An Overview of the Cardiorespiratory Hypothesis and Its Potential Contribution to the Care of Neurodegenerative Disease in Africa


Abstract
1. Introduction
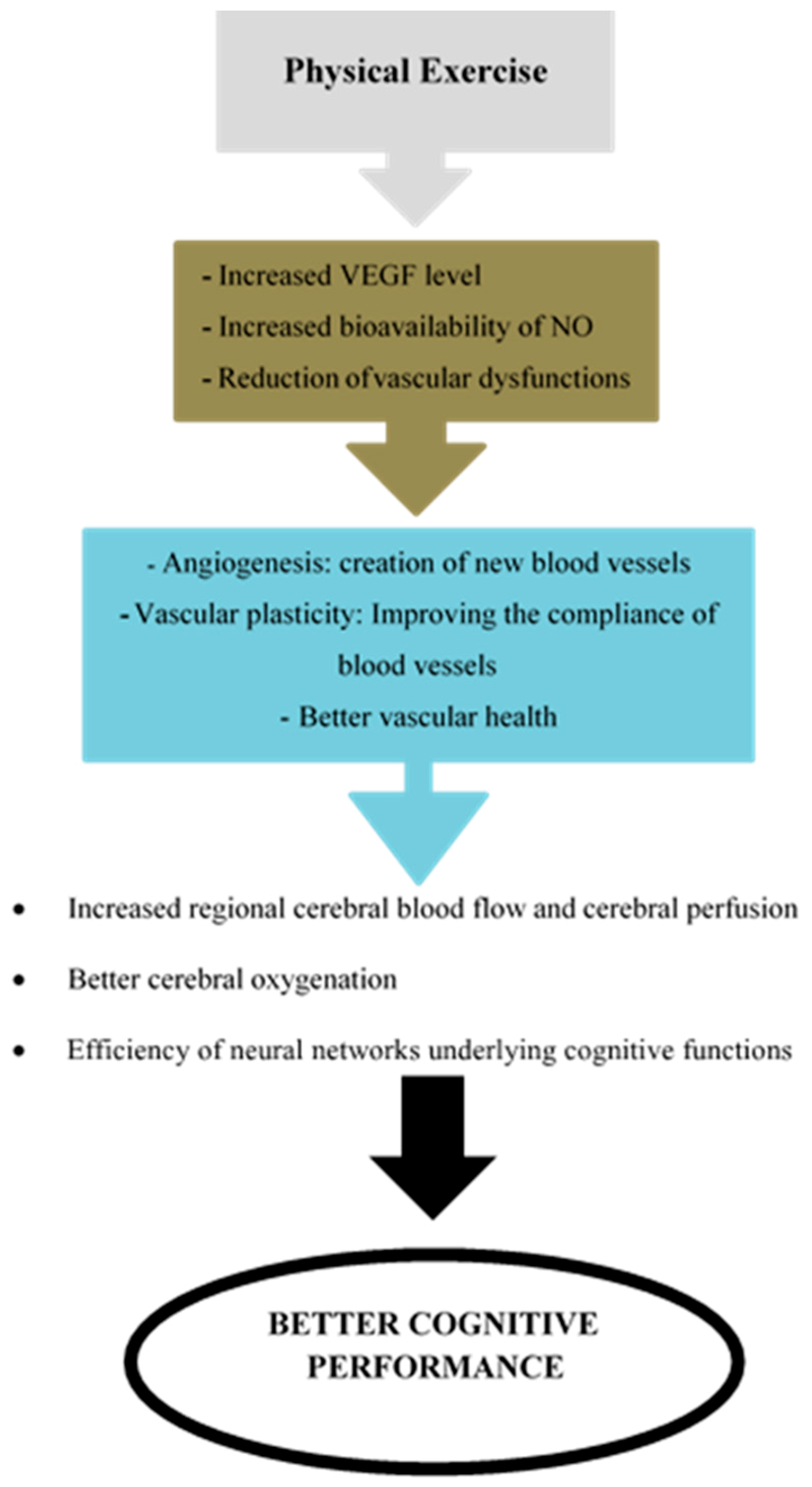
2. What Is the Cardiorespiratory Hypothesis?
3. Cardiorespiratory Hypothesis and Cognitive Decline
4. Future Research Directions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects: The 2017 Revision; UN Department of Economic and Social Affairs: New York, NY, USA, 2017. [Google Scholar]
- Kuate-Defo, B. Facteurs associés à la santé perçue et à la capacité fonctionnelle des personnes âgées dans la préfecture de Bandjoun au Cameroun. Cah. Québécois Démogr. 2005, 34, 1–46. [Google Scholar] [CrossRef]
- Antoine, P. Vieillir en Afrique. Idées Écon. Soc. 2009, 3, 34–37. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Disability 2011; World Health Organization: Geneva, Switzerland, 2011. Available online: https://www.ncbi.nlm.nih.gov/books/NBK304079/ (accessed on 20 June 2019).
