Abstract
Background and Objectives: Diet is closely linked to mental health. The aim of this study was to explore the link between diet and mental health in community dwelling Japanese women. Materials and Methods: A total of 89 community dwelling Japanese women, aged 66.8 ± 7.6 years, were enrolled in this cross-sectional study. Diet surveys were evaluated using the brief-type self-administered diet history questionnaire (BDHQ) and mental health was evaluated using the general health questionnaire-12 (GHQ) and clinical parameters. Results: The mean energy intake was 1806 ± 570 kcal and the GHQ score was 1.0 ± 1.4. Among nutrients, the n-6/n-3 fatty acid ratio was significantly correlated with the GHQ score (r = 0.269, p = 0.011), and some micronutrients and vitamins were weakly or negatively correlated with the GHQ score. Among the food groups, fish and shellfish were negatively correlated with the GHQ scores. Multiple regression analysis demonstrated that the n-6/n-3 fatty acid ratio was the determinant factor for the GHQ score, even after adjusting for confounding factors. Conclusions: These results suggest that a proper diet to reduce the n-6/n-3 fatty acid ratio may improve mental health in community dwelling Japanese women.
1. Introduction
Proper management of mental health has become a public health challenge in Japan [,]. Therefore, several strategies to improve mental health, such as minor psychiatric disorders, have been employed in workplaces, schools and communities in Japan [].
It is well known that mental health is affected by lifestyle, such as physical activity [,], cigarette smoking [], alcohol drinking [,], sleep disturbances [,] and diet [,,,,,,,,,,,], as well as by medications [,]. Although there are some reports of the relationship between diet and mental health [,,,,,,,,,,,], evaluation of diet surveys is not accurate or reliable, as expected. In addition, we previously investigated the link between diet and mental health in female university students enrolled in a training course for registered dietitians, who were thought to be more health conscious than average students [], and found that the consumption of confections is associated with mental health []. However, in other ages, accurately and reliably evaluated, the link between diet and mental health remains to be investigated.
Therefore, in this pilot cross-sectional study, we explored the relationship between diet (nutrients and food groups) and mental health in community dwelling Japanese women.
2. Materials and Methods
This is a secondary analysis study. Participants voluntarily took part in the previously reported randomized controlled trial (RCT) of an exercise program who lived around Seto Inland Sea, Western Japan []. The primary outcome was the general health questionnaire-12 (GHQ-12) between the two groups with the difference (0.7) and standard deviation (SD) (1.2) (α = 0.05, β = 0.20, dropout rate = 10%). The sample size of the first study was 120. A total of 89 community dwelling Japanese women (74.1%) among baseline data of 120 men and women, with a mean age of 66.8 ± 7.6 years, who met the following criteria were enrolled in this secondary study (Table 1): (1) they underwent the survey of diet and mental health, and (2) they provided written informed consent.

Table 1.
Characteristics of the enrolled women.
Clinical parameters, such as age, height (cm), body weight (kg), body fat percentage (%), diet and mental health, were examined. Body mass index (BMI) was calculated as follows: Body weight (kg)/[height (m)]2. Body fat percentage (%) was measured using a professional multifrequency body composition meter (MC-180, Tanita Co Ltd., Tokyo, Japan) [].
Diet was evaluated using the brief-type self-administered diet history questionnaire (BDHQ), which can accurately and reliably estimate the intake of nutrients and food groups, as previously described [,,,].
Mental health was evaluated using GHQ-12, which is well prepared and tested with good validity and reliability as previously described [,,,]. This questionnaire is a screening device for identifying minor psychiatric disorders in the general population, and it is a good screener of short-term psychological wellbeing rather than just a unitary screening measure. GHQ-12 scores were determined according to the original method (0-0-1-1) [].
Data were expressed as the mean ± SD. Simple correlation analysis was used to evaluate the relationship between nutrients and the GHQ score, and between food groups and the GHQ score, where p < 0.05 was significant. Multiple linear regression analysis was used to evaluate which factor among the nutrients was important for the GHQ score in community dwelling Japanese women.
Ethical approval was obtained from the ethics committee of Shikoku Gakuin University (Approved number: 2015001, Date: 26 May 2015).
3. Results
The clinical profiles of enrolled women are summarized in Table 1. The mean age, height (cm), body weight (kg), BMI (kg/m2) and body fat percentage (%) were 66.8 ± 7.6 years, 153.6 ± 5.4 cm, 52.8 ± 6.8 kg, 22.4 ± 2.6 kg/m2 and 28.8 ± 6.3%, respectively. The mean GHQ score was 1.0 ± 1.4.
