Association between Sports Participation in Early Life and Arterial Intima-Media Thickness among Adults

 , ,
, , 
Abstract
1. Background
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef]
- Kim, E.S.H.; Marycz, D.M.; Archinal, D.; Gornik, H.L.; Shishehbor, M.H.; Bartholomew, J.R. Presence of external carotid artery plaque independently predicts mortality in patients without internal carotid artery atherosclerosis. Vasc. Med. 2014, 19, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.W.; Von Kegler, S.; Steinmetz, H.; Markus, H.S.; Sitzer, M. Carotid intima-media thickening indicates a higher vascular risk across a wide age range: Prospective data from the Carotid Atherosclerosis Progression Study (CAPS). Stroke 2006, 37, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Plichart, M.; Celermajer, D.S.; Zureik, M.; Helmer, C.; Jouven, X.; Ritchie, K.; Tzourio, C.; Ducimetière, P.; Empana, J.P. Carotid intima-media thickness in plaque-free site, carotid plaques and coronary heart disease risk prediction in older adults. The Three-City Study. Atherosclerosis 2011, 219, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.J.; Arnold, A.M.; Manolio, T.A.; Polak, J.F.; Psaty, B.M.; Hirsch, C.H.; Kuller, L.H.; Cushman, M. Association of carotid artery intima-media thickness, plaques, and C-reactive protein with future cardiovascular disease and all-cause mortality: The Cardiovascular Health Study. Circulation 2007, 116, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Matthews, C.E.; Dunstan, D.W.; Winkler, E.A.H.; Owen, N. Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 2003–06. Eur. Heart J. 2011, 32, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Cayres, S.U.; Agostinete, R.R.; de Moura Mello Antunes, B.; Lira, F.S.; Fernandes, R.A. Impact of physical exercise/activity on vascular structure and inflammation in pediatric populations: A literature review. J. Spec. Pediatr. Nurs. 2016, 21, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Cayres, S.U.; Júnior, I.F.F.; Barbosa, M.F.; Christofaro, D.G.D.; Fernandes, R.A. Breakfast frequency, adiposity, and cardiovascular risk factors as markers in adolescents. Cardiol. Young 2016, 26, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Boss, H.M.; van der Graaf, Y.; Visseren, F.L.J.; Van den Berg-Vos, R.M.; Bots, M.L.; de Borst, G.J.; Cramer, M.J.; Kappelle, L.J.; Geerlings, M.I. Physical Activity and Characteristics of the Carotid Artery Wall in High-Risk Patients—The SMART (Second Manifestations of Arterial Disease) Study. J. Am. Heart Assoc. 2017, 6, e005143. [Google Scholar] [CrossRef] [PubMed]