- Thorin-Trescases, N.; Voghel, G.; Farhat, N.; Drouin, A.; Gendron, M.E.; Thorin, E. Âge et stress oxydant vers un déséquilibre irréversible de l’homéostasie endothéliale. Méd. Sci. 2010, 26, 875–880. [Google Scholar]
- Guerchet, M.; Houinato, D.; Paraiso, M.N.; von Ahsen, N.; Nubukpo, P.; Otto, M.; Clément, J.-P.; Preux, P.-M.; Dartigues, J.F. Cognitive impairment and dementia in elderly people living in rural Benin, West Africa. Dement. Geriatr. Cogn. Disord. 2009, 27, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Guerchet, M.; M’belesso, P.; Mouanga, A.M.; Bandzouzi, B.; Tabo, A.; Houinato, D.S.; Paraïso, M.N.; Cowppli-Bony, P.; Nubukpo, P.; Aboyans, V.; et al. Prevalence of dementia in elderly living in two cities of Central Africa: The EDAC survey. Dement. Geriatr. Cogn. Disord. 2010, 30, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Guerchet, M.; Mouanga, A.M.; M’belesso, P.; Tabo, A.; Bandzouzi, B.; Paraïso, M.N.; Houinato, D.S.; Cowppli-Bony, P.; Nubukpo, P.; Aboyans, V.; et al. Factors associated with dementia among elderly people living in two cities in Central Africa: The EDAC multicenter study. J. Alzheimer’s Dis. 2012, 29, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Gureje, O.; Ogunniyi, A.; Kola, L. The profile and impact of probable dementia in a sub-Saharan African community: Results from the Ibadan study of ageing. J. Psychosom. Res. 2006, 61, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Hendrie, H.C.; Murrell, J.; Baiyewu, O.; Lane, K.A.; Purnell, C.; Ogunniyi, A.; Unverzagt, F.W.; Hall, K.; Callahan, C.M.; Saykin, A.J.; et al. APOE ε4 and the risk for Alzheimer disease and cognitive decline in African Americans and Yoruba. Int. Psychogeriatr. 2014, 26, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Ogunniyi, A.; Hall, K.S.; Gureje, O.; Baiyewu, O.; Gao, S.; Unverzagt, F.W.; Smith-Gamble, V.; Evans, R.E.; Dickens, J.; Musick, B.S.; et al. Risk factors for incident Alzheimer’s disease in African Americans and Yoruba. Metab. Brain Dis. 2006, 21, 235–240. [Google Scholar] [CrossRef]
- Paraïso, M.N.; Guerchet, M.; Saizonou, J.; Cowppli-Bony, P.; Mouanga, A.M.; Nubukpo, P.; Preux, P.-M.; Houinato, D.S. Prevalence of dementia among elderly people living in Cotonou, an urban area of Benin (West Africa). Neuroepidemiology 2001, 36, 245–251. [Google Scholar] [CrossRef]
- Touré, K.; Coume, M.; Ndiaye, M.; Zunzunegui, M.V.; Bacher, Y.; Diop, A.G.; Ndiaye, M.M. Risk factors for dementia in a Senegalese elderly population aged 65 years and over. Dement. Geriatr. Cogn. Disord. Extra 2012, 2, 160–168. [Google Scholar] [CrossRef]
- Touré, K.; Coume, M.; Ndiaye/Ndongo, N.D.; Basse, A.; Sow, A.; Seck, L.B. Déficit cognitif dans une population de patients âgés sénégalais du centre médico-social et universitaire de l’IPRES, Dakar-Sénégal: Prévalence et facteurs de risque. Rev. Afr. Malgache Rech. Sci. 2013, 1, 55–65. [Google Scholar]
- De Jager, C.A.; Msemburi, W.; Pepper, K.; Combrinck, M.I. Dementia prevalence in a rural region of south Africa: A cross-sectional community study. J. Alzheimer’s Dis. 2017, 60, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- George-Carey, R.; Adeloye, D.; Chan, K.Y.; Paul, A.; Kolčić, I.; Campbell, H.; Rudan, I. An estimate of the prevalence of dementia in Africa: A systematic analysis. J. Glob. Health 2012, 2, 020401. [Google Scholar] [CrossRef] [PubMed]
- Ferri, C.P.; Prince, M.; Brayne, C.; Brodaty, H.; Fratiglioni, L.; Ganguli, M.; Hall, K.; Hasegawa, K.; Hendrie, H.; Huang, Y.; et al. Global prevalence of dementia: A Delphi consensus study. Lancet 2005, 366, 2112–2117. [Google Scholar] [CrossRef]
- El Tallawy, H.N.; Farghly, W.M.; Shehata, G.A.; Rageh, T.A.; Hakeem, N.A.; Abo-Elfetoh, N.; Hegazy, A.M.; Rayan, I.; El-Moselhy, E.A. Prevalence of dementia in Al Kharga District, New Valley Governorate, Egypt. Neuroepidemiology 2012, 38, 130–137. [Google Scholar] [CrossRef]
