
Effect of Lactobacillus reuteri on Gingival Inflammation and Composition of the Oral Microbiota in Patients Undergoing Treatment with Fixed Orthodontic Appliances: Study Protocol of a Randomized Control Trial

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Method
2.1. Research Hypothesis and Objectives
2.1.1. Primary Objective
2.1.2. Secondary Objectives
- Gingival index at 6 months (i.e., 3 months after cessation of the lozenges intake).
- Extent and severity of gingivitis (at 3 and 6 months).
- Plaque accumulation on dental surfaces (at 3 and 6 months).
- Relative abundance of bacterial taxa at the phylum level in the supra and sub gingival microbiota (at 3 and 6 months).
- Level of salivary biomarkers of inflammation (at 3 and 6 months).
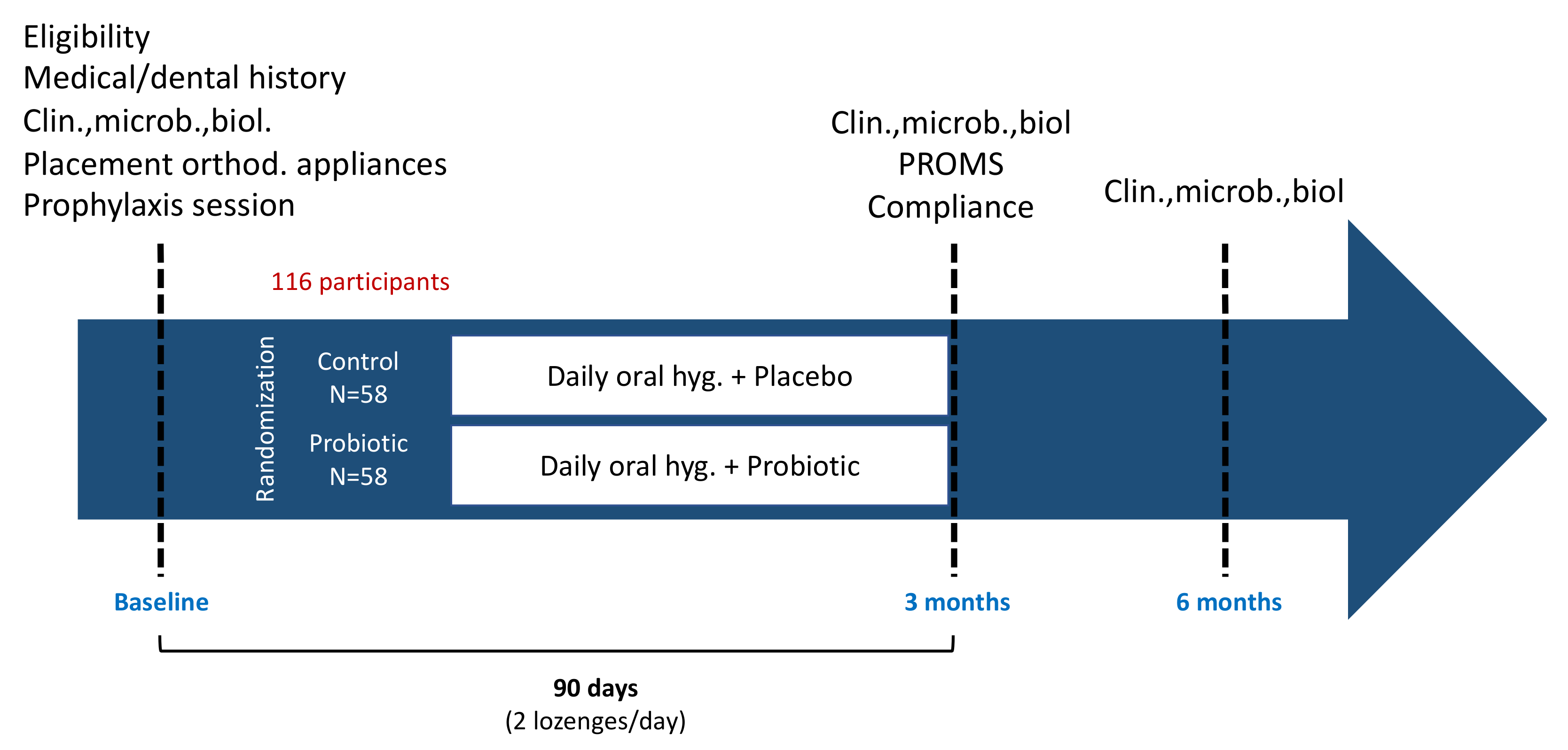
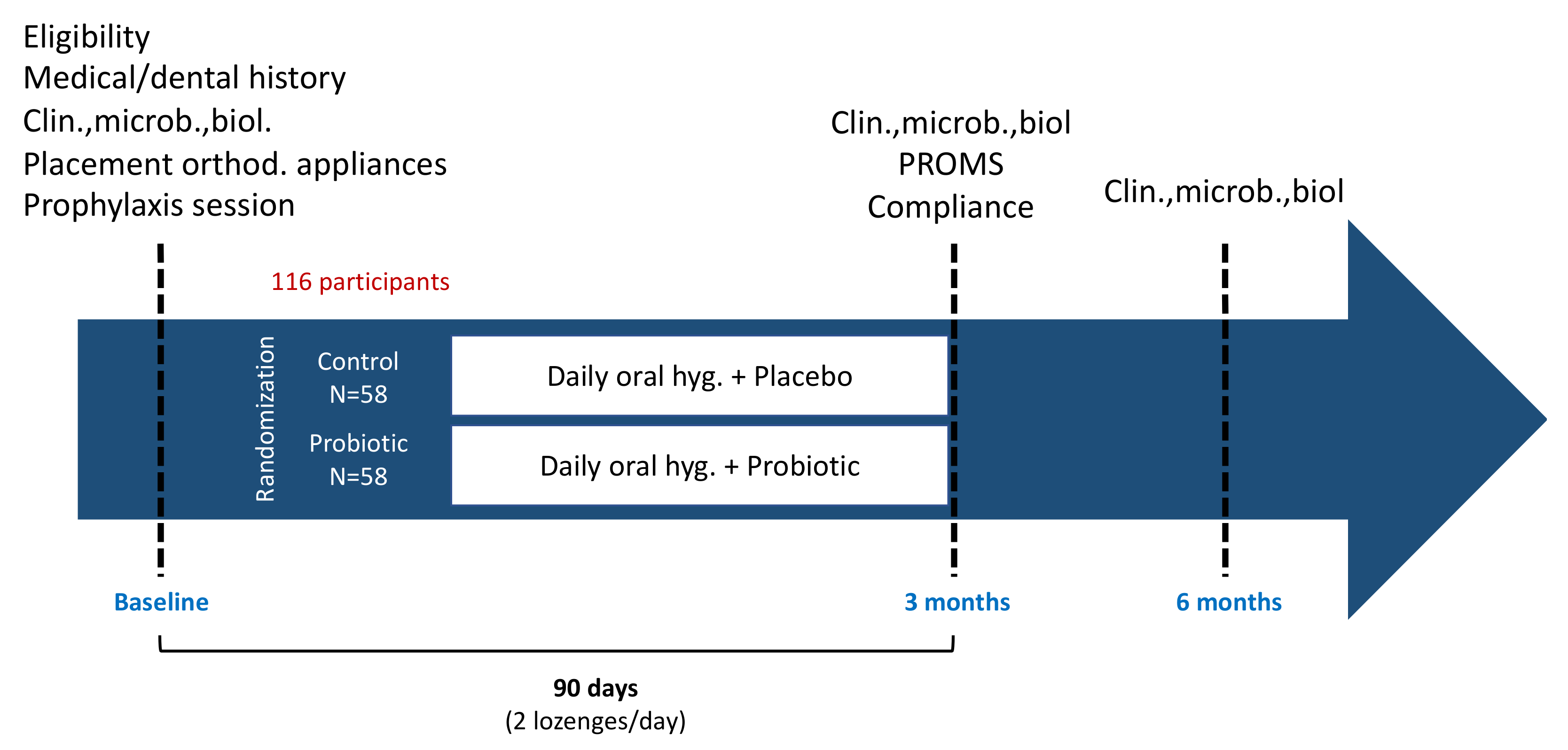
2.2. Study Design
2.3. Ethical Considerations
2.4. Sample Size Calculation
2.5. Subject Population and Inclusion/Exclusion Criteria
2.6. Interventions
2.7. Primary and Secondary Outcomes Variables
2.8. Monitoring of Compliance Patient-Related Outcomes and Adverse Events (3 and/or 6 Months)
2.9. Clinical Examination (Baseline, 3 and 6 Months)
2.10. Microbiological Monitoring (Baseline, 3 and 6 Months)
2.11. Salivary Biomarkers Monitoring (Baseline, 3 and 6 Months)
2.12. Randomization et Data Management
2.13. Statistical Analysis
3. Discussion
4. Trial Status
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ren, Y.; Jongsma, M.A.; Mei, L.; Van Der Mei, H.C.; Busscher, H.J. Orthodontic treatment with fixed appliances and biofilm formation—A potential public health threat? Clin. Oral Investig. 2014, 18, 1711–1718. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Li, J.; Mei, L.; Du, J.; Levrini, L.; Abbate, G.M.; Li, H. Periodontal health during orthodontic treatment with clear aligners and fixed appliances. J. Am. Dent. Assoc. 2018, 149, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Contaldo, M.; Lucchese, A.; Lajolo, C.; Rupe, C.; Di Stasio, D.; Romano, A.; Petruzzi, M.; Serpico, R. The Oral Microbiota Changes in Orthodontic Patients and Effects on Oral Health: An Overview. J. Clin. Med. 2021, 10, 780. [Google Scholar] [CrossRef]
