

Stable Gastric Pentadecapeptide BPC 157 as a Therapy and Safety Key: A Special Beneficial Pleiotropic Effect Controlling and Modulating Angiogenesis and the NO-System

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Angiogenesis
2.1. Angiogenesis, Cornea Neovascularization, and Tumor Growth
2.2. Corneal Transparency to Illustrate the Consistent Organ-Specific Healing Angiogenesis Effect
2.3. BPC 157 and VEGF
2.4. BPC 157 and Tumor
2.5. BPC 157 vs. Procedures and Agents That Particularly Promote Epithelial Growth, a Widely Acknowledged Fear of Inappropriate Levels of Proliferation, or Potentially Carcinomatous Changes
2.6. BPC 157/egr-1
2.7. BPC 157/NO-System
2.8. Summarizing BPC 157/Angiogenesis, Cornea Neovascularization, VEGF, and Tumor Growth
3. NO-System
3.1. Multitude of BPC 157 Beneficial Effects Related to the NO-System as Proof of Concept
3.2. NO-Level in Tissue, Increased or Decreased, Was Regularly Normalized Through BPC 157 Administration, Along with Increased MDA-Level Decrease (and/or Normalization) Through BPC 157 Administration
3.3. BPC 157 and Parkinson’s Disease and Alzheimer’s Disease
4. Final Considerations Regarding General Concerns
5. Human Data
6. Transfer of Animal Data and Reliability of Results
- i.
- ii.
- iii.
- Topical at the injured nerve, intraperitoneal, intragastric [288];
- iv.
- v.
- Intramuscular vs. percutaneous into the bone defect [291];
- vi.
- Intramuscular vs. intragastric [292];
- vii.
- Topical application at the brain vs. intraperitoneal vs. intragastric [133];
- viii.
- Eye drops vs. intraperitoneal vs. per oral [113];
- ix.
- Eye drops vs. intraperitoneal [111].
7. Proving of the Findings’ Relevance by the Extent of Background Concept Development and Realization, and the Extent of the Research
8. Final Remarks and Conclusions
Funding
Conflicts of Interest
References
- Józwiak, M.; Bauer, M.; Kamysz, W.; Kleczkowska, P. Multifunctionality and possible medical application of the BPC 157 peptide-literature and patent review. Pharmaceuticals 2025, 18, 185. [Google Scholar] [CrossRef] [PubMed]
- Dekker, T.J. Injectable therapeutic peptides—An adjunct to regenerative medicine and sports performance? Arthroscopy 2025, 41, 150–152. [Google Scholar] [CrossRef] [PubMed]
- Grubisic, M.M.; Strbe, S.; Barisic, I.; Balenovic, D.; Stambolija, V.; Lozic, M.; Ostojic, S.B.; Oreskovic, I.; Zizek, H.; Brcic, K.; et al. Stable gastric pentadecapeptide BPC 157 as a therapy of severe electrolyte disturbances in rats. Curr. Neuropharmacol. 2025, Online ahead of print. [CrossRef] [PubMed]
- Sikiric, P.; Sever, M.; Krezic, I.; Vranes, H.; Kalogjera, L.; Smoday, I.M.; Vukovic, V.; Oroz, K.; Coric, L.; Skoro, M.; et al. New studies with stable gastric pentadecapeptide protecting gastrointestinal tract. Significance of counteraction of vascular and multiorgan failure of occlusion/occlusion-like syndrome in cytoprotection/organoprotection. Inflammopharmacology 2024, 32, 3119–3161. [Google Scholar] [CrossRef] [PubMed]
- Bajramagic, S.; Sever, M.; Rasic, F.; Staresinic, M.; Skrtic, A.; Beketic Oreskovic, L.; Oreskovic, I.; Strbe, S.; Loga Zec, S.; Hrabar, J.; et al. Stable gastric pentadecapeptide BPC 157 and intestinal anastomosis therapy in rats. A review. Pharmaceuticals 2024, 17, 1081. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Boban Blagaic, A.; Strbe, S.; Beketic Oreskovic, L.; Oreskovic, I.; Sikiric, S.; Staresinic, M.; Sever, M.; Kokot, A.; Jurjevic, I.; et al. The stable gastric pentadecapeptide BPC 157 pleiotropic beneficial activity and its possible relations with neurotransmitter activity. Pharmaceuticals 2024, 17, 461. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Boban Blagaic, A.; Krezic, I.; Zizek, H.; Kalogjera, L.; Smoday, I.M.; Vukovic, V.; Oroz, K.; Chiddenton, H.M.; Buric, S.; et al. From Selye’s and Szabo’s cysteamine-duodenal ulcer in rats to dopamine in the stomach: Therapy significance and possibilities. Pharmaceuticals 2023, 16, 1699. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Kokot, A.; Kralj, T.; Zlatar, M.; Masnec, S.; Lazic, R.; Loncaric, K.; Oroz, K.; Sablic, M.; Boljesic, M.; et al. Stable gastric pentadecapeptide BPC 157—Possible novel therapy of glaucoma and other ocular conditions. Pharmaceuticals 2023, 16, 1052. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Gojkovic, S.; Krezic, I.; Smoday, I.M.; Kalogjera, L.; Zizek, H.; Oroz, K.; Vranes, H.; Vukovic, V.; Labidi, M.; et al. Stable gastric pentadecapeptide BPC 157 may recover brain-gut axis and gut-brain axis function. Pharmaceuticals 2023, 16, 676. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Gojkovic, S.; Knezevic, M.; Tepes, M.; Strbe, S.; Vukojevic, J.; Duzel, A.; Kralj, T.; Krezic, I.; Zizek, H.; et al. Stable gastric pentadecapeptide BPC 157: Prompt particular activation of collateral pathways. Curr. Med. Chem. 2023, 30, 1568–1573. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Drmic, D.; Boban Blagaic, A.; Tvrdeic, A.; Krezic, I.; Gojkovic, S.; Zizek, H.; Sikiric, S.; Strbe, S.; Smoday, I.M.; et al. Stable gastric pentadecapeptide BPC 157 and NO-system. In Nitric Oxide: From Research to Therapeutics, Advances in Biochemistry in Health and Disease 22; Ray, A., Gulati, K., Eds.; Springer Nature: Cham, Switzerland, 2023; pp. 349–375. [Google Scholar] [CrossRef]
- Staresinic, M.; Japjec, M.; Vranes, H.; Prtoric, A.; Zizek, H.; Krezic, I.; Gojkovic, S.; Smoday, I.M.; Oroz, K.; Staresinic, E.; et al. Stable gastric pentadecapeptide BPC 157 and striated, smooth, and heart muscle. Biomedicines 2022, 10, 3221. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Udovicic, M.; Barisic, I.; Balenovic, D.; Zivanovic Posilovic, G.; Strinic, D.; Uzun, S.; Sikiric, S.; Krezic, I.; Zizek, H.; et al. Stable gastric pentadecapeptide BPC 157 as useful cytoprotective peptide therapy in the heart disturbances, myocardial infarction, pulmonary hypertension, arrhythmias, and thrombosis presentation. Biomedicines 2022, 10, 2696. [Google Scholar] [CrossRef] [PubMed]
- Vukojevic, J.; Milavić, M.; Perović, D.; Ilić, S.; Čilić, A.Z.; Đuran, N.; Štrbe, S.; Zoričić, Z.; Filipčić, I.; Brečić, P.; et al. Pentadecapeptide BPC 157 and the central nervous system. Neural Regen. Res. 2022, 17, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Deek, S.A. BPC 157 as potential treatment for COVID-19. Med. Hypotheses 2021, 158, 110736. [Google Scholar] [CrossRef] [PubMed]
- Seiwerth, S.; Milavic, M.; Vukojevic, J.; Gojkovic, S.; Krezic, I.; Vuletic, L.B.; Pavlov, K.H.; Petrovic, A.; Sikiric, S.; Vranes, H.; et al. Stable gastric pentadecapeptide BPC 157 and wound healing. Front. Pharmacol. 2021, 12, 627533. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Hahm, K.B.; Blagaic, A.B.; Tvrdeic, A.; Pavlov, K.H.; Petrovic, A.; Kokot, A.; Gojkovic, S.; Krezic, I.; Drmic, D.; et al. Stable gastric pentadecapeptide BPC 157, Robert’s stomach cytoprotection/adaptive cytoprotection/organoprotection, and Selye’s stress coping response: Progress, achievements, and future. Gut Liver 2020, 14, 153–167. [Google Scholar] [CrossRef] [PubMed]
- Park, J.M.; Lee, H.J.; Sikiric, P.; Hahm, K.B. BPC 157 rescued NSAID-cytotoxicity via stabilizing intestinal permeability and enhancing cytoprotection. Curr. Pharm. Des. 2020, 26, 2971–2981. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Drmic, D.; Sever, M.; Klicek, R.; Blagaic, A.B.; Tvrdeic, A.; Kralj, T.; Kovac, K.K.; Vukojevic, J.; Siroglavic, M.; et al. Fistulas healing. Stable gastric pentadecapeptide BPC 157 therapy. Curr. Pharm. Des. 2020, 26, 2991–3000. [Google Scholar] [CrossRef] [PubMed]