- Achouri-Rassas, A.; Hadj Fredj, S.; Mrabet Khiari, H.; Bibi, A.; Siala, H.; Mrabet, A.; Messaoud, T. Association between Alzheimer disease and the −491T allele of regulatory region polymorphism of apolipoprotein E in a Tunisian population. Neurochem. Res. 2014, 39, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Ineichen, B. The epidemiology of dementia in Africa: A review. Soc. Sci. Med. 2000, 50, 1673–1677. [Google Scholar] [CrossRef]
- Rolland, Y.; van Kan, G.A.; Vellas, B. Physical activity and Alzheimer’s disease: From prevention to therapeutic perspectives. J. Am. Med. Dir. Assoc. 2008, 9, 390–405. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Wang, H.F.; Wan, Y.; Tan, C.C.; Yu, J.T.; Tan, L. Leisure time physical activity and dementia risk: A dose-response meta-analysis of prospective studies. BMJ Open 2017, 7, e014706. [Google Scholar] [CrossRef]
- Dustman, R.E.; Ruhling, R.O.; Russell, E.M.; Shearer, D.E.; Bonekat, H.W.; Shigeoka, J.W.; Wood, J.S.; Bradford, D.C. Aerobic exercise training and improved neuropsychological function of older individuals. Neurobiol. Aging 1984, 5, 35–42. [Google Scholar] [CrossRef]
- Audiffren, M.; André, N.; Albinet, C.T. Positive effects of chronic physical exercise on cognitive functions in aging people: Assessment and prospects. Rev. Neuropsychol. 2011, 3, 207–225. [Google Scholar] [CrossRef]
- Albinet, C.T.; Mandrick, K.; Bernard, P.L.; Perrey, S.; Blain, H. Improved cerebral oxygenation response and executive performance as a function of cardiorespiratory fitness in older women: A fNIRS study. Front. Aging Neurosci. 2014, 6, 272. [Google Scholar] [CrossRef]
- Marmeleira, J. An examination of the mechanisms underlying the effects of physical activity on brain and cognition: A review with implications for research. Eur. Rev. Aging Phys. Act. 2013, 10, 83–94. [Google Scholar] [CrossRef]
- Schmidt, W.; Endres, M.; Dimeo, F.; Jungehulsing, G.J. Train the vessel, gain the brain: Physical: Physical activity and vessel function and the impact on stroke prevention and outcome in cerebrovascular disease. Cerebrovasc. Dis. 2013, 35, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Voss, M.W.; Vivar, C.; Kramer, A.F.; van Praag, H. Bridging animal and human models of exercise-induced brain plasticity. Trends Cogn. Sci. 2013, 17, 525–544. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Lopez, C.; LeRoith, D.; Torres-Aleman, I. Insulin-like growth factor I is required for vessel remodeling in the adult brain. Proc. Natl. Acad. Sci. USA 2004, 101, 9833–9838. [Google Scholar] [CrossRef] [PubMed]
- Kleim, J.A.; Cooper, N.R.; VandenBerg, P.M. Exercise induces angiogenesis but does not alter movement representations within rat motor cortex. Brain Res. 2002, 934, 1–6. [Google Scholar] [CrossRef]
- Creer, D.J.; Romberg, C.; Saksida, L.M.; van Praag, H.; Bussey, T.J. Running enhances spatial pattern separation in mice. Proc. Natl. Acad. Sci. USA 2010, 107, 2367–2372. [Google Scholar] [CrossRef]
- Black, J.E.; Isaacs, K.R.; Anderson, B.J.; Alcantara, A.A.; Greenough, W.T. Learning causes, synaptogenesis, whereas motor activity causes angiogenesis, in cerebellar cortex of adult rats. Proc. Natl. Acad. Sci. USA 1990, 87, 5568–5572. [Google Scholar] [CrossRef]
- Bullitt, E.; Rahman, F.N.; Smith, J.K.; Kim, E.; Zeng, D.; Katz, L.M.; Marks, B.L. The effect of exercise on the cerebral vasculature of healthy aged subjects as visualized by MR angiography. Am. J. Neuroradiol. 2009, 30, 1857–1863. [Google Scholar] [CrossRef] [PubMed]