The daily intake of nutrients and food groups is summarized in Table 2 and Table 3. Among the nutrients, the mean energy intake was 1806 ± 570 kcal. Protein, fat and carbohydrate intakes were 81.0 ± 34.0 g, 59.3 ± 22.9 g and 230.3 ± 76.2 g, respectively. The mean n-6/n-3 fatty acid ratio was 3.6 ± 0.8 (Table 2). Among the food groups, the mean intake of fish and shellfish was 109.4 ± 74.8 g (Table 3).
Table 2.
Daily intake of energy and nutrient measured using the BDHQ.
Table 3.
Daily intake of food groups measured using the BDHQ.
We next evaluated the relationship between nutrients and the GHQ score using simple correlation analysis (Table 4). Among the nutrients, the n-6/n-3 fatty acid ratio was significantly and positively correlated with the GHQ scores (r = 0.269, p = 0.011) (Figure 1). Magnesium, calcium, vitamin D, niacin and vitamin B12 were weakly or negatively (r = −0.209~−0.233) correlated with the GHQ score. Among the food groups (Table 5), fish and shellfish were negatively correlated with the GHQ score (r = −0.233, p = 0.027).
Table 4.
Simple correlation analysis between nutrients and GHQ score.
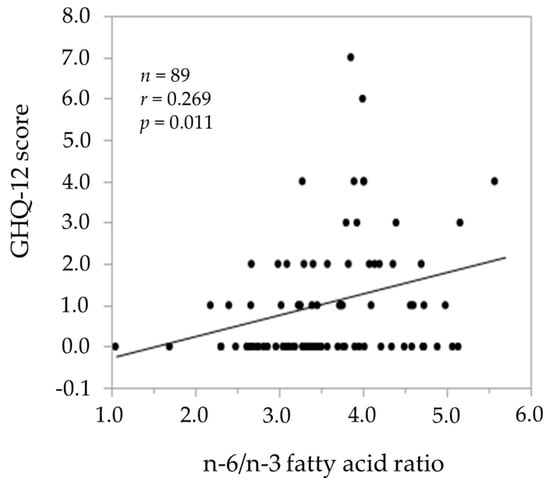
Figure 1.
The relationship between the n-6/n-3 fatty acid ratio and the GHQ-12 score.
Table 5.
Simple correlation analysis between food groups and GHQ score.
Lastly, we examined which nutrients were important for the GHQ score by multiple linear regression analysis (Table 6). We used the GHQ scores as the dependent valuable, and age (years), BMI (kg/m2), n-6/n-3 fatty acid ratio and sucrose (g). The n-6/n-3 fatty acid ratio was statistically significant by simple correlation analysis in our study, and other factors were considered to be clinically important based on our previous study []. As a result, n-6/n-3 fatty acid ratio (β: 0.230, p = 0.049) was found to be a determinant factor for the GHQ scores, even after adjusting for age (years), BMI (kg/m2) and sucrose (g) in community dwelling Japanese women.
Table 6.
Multiple linear regression analysis between clinical parameters and GHQ score.
4. Discussion
There are many reports of the relationship between diet and mental health [,,,,,,,,,,,]. In a cross-sectional study, Miki et al. investigated the relationship between nutrients and mental health using the BDHQ and Center for Epidemiologic Studies Depression Scale (CES-D) in 1792 men and 214 women employees, and found that magnesium, calcium, iron and zinc were associated with depression []. In a cohort study, vitamin D intake was also linked to depression symptoms [] as evaluated by the Burnam scale []. Vitamin B6, B12 and Folate, as evaluated by the Food Frequency Questionnaire (FFQ), were also found to be associated with depressive symptoms in community dwelling older adults []. In the Japan Public Health Center-based prospective Study (JPHC Study), the relationship between fish intake and depression was evaluated by the FFQ [].
Regarding the n-6/n-3 fatty acid ratio, Beydoun et al. previously investigated the link between the n-3/n-6 fatty acid ratio, as evaluated by the 24 h dietary recall method and depressive symptoms in women in a cohort study in the USA, and found that the n-3/n-6 fatty acid ratio was closely associated with depressive symptoms []. Da Rocha et al. also reported the relationship between the n-6/n-3 fatty acid ratio and depression in pregnancy using the FFQ []. Miyake et al. found that fish intake, but not n-6/n3 fatty acid ratio, was associated with depressive symptoms during pregnancy []. On the other hand, Murakami et al. reported in their review that no association was found between dietary variables and depressive symptoms, because of the unreliable or rough assessment of diet or depressive symptoms [].