- Kado, I.; Hisatsune, J.; Tsuruda, K.; Tanimoto, K.; Sugai, M. The impact of fixed orthodontic appliances on oral microbiome dynamics in Japanese patients. Sci. Rep. 2020, 10, 21989. [Google Scholar] [CrossRef] [PubMed]
- Müller, L.K.; Jungbauer, G.; Jungbauer, R.; Wolf, M.; Deschner, J. Biofilm and orthodontic therapy. Monogr. Oral Sci. 2021, 29, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Ghijselings, E.; Coucke, W.; Verdonck, A.; Teughels, W.; Quirynen, M.; Pauwels, M.; Carels, C.; van Gastel, J. Long-term changes in microbiology and clinical periodontal variables after completion of fixed orthodontic appliances. Orthod. Craniofacial Res. 2013, 17, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Jung, W.-S.; Cho, S.; Ahn, S.-J. Changes in salivary periodontal pathogens after orthodontic treatment: An in vivo prospective study. Angle Orthod. 2015, 86, 998–1003. [Google Scholar] [CrossRef] [Green Version]
- FAO; WHO. Probiotics in food: Health and nutritional properties and guidelines for evaluation. In Advances in Probiotics: Microorganisms in Food and Health; Dhansekaran, D., Sankaranarayanan, A., Eds.; Elsevier: Amsterdam, The Netherlands, 2006; p. 272. [Google Scholar]
- Meurman, J.H.; Stamatova, I. Probiotics: Contributions to oral health. Oral Dis. 2007, 13, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Meurman, J.H. Probiotics: Do they have a role in oral medicine and dentistry? Eur. J. Oral Sci. 2005, 113, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Saïz, P.; Taveira, N.; Alves, R. Probiotics in Oral Health and Disease: A Systematic Review. Appl. Sci. 2021, 11, 8070. [Google Scholar] [CrossRef]
- Mahasneh, S.A.; Mahasneh, A.M. Probiotics: A Promising Role in Dental Health. Dent. J. 2017, 5, 26. [Google Scholar] [CrossRef] [Green Version]
- Routier, A.; Blaizot, A.; Agossa, K.; Dubar, M. What do we know about the mechanisms of action of probiotics on factors involved in the pathogenesis of periodontitis? A scoping review of in vitro studies. Arch. Oral Biol. 2021, 129, 105196. [Google Scholar] [CrossRef] [PubMed]
- Martin-Cabezas, R.; Davideau, J.L.; Tenenbaum, H.; Huck, O. Clinical efficacy of probiotics as an adjunctive therapy to non-surgical periodontal treatment of chronic periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2016, 43, 520–530. [Google Scholar] [CrossRef]
