Abstract
One hypothesis that could explain the beneficial effects of physical exercise on cognitive function is the cardiorespiratory hypothesis. This hypothesis proposes that improved cognitive functioning may be in part a result of the physiological processes that occur after physical exercise such as: Increased cerebral perfusion and regional cerebral blood flow. These processes ensure increased oxygenation and glucose transportation to the brain, which together can improve cognitive function. The objective of this narrative review is to examine the contribution of this hypothesis in the care of African older adults with neurodegenerative conditions (i.e., dementia (Alzheimer’s disease)) or with mild cognitive impairments. Although studies in developed countries have examined people of African descent (i.e., with African Americans), only the limited findings presented in this review reflect how these conditions are also important for the African continent. This review revealed that no studies have examined the effects of cardiorespiratory fitness on neurodegenerative disease in Africa. African nations, like many other developing countries, have an aging population that is growing and will face an increased risk of neurodegenerative declines. It is therefore imperative that new research projects be developed to explore the role of the cardiorespiratory fitness in neurodegenerative disease prevention in African nations.
1. Introduction
Africa is considered a continent with a young population. It is estimated that the percentage of people under 25 years will be 59.43% by 2020 [1]. Despite this fact, the number of older adults (>60 years) increases every year according to global health (the World Health Organization; WHO) and the local health promotion/prevention initiatives [2]. For instance, in 2005, the number of people in Africa over 60 years was 53 million and it is expected that this number will reach 200 million in 2050 [3]. While health promotion/prevention initiatives have reduced infectious conditions in low- and middle-income countries, non-communicable diseases (i.e., cardiovascular disease) are on the rise [4]. As a consequence of this, Africa will face important health changes and challenges associated with individuals who are aging in the upcoming decades.
Aging has been defined as the gradual decline of biological functions caused by progressive dysfunction of different cellular systems responsible for repairing and maintaining the homeostasis [5]. This gradual decline, along with other risk factors, can result in the emergence of Mild Cognitive Impairment (MCI; memory decline without pathology) and neurodegenerative pathologies such as dementia and Alzheimer’s disease (AD). The issue of age-related changes and its deleterious effects on cognitive health in Africa is not well documented. The importance of understanding the existing literature and preparing for a population shift in Africa towards older adults cannot be underestimated.
The few studies addressing these issues have focused on determining the risk factors and the prevalence rate of MCI and age-related cognitive pathologies (dementia and AD) [6,7,8,9,10,11,12,13,14]. In the case of MCI, data on prevalence are limited, as only a few studies have been conducted in smaller African countries. The results of these studies have indicated that the prevalence of MCI is 10.4% in rural areas of Benin [6] and 10.8% in Senegal [14]. Risk factors for the development of MCI in these populations are: Poor social network, heart disease, stroke, epilepsy, head trauma, and family history [14]. In addition, other factors such as depression and lack of apolipoprotein ε2 have been highlighted [6]. Regarding dementia, data from several African countries are available. For example, the prevalence of dementia is 8.87% in Senegal [13], 2.6% in rural areas [6] and 3.7% in urban Benin [12], 10.1% in Nigeria [9], 8.1% in the Central African Republic, and 6.7% in the Republic of Congo [7]. Risk factors are gender (women are generally more affected), hypertension, low body mass index (<18.5 Kg/m2), depressive symptoms, and a low level of education [8]. However, a recent study in South Africa found that dementia was not associated with gender nor with education when the age of the participants was controlled [15]. Apart from these main risk factors, other diseases, which are prominent in Africa such as hypertension, diabetes, hypercholesterolemia, and stroke have been shown to contribute to an increase in the prevalence of dementia [15,16].
In summary, the prevalence of dementia in Africa is growing and is moving towards rates seen in developed countries. This prevalence, which seems low in comparison to developed countries, will increase in the coming years because the population is living longer. Indeed, it is predicted that by 2050, 71% of people with dementia will live in low- and middle-income countries [17]. Finally, very little work has been carried out regarding AD in Sub-Saharan Africa. Only risk factors such as age and gender [9], and the presence of apolipoprotein ε4 (APOE ε4) homozygote [10], are well documented. In addition to these studies conducted in Sub-Saharan Africa, other studies have been carried out in North Africa demonstrating that the prevalence increases as a function of age in Egypt going from 2.26% in people over 50 years to 18.48% among people over 80 and over [18]. The presence of APOE ε4 has also been identified as a risk factor in the North African population [19]. The synthesis of these studies confirms that neurodegenerative pathologies linked to aging are present in low rates on the continent. Several factors can explain this low rate such as differential survival rates, unreported cases, and poor access to medical care [20]. In order to manage these age-related diseases, it seems important to develop appropriate strategies. These strategies should integrate several domains including: Medicine, psychology, and sports science.
These findings of cognitive impairment, dementia, and AD are important because physical exercise might be the answer to improving or maintaining cognitive health in this population. Physical exercise remains one of the most robust strategies that contribute to improving the functioning of the brain, helps to prevent cognitive impairment, and reduces the incidence of AD [21]. Findings of a recent meta-analysis demonstrated that low energy expenditure values between 0–2000 Kcal/week or 0–45 Met-h/week were associated with a higher risk of dementia and AD. In contrast, an increase of 500 Kcal/week or 10 Met-h/week of this energy expenditure through leisure activities decreases the risk of dementia and AD by 13% and 10%, respectively [22]. Among the many biological mechanisms underlying this prophylactic effect, an increase in growth factors such as Insulin Growth Factor-1 (IGF-1) and Vascular Endothelial Growth Factor (VEGF) are the most reported [21]. Other mechanisms such as growth of vessels in the hippocampus, the cortex, and the cerebellum, the increased production of nitric oxide (NO) and increased cerebral blood flow and oxygen delivery can help to explain this effect [21]. All these mechanisms are components of an explanatory hypothesis called the cardiorespiratory hypothesis [23]. The cardiorespiratory hypothesis helps explain how these mechanisms may relate to (a) a reduction in cognitive decline and (b) improved cognitive function in an aging population.
The aims of this narrative review are first to present the cardiorespiratory hypothesis. The second aim of this review is to discuss studies examining the effects of cardiorespiratory fitness on MCI, dementia, and Alzheimer’s disease. Finally, we aimed to explore how the cardiorespiratory hypothesis may apply to neurodegenerative diseases in Africa.