- Burdette, J.H.; Laurienti, P.J.; Espeland, M.A.; Morgan, A.; Telesford, Q.; Vechlekar, C.D.; Hayasaka, S.; Jennings, J.M.; Katula, J.A.; Rejeski, W.J.; et al. Using network science to evaluate exercise-associated brain changes in older adults. Front. Aging Neurosci. 2010, 2. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.B.; Aslan, S.; Spence, J.S.; Defina, L.F.; Keebler, M.W.; Didehbani, N. Shorter term aerobic exercise improves brain, cognition, and cardiovascular fitness in aging. Front. Aging Neurosci. 2013, 5, 75. [Google Scholar] [CrossRef] [PubMed]
- Steppan, J.; Sikka, G.; Jandu, S.; Barodka, V.; Halushka, M.K.; Flavahan, N.A.; Belkin, A.M.; Nyhan, D.; Butlin, M.; Santhanam, L.; et al. Exercise, vascular stiffness, and tissue transglutaminase. J. Am. Heart Assoc. 2014, 3, e000599. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Dinenno, F.A.; Monahan, K.D.; Clevenger, C.M.; DeSouza, C.A.; Seals, D.R. Aging, habitual exercise, and dynamic arterial compliance. Circulation 2000, 102, 1270–1275. [Google Scholar] [CrossRef]
- Van Merode, T.; Hick, P.J.; Hoeks, A.P.; Rahn, K.H.; Reneman, R.S. Carotid artery wall properties in normotensive and borderline hypertensive subjects of various ages. Ultrasound Med. Biol. 1988, 14, 563–569. [Google Scholar] [CrossRef]
- Hirai, T.; Sasayama, S.; Kawasaki, T.; Yagi, S. Stiffness of systemic arteries in patients with myocardial infarction. A noninvasive method to predict severity of coronary atherosclerosis. Circulation 1989, 80, 78–86. [Google Scholar] [CrossRef]
- Di Francescomarino, S.; Sciartilli, A.; Di Valerio, V.; Di Baldassarre, A.; Gallina, S. The effect of physical exercise on endothelial function. Sports Med. 2009, 39, 797–812. [Google Scholar] [CrossRef]
- Feairheller, D.L.; Diaz, K.M.; Kashem, M.A.; Thakkar, S.R.; Veerabhadrappa, P.; Sturgeon, K.M.; Williamson, S.T.; Kretzschmar, J.; Lee, H.; Grimm, H.; et al. Effects of moderate aerobic exercise training on vascular health and blood pressure in African Americans. J. Clin. Hypertens. 2014, 16, 504–510. [Google Scholar] [CrossRef]
- Montero, D.; Vinet, A.; Roberts, C.K. Effect of combined aerobic and resistance training versus aerobic training on arterial stiffness. Int. J. Cardiol. 2015, 178, 69–76. [Google Scholar] [CrossRef]
- Hajjar, I.; Goldstein, F.C.; Martin, G.S.; Quyyumi, A.A. Roles of arterial stiffness and blood pressure in hypertension-associated cognitive decline in healthy adults. Hypertension 2016, 67, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Albinet, C.; Fezzani, K.; Thon, B.V. Vieillissement, activité physique et cognition. Mov. Sport Sci. 2008, 63, 9–36. [Google Scholar] [CrossRef]
- Mokdad, A.H.; Marks, J.S.; Stroup, D.F.; Gerberding, J.L. Actual causes of death in the United States, 2000. JAMA 2004, 291, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Barton, M. Aging and endothelin: Determinants of disease. Life Sci. 2014, 118, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Fagard, R.H. Effects of endurance training on blood pressure, blood pressure regulating mechanisms, and cardiovascular risk factors. Hypertension 2005, 46, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Falsetti, L.; Viticchi, G.; Buratti, L.; Grigioni, F.; Capucci, A.; Silvestrini, M. Interactions between atrial fibrillation, cardiovascular risk factors, and ApoE genotype in promoting cognitive decline in patients with Alzheimer’s disease: A prospective cohort study. J. Alzheimer’s Dis. 2018, 62, 713–725. [Google Scholar] [CrossRef] [PubMed]
- Werner, C.; Fürster, T.; Widmann, T.; Pöss, J.; Roggia, C.; Hanhoun, M.; Scharhag, J.; Büchner, N.; Meyer, T.; Kindermann, W.; et al. Physical exercise prevents cellular senescence in circulating leukocytes and in the vessel wall. Circulation 2009, 120, 2438–2447. [Google Scholar] [CrossRef] [PubMed]
- Getty, A.K.; Wisdo, T.R.; Chavis, L.N.; Derella, C.C.; McLaughlin, K.C.; Perez, A.N.; Di Ciurcio, W.T.; Corbin, M.; Feairheller, D.L. Effects of circuit exercise training on vascular health and blood pressure. Prev. Med. Rep. 2018, 10, 106–112. [Google Scholar] [CrossRef]