- Ikram, S.; Hassan, N.; Raffat, M.A.; Mirza, S.; Akram, Z. Systematic review and meta-analysis of double-blind, placebo-controlled, randomized clinical trials using probiotics in chronic periodontitis. J. Investig. Clin. Dent. 2018, 9, e12338. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Zhong, T.; Dai, Q. Clinical efficacy of probiotics as an adjunctive therapy to scaling and root planning in the management of periodontitis: A systematic review and meta-analysis of randomized controlled trails. J. Evid. Based Dent. Pract. 2021, 21, 101547. [Google Scholar] [CrossRef]
- Akram, Z.; Shafqat, S.S.; Aati, S.; Kujan, O.; Fawzy, A. Clinical efficacy of probiotics in the treatment of gingivitis: A systematic review and meta-analysis. Aust. Dent. J. 2020, 65, 12–20. [Google Scholar] [CrossRef]
- Liu, J.; Liu, Z.; Huang, J.; Tao, R. Effect of probiotics on gingival inflammation and oral microbiota: A meta-analysis. Oral Dis. 2021. [CrossRef] [PubMed]
- Barboza, E.P.; Arriaga, P.C.; Luz, D.P.; Montez, C.; Vianna, K.C. Systematic review of the effect of probiotics on experimental gingivitis in humans. Braz. Oral Res. 2020, 34, e031. [Google Scholar] [CrossRef]
- Folke, C.; Carpenter, S.; Walker, B.; Scheffer, M.; Elmqvist, T.; Gunderson, L.; Holling, C.S. Regime shifts, resilience, and biodiversity in ecosystem management. Annu. Rev. Ecol. Evol. Syst. 2004, 35, 557–581. [Google Scholar] [CrossRef] [Green Version]
- Rosier, B.T.; Marsh, P.D.; Mira, A. Resilience of the Oral Microbiota in Health: Mechanisms That Prevent Dysbiosis. J. Dent. Res. 2018, 97, 371–380. [Google Scholar] [CrossRef]
- Pérez-Chaparro, P.J.; Gonçalves, C.; Figueiredo, L.C.; Faveri, M.; Lobão, E.; Tamashiro, N.; Duarte, P.; Feres, M. Newly identified pathogens associated with periodontitis: A systematic review. J. Dent. Res. 2014, 93, 846–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elkaim, R.; Werner, S.; Kocgozlu, L.; Tenenbaum, H. P. gingivalis Regulates the Expression of Cathepsin B and Cystatin C. J. Dent. Res. 2008, 87, 932–936. [Google Scholar] [CrossRef] [PubMed]