2. What Is the Cardiorespiratory Hypothesis?
This hypothesis, which was proposed for the first time by Dustman and collaborators [23], suggests that physical exercise, particularly aerobic exercise, which increases cardiorespiratory fitness, increases cerebral perfusion and regional cerebral blood flow [24]. This induces increased oxygen and glucose transportation to the brain, which results in improved cognitive functioning [25,26]. Several biological mechanisms can underlie this hypothesis. One mechanism is angiogenesis, which is defined as a primary mechanism of formation of new capillaries from existing blood vessels [27]. Beyond the developmental period, the formation of new capillaries in the brain may occur under the influence of the stimulation of physical exercise [28]. Indeed, regular physical exercise can induce the proliferation of a protein called vascular endothelial growth factor (VEGF), which is the main precursor of angiogenesis [24]. However, the peptide hormone insulin-like growth factor one (IGF-1) secreted by the liver also plays an important role in the mechanism of angiogenesis. This peptide hormone promotes the growth of the cerebral blood vessels and influences the regulation of VEGF [29]. Evidence of this angiogenesis mechanism has been supported by the work carried out in animals. In rodents, regular voluntary physical exercise increases angiogenesis in the motor cortex [30], in the dentate gyrus [31], and finally in the cerebellar cortex [32].
In humans, the work of Bullitt and collaborators clarified the role of physical exercise in angiogenesis [33]. The authors investigated cerebral circulation using Magnetic Resonance Angiography (MRA). They observed that active older adults (64 ± 5 years) who do at least 180 min of physical activity per week at a moderate intensity (55–70% of their maximum heart rate) have a larger number of small vessels (diameter less than 0.5 mm) compared to older adults who are sedentary and perform less than 90 min per week of physical exercise [33]. This proliferation of blood vessels could be responsible for the increased regional cerebral blood flow observed following regular physical exercise. For example, using Arterial Spin Labeling and Magnetic Resonance Imaging, researchers studying older adults found that, after four months of aerobic training consisting of walking and stationary cycling (frequency: 2 × 40 min per week; intensity: somewhat hard), there was an increase in blood flow in the hippocampus, an area associated with memory function [34]. Another study demonstrated that an increase in blood flow in the hippocampus correlated positively with delayed logical memory changes after a training program [35]. This finding supports the cardiorespiratory hypothesis such that physical exercise induces an increase in cerebral blood flow, which ensures the availability of metabolic resources (oxygen and glucose) for achieving the best memory performance. However, angiogenesis is not the only mechanism that leads to an increase in cerebral blood flow. Another mechanism associated with cardiorespiratory hypothesis that is likely to play a role is vascular plasticity.
Vascular plasticity can be defined as the ability of the blood vessel to recover its compliance under the effect of a stimulus such as physical exercise. The process by which physical exercise induces better arterial compliance has been investigated by a recent study done in rodents [36]. The authors have shown that in rats, regular physical exercise leads to the bioavailability of nitric oxide (NO), which is an enzyme that plays a vasodilating role. The authors suggest that this bioavailability of NO will inhibit the activity of transglutaminase, which is the main agent of vessel stiffness. This would improve the vasodilator function of blood vessels. In humans, the mechanism of vascular plasticity has been investigated by Tanaka and collaborators with ultrasound imaging and applanation tonometry [37]. Using both devices, the authors have measured the diameter of the arteries and pressure waveform and amplitude. Based on these data, arterial compliance (see [38]) and β stiffness index (see [39]) have been calculated. The authors found, in their cross-sectional study, that older adults who have higher cardiorespiratory fitness have a significantly higher compliance of blood vessels than sedentary older adults. In addition, their study demonstrated that cardiorespiratory fitness correlated positively with compliance of blood vessels (r = 0.44). This positive correlation demonstrates that compliance and cardiorespiratory fitness move in the same direction for older adults. In their second, interventional study, the same authors found that after a 13-week training program, the compliance of blood vessels of older adults increased significantly. The characteristics of this program were: 73% of maximal heart rate (Intensity) for 42 min/day; 5 day/week for 13 weeks. It is clear from this work that improving the compliance of the blood vessels likely contributes to the increase in cerebral blood flow following the practice of physical exercise, partially supporting the cardiorespiratory hypothesis. However, this study did not examine the relationship between increased cerebral blood flow and cognitive performance.
Similar to rodent findings, the increase in blood vessel compliance observed in humans can also be explained by the better availability of NO. The effect of NO on blood vessels in humans is a function of the acute or chronic nature of exercise [40]. Indeed, acute physical exercise induces transient vasodilation of the blood vessel, while chronic physical exercise is associated with remodeling of the blood vessel, which results in increased diameter of the lumen of the blood vessel [38]. In both cases, this leads to a better compliance of the blood vessels and, therefore, allows for an improvement in vascular health. For example, it has been demonstrated that six months of aerobic physical exercise is enough to improve vascular structure and function in African Americans [41]. A systematic review including 21 randomized controlled studies confirmed that aerobic exercise alone or combined with resistance exercises induce significant reductions (standard mean difference of −0.52 ms−1) in the stiffness of the arteries [42]. This has important implications for the maintenance of cognitive function, as stiffness in the arteries contributes to cognitive decline [43].
Finally, the last mechanism associated with the cardiorespiratory hypothesis is the improvement of vascular health. In addition to the impacts of physical exercise on arterial stiffness, exercise can also reduce vascular dysfunctions that can occur with advancing age [44]. Among these dysfunctions, there are atheromatous plaques [45] that promote arterial hypertension and apoptosis of endothelial cells [46]. Aerobic exercise reduces blood pressure by reducing vascular resistance and thus reduces the risk of cardiovascular disease [47], an important contributor to cognitive decline [48]. Moreover, physical exercise can also reduce endothelial cell apoptosis through its positive action on endothelial cell telomerases [49]. All these mechanisms underlying the cardiorespiratory hypothesis are summarized in Figure 1.
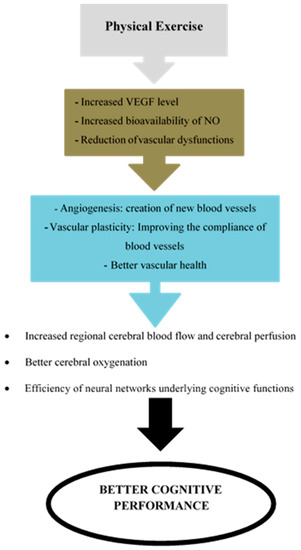
Figure 1.