In this pilot study, the intake of fish and shellfish was 109.4 ± 74.8 g. We noted the consumption of fish and shellfish was higher than that of the National Nutrition Survey (2016: 60.3 ± 57.4 g) [], and it showed a significant relationship between nutrients and food groups, as in previous studies, especially the n-6/n-3 fatty acid ratio, and the GHQ scores in community dwelling Japanese women. We used the BDHQ, which is an accurate and reliable method for evaluating nutrients and food groups [,,]. Based on the multiple regression analysis, the n-6/n-3 fatty acid ratio is a determinant factor for the GHQ score, even after adjusting for confounding factors. Eating n-3 fatty acids improved the symptoms of attention deficit hyperactivity disorder (ADHD) patients [], and also improved anxiety symptoms in medical students [] and depressed adult outpatients [] by RCT. In Japan, the mean consumption of n-6 and n-3 fatty acids are 9.6 g/day and 2.1 g/day [], respectively and the recommended n-6/n-3 fatty acid ratio is 4 by the Ministry of Health, Labour and Welfare, Japan []. Taken together, we recommend reducing the n-6/n-3 fatty acid intake by eating fish and shellfish to improve the mental health of community dwelling Japanese women in clinical practice.
This study has several potential limitations. First, this was a secondary cross-sectional study with small samples. Second, the voluntarily enrolled women were considered to be more health conscious than the average subjects. Third, we were unable to evaluate the relationship between diet and mental health in men because of a small sample in the first study. Fourth, we could not obtain details of sociodemographic characteristics such as educational level, socioeconomic status, marital status, the number of people living in the household with the study subjects, and medical history to adjust the relationship between diet and mental health. However, diet is thought to be a modifiable risk factor contributing to an individual’s mental health and, in combination with other interventions of an individual’s lifestyle factors, may be the main current approach for preventing and improving mental health. Fifth, the mechanism of the correlation between n-6/n-3 fatty acid ratio and the GHQ score was not evaluated. However, a proper diet, which includes an improved n-6/n-3 fatty acid ratio by eating fish and shellfish, may improve the mental health of community dwelling Japanese women. Further prospective and intervention studies are required in the future.
5. Conclusions
In this pilot cross-sectional study, we evaluated the link between diet and mental health in community dwelling Japanese women, and we found that some nutrients and food groups, especially the n-6/n-3 fatty acid ratio, were closely associated with the GHQ score.
Author Contributions
Conceptualization, N.T. and H.S.; methodology, N.T., A.K. and K.D.M.; software, H.S. and S.H.; validation, S.H.; formal analysis, N.T.; investigation, A.K. and K.D.M.; resources, A.K. and K.D.M.; data curation, N.T. and S.H.; writing—original draft preparation, N.T.; writing—review and editing, all authors; visualization, all authors; supervision, N.M.; project administration, N.M.; funding acquisition, A.K.
Funding
This research was supported in part by a research grant from the Ministry of Education, Culture, Sports, Science and Technology, Japan (JSPS KAKENHI Grant Number JP 15K12716).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ministry of Health, Labor and Welfare, Japan. Health Japan 21. Rest, Mental Health. Available online: https://www.mhlw.go.jp/www1/topics/kenko21_11/b3.html#A33 (accessed on 29 July 2019). (In Japanese)
- Welfare Labor White Paper. Mental Health for Everyone. 2014. Available online: https//.mhlw.go.jp/wp/hakusyo/kousei/14/dl/1-02-1.pdf (accessed on 29 July 2019). (In Japanese)
- Ministry of Health, Labor and Welfare, Japan. Everyone’s Mental Health Integrated Site, National Policy and Directionality. 2019. Available online: https://www.mhlw.go.jp/kokoro/nation/index.html (accessed on 29 July 2019). (In Japanese)