- Di Benedetto, A.; Gigante, I.; Colucci, S.; Grano, M. Periodontal disease: Linking the primary inflammation to bone loss. Clin. Dev. Immunol. 2013, 2013, 503754. [Google Scholar] [CrossRef] [Green Version]
- Buduneli, N.; Kinane, D.F. Host-derived diagnostic markers related to soft tissue destruction and bone degradation in periodontitis. J. Clin. Periodontol. 2011, 38 Suppl 11, 85–105. [Google Scholar] [CrossRef]
- Agossa, K.; Morand, D.N.; Tenenbaum, H.; Davideau, J.L.; Huck, O. Systemic applications of anti-inflammatory agents in periodontal treatment. Clin. Anti-Inflamm. Anti-Allergy Drugs 2015, 2, 3–13. [Google Scholar] [CrossRef]
- Anusha, R.L.; Umar, D.; Basheer, B.; Baroudi, K. The magic of magic bugs in oral cavity: Probiotics. J. Adv. Pharm. Technol. Res. 2015, 6, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, P.; Saini, H.; Dixit, J.; Singhal, R. Probiotics and oral health. Natl. J. Maxillofac. Surg. 2011, 2, 6–9. [Google Scholar] [CrossRef]
- Mishra, S.; Rath, S.; Mohanty, N. Probiotics—A complete oral healthcare package. J. Integr. Med. 2020, 18, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Gill, H.; Prasad, J. Probiotics, immunomodulation, and health benefits. Adv. Exp. Med. Biol. 2008, 606, 423–454. [Google Scholar] [CrossRef]
- Kobayashi, R.; Kobayashi, T.; Sakai, F.; Hosoya, T.; Yamamoto, M.; Kurita-Ochiai, T. Oral administration of Lactobacillus gasseri SBT2055 is effective in preventing Porphyromonas gingivalis-accelerated periodontal disease. Sci. Rep. 2017, 7, 545. [Google Scholar] [CrossRef]
- Teughels, W.; Durukan, A.; Ozcelik, O.; Pauwels, M.; Quirynen, M.; Haytac, M.C. Clinical and microbiological effects of Lactobacillus reuteri probiotics in the treatment of chronic periodontitis: A randomized placebo-controlled study. J. Clin. Periodontol. 2013, 40, 1025–1035. [Google Scholar] [CrossRef] [Green Version]
- Montero, E.; Iniesta, M.; Rodrigo, M.; Marín, M.J.; Figuero, E.; Herrera, D.; Sanz, M. Clinical and microbiological effects of the adjunctive use of probiotics in the treatment of gingivitis: A randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 708–716. [Google Scholar] [CrossRef]