- Gwyer, D.; Wragg, N.M.; Wilson, S.L. Gastric pentadecapeptide body protection compound BPC 157 and its role in accelerating musculoskeletal soft tissue healing. Cell Tissue Res. 2019, 377, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Seiwerth, S.; Rucman, R.; Turkovic, B.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; Stupnisek, M.; Misic, M.; Vuletic, L.B.; et al. BPC 157 and standard angiogenic growth factors. Gastrointestinal tract healing, lessons from tendon, ligament, muscle and bone healing. Curr. Pharm. Des. 2018, 24, 1972–1989. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.A.; Han, Y.M.; An, J.M.; Park, Y.J.; Sikiric, P.; Kim, D.H.; Kwon, K.A.; Kim, Y.J.; Yang, D.; Tchah, H.; et al. BPC157 as potential agent rescuing from cancer cachexia. Curr. Pharm. Des. 2018, 24, 1947–1956. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Rucman, R.; Turkovic, B.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; Stupnisek, M.; Misic, M.; Vuletic, L.B.; et al. Novel cytoprotective mediator, stable gastric pentadecapeptide BPC 157. Vascular recruitment and gastrointestinal tract healing. Curr. Pharm. Des. 2018, 24, 1990–2001. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Seiwerth, S.; Rucman, R.; Drmic, D.; Stupnisek, M.; Kokot, A.; Sever, M.; Zoricic, I.; Zoricic, Z.; Batelja, L.; et al. Stress in gastrointestinal tract and stable gastric pentadecapeptide BPC 157. Finally, do we have a solution? Curr. Pharm. Des. 2017, 23, 4012–4028. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S.; Yoshida, M.; Filakovszky, J.; Juhasz, G. “Stress” is 80 years old: From Hans Selye original paper in 1936 to recent advances in GI ulceration. Curr. Pharm. Des. 2017, 23, 4029–4041. [Google Scholar] [CrossRef] [PubMed]
- Gyires, K.; Feher, A. Stress. Neuropeptides and gastric mucosa. Curr. Pharm. Des. 2017, 23, 3928–3940. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Seiwerth, S.; Rucman, R.; Kolenc, D.; Vuletic, L.B.; Drmic, D.; Grgic, T.; Strbe, S.; Zukanovic, G.; Crvenkovic, D.; et al. Brain-gut axis and pentadecapeptide BPC 157: Theoretical and practical implications. Curr. Neuropharmacol. 2016, 14, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Seiwerth, S.; Brcic, L.; Vuletic, L.B.; Kolenc, D.; Aralica, G.; Misic, M.; Zenko, A.; Drmic, D.; Rucman, R.; Sikiric, P. BPC 157 and blood vessels. Curr. Pharm. Des. 2014, 20, 1121–1125. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Seiwerth, S.; Rucman, R.; Turkovic, B.; Rokotov, D.S.; Brcic, L.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; et al. Stable gastric pentadecapeptide BPC 157-NO-system relation. Curr. Pharm. Des. 2014, 20, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Seiwerth, S.; Rucman, R.; Turkovic, B.; Rokotov, D.S.; Brcic, L.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; et al. Toxicity by NSAIDs. Counteraction by stable gastric pentadecapeptide BPC 157. Curr. Pharm. Des. 2013, 19, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Seiwerth, S.; Rucman, R.; Turkovic, B.; Rokotov, D.S.; Brcic, L.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; et al. Focus on ulcerative colitis: Stable gastric pentadecapeptide BPC 157. Curr. Med. Chem. 2012, 19, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Seiwerth, S.; Rucman, R.; Turkovic, B.; Rokotov, D.S.; Brcic, L.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; et al. Stable gastric pentadecapeptide BPC 157: Novel therapy in gastrointestinal tract. Curr. Pharm. Des. 2011, 17, 1612–1632. [Google Scholar] [CrossRef] [PubMed]
- Mózsik, G.; Szabó, I.L.; Czimmer, J. Approaches to gastrointestinal cytoprotection: From isolated cells.; via animal experiments to healthy human subjects and patients with different gastrointestinal disorders. Curr. Pharm. Des. 2011, 17, 1556–1572. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Seiwerth, S.; Brcic, L.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; Ilic, S.; Kolenc, D. Revised Robert’s cytoprotection and adaptive cytoprotection and stable gastric pentadecapeptide BPC 157. Possible significance and implications for novel mediator. Curr. Pharm. Des. 2010, 16, 1224–1234. [Google Scholar] [CrossRef] [PubMed]
- Mózsik, G. Gastric cytoprotection 30 years after its discovery by Andre Robert: A personal perspective. Inflammopharmacology 2010, 18, 209–221. [Google Scholar] [CrossRef]
- Mózsik, G.; Dömötör, A.; Rumi, G.; Szekeres, G. Gastrointestinal cytoprotection: From basic science to clinical perspectives. Inflammopharmacology 2007, 15, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Seiwerth, S.; Brcic, L.; Blagaic, A.B.; Zoricic, I.; Sever, M.; Klicek, R.; Radic, B.; Keller, N.; Sipos, K.; et al. Stable gastric pentadecapeptide BPC 157 in trials for inflammatory bowel disease (PL-10, PLD-116, PL 14736, Pliva, Croatia). Full and distended stomach, and vascular response. Inflammopharmacology 2006, 14, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Wood, J.D. The first Nobel prize for integrated systems physiology: Ivan Petrovich Pavlov, 1904. Physiology 2004, 19, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P. The pharmacological properties of the novel peptide BPC 157 (PL-10). Inflammopharmacology 1999, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Sikirić, P.; Petek, M.; Rucman, R.; Seiwerth, S.; Grabarević, Z.; Rotkvić, I.; Turković, B.; Jagić, V.; Mildner, B.; Duvnjak, M.; et al. A new gastric juice peptide.; BPC. An overview of the stomach-stress-organoprotection hypothesis and beneficial effects of BPC. J. Physiol. Paris. 1993, 87, 313–327. [Google Scholar] [CrossRef] [PubMed]
- Robert, A. Cytoprotection by prostaglandins. Gastroenterology 1979, 77, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Robert, A. Current history of cytoprotection. Prostaglandins 1981, 21 (Suppl. S1), 89–96. [Google Scholar] [CrossRef] [PubMed]
- Robert, A.; Nezamis, J.E.; Lancaster, C.; Davis, J.P.; Field, S.O.; Hanchar, A.J. Mild irritants prevent gastric necrosis through “adaptive cytoprotection” mediated by prostaglandins. Am. J. Physiol. 1983, 245, G113–G121. [Google Scholar] [CrossRef] [PubMed]
- Szabó, S. Role of sulfhydryls and early vascular lesions in gastric mucosal injury. Acta Physiol. Hung. 1984, 64, 203–214. [Google Scholar] [PubMed]
- Trier, J.S.; Szabo, S.; Allan, C.H. Ethanol-induced damage to mucosal capillaries of rat stomach. Ultrastructural features and effects of prostaglandin F2 beta and cysteamine. Gastroenterology 1987, 92, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Pihan, G.; Majzoubi, D.; Haudenschild, C.; Trier, J.S.; Szabo, S. Early microcirculatory stasis in acute gastric mucosal injury in the rat and prevention by 16,16-dimethyl prostaglandin E2 or sodium thiosulfate. Gastroenterology 1986, 91, 1415–2146. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S.; Trier, J.S.; Brown, A.; Schnoor, J. Early vascular injury and increased vascular permeability in gastric mucosal injury caused by ethanol in the rat. Gastroenterology 1985, 88, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S. Experimental basis for a role for sulfhydryls and dopamine in ulcerogenesis: A primer for cytoprotection--organoprotection. Klin. Wochenschr. 1986, 64 (Suppl. S7), 16–122. [Google Scholar] [PubMed]