Main mechanisms of the cardiorespiratory hypothesis. VEGF = Vascular Endothelial Growth Factor; NO = Nitric Oxide.
In addition to aerobic training, other studies have shown the effects of resistance training on the mechanisms underlying the cardiorespiratory hypothesis. For example, recent studies have demonstrated that resistance training increases vascular structure and function [50], vascular endothelial function, and peripheral blood circulation [51] and angiogenesis [52]. However, this effect of resistance training seems to depend on the intensity of training. A recent review demonstrated that in comparison to low intensity training, vigorous resistance training increases arterial stiffness [53]. Despite these effects of resistance training on vascular structure and angiogenesis, studies have supported the neurotrophic hypothesis (and not the cardiorespiratory hypothesis) to explain the prophylactic effects of resistance training on cognitive functions [54,55]. The neurotrophic hypothesis suggests that “endogenous proteins (brain-derived neurotrophic factor, IGF-1, fibroblast growth factor) that support brain plasticity likely mediate the beneficial effects of exercise on the brain” p. 236 [56].
The studies described above, which focused on the explanatory mechanisms of the cardiorespiratory hypothesis, were based on microscopic processes. However, given the complexity of cognitive and cardiorespiratory functions, it is now suggested that the exploration of these mechanisms should be carried out using other approaches, such as the non-linear model (see [57]) or the complex systems methodologies (see [58]). Indeed, biological systems are inherently at diverse hierarchical and heterogeneous multilevel, requiring linking together different types of top-down and bottom-up modeling with various macroscopic and microscopic parameters (see [57]).
3. Cardiorespiratory Hypothesis and Cognitive Decline
Our review revealed that there is no research examining the effect of cardiorespiratory fitness on MCI, dementia, and Alzheimer’s disease in the African continent. However, some relevant cross-sectional and interventional studies with older adults living in industrialised countries exist. The cross-sectional studies examined correlations between cardiorespiratory fitness and other variables such as brain health [59,60,61,62], cognitive function [63], reduced brain atrophy [64], and diminution of amyloid beta (Aβ) related effects on cognition [65]. The main findings of these studies support the cardiorespiratory hypothesis demonstrating that higher levels of cardiorespiratory fitness are associated with preserved cerebral grey matter and white matter, and better cognitive abilities in adults with AD. Further, increasing cardiorespiratory fitness has been associated with reduced brain atrophy and diminution of Aβ in AD [65]. In addition, there is some evidence that patients in the early stages of the disease show low cardiorespiratory fitness compared to non-affected patients [66]. In contrast, higher cardiorespiratory fitness is associated with a low risk of death in AD patients [67]. All these results show that cardiorespiratory fitness may play an important role in the care of AD in any older population.
Apart from these cross-sectional studies, other interventional studies have examined the prophylactic effects of a higher level of cardiorespiratory fitness following aerobic exercise in patients with MCI and AD. In the case of MCI, the results of these studies demonstrate that six-months of high-intensity aerobic exercise improves executive control processes (i.e., planning, inhibiting, and switching) in older women with MCI [68]. Similarly, a 12-week moderate intensity training program improved peak rate of cardiorespiratory fitness and this was associated with widespread increases in cortical thickness in MCI patients [69]. When examining individuals with AD, the results of a pilot exercise intervention study suggests that patients with AD are able to improve their cardiorespiratory fitness [70]. Following this pilot study, two randomized controlled trials demonstrated the positive effect of aerobic exercise on physical performance [71] and functional ability in patients with AD [72]. In addition, cardiorespiratory gains were associated with improved memory performance and reduced hippocampal atrophy [72]. The details of these interventional studies are presented in Table 1. These interventional studies in older adults partially validate the cardiorespiratory hypothesis. Indeed, they show that high cardiorespiratory fitness was associated with an improvement in executive performance [68,72]. In addition, the results show an increase in IGF-1 involved in angiogenesis after aerobic training [68]. However, interventional studies did not examine the links between cardiorespiratory fitness, executive performance, and neurophysiological correlates such as cerebral oxygenation. It seems essential that further research is done in this area in order to fully support the cardiorespiratory hypothesis.

Table 1.
Overview of interventional studies in patients with MCI or AD.
Other studies have investigated the effect of resistance training in patients with cognitive decline and showed mixed results. Some studies have demonstrated improvements in cognition after resistance training without explaining the underlying mechanisms [73,74]. Conversely, another study failed to demonstrate this effect of resistance training [75]. Although resistance training does improve some of the components of the cardiorespiratory hypothesis (angiogenesis (see [52]) and vascular health (see [50,51])), improvements in cognition after resistance training have typically been associated with the neurotrophic hypothesis [54,55]. Therefore, it would be interesting that future studies test the cardiorespiratory hypothesis after a resistance training program.
However, it is worth noting a limitation in relation to the research reviewed in this section. Indeed, whether in cross-sectional or interventional studies, cardiorespiratory fitness was measured with aerobic physiological markers like peak oxygen uptake (VO2peak) or maximal oxygen uptake (VO2max). These physiological markers of cardiorespiratory fitness, which measure metabolic, cardiorespiratory, and pulmonary responses during exercise, provide little information on the coordination between these three subsystems [76]. In order to overcome this problem, recent studies have developed an alternate way of measuring cardiorespiratory function: Cardiorespiratory coordination [76,77]. This approach applies a principal component analysis on several physiological parameters (expired fraction of O2, expired fraction of CO2, ventilation, systolic blood pressure, diastolic blood pressure, and heart rate) measured during an exertion test. The principal component analysis allows for the identification of the component that explains the greatest variation in the physiological parameters included in the analysis [76,77,78]. Thus, the studies reviewed above, which did not use this technique to explore cardiorespiratory function, are unable to provide information on co-variations of the cardiovascular and respiratory systems. As suggested by the authors of references [76,77,79], using the cardiorespiratory coordination approach should be more sensitive to training effects than the traditional aerobic physiological markers, and thus could be advantageously used in cross-sectional and longitudinal protocols. Despite this, its feasibility and validity for use in older populations must be demonstrated first.