- Paffenbarger, R.S.; Hyde, R.; Wing, A.L.; Hsieh, C. Physical activity, all-cause mortality, and longevity of college alumni. N. Engl. J. Med. 1986, 314, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Hallal, P.C.; Victora, C.G.; Azevedo, M.R.; Wells, J.C.K. Adolescent physical activity and health. Sports Med. 2006, 36, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, R.A.; Coelho-E-Silva, M.J.; Spiguel Lima, M.C.; Cayres, S.U.; Codogno, J.S.; Lira, F.S. Possible underestimation by sports medicine of the effects of early physical exercise practice on the prevention of diseases in adulthood. Curr. Diabetes Rev. 2015, 11, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Pälve, K.S.; Pahkala, K.; Magnussen, C.G.; Koivistoinen, T.; Juonala, M.; Kähönen, M.; Lehtimäki, T.; Rönnemaa, T.; Viikari, J.S.; Raitakari, O.T. Association of physical activity in childhood and early adulthood with carotid artery elasticity 21 years later: The cardiovascular risk in Young Finns Study. J. Am. Heart Assoc. 2014, 3, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Guan, Y.; Yu, C.; Shi, M.; Ni, J.; Wu, Y.; Gu, H.; Bai, L.; Liu, J.; Tu, J.; Wang, J.; et al. The association between elevated fasting plasma glucose levels and carotid intima-media thickness in non-diabetic adults: A population-based cross-sectional study. Oncotarget 2017, 8, 111053–111063. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.H.; Lotufo, P.A.; Fujita, A.; Goulart, A.C.; Chor, D.; Mill, J.G.; Bensenor, I.M.; Santos, I.S. Association between short-term systolic blood pressure variability and carotid intima-media thickness in ELSA-Brasil baseline. Am. J. Hypertens. 2017, 30, 954–960. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.A.; Ebrahim, S.; Whincup, P.; Sterne, J.; Papacosta, O.; Wannamethee, G.; Dhanjil, S.; Griffin, M.; Nicolaides, A.N.; Davey Smith, G. Sex differences in body fat distribution and carotid intima media thickness: Cross sectional survey using data from the British regional heart study. J. Epidemiol. Community Health 2004, 58, 700–704. [Google Scholar] [CrossRef] [PubMed]
- Lima, M.C.S.; Cayres, S.U.; Machado-Rodrigues, A.; Coelho-e-Silva, M.J.; Kemper, H.C.G.; Fernandes, R.A. Early sport practice promotes better metabolic profile independently of current physical activity. Med. Sport 2014, 18, 172–178. [Google Scholar] [CrossRef]
- Fernandes, R.A.; Zanesco, A. Early physical activity promotes lower prevalence of chronic diseases in adulthood. Hypertens. Res. 2010, 33, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Sociedade Brasileira de Cardiologia. Normatização dos equipamentos e das técnicas para a realizaçã de exames de ultra-sonografia vascular. Arquivos Brasileiros de Cardiologia 2004, 82, S1–S14. [Google Scholar] [CrossRef]
- Sociedade Brasileira de Cardiologia. VI Brazilian guidelines on hypertension. Arquivos Brasileiros de Cardiologia 2010, 95, 1–51. [Google Scholar]