- Szabo, S.; Usadel, K.H. Cytoprotection-organoprotection by somatostatin: Gastric and hepatic lesions. Experientia 1982, 38, 254–256. [Google Scholar] [CrossRef] [PubMed]
- Sandor, Z.; Nagata, M.; Kusstatscher, S.; Szabo, S. Stimulation of mucosal glutathione and angiogenesis: New mechanisms of gastroprotection and ulcer healing by sucralfate. Scand. J. Gastroenterol. Suppl. 1995, 210, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S. The mode of action of sucralfate: The 1 × 1 × 1 mechanism of action. Scand. J. Gastroenterol. Suppl. 1991, 185, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Whittle, B.J.R.; Lopez-Bermonte, J.; Moncada, S. Regulation of gastric mucosal integrity by endogenous nitric oxide: Interactions with prostanoids and sensory neuropeptides in the rat. Br. J. Pharmacol. 1990, 99, 607–611. [Google Scholar] [CrossRef] [PubMed]
- Tepperman, B.L.; Whittle, B.J. Endogenous nitric oxide and sensory neuropeptides interact in the modulation of the rat gastric microcirculation. Br. J. Pharmacol. 1992, 105, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Peskar, B.M.; Respondek, M.; Muller, K.M.; Peskar, B.E. A role of nitric oxide in capsaicin-induced gastroprotection. Eur. J. Pharmacol. 1991, 198, 113–114. [Google Scholar] [CrossRef] [PubMed]
- Dembinska-Kiec, A.; Pallapies, D.; Simmet, T.; Peskar, B.M.; Peskar, B.A. Effect of carbenoxolone on the biological activity of nitric oxide: Relation to gastroprotection. Br. J. Pharmacol. 1991, 104, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.K.S.; Cho, C.H. Involvement of nitric oxide in the adaptive cytoprotection of mild irritants against injury caused by ethanol. Digestion 1994, 55 (Suppl. S2), 20. [Google Scholar] [CrossRef]
- Holzer, P. Peptidergic sensory neurons in the control of vascular functions: Mechanisms and significance in the cutaneous and splanchnic vascular beds. Rev. Physiol. Biochem. Pharmacol. 1992, 121, 49–146. [Google Scholar] [CrossRef] [PubMed]
- Veljaca, M.; Chan, K.; Guglietta, A. Digestion of h-EGF, h-TGF alpha, and BPC-15 in human gastric juice. Gastroenterology 1995, 108, 761. [Google Scholar] [CrossRef]
- Selye, H. A syndrome produced by diverse nocuous agents. Nature 1936, 138, 32. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S.; Tache, Y.; Somogyi, A. The legacy of Hans Selye and the origins of stress research: A retrospective 75 years after his landmark brief “letter” to the editor# of Nature. Stress 2012, 15, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Masson, G.; Selye, H. Réaction générale d’adaptation: Ses indications pratiques. Can. J. Comp. Med. 1938, 2, 282–285. [Google Scholar] [PubMed]
- Szabo, S.; Glavin, G.B. Hans Selye and the concept of biologic stress. Ulcer pathogenesis as a historical paradigm. Ann. N. Y. Acad. Sci. 1990, 597, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Sikirić, P.; Seiwerth, S.; Desković, S.; Grabarević, Z.; Marović, A.; Rucman, R.; Petek, M.; Konjevoda, P.; Jadrijević, S.; Sosa, T.; et al. New model of cytoprotection/adaptive cytoprotection in rats: Endogenous small irritants, antiulcer agents and indomethacin. Eur. J. Pharmacol. 1999, 364, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Becejac, T.; Cesarec, V.; Drmic, D.; Hirsl, D.; Madzarac, G.; Djakovic, Z.; Bunjevac, I.; Zenko Sever, A.; Sepac, A.; Batelja Vuletic, L.; et al. An endogeous defensive concept, renewed cytoprotection/adaptive cytoprotection: Intra(per)-oral/intragastric strong alcohol in rat. Involvement of pentadecapeptide BPC 157 and nitric oxide system. J. Physiol. Pharmacol. 2018, 69, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Van Epps, H.L. What tumors need a brief history of angiogenesis. J. Exp. Med. 2005, 201, 1024. [Google Scholar] [CrossRef]
- Langer, R.; Folkman, J. Polymers for the sustained release of proteins and other macromolecules. Nature 1976, 263, 797–800. [Google Scholar] [CrossRef] [PubMed]
- Klagsbrun, M.; Moses, M.A. Obituary: M. Judah Folkman (1933–2008). Nature 2008, 451, 781. [Google Scholar] [CrossRef] [PubMed]
- Brower, V. Judah Folkman leaves expanding legacy. J. Natl. Cancer Inst. 2008, 100, 380. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Retrospective: Judah Folkman (1933–2008). Science 2008, 319, 1055. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J. Tumor angiogenesis: Therapeutic implications. N. Engl. J. Med. 1971, 285, 1182–1186. [Google Scholar] [CrossRef]
- Folkman, J.; Klagsbrun, M. Angiogenic factors. Science 1987, 235, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Ausprunk, D.H.; Falterman, K.; Folkman, J. The sequence of events in the regression of corneal capillaries. Lab. Investig. 1978, 38, 284–294. [Google Scholar] [PubMed]
- Langer, R.; Brem, H.; Falterman, K.; Klein, M.; Folkman, J. Isolation of a cartilage factor which inhibits tumor neovascularization. Science 1976, 193, 70–72. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Separovic, J.; Anic, T.; Buljat, G.; Mikus, D.; Seiwerth, S.; Grabarevic, Z.; Stancic-Rokotov, D.; Pigac, B.; Hanzevacki, M.; et al. The effect of pentadecapeptide BPC 157, H2-blockers, omeprazole and sucralfate on new vessels and new granulation tissue formation. J. Physiol. Paris. 1999, 93, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S.; Vattay, P.; Scarbrough, E.; Folkman, J. Role of vascular factors, including angiogenesis, in the mechanisms of action of sucralfate. Am. J. Med. 1991, 91, 158S–160S. [Google Scholar] [CrossRef] [PubMed]
- Masnec, S.; Kokot, A.; Zlatar, M.; Kalauz, M.; Kunjko, K.; Radic, B.; Klicek, R.; Drmic, D.; Lazic, R.; Brcic, L.; et al. Perforating corneal injury in rat and pentadecapeptide BPC 157. Exp. Eye Res. 2015, 136, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Lazić, R.; Gabrić, N.; Dekaris, I.; Bosnar, D.; Boban-Blagaić, A.; Sikirić, P. Gastric pentadecapeptide BPC 157 promotes corneal epithelial defects healing in rats. Coll. Antropol. 2005, 29, 321–325. [Google Scholar] [PubMed]
- Mirković, I.; Kralj, T.; Lozić, M.; Stambolija, V.; Kovačević, J.; Vrdoljak, L.; Zlatar, M.; Milanović, K.; Drmić, D.; Predović, J.; et al. Pentadecapeptide BPC 157 shortens duration of tetracaine- and oxybuprocaine-induced corneal anesthesia in rats. Acta Clin. Croat. 2020, 59, 394–406. [Google Scholar] [CrossRef] [PubMed]
- Kralj, T.; Kokot, A.; Kasnik, K.; Drmic, D.; Zlatar, M.; Seiwerth, S.; Sikiric, P. Effects of pentadecapeptide BPC 157 on experimental rat model of dry eye. FASEB J. 2017, 31 (Suppl. S1), 993.3. [Google Scholar] [CrossRef]
- Japjec, M.; Horvat Pavlov, K.; Petrovic, A.; Staresinic, M.; Sebecic, B.; Buljan, M.; Vranes, H.; Giljanovic, A.; Drmic, D.; Japjec, M.; et al. Stable gastric pentadecapeptide BPC157 as a therapy for the disable myotendinous junctions in rats. Biomedicines 2021, 9, 1547. [Google Scholar] [CrossRef] [PubMed]
- Matek, D.; Matek, I.; Staresinic, E.; Japjec, M.; Bojanic, I.; Boban Blagaic, A.; Beketic Oreskovic, L.; Oreskovic, I.; Ziger, T.; Novinscak, T.; et al. Stable gastric pentadecapeptide BPC157 as therapy after surgical detachment of the quadriceps muscle from its attachments for muscle-to-bone reattachment in rats. Pharmaceutics 2025, 17, 119. [Google Scholar] [CrossRef] [PubMed]