4. Future Research Directions
The results of our narrative review revealed that the studies that have investigated the effects of cardiorespiratory fitness on cognitive decline and pathological aging in Africa are non-existent. Similarly, data on African Americans with AD, dementia, or MCI regarding advantageous effects of cardiorespiratory fitness on cognition are also lacking [80]. However, one study conducted among African Americans without AD, dementia, or MCI demonstrated a relationship between poor cardiorespiratory fitness and poor cognitive performance [81]. The lack of studies in the African continent could be explained by the fact that age-related problems are not an immediate priority for decision makers or the African population. Indeed, the current priorities are focused on the problems of young people (unemployment, education). As the proportion of older adults within this population increases along with the number of cases of cognitive decline, this area will become an increasing priority.
In contrast, the ability of cardiorespiratory fitness to influence cognitive performance, physical ability, and brain structure in Caucasians with MCI or AD have been supported in interventional studies (see Table 1). Based on these studies, it is imperative that researchers initiate research projects aimed at replicating the findings reported in this narrative review and to identify, if any, potential specificities related to the relationship between the cardiorespiratory hypothesis and cognitive decline in the African population. As life expectancy increases in Africa and the continent faces higher non-communicable disease rates [16] and increasing incidence of cognitive decline (MCI, dementia, AD), it will be important for researchers to evaluate how the cardiorespiratory hypothesis applies to this population. For example, a longitudinal study could examine the effect of a physical training program on cardiorespiratory fitness parameters and the prevalence and incidence of age-related diseases. Based on the intervention studies reviewed, characteristics of the program could be: (a) Training time per week: Between 60 and 240 min; (b) total duration of the intervention program: For at least six months; (c) frequency: Between three and five sessions; intensity: Should vary from 40% to 85% of Heart Rate Reserve (HRR) if possible [68,69,70,71,72].
One of the interventional studies in our narrative review [72] demonstrates that a physical exercise program can induce an increase in cardiorespiratory fitness that correlates with memory performance in older adults with AD. This effect of physical exercise on memory could be explained by the mechanisms underlying the cardiorespiratory hypothesis, namely angiogenesis and the improvement of vascular plasticity. Another avenue for investigation could, therefore, be exploring the effects of physical exercise on angiogenesis and/or vascular plasticity in the elderly with AD, dementia or MCI in African nations. The objective would be to replicate the effect of physical exercise on angiogenesis and/or vascular plasticity in African older adults with AD, dementia, or MCI. Although data on the effects of cardiorespiratory fitness on aging-related diseases are lacking in Africans, results should be consistent with those observed in Caucasian populations after controlling for other factors (e.g., age, education, etc.).
It is well known that the mechanisms of angiogenesis and vascular plasticity allow the increase of cerebral blood flow and, consequently, the increase in cerebral oxygenation. Another possible direction could be the investigation of the cerebral oxygenation of AD, dementia, and MCI patients following regular physical activity. The cerebral oxygenation of patients could be investigated with cutting edge portable imaging tools such as functional near-infrared spectroscopy (fNIRS). fNIRS is a relatively low-cost optical imaging technique that allows for the investigation of hemodynamic changes associated with brain activity and has been successfully used to examine activations of the cerebral cortex in normal aging [82] and in patients with AD [83]. Moreover, this optical neuroimaging technique has been proved to be sensitive to brain activation differences as a function of cardiorespiratory fitness in older adults [84]. In addition, it has been shown that this tool can be used in the African population to monitor cerebral hemodynamic activity [85,86]. This technique could, therefore, be used to establish additional evidence of the cardiorespiratory hypothesis by measuring the hemodynamic activity of the cerebral cortex before and after a physical exercise program in African older adults with MCI, dementia, or AD.
Finally, following the same rationale as the limitations outlined at the end of Section 2 on the complexity of the biological systems, because the human organism can be seen as an integrated network, a new field of exploration called the network physiology has been developed [87,88]. This field uses a network approach to better understand “how diverse physiological systems and organs coordinate their functions over a broad range of space and time scales and horizontally integrate to generate distinct physiologic states at the organism level” p. 1 [88]. A last potential direction of research could be to explore the nature of the links and whether there are mediating or moderating pathways that exist between the cardiac (heart rate, heart rate variability), respiratory (breathing rate, breathing variability), and central nervous (brain activity, brain variability) systems in patients with neurodegenerative diseases. Subsequently, the effects of physical exercise on the functional connectivity between the three systems could be examined (see [89], chap. III and IV).
5. Conclusions
This review highlights the absence of studies on the effects of cardiorespiratory fitness on cognitive performance in patients with MCI or AD in the African continent. However, there are some studies in industrialized countries on Caucasians and African Americans that highlight the possible beneficial effects of cardiorespiratory fitness on the physical and cognitive performances of older individuals with cognitive decline or pathological aging. Based on these results, we have proposed some potential avenues of research that should be developed for the African continent. Future studies examining these avenues of research could lead to a better strategy for the prevention of MCI, dementia, and AD in Africa prior to a major increase in the older population. To adopt these strategies, it seems essential that the area of geriatric medicine develops and fosters research into the cardiorespiratory hypothesis in aging and disease as an important area of inquiry, as aging is becoming widespread in all the countries of the continent.
Author Contributions
Conceptualization, N.F.A., S.A.F.; writing—original draft preparation, N.F.A., S.A.F., and C.T.A.; writing—review and editing, N.F.A., S.A.F., and C.T.A.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects: The 2017 Revision; UN Department of Economic and Social Affairs: New York, NY, USA, 2017. [Google Scholar]
- Kuate-Defo, B. Facteurs associés à la santé perçue et à la capacité fonctionnelle des personnes âgées dans la préfecture de Bandjoun au Cameroun. Cah. Québécois Démogr. 2005, 34, 1–46. [Google Scholar] [CrossRef]
- Antoine, P. Vieillir en Afrique. Idées Écon. Soc. 2009, 3, 34–37. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Disability 2011; World Health Organization: Geneva, Switzerland, 2011. Available online: https://www.ncbi.nlm.nih.gov/books/NBK304079/ (accessed on 20 June 2019).