- Meng, C.; Sun, M.; Wang, Z.; Fu, Q.; Cao, M.; Zhu, Z.; Mao, J.; Shi, Y.; Tang, W.; Huang, X.; et al. Insulin sensitivity and beta-cell function are associated with arterial stiffness in individuals without hypertension. J. Diabetes Res. 2013, 2013, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Shoji, T.; Maekawa, K.; Emoto, M.; Okuno, S.; Yamakawa, T.; Ishimura, E.; Inaba, M.; Nishizawa, Y. Arterial stiffness predicts cardiovascular death independent of arterial thickness in a cohort of hemodialysis patients. Atherosclerosis 2010, 210, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Raitakari, O.T.; Juonala, M.; Kähönen, M.; Taittonen, L.; Laitinen, T.; Mäki-Torkko, N.; Järvisalo, M.J.; Uhari, M.; Jokinen, E.; Rönnemaa, T.; et al. Cardiovascular risk factors in childhood and carotid artery intima-media thickness in adulthood: The Cardiovascular Risk in Young Finns Study. JAMA 2003, 290, 2277–2283. [Google Scholar] [CrossRef] [PubMed]
- Cayres, S.U.; Lira, F.S.; Kemper, H.C.G.; Codogno, J.S.; Barbosa, M.F.; Fernandes, R.A. Sport-based physical activity recommendations and modifications in C-reactive protein and arterial thickness. Eur. J. Pediatr. 2018, 177, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Boreham, C.A.G.; McKay, H.A. Physical activity in childhood and bone health. Br. J. Sports Med. 2011, 45, 877–879. [Google Scholar] [CrossRef] [PubMed]
- White, A.J.; Sandler, D.P.; Bolick, S.C.E.; Xu, Z.; Taylor, J.A.; DeRoo, L.A. Recreational and household physical activity at different time points and DNA global methylation. Eur. J. Cancer 2013, 49, 2199–2206. [Google Scholar] [CrossRef] [PubMed]
- Van De Laar, R.J.; Ferreira, I.; Van Mechelen, W.; Prins, M.H.; Twisk, J.W.; Stehouwer, C.D. Lifetime vigorous but not light-to-moderate habitual physical activity impacts favorably on carotid stiffness in young adults: The amsterdam growth and health longitudinal study. Hypertension 2010, 55, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Boaz, M.; Chernin, G.; Schwartz, I.; Katzir, Z.; Schwartz, D.; Agbaria, A.; Gal-Oz, A.; Weinstein, T. C-reactive protein and carotid and femoral intima media thickness: Predicting inflammation. Clin. Nephrol. 2013, 80, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Lipert, A.; Jegier, A. Comparison of different physical activity measurement methods in adults aged 45 to 64 years under free-living conditions. Clin. J. Sport Med. 2017, 27, 400–408. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Early Sports Practice (n = 52) | No early Sports Practice (n = 55) | p-Value |
|---|---|---|---|
| Chronological age (years) | 39.8 (29.7–50.5) | 37.4 (29.6–53.7) | 0.609 |
| Body Mass (kg) | 77.3 (45.9–103.1) | 80.6 (51.4–137.3) | 0.035 |
| Stature (cm) | 175.1 (150.1–195.0) | 170.5 (148.6–188.0) | 0.013 |