- Cerovecki, T.; Bojanic, I.; Brcic, L.; Radic, B.; Vukoja, I.; Seiwerth, S.; Sikiric, P. Pentadecapeptide BPC 157 (PL 14736) improves ligament healing in the rat. J. Orthop. Res. 2010, 28, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Pevec, D.; Novinscak, T.; Brcic, L.; Sipos, K.; Jukic, I.; Staresinic, M.; Mise, S.; Brcic, I.; Kolenc, D.; Klicek, R. Impact of pentadecapeptide BPC 157 on muscle healing impaired by systemic corticosteroid application. Med. Sci. Monit. 2010, 16, BR81–BR88. [Google Scholar] [PubMed]
- Brcic, L.; Brcic, I.; Staresinic, M.; Novinscak, T.; Sikiric, P.; Seiwerth, S. Modulatory effect of gastric pentadecapeptide BPC 157 on angiogenesis in muscle and tendon healing. J. Physiol. Pharmacol. 2009, 60 (Suppl. S7), 191–196. [Google Scholar] [PubMed]
- Mihovil, I.; Radic, B.; Brcic, L.; Brcic, I.; Vukoja, I.; Ilic, S.; Boban Blagaic, A.; Seiwerth, S.; Sikiric, P. Beneficial effect of pentadecapeptide BPC 157 on denervated muscle in rats. J. Physiol. Pharmacol. 2009, 60, 69. [Google Scholar]
- Krivic, A.; Majerovic, M.; Jelic, I.; Seiwerth, S.; Sikiric, P. Modulation of early functional recovery of Achilles tendon to bone unit after transection by BPC 157 and methylprednisolone. Inflamm. Res. 2008, 57, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Novinscak, T.; Brcic, L.; Staresinic, M.; Jukic, I.; Radic, B.; Pevec, D.; Mise, S.; Tomasovic, S.; Brcic, I.; Banic, T.; et al. Gastric pentadecapeptide BPC 157 as an effective therapy for muscle crush injury in the rat. Surg. Today 2008, 38, 716–725. [Google Scholar] [CrossRef] [PubMed]
- Staresinic, M.; Petrovic, I.; Novinscak, T.; Jukic, I.; Pevec, D.; Suknaic, S.; Kokic, N.; Batelja, L.; Brcic, L.; Boban-Blagaic, A.; et al. Effective therapy of transected quadriceps muscle in rat: Gastric pentadecapeptide BPC 157. J. Orthop. Res. 2006, 24, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Krivic, A.; Anic, T.; Seiwerth, S.; Huljev, D.; Sikiric, P. Achilles detachment in rat and stable gastric pentadecapeptide BPC 157: Promoted tendon-to-bone healing and opposed corticosteroid aggravation. J. Orthop. Res. 2006, 24, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Staresinic, M.; Sebecic, B.; Patrlj, L.; Jadrijevic, S.; Suknaic, S.; Perovic, D.; Aralica, G.; Zarkovic, N.; Borovic, S.; Srdjak, M.; et al. Gastric pentadecapeptide BPC 157 accelerates healing of transected rat Achilles tendon and in vitro stimulates tendocytes growth. J. Orthop. Res. 2003, 21, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Krivic, A.; Sikiric, P. Comment on “Use of recombinant human bone morphogenetic protein-2 to enhance tendon healing in a bone tunnel”. Am. J. Sports Med. 2003, 31, 636–637, author reply 637–638. [Google Scholar] [PubMed]
- Wu, H.; Wei, M.; Li, N.; Lu, Q.; Shrestha, S.M.; Tan, J.; Zhang, Z.; Wu, G.; Shi, R. Clopidogrel-induced gastric injury in rats is attenuated by stable gastric pentadecapeptide BPC 157. Drug Des. Devel. Ther. 2020, 14, 5599–5610. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.J.; Lee, C.H.; Chueh, H.Y.; Chang, G.J.; Huang, H.Y.; Lin, Y.; Pang, J.S. Modulatory effects of BPC 157 on vasomotor tone and the activation of Src-Caveolin-1-endothelial nitric oxide synthase pathway. Sci. Rep. 2020, 10, 17078. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.J.; Liu, H.T.; Wang, C.N.; Huang, H.Y.; Lin, Y.; Ko, Y.S.; Wang, J.S.; Chang, V.H.; Pang, J.S. Therapeutic potential of pro-angiogenic BPC157 is associated with VEGFR2 activation and up-regulation. J. Mol. Med. 2017, 95, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Radeljak, S.; Seiwerth, S.; Sikiric, P. BPC 157 inhibits cell growth and VEGF signalling via the MAPK kinase pathway in the human melanoma cell line. Melanoma Res. 2004, 14, A14–A15. [Google Scholar] [CrossRef]
- Huang, T.; Zhang, K.; Sun, L.; Xue, X.; Zhang, C.; Shu, Z.; Mu, N.; Gu, J.; Zhang, W.; Wang, Y.; et al. Body protective compound-157 enhances alkali-burn wound healing in vivo and promotes proliferation, migration, and angiogenesis in vitro. Drug Des. Devel. Ther. 2015, 9, 2485–2499. [Google Scholar] [CrossRef] [PubMed]
- Sikirić, P.; Seiwerth, S.; Grabarević, Z.; Rucman, R.; Petek, M.; Jagić, V.; Turković, B.; Rotkvić, I.; Mise, S.; Zoricić, I.; et al. The influence of a novel pentadecapeptide, BPC 157, on N(G)-nitro-L-arginine methylester and L-arginine effects on stomach mucosa integrity and blood pressure. Eur. J. Pharmacol. 1997, 332, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Turkovic, B.; Sikiric, P.; Seiwerth, S.; Mise, S.; Anic, T.; Petek, M. Stable gastric pentadecapeptide BPC 157 studied for inflammatory bowel disease (PLD-116, PL14736, Pliva) induces nitric oxide synthesis. Gastroenterology 2004, 126, 287. [Google Scholar] [CrossRef]
- Stupnisek, M.; Kokot, A.; Drmic, D.; Hrelec Patrlj, M.; Zenko Sever, A.; Kolenc, D.; Radic, B.; Suran, J.; Bojic, D.; Vcev, A.; et al. Pentadecapeptide BPC 157 reduces bleeding and thrombocytopenia after amputation in rats treated with heparin, warfarin, L-NAME and L-arginine. PLoS ONE 2015, 10, e0123454. [Google Scholar] [CrossRef] [PubMed]
- Tkalcević, V.I.; Cuzić, S.; Brajsa, K.; Mildner, B.; Bokulić, A.; Situm, K.; Perović, D.; Glojnarić, I.; Parnham, M.J. Enhancement by PL 14736 of granulation and collagen organization in healing wounds and the potential role of egr-1 expression. Eur. J. Pharmacol. 2007, 570, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.H.; Garg, N.K.; Lunde, E.; Han, K.Y.; Jain, S.; Azar, D.T. Corneal neovascularization: An anti-VEGF therapy review. Surv. Ophthalmol. 2012, 57, 415–429. [Google Scholar] [CrossRef]
- Folkman, J.; Klagsbrun, M. Vascular physiology. A family of angiogenic peptides. Nature 1987, 329, 671–672. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Li, X.; Ma, J.; Lv, X.; Zhao, S.; Lang, W.; Zhang, Y. Blockade of the intermediate-conductance Ca(2+)-activated K+ channel inhibits the angiogenesis induced by epidermal growth factor in the treatment of corneal alkali burn. Exp. Eye Res. 2013, 110, 76–87. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S.; Sandor, Z. The diagnostic and prognostic value of tumor angiogenesis. Eur. J. Surg. Suppl. 1998, 582, 99–103. [Google Scholar] [CrossRef]
- Li, Z.; Shimada, Y.; Uchida, S.; Maeda, M.; Kawabe, A.; Mori, A.; Itami, A.; Kano, M.; Watanabe, G.; Imamura, M. TGF-alpha as well as VEGF, PD-ECGF and bFGF contribute to angiogenesis of esophageal squamous cell carcinoma. Int. J. Oncol. 2000, 17, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Rofstad, E.K.; Halsør, E.F. Vascular endothelial growth factor, interleukin 8, platelet-derived endothelial cell growth factor, and basic fibroblast growth factor promote angiogenesis and metastasis in human melanoma xenografts. Cancer Res. 2000, 60, 4932–4938. [Google Scholar] [PubMed]
- Pötgens, A.J.; Westphal, H.R.; de Waal, R.M.; Ruiter, D.J. The role of vascular permeability factor and basic fibroblast growth factor in tumor angiogenesis. Biol. Chem. Hoppe Seyler. 1995, 376, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Relf, M.; LeJeune, S.; Scott, P.A.; Fox, S.; Smith, K.; Leek, R.; Moghaddam, A.; Whitehouse, R.; Bicknell, R.; Harris, A.L. Expression of the angiogenic factors vascular endothelial cell growth factor.; acidic and basic fibroblast growth factor, tumor growth factor beta-1, platelet-derived endothelial cell growth factor, placenta growth factor, and pleiotrophin in human primary breast cancer and its relation to angiogenesis. Cancer Res. 1997, 57, 963–969. [Google Scholar] [PubMed]
