety in full-term pregnancy and its influence on childbirth: A randomized controlled trial. J. Matern. Neonatal Med. 2017, 31, 1058–1065. [Google Scholar] [CrossRef]
- Hepp, P.; Hagenbeck, C.; Gilles, J.; Wolf, O.T.; Goertz, W.; Janni, W.; Balan, P.; Fleisch, M.; Fehm, T.; Schaal, N.K. Effects of music intervention during caesarean delivery on anxiety and stress of the mother a controlled, randomised study. BMC Pregnancy Childbirth 2018, 18, 435. [Google Scholar] [CrossRef]
- Teckenberg-Jansson, P.; Turunen, S.; Pölkki, T.; Lauri-Haikala, M.-J.; Lipsanen, J.; Henelius, A.; Aitokallio-Tallberg, A.; Pakarinen, S.; Leinikka, M.; Huotilainen, M. Effects of live music therapy on heart rate variability and self-reported stress and anxiety among hospitalized pregnant women: A randomized controlled trial. Nord. J. Music. Ther. 2019, 28, 7–26. [Google Scholar] [CrossRef]
- Smith, C.A.; Levett, K.M.; Collins, C.T.; Armour, M.; Dahlen, H.G.; Suganuma, M. Relaxation techniques for pain management in labour. Cochrane Database Syst. Rev. 2018, 2018, CD009514. [Google Scholar] [CrossRef]
- Ministerio de Salud. Guía Técnica para la Psicoprofilaxis Obstétrica y Estimulación Prenatal; MINSA: Lima, Peru, 2012; pp. 1–49. [Google Scholar]
- Santiváñez, R.; Condori, C.; Loayza, M.; Vásquez, P.; Valeriano, L.; Instituto Nacional de Salud. Manual de Registro y Codificación de Actividades en la Atención de Medicina Alternativa y Medicina Complementaria. Serie de Manuales HIS N°05; INS-MINSA: Lima, Peru, 2016. [Google Scholar]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef]
- Gokyildiz Surucu, S.; Ozturk, M.; Avcibay Vurgec, B.; Alan, S.; Akbas, M. The effect of music on pain and anxiety of women during labour on first time pregnancy: A study from Turkey. Complement. Ther. Clin. Pract. 2018, 30, 96–102. [Google Scholar] [CrossRef]
- Dehcheshmeh, F.S.; Rafiei, H. Complementary and alternative therapies to relieve labor pain: A comparative study between music therapy and Hoku point ice massage. Complement. Ther. Clin. Pract. 2015, 21, 229–232. [Google Scholar] [CrossRef]
- Simavli, S.A.; Kaygusuz, I.; Gumus, I.; Usluogulları, B.; Yildirim, M.; Kafali, H.; Usluogullari, B.; Yildirim, M. Effect of music therapy during vaginal delivery on postpartum pain relief and mental health. J. Affect. Disord. 2014, 156, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Simavli, S.A.; Gumus, I.; Kaygusuz, I.; Yildirim, M.; Usluogullari, B.; Kafali, H. Effect of Music on Labor Pain Relief, Anxiety Level and Postpartum Analgesic Requirement: A Randomized Controlled Clinical Trial. Gynecol. Obstet. Investig. 2014, 78, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.E.; Bagheri, M.; Honarparvaran, N. Investigating the effect of music on labor pain and progress in the active stage of first labor. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 1479–1487. [Google Scholar] [PubMed]
- Li, Y.; Dong, Y. Preoperative music intervention for patients undergoing cesarean delivery. Int. J. Gynecol. Obstet. 2012, 119, 81–83. [Google Scholar] [CrossRef]
- Liu, Y.-H.; Chang, M.-Y.; Chen, C.-H. Effects of music therapy on labour pain and anxiety in Taiwanese first-time mothers. J. Clin. Nurs. 2010, 19, 1065–1072. [Google Scholar] [CrossRef]
- Taghinejad, H.; Delpisheh, A.; Suhrabi, Z. Comparison between massage and music therapies to relieve the severity of labor pain. Womens Health 2010, 6, 377–381. [Google Scholar] [CrossRef]
- Kimber, L.; McNabb, M.; Court, C.; Haines, A.; Brocklehurst, P. Massage or music for pain relief in labour: A pilot randomised placebo controlled trial. Eur. J. Pain 2008, 12, 961–969. [Google Scholar] [CrossRef]
- Ebneshahidi, A.; Mohseni, M. The Effect of Patient-Selected Music on Early Postoperative Pain, Anxiety, and Hemodynamic Profile in Cesarean Section Surgery. J. Altern. Complement. Med. 2008, 14, 827–831. [Google Scholar] [CrossRef]
- Reza, N.; Ali, S.M.; Saeed, K.; Abul-Qasim, A.; Reza, T.H. The impact of music on postoperative pain and anxiety following cesarean section. Middle East J. Anaesthesiol. 2007, 19, 573–586. [Google Scholar]
- Phumdoung, S.; Good, M. Music reduces sensation and distress of labor pain. Pain Manag. Nurs. 2003, 4, 54–61. [Google Scholar] [CrossRef]
- Smith, C.A.; Levett, K.M.; Collins, C.T.; Dahlen, H.G.; Ee, C.C.; Suganuma, M. Massage, reflexology and other manual methods for pain management in labour. Cochrane Database Syst. Rev. 2018, 2018, CD009290. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | n | Comparator | Patients | Type of Delivery | Kind of Music | Evaluation |