- Lubans, D.; Richards, J.; Hillman, C.; Faulkner, G.; Beauchamp, M.; Nilsson, M.; Kelly, P.; Smith, J.; Rain, L.; Biddle, S. Physical activity for cognitive and mental health in youth: A systematic review of mechanisms. Pediatrics 2016, 138, e20161642. [Google Scholar] [CrossRef] [PubMed]
- Conn, V.S. Anxiety outcomes after physical activity interventions: Meta-analysis findings. Nurs. Res. 2010, 59, 224–231. [Google Scholar] [CrossRef]
- Taylor, G.; McNeill, A.; Girling, A.; Farley, A.; Lindson-Hawley, N.; Aveyard, P. Change in mental health after smoking cessation: Systematic review and meta-analysis. BMJ 2014, 348, g1151. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Tao, R.; He, C.; Liu, S.; Wang, Y.; Zhang, X. The risk factors of the alcohol use disorders—Through review of its comorbidities. Front. Neurosci. 2018, 12, 303. [Google Scholar] [CrossRef]
- Berglund, M.; Ojehagen, A. The influence of alcohol drinking and alcohol use disorders on psychiatric disorders and suicidal behavior. Alcohol. Clin. Exp. Res. 1998, 22, 333S–345S. [Google Scholar] [CrossRef]
- Sutton, E.L. Psychiatric disorders and sleep issues. Med. Clin. N. Am. 2014, 98, 1123–1143. [Google Scholar] [CrossRef] [PubMed]
- Owens, J. Adolescent Sleep Working Group, Committee on Adolescence. Insufficient sleep in adolescents and young adults: An update on causes and consequences. Pediatrics 2014, 134, e921–e932. [Google Scholar] [CrossRef]
- Miki, T.; Kochi, T.; Eguchi, M.; Kuwahara, K.; Kurotani, K.; Tsuruoka, H.; Ito, R.; Akter, S.; Kashino, I.; Pham, N.M.; et al. Dietary intake of minerals in relation to depressive symptoms in Japanese employees: The Furukawa Nutrition and Health Study. Nutrition 2015, 31, 686–690. [Google Scholar] [CrossRef]
- Bertone-Johnson, E.R.; Powers, S.I.; Spangler, L.; Brunner, R.L.; Michael, Y.L.; Larson, J.C.; Millen, A.E.; Bueche, M.N.; Salmoirago-Blotcher, E.; Liu, S.; et al. Vitamin D intake from foods and supplements and depressive symptoms in a diverse population of older women. Am. J. Clin. Nutr. 2011, 94, 1104–1112. [Google Scholar] [CrossRef]
- Burnam, M.A.; Wells, K.B.; Leake, B.; Landsverk, J. Development of a brief screening instrument for detecting depressive disorders. Med. Care 1988, 26, 775–789. [Google Scholar] [CrossRef]
- Skarupski, K.A.; Tangney, C.; Li, H.; Ouyang, B.; Evans, D.A.; Morris, M.C. Longitudinal association of vitamin B-6, folate, and vitamin B-12 with depressive symptoms among older adults over time. Am. J. Clin. Nutr. 2010, 92, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, Y.J.; Sawada, N.; Mimura, M.; Shikimoto, R.; Nozaki, S.; Hamazaki, K.; Uchitomi, Y.; Tsugane, S. Dietary fish, n-3 polyunsaturated fatty acid consumption, and depression risk in Japan: A population-based prospective cohort study. Transl. Psychiatry 2017, 7, e1242. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, M.A.; Fanelli Kuczmarski, M.T.; Beydoun, H.A.; Hibbeln, J.R.; Evans, M.K.; Zonderman, A.B. ω-3 fatty acid intakes are inversely related to elevated depressive symptoms among United States women. J. Nutr. 2013, 143, 1743–1752. [Google Scholar] [CrossRef] [PubMed]
- Da Rocha, C.M.M.; Kac, G. High dietary ratio of omega-6 to omega-3 polyunsaturated acids during pregnancy and prevalence of post-partum depression: Omega dietary intake and post-partum depression. Matern. Child Nutr. 2012, 8, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Miyake, Y.; Tanaka, K.; Okubo, H.; Sasaki, S.; Arakawa, M. Fish and fat intake and prevalence of depressive symptoms during pregnancy in Japan: Baseline data from the Kyushu Okinawa Maternal and Child Health Study. J. Psychiatr. Res. 2013, 47, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Sasaki, S. Dietary intake and depressive symptoms: A systematic review of observational studies. Mol. Nutr. Food Res. 2010, 54, 471–488. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.; Månsson, J.-E.; Östlund, S.; Fransson, G.; Areskoug, B.; Hjalmarsson, K.; Landgren, M.; Kadesjö, B.; Gillberg, C. Fatty acids in ADHD: Plasma profiles in a placebo-controlled study of Omega 3/6 fatty acids in children and adolescents. Atten. Defic. Hyperact. Disord. 2012, 4, 199–204. [Google Scholar] [CrossRef]