- Locopo, N.; Fanelli, M.; Gasparini, G. Clinical significance of angiogenic factors in breast cancer. Breast Cancer Res. Treat. 1998, 52, 159–173. [Google Scholar] [CrossRef] [PubMed]
- Kralj, T.; Kokot, A.; Zlatar, M.; Busic, M.; Milkovic Perisa, M.; Batelja Vuletic, L.; Horvat Pavlov, K.; Drmic, D.; Seiwerth, S.; Sikiric, P. Stable gastric pentadecapeptide BPC 157 in rats with episcleral veins cauterization, glaucoma model, preserved retinal and optic nerve integrity. FASEB J. 2019, 33 (Suppl. S1), 822.6. [Google Scholar] [CrossRef]
- Kokot, A.; Zlatar, M.; Stupnisek, M.; Drmic, D.; Radic, R.; Vcev, A.; Seiwerth, S.; Sikiric, P. NO system dependence of atropine-induced mydriasis and L-NAME- and L-arginine-induced miosis: Reversal by the pentadecapeptide BPC 157 in rats and guinea pigs. Eur. J. Pharmacol. 2016, 771, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Zlatar, M.; Kokot, A.; Vuletic, L.B.; Masnec, S.; Kralj, T.; Perisa, M.M.; Barisic, I.; Radic, B.; Milanovic, K.; Drmic, D.; et al. BPC 157 as a therapy for retinal ischemia induced by retrobulbar application of L-NAME in rats. Front. Pharmacol. 2021, 12, 632295. [Google Scholar] [CrossRef] [PubMed]
- Kralj, T.; Kokot, A.; Zlatar, M.; Masnec, S.; Kasnik Kovac, K.; Milkovic Perisa, M.; Batelja Vuletic, L.; Giljanovic, A.; Strbe, S.; Sikiric, S.; et al. Stable gastric pentadecapeptide BPC 157 therapy of rat glaucoma. Biomedicines 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.M.; Lagopoulos, M.; McConnell, P.; Soames, R.W.; Sefton, G.K. Blood supply of the Achilles tendon. J. Orthop. Res. 1998, 16, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Gelberman, R.H. Flexor tendon physiology: Tendon nutrition and cellular activity in injury and repair. Instr. Course Lect. 1985, 34, 351–360. [Google Scholar] [PubMed]
- Schmidt-Rohlfing, B.; Graf, J.; Schneider, U.; Niethard, F.U. The blood supply of the Achilles tendon. Int. Orthop. 1992, 16, 29–31. [Google Scholar] [CrossRef] [PubMed]
- Peacock, E.E., Jr. A study of the circulation in normal tendons and healing grafts. Ann. Surg. 1959, 149, 415–428. [Google Scholar] [CrossRef] [PubMed]
- Sever, A.Z.; Sever, M.; Vidovic, T.; Lojo, N.; Kolenc, D.; Vuletic, L.B.; Drmic, D.; Kokot, A.; Zoricic, I.; Coric, M.; et al. Stable gastric pentadecapeptide BPC 157 in the therapy of the rats with bile duct ligation. Eur. J. Pharmacol. 2019, 847, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Bocca, C.; Novo, E.; Miglietta, A.; Parola, M. Angiogenesis and fibrogenesis in chronic liver diseases. Cell Mol. Gastroenterol. Hepatol. 2015, 1, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Bosch, J.; Abraldes, J.G.; Fernández, M.; García-Pagán, J.C. Hepatic endothelial dysfunction and abnormal angiogenesis: New targets in the treatment of portal hypertension. J. Hepatol. 2010, 53, 558–567. [Google Scholar] [CrossRef] [PubMed]
- Fernández, M.; Semela, D.; Bruix, J.; Colle, I.; Pinzani, M.; Bosch, J. Angiogenesis in liver disease. J. Hepatol. 2009, 50, 604–620. [Google Scholar] [CrossRef] [PubMed]
- Tshionyi, M.; Shay, E.; Lunde, E.; Lin, A.; Han, K.Y.; Jain, S.; Chang, J.H.; Azar, D.T. Hemangiogenesis and lymphangiogenesis in corneal pathology. Cornea 2012, 31, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Ciftci, M.D.; Selver, O.B. Clinical evaluation of corneal neovascularization: A brief review. J. Ophthalmic. Res. Vis. Care. 2022, 2. [Google Scholar] [CrossRef]
- Kaminska, G.M.; Niederkorn, J.Y. Spontaneous corneal neovascularization in nude mice. Local imbalance between angiogenic and anti-angiogenic factors. Investig. Ophthalmol. Vis. Sci. 1993, 34, 222–230. [Google Scholar] [PubMed]
- Maisonpierre, P.C.; Suri, C.; Jones, P.F.; Bartunkova, S.; Wiegand, S.J.; Radziejewski, C.; Compton, D.; McClain, J.; Aldrich, T.H.; Papadopoulos, N.; et al. Angiopoietin-2, a natural antagonist for Tie2 that disrupts in vivo angiogenesis. Science 1997, 277, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Azar, D.T. Corneal angiogenic privilege: Angiogenic and antiangiogenic factors in corneal avascularity, vasculogenesis, and wound healing (an American Ophthalmological Society thesis). Trans. Am. Ophthalmol. Soc. 2006, 104, 264–302. [Google Scholar] [PubMed]
- Maddula, S.; Davis, D.K.; Maddula, S.; Burrow, M.K.; Ambati, B.K. Horizons in therapy for corneal angiogenesis. Ophthalmology 2011, 118, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Di Zazzo, A.; Gaudenzi, D.; Yin, J.; Coassin, M.; Fernandes, M.; Dana, R.; Bonini, S. Corneal angiogenic privilege and its failure. Exp. Eye Res. 2021, 204, 108457. [Google Scholar] [CrossRef] [PubMed]
- Vukojević, J.; Siroglavić, M.; Kašnik, K.; Kralj, T.; Stanćić, D.; Kokot, A.; Kolarić, D.; Drmić, D.; Sever, A.Z.; Barišić, I.; et al. Rat inferior caval vein (ICV) ligature and particular new insights with the stable gastric pentadecapeptide BPC 157. Vascul. Pharmacol. 2018, 106, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Vranes, H.; Malekinusic, D.; Vrdoljak, B.; Knezevic, T.; Horvat Pavlov, K.; Drmic, D.; et al. Complex syndrome of complete occlusion of the end of the superior mesenteric vein, opposed with the stable gastric pentadecapeptide BPC 157 in rats. Biomedicines 2021, 9, 1029. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Malekinusic, D.; Vrdoljak, B.; Knezevic, T.; Vranes, H.; Drmic, D.; Staroveski, M.; et al. Occluded superior mesenteric artery and vein. Therapy with the stable gastric pentadecapeptide BPC 157. Biomedicines 2021, 9, 792. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Malekinusic, D.; Vrdoljak, B.; Vranes, H.; Knezevic, T.; Barisic, I.; Horvat Pavlov, K.; et al. Occlusion of the superior mesenteric artery in rats reversed by collateral pathways activation: Gastric pentadecapeptide BPC 157 therapy counteracts multiple organ dysfunction syndrome, intracranial, portal and caval hypertension, and aortal hypotension. Biomedicines 2021, 9, 609. [Google Scholar] [CrossRef] [PubMed]
- Gojkovic, S.; Krezic, I.; Vranes, H.; Zizek, H.; Drmic, D.; Horvat Pavlov, K.; Petrovic, A.; Batelja Vuletic, L.; Milavic, M.; Sikiric, S.; et al. BPC 157 therapy and permanent occlusion of the superior sagittal sinus in rats: Vascular recruitment. Biomedicines 2021, 9, 744. [Google Scholar] [CrossRef] [PubMed]
- Tepes, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Vranes, H.; Madzar, Z.; Santak, G.; Batelja, L.; Milavic, M.; Sikiric, S.; et al. Stable gastric pentadecapeptide BPC 157 therapy for primary abdominal compartment syndrome. Front. Pharmacol. 2021, 12, 718147. [Google Scholar] [CrossRef] [PubMed]
- Tepes, M.; Krezic, I.; Vranes, H.; Smoday, I.M.; Kalogjera, L.; Zizek, H.; Vukovic, V.; Oroz, K.; Kovac, K.K.; Madzar, Z.; et al. Stable gastric pentadecapeptide BPC 157: Effect on reperfusion following maintained intra-abdominal hypertension (grade III and grade IV) in rats. Pharmaceuticals 2023, 16, 1554. [Google Scholar] [CrossRef] [PubMed]