- Thorin-Trescases, N.; Voghel, G.; Farhat, N.; Drouin, A.; Gendron, M.E.; Thorin, E. Âge et stress oxydant vers un déséquilibre irréversible de l’homéostasie endothéliale. Méd. Sci. 2010, 26, 875–880. [Google Scholar]
- Guerchet, M.; Houinato, D.; Paraiso, M.N.; von Ahsen, N.; Nubukpo, P.; Otto, M.; Clément, J.-P.; Preux, P.-M.; Dartigues, J.F. Cognitive impairment and dementia in elderly people living in rural Benin, West Africa. Dement. Geriatr. Cogn. Disord. 2009, 27, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Guerchet, M.; M’belesso, P.; Mouanga, A.M.; Bandzouzi, B.; Tabo, A.; Houinato, D.S.; Paraïso, M.N.; Cowppli-Bony, P.; Nubukpo, P.; Aboyans, V.; et al. Prevalence of dementia in elderly living in two cities of Central Africa: The EDAC survey. Dement. Geriatr. Cogn. Disord. 2010, 30, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Guerchet, M.; Mouanga, A.M.; M’belesso, P.; Tabo, A.; Bandzouzi, B.; Paraïso, M.N.; Houinato, D.S.; Cowppli-Bony, P.; Nubukpo, P.; Aboyans, V.; et al. Factors associated with dementia among elderly people living in two cities in Central Africa: The EDAC multicenter study. J. Alzheimer’s Dis. 2012, 29, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Gureje, O.; Ogunniyi, A.; Kola, L. The profile and impact of probable dementia in a sub-Saharan African community: Results from the Ibadan study of ageing. J. Psychosom. Res. 2006, 61, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Hendrie, H.C.; Murrell, J.; Baiyewu, O.; Lane, K.A.; Purnell, C.; Ogunniyi, A.; Unverzagt, F.W.; Hall, K.; Callahan, C.M.; Saykin, A.J.; et al. APOE ε4 and the risk for Alzheimer disease and cognitive decline in African Americans and Yoruba. Int. Psychogeriatr. 2014, 26, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Ogunniyi, A.; Hall, K.S.; Gureje, O.; Baiyewu, O.; Gao, S.; Unverzagt, F.W.; Smith-Gamble, V.; Evans, R.E.; Dickens, J.; Musick, B.S.; et al. Risk factors for incident Alzheimer’s disease in African Americans and Yoruba. Metab. Brain Dis. 2006, 21, 235–240. [Google Scholar] [CrossRef]
- Paraïso, M.N.; Guerchet, M.; Saizonou, J.; Cowppli-Bony, P.; Mouanga, A.M.; Nubukpo, P.; Preux, P.-M.; Houinato, D.S. Prevalence of dementia among elderly people living in Cotonou, an urban area of Benin (West Africa). Neuroepidemiology 2001, 36, 245–251. [Google Scholar] [CrossRef]
- Touré, K.; Coume, M.; Ndiaye, M.; Zunzunegui, M.V.; Bacher, Y.; Diop, A.G.; Ndiaye, M.M. Risk factors for dementia in a Senegalese elderly population aged 65 years and over. Dement. Geriatr. Cogn. Disord. Extra 2012, 2, 160–168. [Google Scholar] [CrossRef]
- Touré, K.; Coume, M.; Ndiaye/Ndongo, N.D.; Basse, A.; Sow, A.; Seck, L.B. Déficit cognitif dans une population de patients âgés sénégalais du centre médico-social et universitaire de l’IPRES, Dakar-Sénégal: Prévalence et facteurs de risque. Rev. Afr. Malgache Rech. Sci. 2013, 1, 55–65. [Google Scholar]
- De Jager, C.A.; Msemburi, W.; Pepper, K.; Combrinck, M.I. Dementia prevalence in a rural region of south Africa: A cross-sectional community study. J. Alzheimer’s Dis. 2017, 60, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- George-Carey, R.; Adeloye, D.; Chan, K.Y.; Paul, A.; Kolčić, I.; Campbell, H.; Rudan, I. An estimate of the prevalence of dementia in Africa: A systematic analysis. J. Glob. Health 2012, 2, 020401. [Google Scholar] [CrossRef] [PubMed]
- Ferri, C.P.; Prince, M.; Brayne, C.; Brodaty, H.; Fratiglioni, L.; Ganguli, M.; Hall, K.; Hasegawa, K.; Hendrie, H.; Huang, Y.; et al. Global prevalence of dementia: A Delphi consensus study. Lancet 2005, 366, 2112–2117. [Google Scholar] [CrossRef]
- El Tallawy, H.N.; Farghly, W.M.; Shehata, G.A.; Rageh, T.A.; Hakeem, N.A.; Abo-Elfetoh, N.; Hegazy, A.M.; Rayan, I.; El-Moselhy, E.A. Prevalence of dementia in Al Kharga District, New Valley Governorate, Egypt. Neuroepidemiology 2012, 38, 130–137. [Google Scholar] [CrossRef]
- Achouri-Rassas, A.; Hadj Fredj, S.; Mrabet Khiari, H.; Bibi, A.; Siala, H.; Mrabet, A.; Messaoud, T. Association between Alzheimer disease and the −491T allele of regulatory region polymorphism of apolipoprotein E in a Tunisian population. Neurochem. Res. 2014, 39, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Ineichen, B. The epidemiology of dementia in Africa: A review. Soc. Sci. Med. 2000, 50, 1673–1677. [Google Scholar] [CrossRef]
- Rolland, Y.; van Kan, G.A.; Vellas, B. Physical activity and Alzheimer’s disease: From prevention to therapeutic perspectives. J. Am. Med. Dir. Assoc. 2008, 9, 390–405. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Wang, H.F.; Wan, Y.; Tan, C.C.; Yu, J.T.; Tan, L. Leisure time physical activity and dementia risk: A dose-response meta-analysis of prospective studies. BMJ Open 2017, 7, e014706. [Google Scholar] [CrossRef]
- Dustman, R.E.; Ruhling, R.O.; Russell, E.M.; Shearer, D.E.; Bonekat, H.W.; Shigeoka, J.W.; Wood, J.S.; Bradford, D.C. Aerobic exercise training and improved neuropsychological function of older individuals. Neurobiol. Aging 1984, 5, 35–42. [Google Scholar] [CrossRef]
- Audiffren, M.; André, N.; Albinet, C.T. Positive effects of chronic physical exercise on cognitive functions in aging people: Assessment and prospects. Rev. Neuropsychol. 2011, 3, 207–225. [Google Scholar] [CrossRef]
- Albinet, C.T.; Mandrick, K.; Bernard, P.L.; Perrey, S.; Blain, H. Improved cerebral oxygenation response and executive performance as a function of cardiorespiratory fitness in older women: A fNIRS study. Front. Aging Neurosci. 2014, 6, 272. [Google Scholar] [CrossRef]