- Shimizu, R.; Hotta, K.; Yamamoto, S.; Matsumoto, T.; Kamiya, K.; Kato, M.; Hamazaki, N.; Kamekawa, D.; Akiyama, A.; Kamada, Y.; et al. Low-intensity resistance training with blood flow restriction improves vascular endothelial function and peripheral blood circulation in healthy elderly people. Eur. J. Appl. Physiol. 2016, 116, 749–757. [Google Scholar] [CrossRef]
- Holloway, T.M.; Morton, R.W.; Oikawa, S.Y.; McKellar, S.; Baker, S.K.; Phillips, S.M. Microvascular adaptations to resistance training are independent of load in resistance-trained young men. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2018, 315, 267–273. [Google Scholar] [CrossRef]
- Li, Y.; Hanssen, H.; Cordes, M.; Rossmeissl, A.; Endes, S.; Schmidt-Trucksäss, A. Aerobic, resistance and combined exercise training on arterial stiffness in normotensive and hypertensive adults: A review. Eur. J. Sport Sci. 2015, 15, 443–457. [Google Scholar] [CrossRef] [PubMed]
- Herold, F.; Törpel, A.; Schega, L.; Müller, N.G. Functional and/or structural brain changes in response to resistance exercises and resistance training lead to cognitive improvements—A systematic review. Eur. Rev. Aging Phys. Act. 2019, 16, 10. [Google Scholar] [CrossRef] [PubMed]
- Portugal, E.M.; Vasconcelos, P.G.; Souza, R.; Lattari, E.; Monteiro-Junior, R.S.; Machado, S.; Deslandes, A.C. Aging process, cognitive decline and Alzheimer’s disease: Can strength training modulate these responses? CNS Neurol. Disord. Drug Targets 2015, 14, 1209–1213. [Google Scholar] [CrossRef] [PubMed]
- Ploughman, M. Exercise is brain food: The effects of physical activity on cognitive function. Dev. Neurorehabilit. 2008, 11, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Goushcha, A.; Hushcha, T.; Christophorov, L.; Goldsby, M. Self-Organization and Coherency in Biology and Medicine. Open J. Biophys. 2014, 4, 119–146. [Google Scholar] [CrossRef][Green Version]
- Schulz, S.; Adochiei, F.C.; Edu, I.R.; Schroeder, R.; Costin, H.; Bär, K.J.; Voss, A. Cardiovascular and cardiorespiratory coupling analyses: A review. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2013, 371, 20120191. [Google Scholar] [CrossRef]
- Honea, R.; Thomas, G.P.; Harsha, A.; Anderson, H.S.; Donnelly, J.E.; Brooks, W.M.; Burns, J.M. Cardiorespiratory fitness and preserved medial temporal lobe volume in Alzheimer’s Disease. Alzheimer Dis. Assoc. Disord. 2009, 23, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Perea, R.; Vidoni, E.; Morris, J.; Graves, R.; Burns, J.; Honea, R. Cardiorespiratory fitness and white matter integrity in Alzheimer’s disease. Brain Imaging Behav. 2016, 10, 660–668. [Google Scholar] [CrossRef] [PubMed]
- Vidoni, E.D.; Honea, R.A.; Billinger, S.A.; Swerdlow, R.H.; Burns, J.M. Cardiorespiratory fitness is associated with atrophy in Alzheimer’s and aging over two years. Neurobiol. Aging 2012, 33, 1624–1632. [Google Scholar] [CrossRef]
- Vidoni, E.D.; Gayed, M.R.; Honea, R.A.; Savage, C.R.; Hobbs, D.; Burns, J.M. Alzheimer Disease alters the relationship of cardiorespiratory fitness with brain activity during the stroop task. Phys. Ther. 2013, 93, 993–1002. [Google Scholar] [CrossRef]