- Smoday, I.M.; Petrovic, I.; Kalogjera, L.; Vranes, H.; Zizek, H.; Krezic, I.; Gojkovic, S.; Skorak, I.; Hriberski, K.; Brizic, I.; et al. Therapy effect of the stable gastric pentadecapeptide BPC 157 on acute pancreatitis as vascular failure-induced severe peripheral and central syndrome in rats. Biomedicines 2022, 10, 1299. [Google Scholar] [CrossRef] [PubMed]
- Kalogjera, L.; Krezic, I.; Smoday, I.M.; Vranes, H.; Zizek, H.; Yago, H.; Oroz, K.; Vukovic, V.; Kavelj, I.; Novosel, L.; et al. Stomach perforation-induced general occlusion/occlusion-like syndrome and stable gastric pentadecapeptide BPC 157 therapy effect. World J. Gastroenterol. 2023, 29, 4289–4316. [Google Scholar] [CrossRef] [PubMed]
- Strbe, S.; Gojkovic, S.; Krezic, I.; Zizek, H.; Vranes, H.; Barisic, I.; Strinic, D.; Orct, T.; Vukojevic, J.; Ilic, S.; et al. Over-dose lithium toxicity as an occlusive-like syndrome in rats and gastric pentadecapeptide BPC 157. Biomedicines 2021, 9, 1506. [Google Scholar] [CrossRef] [PubMed]
- Gojkovic, S.; Krezic, I.; Vranes, H.; Zizek, H.; Drmic, D.; Batelja Vuletic, L.; Milavic, M.; Sikiric, S.; Stilinovic, I.; Simeon, P.; et al. Robert’s intragastric alcohol-induced gastric lesion model as an escalated general peripheral and central syndrome, counteracted by the stable gastric pentadecapeptide BPC 157. Biomedicines 2021, 9, 1300. [Google Scholar] [CrossRef] [PubMed]
- Smoday, I.M.; Krezic, I.; Kalogjera, L.; Vukovic, V.; Zizek, H.; Skoro, M.; Kovac, K.K.; Vranes, H.; Barisic, I.; Sikiric, S.; et al. Pentadecapeptide BPC 157 as therapy for inferior caval vein embolization: Recovery of sodium laurate-post-embolization syndrome in rats. Pharmaceuticals 2023, 16, 1507. [Google Scholar] [CrossRef] [PubMed]
- Premuzic Mestrovic, I.; Smoday, I.M.; Kalogjera, L.; Krezic, I.; Zizek, H.; Vranes, H.; Vukovic, V.; Oroz, K.; Skorak, I.; Brizic, I.; et al. Antiarrhythmic sotalol, occlusion/occlusion-like syndrome in rats, and stable gastric pentadecapeptide BPC 157 therapy. Pharmaceuticals 2023, 16, 977. [Google Scholar] [CrossRef] [PubMed]
- Strbe, S.; Smoday, I.M.; Krezic, I.; Kalogjera, L.; Vukovic, V.; Zizek, H.; Gojkovic, S.; Vranes, H.; Barisic, I.; Sikiric, S.; et al. Innate vascular failure by application of neuroleptics, amphetamine, and domperidone rapidly induced severe occlusion/occlusion-like syndromes in rats and stable gastric pentadecapeptide BPC 157 as therapy. Pharmaceuticals 2023, 16, 788. [Google Scholar] [CrossRef] [PubMed]
- Gamulin, O.; Oroz, K.; Coric, L.; Krajacic, M.; Skrabic, M.; Dretar, V.; Strbe, S.; Talapko, J.; Juzbasic, M.; Krezic, I.; et al. Fourier transform infrared spectroscopy reveals molecular changes in blood vessels of rats treated with pentadecapeptide BPC 157. Biomedicines 2022, 10, 3130. [Google Scholar] [CrossRef] [PubMed]
- Bilic, Z.; Gojkovic, S.; Kalogjera, L.; Krezic, I.; Malekinusic, D.; Knezevic, M.; Sever, M.; Lojo, N.; Kokot, A.; Kasnik, K.; et al. Novel insight into Robert’s cytoprotection: Complex therapeutic effect of cytoprotective pentadecapeptide BPC 157 in rats with perforated stomach throughout modulation of nitric oxide-system. Comparison with L-arginine, ranitidine and pantoprazole therapy and L-NG-nitro-L-arginine methyl ester worsening. J. Physiol. Pharmacol. 2021, 72, 939–955. [Google Scholar] [CrossRef] [PubMed]
- Vukojević, J.; Vrdoljak, B.; Malekinušić, D.; Siroglavić, M.; Milavić, M.; Kolenc, D.; Boban Blagaić, A.; Batelja, L.; Drmić, D.; Seiverth, S.; et al. The effect of pentadecapeptide BPC 157 on hippocampal ischemia/reperfusion injuries in rats. Brain Behav. 2020, 10, e01726. [Google Scholar] [CrossRef] [PubMed]
- Weissman, A.M. Themes and variations on ubiquitylation. Nat. Rev. Mol. Cell Biol. 2001, 2, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.; Xu, S.; Joazeiro, C.; Cobb, M.H.; Hunter, T. The PHD domain of MEKK1 acts as an E3 ubiquitin ligase and mediates ubiquitination and degradation of ERK1/2. Mol. Cell 2002, 9, 945–956. [Google Scholar] [CrossRef] [PubMed]
- Bergers, G.; Song, S.; Meyer-Morse, N.; Bergsland, E.; Hanahan, D. Benefits of targeting both pericytes and endothelial cells in the tumor vasculature with kinase inhibitors. J. Clin. Investig. 2003, 111, 1287–1295. [Google Scholar] [CrossRef] [PubMed]
- Dancey, J.; Sausville, E.A. Issues and progress with protein kinase inhibitors for cancer treatment. Nat. Rev. Drug Discov. 2003, 2, 296–313. [Google Scholar] [CrossRef] [PubMed]
- Hood, J.D.; Bednarski, M.; Frausto, R.; Guccione, S.; Reisfeld, R.A.; Xiang, R.; Cheresh, D.A. Tumor regression by targeted gene delivery to the neovasculature. Science 2002, 296, 2404–2407. [Google Scholar] [CrossRef] [PubMed]
- Hood, J.D.; Cheresh, D.A. Role of integrins in cell invasion and migration. Nat. Rev. Cancer 2002, 2, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Crvenkovic, D.; Sever, M.; Lojo, N.; Krstonijevic, Z.; Drmic, D.; Zenko, A.; Brcic, L.; Zoricic, I.; Rasic, Z.; et al. Pentadecapeptide BPC 157 after 70% liver resection in rats. FASEB J. 2013, 27 (Suppl. S1), 1093.26. [Google Scholar] [CrossRef]
- Crvenkovic, D.; Sever, M.; Zenko Sever, A.; Drmic, D.; Petrovic, I.; Romic, Z.; Seiwerth, S.; Sikiric, P. Pentadecapeptide BPC 157 after 70% liver resection in rats. Gastroenterology 2015, 1, S964. [Google Scholar] [CrossRef]
- Crvenkovic, D.; Sever, M.; Zenko Sever, A.; Zoricic, I.; Rasic, Z.; Romic, Z.; Seiwerth, S.; Sikiric, P. 70% liver resection in rats. Pentadecapeptide BPC 157, L-arginine, L-NAME: BPC 157 beneficial effect counteracts worsening induced by L-NAME. Gastroenterology 2016, 150, S342–S343. [Google Scholar] [CrossRef]
- Sever, M.; Klicek, R.; Radic, B.; Brcic, L.; Zoricic, I.; Drmic, D.; Ivica, M.; Barisic, I.; Ilic, S.; Berkopic, L.; et al. Gastric pentadecapeptide BPC 157 and short bowel syndrome in rats. Dig. Dis. Sci. 2009, 54, 2070–2083. [Google Scholar] [CrossRef] [PubMed]
- Pereira, P.M.; Bines, J.E. New growth factor therapies aimed at improving intestinal adaptation in short bowel syndrome. J. Gastroenterol. Hepatol. 2006, 21, 932–940. [Google Scholar] [CrossRef] [PubMed]
- Gimbrone, M.A.; Cotran, R.S.; Leapman, S.B.; Folkman, J. Tumor growth and neovascularization: An experimental model using the rabbit cornea. Natl. Cancer Inst. 1974, 52, 413–427. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Ameri, A.H.; Wang, S.; Jansson, K.H.; Casey, O.M.; Yang, Q.; Beshiri, M.L.; Fang, L.; Lake, R.G.; Agarwal, S.; et al. EGR1 regulates angiogenic and osteoclastogenic factors in prostate cancer and promotes metastasis. Oncogene 2019, 38, 6241–6255. [Google Scholar] [CrossRef] [PubMed]
- Myung, E.; Park, Y.-L.; Kim, N.; Chung, C.-Y.; Park, H.-C.; Myung, D.-S.; Kim, J.-S.; Cho, S.-B.; Lee, W.-S.; Joo, Y.-E. Expression of early growth response-1 in human gastric cancer and its relationship with tumor cell behaviors and prognosis. Pathol. Res. Pract. 2013, 209, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Kumbrink, J.; Gerlinger, M.; Johnson, J.P. Egr-1 induces the expression of its corepressor nab2 by activation of the nab2 promoter thereby establishing a negative feedback loop. J. Biol. Chem. 2005, 280, 42785–42793. [Google Scholar] [CrossRef] [PubMed]
- Du, B.; Fu, C.; Kent, K.C.; Bush, H., Jr.; Schulick, A.H.; Kreiger, K.; Collins, T.; McCaffrey, T.A. Elevated Egr-1 in human atherosclerotic cells transcriptionally represses the transforming growth factor-beta type II receptor. J. Biol. Chem. 2000, 275, 39039–39047. [Google Scholar] [CrossRef] [PubMed]