- Marmeleira, J. An examination of the mechanisms underlying the effects of physical activity on brain and cognition: A review with implications for research. Eur. Rev. Aging Phys. Act. 2013, 10, 83–94. [Google Scholar] [CrossRef]
- Schmidt, W.; Endres, M.; Dimeo, F.; Jungehulsing, G.J. Train the vessel, gain the brain: Physical: Physical activity and vessel function and the impact on stroke prevention and outcome in cerebrovascular disease. Cerebrovasc. Dis. 2013, 35, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Voss, M.W.; Vivar, C.; Kramer, A.F.; van Praag, H. Bridging animal and human models of exercise-induced brain plasticity. Trends Cogn. Sci. 2013, 17, 525–544. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Lopez, C.; LeRoith, D.; Torres-Aleman, I. Insulin-like growth factor I is required for vessel remodeling in the adult brain. Proc. Natl. Acad. Sci. USA 2004, 101, 9833–9838. [Google Scholar] [CrossRef] [PubMed]
- Kleim, J.A.; Cooper, N.R.; VandenBerg, P.M. Exercise induces angiogenesis but does not alter movement representations within rat motor cortex. Brain Res. 2002, 934, 1–6. [Google Scholar] [CrossRef]
- Creer, D.J.; Romberg, C.; Saksida, L.M.; van Praag, H.; Bussey, T.J. Running enhances spatial pattern separation in mice. Proc. Natl. Acad. Sci. USA 2010, 107, 2367–2372. [Google Scholar] [CrossRef]
- Black, J.E.; Isaacs, K.R.; Anderson, B.J.; Alcantara, A.A.; Greenough, W.T. Learning causes, synaptogenesis, whereas motor activity causes angiogenesis, in cerebellar cortex of adult rats. Proc. Natl. Acad. Sci. USA 1990, 87, 5568–5572. [Google Scholar] [CrossRef]
- Bullitt, E.; Rahman, F.N.; Smith, J.K.; Kim, E.; Zeng, D.; Katz, L.M.; Marks, B.L. The effect of exercise on the cerebral vasculature of healthy aged subjects as visualized by MR angiography. Am. J. Neuroradiol. 2009, 30, 1857–1863. [Google Scholar] [CrossRef] [PubMed]
- Burdette, J.H.; Laurienti, P.J.; Espeland, M.A.; Morgan, A.; Telesford, Q.; Vechlekar, C.D.; Hayasaka, S.; Jennings, J.M.; Katula, J.A.; Rejeski, W.J.; et al. Using network science to evaluate exercise-associated brain changes in older adults. Front. Aging Neurosci. 2010, 2. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.B.; Aslan, S.; Spence, J.S.; Defina, L.F.; Keebler, M.W.; Didehbani, N. Shorter term aerobic exercise improves brain, cognition, and cardiovascular fitness in aging. Front. Aging Neurosci. 2013, 5, 75. [Google Scholar] [CrossRef] [PubMed]
- Steppan, J.; Sikka, G.; Jandu, S.; Barodka, V.; Halushka, M.K.; Flavahan, N.A.; Belkin, A.M.; Nyhan, D.; Butlin, M.; Santhanam, L.; et al. Exercise, vascular stiffness, and tissue transglutaminase. J. Am. Heart Assoc. 2014, 3, e000599. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Dinenno, F.A.; Monahan, K.D.; Clevenger, C.M.; DeSouza, C.A.; Seals, D.R. Aging, habitual exercise, and dynamic arterial compliance. Circulation 2000, 102, 1270–1275. [Google Scholar] [CrossRef]
- Van Merode, T.; Hick, P.J.; Hoeks, A.P.; Rahn, K.H.; Reneman, R.S. Carotid artery wall properties in normotensive and borderline hypertensive subjects of various ages. Ultrasound Med. Biol. 1988, 14, 563–569. [Google Scholar] [CrossRef]
- Hirai, T.; Sasayama, S.; Kawasaki, T.; Yagi, S. Stiffness of systemic arteries in patients with myocardial infarction. A noninvasive method to predict severity of coronary atherosclerosis. Circulation 1989, 80, 78–86. [Google Scholar] [CrossRef]
- Di Francescomarino, S.; Sciartilli, A.; Di Valerio, V.; Di Baldassarre, A.; Gallina, S. The effect of physical exercise on endothelial function. Sports Med. 2009, 39, 797–812. [Google Scholar] [CrossRef]
- Feairheller, D.L.; Diaz, K.M.; Kashem, M.A.; Thakkar, S.R.; Veerabhadrappa, P.; Sturgeon, K.M.; Williamson, S.T.; Kretzschmar, J.; Lee, H.; Grimm, H.; et al. Effects of moderate aerobic exercise training on vascular health and blood pressure in African Americans. J. Clin. Hypertens. 2014, 16, 504–510. [Google Scholar] [CrossRef]
- Montero, D.; Vinet, A.; Roberts, C.K. Effect of combined aerobic and resistance training versus aerobic training on arterial stiffness. Int. J. Cardiol. 2015, 178, 69–76. [Google Scholar] [CrossRef]
- Hajjar, I.; Goldstein, F.C.; Martin, G.S.; Quyyumi, A.A. Roles of arterial stiffness and blood pressure in hypertension-associated cognitive decline in healthy adults. Hypertension 2016, 67, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Albinet, C.; Fezzani, K.; Thon, B.V. Vieillissement, activité physique et cognition. Mov. Sport Sci. 2008, 63, 9–36. [Google Scholar] [CrossRef]
- Mokdad, A.H.; Marks, J.S.; Stroup, D.F.; Gerberding, J.L. Actual causes of death in the United States, 2000. JAMA 2004, 291, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Barton, M. Aging and endothelin: Determinants of disease. Life Sci. 2014, 118, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Fagard, R.H. Effects of endurance training on blood pressure, blood pressure regulating mechanisms, and cardiovascular risk factors. Hypertension 2005, 46, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Falsetti, L.; Viticchi, G.; Buratti, L.; Grigioni, F.; Capucci, A.; Silvestrini, M. Interactions between atrial fibrillation, cardiovascular risk factors, and ApoE genotype in promoting cognitive decline in patients with Alzheimer’s disease: A prospective cohort study. J. Alzheimer’s Dis. 2018, 62, 713–725. [Google Scholar] [CrossRef] [PubMed]