- Stuckenschneider, T.; Askew, C.D.; Rüdiger, S.; Polidori, M.C.; Abeln, V.; Vogt, T.; Krome, A.; Olde Rikkert, M.; Lawlor, B.; Schneider, S.; et al. Cardiorespiratory fitness and cognitive function are positively related among participants with mild and subjective cognitive impairment. J. Alzheimer’s Dis. 2018, 62, 1865–1875. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.M.; Cronk, B.B.; Anderson, H.S.; Donnelly, J.E.; Thomas, G.P.; Harsha, A.; Brooks, R.H.; Swerdlow, R.H. Cardiorespiratory fitness and brain atrophy in early Alzheimer’s disease. Neurology 2008, 71, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Schultz, S.A.; Boots, E.A.; Almeida, R.P.; Oh, J.M.; Einerson, J.; Korcarz, C.E.; Edwards, D.F.; Koscik, R.L.; Dowling, M.N.; Gallagher, C.L.; et al. Cardiorespiratory fitness attenuates the influence of amyloid on cognition. J. Int. Neuropsychol. Soc. 2015, 21, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Billinger, S.A.; Vidoni, E.D.; Morris, J.K.; Thyfault, J.P.; Burns, J.M. Exercise test performance reveals support of the cardiorespiratory fitness hypothesis. J. Aging Phys. Act. 2017, 25, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Sui, X.; Laditka, J.N.; Church, T.S.; Colabianchi, N.; Hussey, J.; Blair, S.N. Cardiorespiratory fitness as a predictor of dementia mortality in men and women. Med. Sci. Sports Exerc. 2012, 44, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Baker, L.D.; Frank, L.L.; Foster-Schubert, K.; Green, P.S.; Wilkinson, C.W.; McTiernan, A.; Plymate, S.R.; Fishel, M.A.; Watson, G.S.; Cholerton, B.A.; et al. Effects of Aerobic Exercise on Mild Cognitive Impairment: A Controlled Trial. Arch. Neurol. 2010, 67, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Reiter, K.; Nielson, K.A.; Smith, T.J.; Weiss, L.R.; Alfini, A.J.; Smith, J.C. Improved cardiorespiratory fitness is associated with increased cortical thickness in MCI. J. Int. Neuropsychol. Soc. 2015, 21, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Savik, K.; Wyman, J.F.; Bronas, U.G. Maintaining physical fitness and function in Alzheimer’s disease: A pilot study. Am. J. Alzheimer’s Dis. Dement. 2011, 26, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Sobol, N.A.; Hoffmann, K.; Frederiksen, K.S.; Vogel, A.; Vestergaard, K.; Brændgaard, H.; Gottrup, H.; Lolk, A.; Wermuth, L.; Jakobsen, S.; et al. Effect of aerobic exercise on physical performance in patients with Alzheimer’s disease. Alzheimer’s Dement. 2016, 12, 1207–1215. [Google Scholar] [CrossRef]
- Morris, J.K.; Vidoni, E.D.; Johnson, D.K.; Van Sciver, A.; Mahnken, J.D.; Honea, R.A.; Wilkins, H.M.; Brooks, W.M.; Billinger, S.A.; Swerdlow, R.H.; et al. Aerobic exercise for Alzheimer’s disease: A randomized controlled pilot trial. PLoS ONE 2017, 12, e0170547. [Google Scholar] [CrossRef]
- Bossers, W.J.; van der Woude, L.H.; Boersma, F.; Hortobágyi, T.; Scherder, E.J.; van Heuvelen, M.J. A 9-Week Aerobic and Strength Training Program Improves Cognitive and Motor Function in Patients with Dementia: A Randomized, Controlled Trial. Am. J. Geriatr. Psychiatry 2015, 23, 1106–1116. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.C.; Bryan, S.; Marra, C.A.; Sharma, D.; Chan, A.; Beattie, B.L.; Liu-Ambrose, T. An Economic Evaluation of Resistance Training and Aerobic Training versus Balance and Toning Exercises in Older Adults with Mild Cognitive Impairment. PLoS ONE 2013, 8, e63031. [Google Scholar] [CrossRef]
- Vital, T.M.; Hernández, S.S.S.; Pedroso, R.V.; Teixeira, C.V.L.; Garuffi, M.; Stein, A.M.; Costa, J.L.R.; Stella, F. Effects of weight training on cognitive functions in elderly with Alzheimer’s disease. Dement. Neuropsychol. 2012, 6, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Balagué, N.; González, J.; Javierre, C.; Hristovski, R.; Aragonés, D.; Álamo, J.; Ventura, J.L. Cardiorespiratory Coordination after Training and Detraining. A Principal Component Analysis Approach. Front. Physiol. 2016, 7, 35. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Retortillo, S.; Javierre, C.; Hristovski, R.; Ventura, J.L.; Balagué, N. Cardiorespiratory Coordination in Repeated Maximal Exercise. Front. Physiol. 2017, 8, 387. [Google Scholar] [CrossRef] [PubMed]