- Buitrago, M.; Lorenz, K.; Maass, A.H.; Oberdorf-Maass, S.; Keller, U.; Schmitteckert, E.M.; Ivashchenko, Y.; Lohse, M.J.; Engelhardt, S. The transcriptional repressor Nab1 is a specific regulator of pathological cardiac hypertrophy. Nat. Med. 2005, 11, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, S.; Velmurugan, G.; Rekha, B.; Anusha, S.; Shanmugha Rajan, K.; Shanmugarajan, S.; Ramprasath, T.; Gopal, P.; Tomar, D.; Karthik, K.V.; et al. Egr-1 mediated cardiac miR-99 family expression diverges physiological hypertrophy from pathological hypertrophy. Exp. Cell Res. 2018, 365, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.Y.; Guo, J.H.; Liu, Y.Q.; Dong, J.H.; Zhu, C.H. PPARgama activation-mediated egr-1 inhibition benefits against brain injury in an experimental ischaemic stroke model. J. Stroke Cerebrovasc. Dis. 2020, 29, 105255. [Google Scholar] [CrossRef] [PubMed]
- Magee, N.; Zhang, Y. Role of early growth response 1 in liver metabolism and liver cancer. Hepatoma Res. 2017, 3, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Tian, H.; Feng, Y.; Zhu, Y.; Zhang, W. Egr-1 promotes cell proliferation and invasion by increasing β-catenin expression in gastric cancer. Dig. Dis. Sci. 2013, 58, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Du, K.; Wu, X.; Ji, X.; Liang, N.; Li, Z. Early growth response 1 promoted the invasion of glioblastoma multiforme by elevating HMGB1. J. Neurosurg. Sci. 2023, 67, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Barisic, I.; Balenovic, D.; Udovicic, M.; Bardak, D.; Strinic, D.; Vlainić, J.; Vranes, H.; Smoday, I.M.; Krezic, I.; Milavic, M.; et al. Stable gastric pentadecapeptide BPC 157 may counteract myocardial infarction induced by isoprenaline in rats. Biomedicines 2022, 10, 265. [Google Scholar] [CrossRef] [PubMed]
- Vukusic, D.; Zenko Sever, A.; Sever, M.; Drmic, D.; Milavic, M.; Sikiric, S.; Rasic, D.; Krezic, I.; Gojkovic, S.; Prtoric, A.; et al. Duodenocolic fistula healing by pentadecapeptide BPC 157 in rats. A cytoprotection viewpoint. J. Physiol. Pharmacol. 2024, 75, 89–104. [Google Scholar] [CrossRef] [PubMed]
- Perovic, D.; Milavic, M.; Dokuzovic, S.; Krezic, I.; Gojkovic, S.; Vranes, H.; Bebek, I.; Bilic, V.; Somun, N.; Brizic, I.; et al. Novel therapeutic effects in rats spinal cord injuries: Recovery of definitive and early spinal cord injury by the administration of pentadecapeptide BPC 157 therapy. Curr. Issues Mol. Biol. 2022, 44, 1901–1927. [Google Scholar] [CrossRef] [PubMed]
- Zemba Cilic, A.; Zemba, M.; Cilic, M.; Strbe, S.; Ilic, S.; Vukojevic, J.; Zoricic, Z.; Filipcic, I.; Kokot, A.; Smoday, I.M.; et al. BPC 157, L-NAME, L-arginine, NO-relation, in the suited rat ketamine models resembling, “negative-like” symptoms of schizophrenia. Biomedicines 2022, 10, 1462. [Google Scholar] [CrossRef] [PubMed]
- Deng, X.; Xiong, X.; Khomenko, T.; Sandor, Z.; Osapay, K.; Tolstanova, G.; Shiloach, J.; Chen, L.; Folkman, J.; Szabo, S. Inappropriate angiogenic response as a novel mechanism of duodenal ulceration and impaired healing. Dig. Dis. Sci. 2011, 56, 2792–2801. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S.; Deng, X.; Tolstanova, G.; Khomenko, T.; Paunovic, B.; Chen, L.; Jadus, M.; Sandor, Z. Angiogenic and anti-angiogenic therapy for gastrointestinal ulcers: New challenges for rational therapeutic predictions and drug design. Curr. Pharm. Des. 2011, 17, 1633–1642. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S. Mechanisms of gastric mucosal injury and protection. J. Clin. Gastroenterol. 1991, 13 (Suppl. S2), S21–S34. [Google Scholar] [CrossRef] [PubMed]
- Grivennikov, S.I.; Karin, M. Inflammatory cytokines in cancer: Tumour necrosis factor and interleukin 6 take the stage. Ann. Rheum. Dis. 2011, 70 (Suppl. S1), i104–i108. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huang, L.; Zhao, H.; Yan, Y.; Lu, J. The role of interleukins in colorectal cancer. Int. J. Biol. Sci. 2020, 16, 2323–2339. [Google Scholar] [CrossRef] [PubMed]
- Ning, C.; Li, Y.-Y.; Wang, Y.; Han, G.-C.; Wang, R.-X.; Xiao, H.; Li, X.-Y.; Hou, C.-M.; Ma, Y.-F.; Sheng, D.-S.; et al. Complement activation promotes colitis-associated carcinogenesis through activating intestinal IL-1beta/IL-17A axis. Mucosal Immunol. 2015, 8, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- Hai Ping, P.; Feng Bo, T.; Li, L.; Nan Hui, Y.; Hong, Z. IL-1beta/NF-kb signaling promotes colorectal cancer cell growth through miR-181a/PTEN axis. Arch. Biochem. Biophys. 2016, 604, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Davis, C.; Shah, S.; Hughes, D.; Ryan, J.C.; Altomare, D.; Peña, M.M. IL-33 promotes growth and liver metastasis of colorectal cancer in mice by remodeling the tumor microenvironment and inducing angiogenesis. Mol. Carcinog. 2017, 56, 272–287. [Google Scholar] [CrossRef] [PubMed]
- Sucic, M.; Luetic, K.; Jandric, I.; Drmic, D.; Sever, A.Z.; Vuletic, L.B.; Halle, Z.B.; Strinic, D.; Kokot, A.; Seiwerth, R.S.; et al. Therapy of the rat hemorrhagic cystitis induced by cyclophosphamide. Stable gastric pentadecapeptide BPC 157, L-arginine, L-NAME. Eur. J. Pharmacol. 2019, 861, 172593. [Google Scholar] [CrossRef] [PubMed]
- Luetic, K.; Sucic, M.; Vlainic, J.; Halle, Z.B.; Strinic, D.; Vidovic, T.; Luetic, F.; Marusic, M.; Gulic, S.; Pavelic, T.T.; et al. Cyclophosphamide induced stomach and duodenal lesions as a NO-system disturbance in rats: L-NAME, L-arginine, stable gastric pentadecapeptide BPC 157. Inflammopharmacology 2017, 25, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Lovric-Bencic, M.; Sikiric, P.; Hanzevacki, J.S.; Seiwerth, S.; Rogic, D.; Kusec, V.; Aralica, G.; Konjevoda, P.; Batelja, L.; Blagaic, A.B. Doxorubicine-congestive heart failure-increased big endothelin-1 plasma concentration: Reversal by amlodipine, losartan, and gastric pentadecapeptide BPC157 in rat and mouse. J. Pharmacol. Sci. 2004, 95, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.S.; Huang, S.C.; Chen, F.H.; Chang, Y.; Mei, H.F.; Huang, H.Y.; Chen, W.Y.; Pang, J.S. Pentadecapeptide BPC 157 efficiently reduces radiation-induced liver injury and lipid accumulation through Kruppel-like factor 4 upregulation both in vivo and in vitro. Life Sci. 2022, 310, 121072. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Y.; Qu, M.; Duan, R.; Shi, D.; Jin, L.; Gao, J.; Wood, J.D.; Li, J.; Wang, G.D. Cytoprotective mechanism of the novel gastric peptide in gastrointestinal tract and cultured enteric neurons and glial cells. Neurosci. Bull. 2019, 35, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Tsai, W.C.; Hsu, Y.H.; Pang, J.H. Pentadecapeptide BPC 157 enhances the growth hormone receptor expression in tendon fibroblasts. Molecules 2014, 19, 19066–19077. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Tsai, W.C.; Lin, M.S.; Hsu, Y.H.; Pang, J.H. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. J. Appl. Physiol. 2011, 110, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Stupnisek, M.; Franjic, S.; Drmic, D.; Hrelec, M.; Kolenc, D.; Radic, B.; Bojic, D.; Vcev, A.; Seiwerth, S.; Sikiric, P. Pentadecapeptide BPC 157 reduces bleeding time and thrombocytopenia after amputation in rats treated with heparin, warfarin or aspirin. Thromb. Res. 2012, 129, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Konosic, S.; Petricevic, M.; Ivancan, V.; Konosic, L.; Goluza, E.; Krtalic, B.; Drmic, D.; Stupnisek, M.; Seiwerth, S.; Sikiric, P. Intragastric application of aspirin, clopidogrel, cilostazol, and BPC 157 in rats: Platelet aggregation and blood clot. Oxid. Med. Cell Longev. 2019, 2019, 9084643. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Belmonte, J.; Whittle, B.J.; Moncada, S. The actions of nitric oxide donors in the prevention or induction of injury to the rat gastric mucosa. Br. J. Pharmacol. 1993, 108, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Whittle, B.J.; Boughton-Smith, N.K.; Moncada, S. Biosynthesis and role of the endothelium-derived vasodilator, nitric oxide, in the gastric mucosa. Ann. N. Y. Acad. Sci. 1992, 664, 126–139. [Google Scholar] [CrossRef] [PubMed]