- Twetman, S.; Derawi, B.; Keller, M.; Ekstrand, K.; Yucel-Lindberg, T.; Stecksen-Blicks, C. Short-term effect of chewing gums containing probiotic Lactobacillus reuteri on the levels of inflammatory mediators in gingival crevicular fluid. Acta Odontol. Scand. 2009, 67, 19–24. [Google Scholar] [CrossRef]
- Shimauchi, H.; Mayanagi, G.; Nakaya, S.; Minamibuchi, M.; Ito, Y.; Yamaki, K.; Hirata, H. Improvement of periodontal condition by probiotics with Lactobacillus salivarius WB21: A randomized, double-blind, placebo-controlled study. J. Clin. Periodontol. 2008, 35, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Schlagenhauf, U.; Rehder, J.; Gelbrich, G.; Jockel-Schneider, Y. Consumption of Lactobacillus reuteri-containing lozenges improves periodontal health in navy sailors at sea: A randomized controlled trial. J. Periodontol. 2020, 91, 1328–1338. [Google Scholar] [CrossRef] [Green Version]
- Schlagenhauf, U.; Jakob, L.; Eigenthaler, M.; Segerer, S.; Jockel-Schneider, Y.; Rehn, M. Regular consumption of Lactobacillus reuteri-containing lozenges reduces pregnancy gingivitis: An RCT. J. Clin. Periodontol. 2016, 43, 948–954. [Google Scholar] [CrossRef] [Green Version]
- Hadj-Hamou, R.; Senok, A.C.; Athanasiou, A.E.; Kaklamanos, E.G. Do probiotics promote oral health during orthodontic treatment with fixed appliances? A systematic review. BMC Oral Heal. 2020, 20, 126. [Google Scholar] [CrossRef]
- Pietri, F.K.; Rossouw, P.E.; Javed, F.; Michelogiannakis, D. Role of Probiotics in Oral Health Maintenance Among Patients Undergoing Fixed Orthodontic Therapy: A Systematic Review of Randomized Controlled Clinical Trials. Probiotics Antimicrob. Proteins 2020, 12, 1349–1359. [Google Scholar] [CrossRef]
- Benic, G.Z.; Farella, M.; Morgan, X.C.; Viswam, J.; Heng, N.C.; Cannon, R.D.; Mei, L. Oral probiotics reduce halitosis in patients wearing orthodontic braces: A randomized, triple-blind, placebo-controlled trial. J. Breath Res. 2019, 13, 036010. [Google Scholar] [CrossRef] [PubMed]
- Habib, S. Assessment of the Therapeutic Potential of a Dental Probiotic in Orthodontic Patients Affected by Gingivitis: A Randomized Controlled Trial. Master’s Thesis, University of Toronto, Toronto, ON, Canada, November 2016. Available online: https://tspace.library.utoronto.ca/handle/1807/79737 (accessed on 16 December 2021).