- Kiecolt-Glaser, J.K.; Belury, M.A.; Andridge, R.; Malarkey, W.B.; Glaser, R. Omega-3 supplementation lowers inflammation and anxiety in medical students: A randomized controlled trial. Brain Behav. Immun. 2011, 25, 1725–1734. [Google Scholar] [CrossRef]
- Mischoulon, D.; Best-Popescu, C.; Laposata, M.; Merens, W.; Murakami, J.L.; Wu, S.L.; Papakostas, G.I.; Dording, C.M.; Sonawalla, S.B.; Nierenberg, A.A.; et al. A double-blind dose-finding pilot study of docosahexaenoic acid (DHA) for major depressive disorder. Eur. Neuropsychopharmacol. 2008, 18, 639–645. [Google Scholar] [CrossRef]
- Kodish, I.; Rockhill, C.; Varley, C. Pharmacotherapy for anxiety disorders in children and adolescents. Dialogues Clin. Neurosci. 2011, 13, 439–452. [Google Scholar] [CrossRef]
- Nieuwsma, J.A.; Williams, J.W., Jr.; Namdari, N.; Washam, J.B.; Raitz, G.; Blumenthal, J.A.; Jiang, W.; Yapa, R.; McBroom, A.J.; Lallinger, K.; et al. Diagnostic accuracy of screening tests and treatment for post–acute coronary syndrome depression: A systematic review. Ann. Intern. Med. 2017, 167, 725–735. [Google Scholar] [CrossRef]
- Mochimasu, K.D.; Miyatake, N.; Hase, A. A pilot study of the relationship between diet and mental health in female university students enrolled in a training course for registered dietitians. Environ. Health Prev. Med. 2016, 21, 345–349. [Google Scholar] [CrossRef][Green Version]
- Katayama, A.; Miyatake, N.; Uchida, H. A Randomized Controlled Trial of the Effect of Exercise Program in Community Dwelling Elderly People. Abstract of the 20th of Annual Meeting of Japanese Association of Exercise Epidemiology.50, 2017. Available online: http://jaee.umin.jp/doc/meeting_20_presentation.pdf (accessed on 14 April 2019).
- Wang, Z.H.; Yang, Z.P.; Wang, X.J.; Dong, Y.H.; Ma, J. Comparative analysis of the multi-frequency bio-impedance and dual-energy X-ray absorptiometry on body composition in obese subjects. Biomed. Environ. Sci. 2018, 31, 72–75. [Google Scholar]
- Okubo, H.; Sasaki, S.; Rafamantanantsoa, H.H.; Ishikawa-Takata, K.; Okazaki, H.; Tabata, I. Validation of self-reported energy intake by a self-administered diet history questionnaire using the doubly labeled water method in 140 Japanese adults. Eur. J. Clin. Nutr. 2008, 62, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Ushio, F.; Amano, K.; Morihara, M.; Todoriki, T.; Uehara, Y.; Toyooka, T. Serum biomarker-based validation of a self-administered diet history questionnaire for Japanese subjects. J. Nutr. Sci. Vitaminol. 2000, 46, 285–296. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Yanagibori, R.; Amano, K. Self-administered diet history questionnaire developed for health education: A relative validation of the test-version by comparison with 3-day diet record in women. J. Epidemiol. 1998, 8, 203–215. [Google Scholar] [CrossRef] [PubMed]
- EBNJAPAN DHQ Support Centre. Available online: http://www.ebnjapan.org (accessed on 29 July 2019.). (In Japanese).
- Goldberg, D.P.; Hillier, V.F. A scaled version of the General Health Questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Bazazan, A.; Dianat, I.; Rastgoo, L.; Zandi, H. Relationships between dimensions of fatigue and psychological distress among public hospital nurses. Health Promot. Perspect. 2018, 8, 195–199. [Google Scholar] [CrossRef]
- Doi, Y.; Minowa, M. Factor structure of the 12-item General Health Questionnaire in the Japanese general adult population. Psychiatry Clin. Neurosci. 2003, 57, 379–383. [Google Scholar] [CrossRef]
- Goldberg, D.; Williams, P. A User’s Guide to the General Health Questionnaire; Nfer-Nelson: London, UK, 1988. [Google Scholar]
- National Health and Nutrition Survey in Japan in 2016. 2016. Available online: https://www.mhlw.go.jp/bunya/kenkou/eiyou/dl/h28-houkoku.pdf (accessed on 14 April 2019). (In Japanese)
- Ministry of Health, Labor and Welfare Public Health Council Report. Nutritional Requirement of the 6th Revised Version in Japan. 1999. Available online: https://www.mhlw.go.jp/www1/shingi/s9906/s0628-1_11.html (accessed on 14 April 2019). (In Japanese)
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).