- Esquius, L.; Garcia-Retortillo, S.; Balagué, N.; Hristovski, R.; Javierre, C. Physiological- and performance-related effects of acute olive oil supplementation at moderate exercise intensity. J. Int. Soc. Sports Nutr. 2019, 16, 12. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Retortillo, S.; Gacto, M.; O’Leary, T.J.; Noon, M.; Hristovski, R.; Balagué, N.; Morris, M.G. Cardiorespiratory coordination reveals training-specific physiological adaptations. Eur. J. Appl. Physiol. 2019, 119, 1701–1709. [Google Scholar] [CrossRef]
- Obisesan, T.O.; Gillum, R.F.; Johnson, S.; Umar, N.; Williams, D.; Bond, V.; Kwagyan, J. Neuroprotection and neurodegeneration in Alzheimers disease: Role of cardiovascular disease risk factors, implications for dementia rates, and prevention with aerobic exercise in African Americans. Int. J. Alzheimer’s Dis. 2012, 2012, 568382. [Google Scholar]
- Izquierdo-Porrera, A.; Waldstein, S. Cardiovascular risk factors and cognitive function in African Americans. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2002, 57, 377–380. [Google Scholar] [CrossRef]
- Agbangla, N.F.; Audiffren, M.; Albinet, C.T. Use of near-infrared spectroscopy in the investigation of brain activation during cognitive aging: A systematic review of an emerging area of research. Ageing Res. Rev. 2017, 38, 52–66. [Google Scholar] [CrossRef]
- Metzger, F.G.; Schopp, B.; Haeussinger, F.B.; Dehnen, K.; Synofzik, M.; Fallgatter, A.J.; Ehlis, A.-C. Brain activation in frontotemporal and Alzheimer’s dementia: A functional near-infrared spectroscopy study. Alzheimer’s Res. Ther. 2016, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Agbangla, N.F.; Audiffren, M.; Pylouster, J.; Albinet, C.T. Working memory, cognitive load and cardiorespiratory fitness: Testing the CRUNCH model with near-infrared spectroscopy. Brain Sci. 2019, 9, 38. [Google Scholar] [CrossRef] [PubMed]
- Blasi, A.; Lloyd-Fox, S.; Johnson, M.H.; Elwell, C. Test-retest reliability of functional near infrared spectroscopy in infants. Neurophotonics 2014, 1, 025005. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Fox, S.; Begus, K.; Halliday, D.; Pirazzoli, L.; Blasi, A.; Papademetriou, M.; Darboe, M.K.; Prentice, A.M.; Johnson, M.H.; Moore, S.E. Cortical specialisation to social stimuli from the first days to the second year of life: A rural Gambian cohort. Dev. Cogn. Neurosci. 2017, 25, 92–104. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, R.P.; Liu, K.K.L.; Bashan, A.; Ivanov, P.C. Network Physiology: How Organ Systems Dynamically Interact. PLoS ONE 2015, 10, e0142143. [Google Scholar] [CrossRef]
- Ivanov, P.C.; Liu, K.K.L.; Bartsch, R.P. Focus on the emerging new fields of Network Physiology and Network Medicine. New J. Phys. 2016, 18, 100201. [Google Scholar] [CrossRef]
- Albinet, C. Habilitation à Diriger des Recherches “Des Effets de l’Exercice Physique Régulier sur les Performances Cognitives des Seniors, à la Recherche de Leurs Marqueurs Neuro-Physiologiques”; Sciences Cognitives; Université de Poitiers: Poitiers, France, 2016. [Google Scholar]


{kind=link}
| References | Characteristics of Training | Subjects | Measures | Main Results |
|---|---|---|---|---|
| [68] | Aerobic exercise: 4 sessions per week. The duration of the session varies between 45 and 60 min. The intensity of training increased from 75% to 85% HRR. Subjects of the control group carried out stretching and balance with an intensity that is less than 50% of the heart rate reserve. The duration of the training is six months. | 33 subjects (mean age 70 years) diagnosed with amnestic MCI were enrolled in the study. However, 19 subjects of the aerobic group and 10 subjects of control group included in analysis. | CRF, executive function and memory tests and plasma IGF-1 | CRF increased only in the aerobic exercise group. High-Intensity aerobic exercise improved the performance of multiple tests of executive function in women. However, for men, only the performance of the Trail-making test B has increased. Plasma IGF-1 increased after aerobic exercise intervention specifically in men. |