- Kohar, M.; Emmanuel, V.; Astuti, L. Comparison between probiotic lozenges and drinks towards periodontal status improvement of orthodontic patients. Dent. J. (Maj. Kedokt. Gigi) 2015, 48, 126–129. [Google Scholar] [CrossRef]
- Shah, S.S.; Nambiar, S.; Kamath, D.; Suman, E.; Unnikrishnan, B.; Desai, A.; Mahajan, S.; Dhawan, K.K. Comparative evaluation of plaque inhibitory and antimicrobial efficacy of probiotic and chlorhexidine oral rinses in orthodontic patients: A randomized clinical trial. Int. J. Dent. 2019, 2019, 1964158. [Google Scholar] [CrossRef] [Green Version]
- Löe, H. The Gingival Index, the Plaque Index and the Retention Index Systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Alanzi, A.; Honkala, S.; Honkala, E.; Varghese, A.; Tolvanen, M.; Söderling, E. Effect of Lactobacillus rhamnosus and Bifidobacterium lactis on gingival health, dental plaque, and periodontopathogens in adolescents: A randomised placebo-controlled clinical trial. Benef. Microbes 2018, 9, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Löe, H.; Silness, J. Periodontal disease in pregnancy I. Prevalence and severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef]
- Benamghar, L.; Leclercq, M.H.; Bourgeois, D.; McCombie, B.J.; Barmes, D.E. Standard descriptive tables in WHO Oral Health epidemiological studies. World Health Stat. Q. 1994, 47, 75–82. [Google Scholar] [PubMed]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef] [PubMed]
- Hedayati-Hajikand, T.; Lundberg, U.; Eldh, C.; Twetman, S. Effect of probiotic chewing tablets on early childhood caries-a randomized controlled trial. BMC Oral Health. 2015, 15, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera, D.; Escudero, N.; Perez, L.; Otheo, M.; Canete-Sanchez, E.; Perez, T.; Alonso, B.; Serrano, J.; Palma, J.C.; Sanz, M.; et al. Clinical and microbiological effects of the use of a cetylpyridinium chloride dentifrice and mouth rinse in orthodontic patients: A 3-month randomized clinical trial. Eur. J. Orthod. 2018, 40, 465–474. [Google Scholar] [CrossRef]
- Boyer, E.; Le Gall-David, S.; Martin, B.; Fong, S.B.; Loréal, O.; Deugnier, Y.; Bonnaure-Mallet, M.; Meuric, V. Increased transferrin saturation is associated with subgingival microbiota dysbiosis and severe periodontitis in genetic haemochromatosis. Sci. Rep. 2018, 8, 15532. [Google Scholar] [CrossRef]
- Lundmark, A.; Hu, Y.O.O.; Huss, M.; Johannsen, G.; Andersson, A.F.; Yucel-Lindberg, T. Identification of Salivary Microbiota and Its Association With Host Inflammatory Mediators in Periodontitis. Front. Cell. Infect. Microbiol. 2019, 9, 216. [Google Scholar] [CrossRef] [PubMed]
- Liang, K.Y.; Zeger, S. Longitudinal data analysis of continuous and discrete responses for pre-post designs. Sankhya Ind. J. Stat. Ser. B. 2000, 62, 134–148. [Google Scholar]
- Liu, G.F.; Lu, K.; Mogg, R.; Mallick, M.; Mehrotra, D.V. Should baseline be a covariate or dependent variable in analyses of change form baseline in clinical trials? Stat. Med. 2009, 28, 2509–2530. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J. Parametric versus non-parametric statistics in the analysis of randomized trials with non-normally distributed data. BMC Med. Res. Methodol. 2005, 5, 35. [Google Scholar] [CrossRef] [Green Version]
- Conover, W.J.; Iman, R.L. Analysis of covariance using the rank transformation. Biometrics 1982, 38, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Meuric, V.; Lainé, F.; Boyer, E.; Le Gall-David, S.; Oger, E.; Bourgeois, D.; Bouchard, P.; Bardou-Jacquet, E.; Turmel, V.; Bonnaure-Mallet, M.; et al. Periodontal status and serum biomarker levels in HFE haemochromatosis patients. A case-series study. J. Clin. Periodontol. 2017, 44, 892–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John and Wiley and Sons: Hoboken, NJ, USA, 1987. [Google Scholar] [CrossRef]
- Cenzato, N.; Nobili, A.; Maspero, C. Prevalence of Dental Malocclusions in Different Geographical Areas: Scoping Review. Dent. J. 2021, 9, 117. [Google Scholar] [CrossRef] [PubMed]