| BMI (kg/m2) | 24.3 (19.6–32.3) | 28.1 (18.8–38.9) | <0.001 |
| Body fat (%) | 23.9 (7.9–50.0) | 36.8 (20.1–57.8) | <0.001 |
| Systolic blood pressure (mmHg) | 110.0 (90.0–140.0) | 120.0 (80.0–140.0) | 0.141 |
| Diastolic blood pressure (mmHg) | 80.0 (60.0–90.0) | 80.0 (60.0–90.0) | 0.072 |
| Mean blood pressure (score) | 90.0 (71.7–108.3) | 93.3 (66.7–106.7) | 0.073 |
| C-reactive protein (mg/dL) | 0.87 (0.15–18.65) | 2.49 (0.29–16.45) | <0.001 |
| HOMA (score) | 0.91 (0.21–3.21) | 1.53 (0.51–8.40) | <0.001 |
| Carotid intima-media thickness (mm) | 0.57 (0.42–0.98) | 0.65 (0.47–1.70) | 0.057 |
| Femoral intima-media thickness (mm) | 0.49 (0.35–0.82) | 0.55 (0.34–1.85) | 0.095 |
| Carotid resistive index (score) | 0.79 (0.62–0.87) | 0.76 (0.56–0.88) | 0.022 |
| Femoral resistive index (score) | 0.85 (0.73–0.93) | 0.86 (0.74–0.94) | 0.499 |
| Mean number of steps (n) | 10,107 (4532–21,740) | 6394 (1517–16,354) | <0.001 |
| Tobacco smoking (%) | 5.5 | 0 | 0.089 |
| Alcohol drinking (%) | 20 | 30.8 | 0.542 |
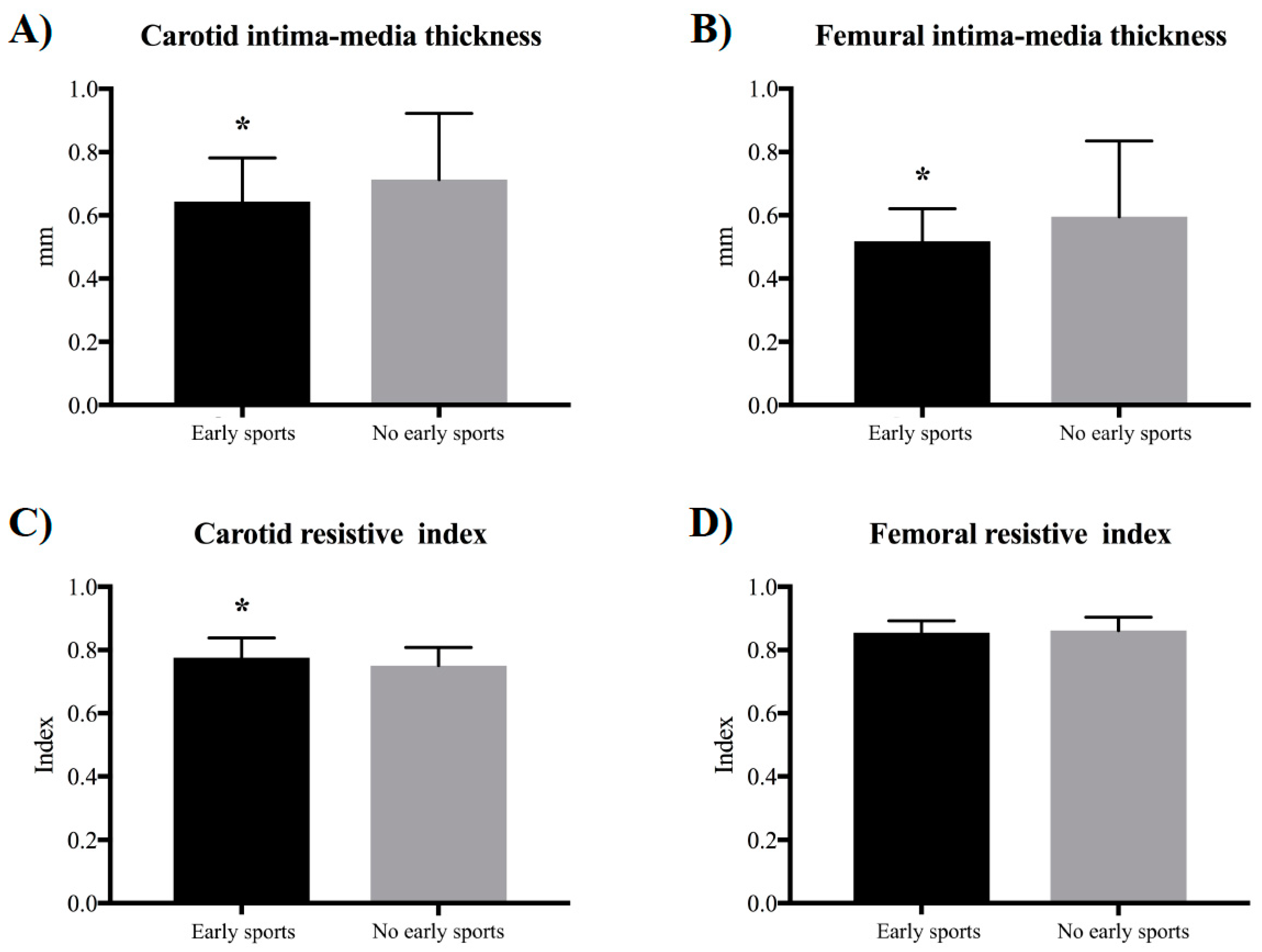
| Sports Participation in Early Life | No Early Sports Participation | Wald | p | r | R2 | |
|---|---|---|---|---|---|---|
| Carotid intima-media thickness (mm) | 0.64 ± 0.14 | 0.71 ± 0.21 | 6.54 | 0.011 | −0.231 | 0.053 |
| Femoral intima-media thickness (mm) | 0.52 ± 0.10 | 0.60 ± 0.24 | 2.47 | 0.116 | −0.119 | 0.014 |
| Carotid resistive index (score) | 0.78 ± 0.06 | 0.75 ± 0.06 | 0.40 | 0.529 | 0.053 | 0.003 |
| Femoral resistive index (score) | 0.85 ± 0.04 | 0.86 ± 0.04 | 3.18 | 0.075 | −0.189 | 0.036 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Werneck, A.O.; Lima, M.C.S.; Agostinete, R.R.; Silva, D.R.; Turi-Lynch, B.C.; Codogno, J.S.; Fernandes, R.A. Association between Sports Participation in Early Life and Arterial Intima-Media Thickness among Adults. Medicina 2018, 54, 85. https://doi.org/10.3390/medicina54050085
Werneck AO, Lima MCS, Agostinete RR, Silva DR, Turi-Lynch BC, Codogno JS, Fernandes RA. Association between Sports Participation in Early Life and Arterial Intima-Media Thickness among Adults. Medicina. 2018; 54(5):85. https://doi.org/10.3390/medicina54050085
Chicago/Turabian StyleWerneck, André O., Manoel C. S. Lima, Ricardo R. Agostinete, Danilo R. Silva, Bruna C. Turi-Lynch, Jamile S. Codogno, and Rômulo A. Fernandes. 2018. "Association between Sports Participation in Early Life and Arterial Intima-Media Thickness among Adults" Medicina 54, no. 5: 85. https://doi.org/10.3390/medicina54050085
APA StyleWerneck, A. O., Lima, M. C. S., Agostinete, R. R., Silva, D. R., Turi-Lynch, B. C., Codogno, J. S., & Fernandes, R. A. (2018). Association between Sports Participation in Early Life and Arterial Intima-Media Thickness among Adults. Medicina, 54(5), 85. https://doi.org/10.3390/medicina54050085