| [69] | Aerobic exercise: 120 min per week, spread over four sessions. The intensity of aerobic exercise increased from 50% to 60% of HRR. The duration of the training is three months. | 14 subjects with MCI (78.85 ± 7.75 years) and 16 healthy subjects (75.87 ± 6.9 years) were enrolled in the study. | Changes in CRF, cortical thickness with MRI | CRF increased from pre to post intervention in both groups. The increase in CRF was associated with widespread increased cortical thickness. |
| [70] | Aerobic exercise: Three sessions per week. The duration of the session was progressively increased to reach 45 min. The intensity of training is moderate and was evaluated by perceived exertion rating. The duration of the training is six months. | Eight subjects with AD (81.4 ± 3.58 years) were enrolled in the study. | CRF, lower extremity function with short physical performance battery | Subjects with AD are capable of participating in aerobic exercise intervention and appear to improve their CRF. |
| [71] | Aerobic exercise: 180 min per week, spread over three sessions; intensity: from 70% to 80% of maximal heart rate. The control group received usual care during the intervention period. The duration of the training is four months. | After the exclusion criteria, 200 subjects with AD were enrolled. 107 in aerobic exercise group (69.8 ± 7.4 years) and 93 in control group (71.3 ± 7.3 years). | Test of physical performance, test of dual-task performance (walk and naming the months backwards starting with January (dual-task month), test of exercise self-efficacy and tests of cognition and neuropsychiatric symptoms | Aerobic exercise improved potentially CRF single-task physical performance, dual-task performance, and exercise self-efficacy in patients with mild AD. |
| [72] | Aerobic exercise: 60–150 min per week, spread over 3–5 sessions; intensity: From 40–55% to 60–75% of HRR. Stretching and toning control group: Non-aerobic exercises with an intensity below 100 beats per minutes. The duration of the training is six months. | After the exclusion criteria, 76 subjects with probable AD were enrolled. 39 in aerobic exercise group (74.4 ± 6.7 years) and 37 in control group (71.4 ± 8.4 years). | Cognitive test battery, depression and functional ability, CRF, hippocampal and total gray matter volume with MRI (magnetic resonance imagery) | Aerobic exercise was associated with a modest gain in functional ability. Exercise-related gains in CRF were associated with improved memory performance and reduced hippocampal atrophy. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agbangla, N.F.; Fraser, S.A.; Albinet, C.T. An Overview of the Cardiorespiratory Hypothesis and Its Potential Contribution to the Care of Neurodegenerative Disease in Africa. Medicina 2019, 55, 601. https://doi.org/10.3390/medicina55090601
Agbangla NF, Fraser SA, Albinet CT. An Overview of the Cardiorespiratory Hypothesis and Its Potential Contribution to the Care of Neurodegenerative Disease in Africa. Medicina. 2019; 55(9):601. https://doi.org/10.3390/medicina55090601
Chicago/Turabian StyleAgbangla, Nounagnon Frutueux, Sarah A. Fraser, and Cédric T. Albinet. 2019. "An Overview of the Cardiorespiratory Hypothesis and Its Potential Contribution to the Care of Neurodegenerative Disease in Africa" Medicina 55, no. 9: 601. https://doi.org/10.3390/medicina55090601
APA StyleAgbangla, N. F., Fraser, S. A., & Albinet, C. T. (2019). An Overview of the Cardiorespiratory Hypothesis and Its Potential Contribution to the Care of Neurodegenerative Disease in Africa. Medicina, 55(9), 601. https://doi.org/10.3390/medicina55090601