- Werner, C.; Fürster, T.; Widmann, T.; Pöss, J.; Roggia, C.; Hanhoun, M.; Scharhag, J.; Büchner, N.; Meyer, T.; Kindermann, W.; et al. Physical exercise prevents cellular senescence in circulating leukocytes and in the vessel wall. Circulation 2009, 120, 2438–2447. [Google Scholar] [CrossRef] [PubMed]
- Getty, A.K.; Wisdo, T.R.; Chavis, L.N.; Derella, C.C.; McLaughlin, K.C.; Perez, A.N.; Di Ciurcio, W.T.; Corbin, M.; Feairheller, D.L. Effects of circuit exercise training on vascular health and blood pressure. Prev. Med. Rep. 2018, 10, 106–112. [Google Scholar] [CrossRef]
- Shimizu, R.; Hotta, K.; Yamamoto, S.; Matsumoto, T.; Kamiya, K.; Kato, M.; Hamazaki, N.; Kamekawa, D.; Akiyama, A.; Kamada, Y.; et al. Low-intensity resistance training with blood flow restriction improves vascular endothelial function and peripheral blood circulation in healthy elderly people. Eur. J. Appl. Physiol. 2016, 116, 749–757. [Google Scholar] [CrossRef]
- Holloway, T.M.; Morton, R.W.; Oikawa, S.Y.; McKellar, S.; Baker, S.K.; Phillips, S.M. Microvascular adaptations to resistance training are independent of load in resistance-trained young men. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2018, 315, 267–273. [Google Scholar] [CrossRef]
- Li, Y.; Hanssen, H.; Cordes, M.; Rossmeissl, A.; Endes, S.; Schmidt-Trucksäss, A. Aerobic, resistance and combined exercise training on arterial stiffness in normotensive and hypertensive adults: A review. Eur. J. Sport Sci. 2015, 15, 443–457. [Google Scholar] [CrossRef] [PubMed]
- Herold, F.; Törpel, A.; Schega, L.; Müller, N.G. Functional and/or structural brain changes in response to resistance exercises and resistance training lead to cognitive improvements—A systematic review. Eur. Rev. Aging Phys. Act. 2019, 16, 10. [Google Scholar] [CrossRef] [PubMed]
- Portugal, E.M.; Vasconcelos, P.G.; Souza, R.; Lattari, E.; Monteiro-Junior, R.S.; Machado, S.; Deslandes, A.C. Aging process, cognitive decline and Alzheimer’s disease: Can strength training modulate these responses? CNS Neurol. Disord. Drug Targets 2015, 14, 1209–1213. [Google Scholar] [CrossRef] [PubMed]
- Ploughman, M. Exercise is brain food: The effects of physical activity on cognitive function. Dev. Neurorehabilit. 2008, 11, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Goushcha, A.; Hushcha, T.; Christophorov, L.; Goldsby, M. Self-Organization and Coherency in Biology and Medicine. Open J. Biophys. 2014, 4, 119–146. [Google Scholar] [CrossRef][Green Version]
- Schulz, S.; Adochiei, F.C.; Edu, I.R.; Schroeder, R.; Costin, H.; Bär, K.J.; Voss, A. Cardiovascular and cardiorespiratory coupling analyses: A review. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2013, 371, 20120191. [Google Scholar] [CrossRef]
- Honea, R.; Thomas, G.P.; Harsha, A.; Anderson, H.S.; Donnelly, J.E.; Brooks, W.M.; Burns, J.M. Cardiorespiratory fitness and preserved medial temporal lobe volume in Alzheimer’s Disease. Alzheimer Dis. Assoc. Disord. 2009, 23, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Perea, R.; Vidoni, E.; Morris, J.; Graves, R.; Burns, J.; Honea, R. Cardiorespiratory fitness and white matter integrity in Alzheimer’s disease. Brain Imaging Behav. 2016, 10, 660–668. [Google Scholar] [CrossRef] [PubMed]
- Vidoni, E.D.; Honea, R.A.; Billinger, S.A.; Swerdlow, R.H.; Burns, J.M. Cardiorespiratory fitness is associated with atrophy in Alzheimer’s and aging over two years. Neurobiol. Aging 2012, 33, 1624–1632. [Google Scholar] [CrossRef]
- Vidoni, E.D.; Gayed, M.R.; Honea, R.A.; Savage, C.R.; Hobbs, D.; Burns, J.M. Alzheimer Disease alters the relationship of cardiorespiratory fitness with brain activity during the stroop task. Phys. Ther. 2013, 93, 993–1002. [Google Scholar] [CrossRef]
- Stuckenschneider, T.; Askew, C.D.; Rüdiger, S.; Polidori, M.C.; Abeln, V.; Vogt, T.; Krome, A.; Olde Rikkert, M.; Lawlor, B.; Schneider, S.; et al. Cardiorespiratory fitness and cognitive function are positively related among participants with mild and subjective cognitive impairment. J. Alzheimer’s Dis. 2018, 62, 1865–1875. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.M.; Cronk, B.B.; Anderson, H.S.; Donnelly, J.E.; Thomas, G.P.; Harsha, A.; Brooks, R.H.; Swerdlow, R.H. Cardiorespiratory fitness and brain atrophy in early Alzheimer’s disease. Neurology 2008, 71, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Schultz, S.A.; Boots, E.A.; Almeida, R.P.; Oh, J.M.; Einerson, J.; Korcarz, C.E.; Edwards, D.F.; Koscik, R.L.; Dowling, M.N.; Gallagher, C.L.; et al. Cardiorespiratory fitness attenuates the influence of amyloid on cognition. J. Int. Neuropsychol. Soc. 2015, 21, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Billinger, S.A.; Vidoni, E.D.; Morris, J.K.; Thyfault, J.P.; Burns, J.M. Exercise test performance reveals support of the cardiorespiratory fitness hypothesis. J. Aging Phys. Act. 2017, 25, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Sui, X.; Laditka, J.N.; Church, T.S.; Colabianchi, N.; Hussey, J.; Blair, S.N. Cardiorespiratory fitness as a predictor of dementia mortality in men and women. Med. Sci. Sports Exerc. 2012, 44, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Baker, L.D.; Frank, L.L.; Foster-Schubert, K.; Green, P.S.; Wilkinson, C.W.; McTiernan, A.; Plymate, S.R.; Fishel, M.A.; Watson, G.S.; Cholerton, B.A.; et al. Effects of Aerobic Exercise on Mild Cognitive Impairment: A Controlled Trial. Arch. Neurol. 2010, 67, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Reiter, K.; Nielson, K.A.; Smith, T.J.; Weiss, L.R.; Alfini, A.J.; Smith, J.C. Improved cardiorespiratory fitness is associated with increased cortical thickness in MCI. J. Int. Neuropsychol. Soc. 2015, 21, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Savik, K.; Wyman, J.F.; Bronas, U.G. Maintaining physical fitness and function in Alzheimer’s disease: A pilot study. Am. J. Alzheimer’s Dis. Dement. 2011, 26, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Sobol, N.A.; Hoffmann, K.; Frederiksen, K.S.; Vogel, A.; Vestergaard, K.; Brændgaard, H.; Gottrup, H.; Lolk, A.; Wermuth, L.; Jakobsen, S.; et al. Effect of aerobic exercise on physical performance in patients with Alzheimer’s disease. Alzheimer’s Dement. 2016, 12, 1207–1215. [Google Scholar] [CrossRef]