- Chestnutt, I.G.; Burden, D.J.; Steele, J.G.; Pitts, N.B.; Nuttall, N.M.; Morris, A.J. The orthodontic condition of children in the United Kingdom, 2003. Br. Dent. J. 2006, 200, 609–612. [Google Scholar] [CrossRef] [PubMed]
- Jawad, Z.; Bates, C.; Hodge, T. Who needs orthodontic treatment? Who gets it? And who wants it? Br. Dent. J. 2015, 218, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Bilgic, F.; Gelgor, I.E.; Celebi, A.A. Malocclusion prevalence and orthodontic treatment need in central Anatolian adolescents compared to European and other nations’ adolescents. Dent. Press J. Orthod. 2015, 20, 75–81. [Google Scholar] [CrossRef]
- Josefsson, E.; Bjerklin, K.; Lindsten, R. Malocclusion frequency in Swedish and immigrant adolescents: Influence of origin on orthodontic treatment need. Eur. J. Orthod. 2007, 29, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perillo, L.; Masucci, C.; Ferro, F.; Apicella, D.; Baccetti, T. Prevalence of orthodontic treatment need in southern Italian schoolchildren. Eur. J. Orthod. 2010, 32, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Travess, H.; Roberts-Harry, D.; Sandy, J. Orthodontics. Part 6: Risks in orthodontic treatment. Br. Dent. J. 2004, 196, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlagenhauf, U.; Jockel-Schneider, Y. Probiotics in the management of gingivitis and periodontitis. Front. Dent. Med. 2021, 2, 708666. [Google Scholar] [CrossRef]
- Kuru, B.E.; Laleman, I.; Yalnizoglu, T.; Kuru, L.; Teughels, W. The influence of a bifidobacterium animalis probiotic on gingival health: A randomized controlled clinical trial. J. Periodontol. 2017, 88, 1115–1123. [Google Scholar] [CrossRef]
- Toiviainen, A.; Jalasvuori, H.; Lahti, E.; Gursoy, U.; Salminen, S.; Fontana, M.; Flannagan, S.; Eckert, G.; Kokaras, A.; Paster, B.; et al. Impact of orally administered lozenges with Lactobacillus rhamnosus GG and Bifidobacterium animalis subsp. lactis BB-12 on the number of salivary mutans streptococci, amount of plaque, gingival inflammation and the oral microbiome in healthy adults. Clin. Oral Investig. 2015, 19, 77–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkaya, B.; Laleman, I.; Keceli, S.; Ozcelik, O.; Haytac, M.C.; Teughels, W. Clinical effects of probiotics containing Bacillus species on gingivitis: A pilot randomized controlled trial. J. Periodontal Res. 2017, 52, 497–504. [Google Scholar] [CrossRef]
- Iniesta, M.; Herrera, D.; Montero, E.; Zurbriggen, M.; Matos, A.R.; Marin, M.J.; Sanchez-Beltran, M.C.; Llama-Palacio, A.; Sanz, M. Probiotic effects of orally administered Lactobacillus reuteri-containing tablets on the subgingival and salivary microbiota in patients with gingivitis. A randomized clinical trial. J. Clin. Periodontol. 2012, 39, 736–744. [Google Scholar] [CrossRef]
- Hallstrom, H.; Lindgren, S.; Yucel-Lindberg, T.; Dahlen, G.; Renvert, S.; Twetman, S. Effect of probiotic lozenges on inflammatory reactions and oral biofilm during experimental gingivitis. Acta Odontol. Scand. 2013, 71, 828–833. [Google Scholar] [CrossRef]
- Yuki, O.; Furutani, C.; Mizota, Y.; Wakita, A.; Mimura, S.; Kihara, T.; Ohara, M.; Okada, Y.; Okada, M.; Nikawa, H. Effect of bovine milk fermented with Lactobacillus rhamnosus L8020 on periodontal disease in individuals with intellectual disability: A randomized clinical trial. J. Appl. Oral Sci. 2019, 27, e20180564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trombelli, L.; Farina, R. A review of factors influencing the incidence and severity of plaque-induced gingivitis. Minerva Stomatol. 2013, 62, 207–234. [Google Scholar] [PubMed]
- Benic, G.Z. Biofilm Management with Oral probiotics in Patients with Fixed Orthodontic Appliances. Ph.D. Thesis, University of Otago, Dunedin, New Zealand, August 2016. Available online: https://ourarchive.otago.ac.nz/handle/10523/6924 (accessed on 11 January 2022).