|---|---|---|---|---|---|---|
| Gokyildiz (2018) [12] | 50 | Conventional therapy | Primiparous | Normal delivery | Acemasiran | Labor (active phase) and postpartum |
| Dehcheshmeh (2015) [13] | 90 | Hoku point ice massage and conventional therapy | Primiparous | Normal delivery | Sounds of the sea | Labor (active phase) |
| Simavli (2014) [14] | 156 | Conventional therapy | Primiparous | Both of them | Classical, Turkish artistic music, Turkish folklore, Turkish classical and popular music | Labor (latent phase and active phase) and postpartum |
| Simavli (2014) [15] | 161 | Conventional therapy | Primiparous | Normal delivery | Classical, light, popular, artistic Turkish or Turkish folk music and Turkish Sufi music. | Postpartum |
| Hosseini (2013) [16] | 30 | Conventional therapy | Primiparous | Normal delivery | Relaxing music | Labor (active phase) |
| Li (2012) [17] | 60 | Conventional therapy | Not specified | Cesarean delivery | Not specified | Post caesarean |
| Liu (2010) [18] | 103 | Conventional therapy | Primiparous | Normal delivery | Five types of relaxing music | Labor (latent phase and active phase) |
| Taghinejad (2010) [19] | 101 | Massage | Primiparous | Normal delivery | Classic | Labor (active phase) |
| Kimber (2008) [20] | 90 | Massage | Both of them | Both of them | Not specified | Labor (active phase) |
| Ebneshahidi (2008) [21] | 77 | Conventional therapy | Not specified | Cesarean delivery | Not specified | Post Caesarean |
| Reza (2007) [22] | 100 | White music | Not specified | Cesarean delivery | Spanish guitar | Post Caesarean |
| Phumdoung (2003) [23] | 110 | Conventional therapy | Primiparous | Normal delivery | Five types of soft music | Labor (active phase) |
| Outcomes | Absolute Anticipated Effects * (95% CI) | Relative Effect (95% CI) | No. of Participants (Studies) | Certainty of the Evidence (GRADE) | |
|---|---|---|---|---|---|
| Risk with or without Therapies | Risk with Music Intervention for Pain and Anxiety Management | ||||
| Labor Pain | |||||
| Latent labor pain | The average pain during latent labor in the intervention group was 0.73 lower (0.99 less than 0.48 less) | - | 2 Randomized controlled experiments (RCTs) | ⨁◯◯◯ VERY LOW | |
| Active labor pain | The mean pain in the active phase of labor in the intervention group was 0.68 lower (0.92 less than 0.44 less) | - | 3 RCTs | ⨁⨁⨁◯ MODERATE | |
| Pain in the first hour postintervention during the active phase of labor | The average pain in the first hour after intervention during the active phase of labor in the intervention group was 1.71 lower (2.65 less than 0.77 less) | - | 3 RCTs | ⨁⨁◯◯ LOW | |
| Pain in the second hour postintervention during the active phase of labor | The average pain in the second hour postintervention during the active phase of labor in the intervention group was 2.9 lower (3.79 less than 2.01 less) | - | 3 RCTs | ⨁⨁◯◯ LOW | |
| Pain in the third hour postintervention during the active phase of labor | The average pain in the third hour postintervention during the active phase of labor in the intervention group was 6.04 lower (12.8 lower than 0.71 higher) | - | 2 RCTs | ⨁⨁◯◯ LOW | |
| Anxiety during Labor | |||||
| Latent labor anxiety | The average latent phase anxiety of labor in the intervention group was 0.74 lower (1 lower than 0.48 lower) | - | 2 RCTs | ⨁◯◯◯ VERY LOW | |
| Anxiety in active phase of labor | The average anxiety during labor phase in the intervention group was 0.76 lower (0.88 lower than 0.64 lower) | - | 3 RCTs | ⨁⨁⨁◯ MODERATE | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santiváñez-Acosta, R.; Tapia-López, E.d.l.N.; Santero, M. Music Therapy in Pain and Anxiety Management during Labor: A Systematic Review and Meta-Analysis. Medicina 2020, 56, 526. https://doi.org/10.3390/medicina56100526
Santiváñez-Acosta R, Tapia-López EdlN, Santero M. Music Therapy in Pain and Anxiety Management during Labor: A Systematic Review and Meta-Analysis. Medicina. 2020; 56(10):526. https://doi.org/10.3390/medicina56100526
Chicago/Turabian StyleSantiváñez-Acosta, Rocio, Elena de las Nieves Tapia-López, and Marilina Santero. 2020. "Music Therapy in Pain and Anxiety Management during Labor: A Systematic Review and Meta-Analysis" Medicina 56, no. 10: 526. https://doi.org/10.3390/medicina56100526
APA StyleSantiváñez-Acosta, R., Tapia-López, E. d. l. N., & Santero, M. (2020). Music Therapy in Pain and Anxiety Management during Labor: A Systematic Review and Meta-Analysis. Medicina, 56(10), 526. https://doi.org/10.3390/medicina56100526