- Morris, J.K.; Vidoni, E.D.; Johnson, D.K.; Van Sciver, A.; Mahnken, J.D.; Honea, R.A.; Wilkins, H.M.; Brooks, W.M.; Billinger, S.A.; Swerdlow, R.H.; et al. Aerobic exercise for Alzheimer’s disease: A randomized controlled pilot trial. PLoS ONE 2017, 12, e0170547. [Google Scholar] [CrossRef]
- Bossers, W.J.; van der Woude, L.H.; Boersma, F.; Hortobágyi, T.; Scherder, E.J.; van Heuvelen, M.J. A 9-Week Aerobic and Strength Training Program Improves Cognitive and Motor Function in Patients with Dementia: A Randomized, Controlled Trial. Am. J. Geriatr. Psychiatry 2015, 23, 1106–1116. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.C.; Bryan, S.; Marra, C.A.; Sharma, D.; Chan, A.; Beattie, B.L.; Liu-Ambrose, T. An Economic Evaluation of Resistance Training and Aerobic Training versus Balance and Toning Exercises in Older Adults with Mild Cognitive Impairment. PLoS ONE 2013, 8, e63031. [Google Scholar] [CrossRef]
- Vital, T.M.; Hernández, S.S.S.; Pedroso, R.V.; Teixeira, C.V.L.; Garuffi, M.; Stein, A.M.; Costa, J.L.R.; Stella, F. Effects of weight training on cognitive functions in elderly with Alzheimer’s disease. Dement. Neuropsychol. 2012, 6, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Balagué, N.; González, J.; Javierre, C.; Hristovski, R.; Aragonés, D.; Álamo, J.; Ventura, J.L. Cardiorespiratory Coordination after Training and Detraining. A Principal Component Analysis Approach. Front. Physiol. 2016, 7, 35. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Retortillo, S.; Javierre, C.; Hristovski, R.; Ventura, J.L.; Balagué, N. Cardiorespiratory Coordination in Repeated Maximal Exercise. Front. Physiol. 2017, 8, 387. [Google Scholar] [CrossRef] [PubMed]
- Esquius, L.; Garcia-Retortillo, S.; Balagué, N.; Hristovski, R.; Javierre, C. Physiological- and performance-related effects of acute olive oil supplementation at moderate exercise intensity. J. Int. Soc. Sports Nutr. 2019, 16, 12. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Retortillo, S.; Gacto, M.; O’Leary, T.J.; Noon, M.; Hristovski, R.; Balagué, N.; Morris, M.G. Cardiorespiratory coordination reveals training-specific physiological adaptations. Eur. J. Appl. Physiol. 2019, 119, 1701–1709. [Google Scholar] [CrossRef]
- Obisesan, T.O.; Gillum, R.F.; Johnson, S.; Umar, N.; Williams, D.; Bond, V.; Kwagyan, J. Neuroprotection and neurodegeneration in Alzheimers disease: Role of cardiovascular disease risk factors, implications for dementia rates, and prevention with aerobic exercise in African Americans. Int. J. Alzheimer’s Dis. 2012, 2012, 568382. [Google Scholar]
- Izquierdo-Porrera, A.; Waldstein, S. Cardiovascular risk factors and cognitive function in African Americans. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2002, 57, 377–380. [Google Scholar] [CrossRef]
- Agbangla, N.F.; Audiffren, M.; Albinet, C.T. Use of near-infrared spectroscopy in the investigation of brain activation during cognitive aging: A systematic review of an emerging area of research. Ageing Res. Rev. 2017, 38, 52–66. [Google Scholar] [CrossRef]
- Metzger, F.G.; Schopp, B.; Haeussinger, F.B.; Dehnen, K.; Synofzik, M.; Fallgatter, A.J.; Ehlis, A.-C. Brain activation in frontotemporal and Alzheimer’s dementia: A functional near-infrared spectroscopy study. Alzheimer’s Res. Ther. 2016, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Agbangla, N.F.; Audiffren, M.; Pylouster, J.; Albinet, C.T. Working memory, cognitive load and cardiorespiratory fitness: Testing the CRUNCH model with near-infrared spectroscopy. Brain Sci. 2019, 9, 38. [Google Scholar] [CrossRef] [PubMed]
- Blasi, A.; Lloyd-Fox, S.; Johnson, M.H.; Elwell, C. Test-retest reliability of functional near infrared spectroscopy in infants. Neurophotonics 2014, 1, 025005. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Fox, S.; Begus, K.; Halliday, D.; Pirazzoli, L.; Blasi, A.; Papademetriou, M.; Darboe, M.K.; Prentice, A.M.; Johnson, M.H.; Moore, S.E. Cortical specialisation to social stimuli from the first days to the second year of life: A rural Gambian cohort. Dev. Cogn. Neurosci. 2017, 25, 92–104. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, R.P.; Liu, K.K.L.; Bashan, A.; Ivanov, P.C. Network Physiology: How Organ Systems Dynamically Interact. PLoS ONE 2015, 10, e0142143. [Google Scholar] [CrossRef]
- Ivanov, P.C.; Liu, K.K.L.; Bartsch, R.P. Focus on the emerging new fields of Network Physiology and Network Medicine. New J. Phys. 2016, 18, 100201. [Google Scholar] [CrossRef]
- Albinet, C. Habilitation à Diriger des Recherches “Des Effets de l’Exercice Physique Régulier sur les Performances Cognitives des Seniors, à la Recherche de Leurs Marqueurs Neuro-Physiologiques”; Sciences Cognitives; Université de Poitiers: Poitiers, France, 2016. [Google Scholar]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).