- Tsichlaki, A.; Chin, S.Y.; Pandis, N.; Fleming, P.S. How long does treatment with fixed orthodontic appliances last? A systematic review. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 308–318. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Enrolment | Allocation | Post-Allocation | |||
|---|---|---|---|---|---|
| TIMEPOINT | T-1 | Intervention (T0) | 3 Month Follow-Up (T1) | 6 Month Follow-Up (T2) | |
| ENROLMENT: | |||||
| Elligibility screen | X | ||||
| Informed consent | X | ||||
| Medical/dental history | X | ||||
| Allocation | X | ||||
| INTERVENTIONS: | |||||
| Orthodontic appliances | X | ||||
| Prophylaxis session | X | ||||
| Probiotic/placebo delivery | X | ||||
| ASSESSMENTS: | |||||
| Clinical | X | X | X | ||
| Microbiological | X | X | X | ||
| Biological | X | X | X | ||
| PROMS 1 | X | ||||
| Compliance | X | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agossa, K.; Dubar, M.; Lemaire, G.; Blaizot, A.; Catteau, C.; Bocquet, E.; Nawrocki, L.; Boyer, E.; Meuric, V.; Siepmann, F. Effect of Lactobacillus reuteri on Gingival Inflammation and Composition of the Oral Microbiota in Patients Undergoing Treatment with Fixed Orthodontic Appliances: Study Protocol of a Randomized Control Trial. Pathogens 2022, 11, 112. https://doi.org/10.3390/pathogens11020112
Agossa K, Dubar M, Lemaire G, Blaizot A, Catteau C, Bocquet E, Nawrocki L, Boyer E, Meuric V, Siepmann F. Effect of Lactobacillus reuteri on Gingival Inflammation and Composition of the Oral Microbiota in Patients Undergoing Treatment with Fixed Orthodontic Appliances: Study Protocol of a Randomized Control Trial. Pathogens. 2022; 11(2):112. https://doi.org/10.3390/pathogens11020112
Chicago/Turabian StyleAgossa, Kevimy, Marie Dubar, Grégoire Lemaire, Alessandra Blaizot, Céline Catteau, Emmanuël Bocquet, Laurent Nawrocki, Emile Boyer, Vincent Meuric, and Florence Siepmann. 2022. "Effect of Lactobacillus reuteri on Gingival Inflammation and Composition of the Oral Microbiota in Patients Undergoing Treatment with Fixed Orthodontic Appliances: Study Protocol of a Randomized Control Trial" Pathogens 11, no. 2: 112. https://doi.org/10.3390/pathogens11020112
APA StyleAgossa, K., Dubar, M., Lemaire, G., Blaizot, A., Catteau, C., Bocquet, E., Nawrocki, L., Boyer, E., Meuric, V., & Siepmann, F. (2022). Effect of Lactobacillus reuteri on Gingival Inflammation and Composition of the Oral Microbiota in Patients Undergoing Treatment with Fixed Orthodontic Appliances: Study Protocol of a Randomized Control Trial. Pathogens, 11(2), 112. https://doi.org/10.3390/pathogens11020112