- Moncada, S. Nitric oxide. J. Hypertens. Suppl. 1994, 12, S35–S39. [Google Scholar] [PubMed]
- Drmic, D.; Samara, M.; Vidovic, T.; Malekinusic, D.; Antunovic, M.; Vrdoljak, B.; Ruzman, J.; Milkovic Perisa, M.; Horvat Pavlov, K.; Jeyakumar, J.; et al. Counteraction of perforated cecum lesions in rats: Effects of pentadecapeptide BPC 157, L-NAME and L-arginine. World J. Gastroenterol. 2018, 24, 5462–5476. [Google Scholar] [CrossRef] [PubMed]
- Amic, F.; Drmic, D.; Bilic, Z.; Krezic, I.; Zizek, H.; Peklic, M.; Klicek, R.; Pajtak, A.; Amic, E.; Vidovic, T.; et al. Bypassing major venous occlusion and duodenal lesions in rats, and therapy with the stable gastric pentadecapeptide BPC 157, L-NAME and L-arginine. World J. Gastroenterol. 2018, 24, 5366–5378. [Google Scholar] [CrossRef] [PubMed]
- Duzel, A.; Vlainic, J.; Antunovic, M.; Malekinusic, D.; Vrdoljak, B.; Samara, M.; Gojkovic, S.; Krezic, I.; Vidovic, T.; Bilic, Z.; et al. Stable gastric pentadecapeptide BPC 157 in the treatment of colitis and ischemia and reperfusion in rats: New insights. World J. Gastroenterol. 2017, 23, 8465–8488. [Google Scholar] [CrossRef] [PubMed]
- Gojkovic, S.; Krezic, I.; Vrdoljak, B.; Malekinusic, D.; Barisic, I.; Petrovic, A.; Horvat Pavlov, K.; Kolovrat, M.; Duzel, A.; Knezevic, M.; et al. Pentadecapeptide BPC 157 resolves suprahepatic occlusion of the inferior caval vein, Budd-Chiari syndrome model in rats. World J. Gastrointest. Pathophysiol. 2020, 11, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Kolovrat, M.; Gojkovic, S.; Krezic, I.; Malekinusic, D.; Vrdoljak, B.; Kasnik Kovac, K.; Kralj, T.; Drmic, D.; Barisic, I.; Horvat Pavlov, K.; et al. Pentadecapeptide BPC 157 resolves Pringle maneuver in rats.; both ischemia and reperfusion. World. J. Hepatol. 2020, 12, 184–206. [Google Scholar] [CrossRef] [PubMed]
- Belosic Halle, Z.; Vlainic, J.; Drmic, D.; Strinic, D.; Luetic, K.; Sucic, M.; Medvidovic-Grubisic, M.; Pavelic Turudic, T.; Petrovic, I.; Seiwerth, S.; et al. Class side effects: Decreased pressure in the lower oesophageal and the pyloric sphincters after the administration of dopamine antagonists, neuroleptics, anti-emetics, L-NAME, pentadecapeptide BPC 157 and L-arginine. Inflammopharmacology 2017, 25, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Marovic, A.; Matoz, W.; Anic, T.; Buljat, G.; Mikus, D.; Stancic-Rokotov, D.; Separovic, J.; Seiwerth, S.; Grabarevic, Z.; et al. A behavioural study of the effect of pentadecapeptide BPC 157 in Parkinson’s disease models in mice and gastric lesions induced by 1-methyl-4-phenyl-1,2,3,6-tetrahydrophyridine. J. Physiol. Paris. 1999, 93, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Jelovac, N.; Sikiric, P.; Rucman, R.; Petek, M.; Marovic, A.; Perovic, D.; Seiwerth, S.; Mise, S.; Turkovic, B.; Dodig, G.; et al. Pentadecapeptide BPC 157 attenuates disturbances induced by neuroleptics: The effect on catalepsy and gastric ulcers in mice and rats. Eur. J. Pharmacol. 1999, 379, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Zemba Cilic, A.; Zemba, M.; Cilic, M.; Balenovic, I.; Strbe, S.; Ilic, S.; Vukojevic, J.; Zoricic, Z.; Filipcic, I.; Kokot, A.; et al. Pentadecapeptide BPC 157 counteracts L-NAME-induced catalepsy. BPC 157, L-NAME, L-arginine, NO-relation, in the suited rat acute and chronic models resembling ‘positive-like’ symptoms of schizophrenia. Behav. Brain Res. 2021, 396, 112919. [Google Scholar] [CrossRef] [PubMed]
- Drmic, D.; Kolenc, D.; Ilic, S.; Bauk, L.; Sever, M.; Zenko Sever, A.; Luetic, K.; Suran, J.; Seiwerth, S.; Sikiric, P. Celecoxib-induced gastrointestinal.; liver and brain lesions in rats.; counteraction by BPC 157 or L-arginine.; aggravation by L-NAME. World J. Gastroenterol. 2017, 23, 5304–5312. [Google Scholar] [CrossRef] [PubMed]
- Zemba, M.; Cilic, A.Z.; Balenovic, I.; Cilic, M.; Radic, B.; Suran, J.; Drmic, D.; Kokot, A.; Stambolija, V.; Murselovic, T.; et al. BPC 157 antagonized the general anaesthetic potency of thiopental and reduced prolongation of anaesthesia induced by L-NAME/thiopental combination. Inflammopharmacology 2015, 23, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Lozic, M.; Stambolija, V.; Krezic, I.; Dugandzic, A.; Zivanovic-Posilovic, G.; Gojkovic, S.; Kovacevic, J.; Vrdoljak, L.; Mirkovic, I.; Kokot, A.; et al. In relation to NO-system, table gastric pentadecapeptide BPC 157 counteracts lidocaine-induced adverse effects in rats and depolarisation in vitro. Emerg. Med. Int. 2020, 2020, 6805354. [Google Scholar] [CrossRef] [PubMed]
- Georgiadou, G.; Pitsikas, N. Repeated administration of the nitric oxide synthase inhibitor l-NAME differentially affects rats’ recognition memory. Behav. Brain Res. 2011, 224, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Boultadakis, A.; Georgiadou, G.; Pitsikas, N. Effects of the nitric oxide synthase inhibitor L-NAME on different memory components as assessed in the object recognition task in the rat. Behav. Brain Res. 2010, 20, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Pitsikas, N.; Boultadakis, A.; Sakellaridis, N. Effects of sub-anesthetic doses of ketamine on rats’ spatial and non-spatial recognition memory. Neuroscience 2008, 154, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Trevlopoulou, A.; Touzlatzi, N.; Pitsikas, N. The nitric oxide donor sodium nitroprusside attenuates recognition memory deficits and social withdrawal produced by the NMDA receptor antagonist ketamine and induces anxiolytic-like behaviour in rats. Psychopharmacology 2016, 233, 1045–1054. [Google Scholar] [CrossRef] [PubMed]
- Tieppo, C.A.; Ferreira, F.S.; Sassatani, A.S.; Felicio, L.F.; Nasello, A.G. Opposite modulation of apomorphine- or amphetamine-induced stereotypy by antagonists of CCK receptors. Eur. J. Pharmacol. 2000, 387, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Moore, H.; Grace, A.A. A role for electrotonic coupling in the striatum in the expression of dopamine receptor-mediated stereotypies. Neuropsychopharmacology 2002, 27, 980–992. [Google Scholar] [CrossRef] [PubMed]
- Andine, P.; Widemark, N.; Axelsson, R.; Nyberg, G.; Olofsson, U.; Martensson, E.; Sandberg, M. Characterization of MK-801-induced behavior as a putative rat model of psychosis. J. Pharmacol. Exp. Ther. 1999, 290, 1393–1408. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, R.E.; Kapur, S.; Fletcher, P.J. The amphetamine-induced sensitized state as a model of schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2007, 31, 1556–1571. [Google Scholar] [CrossRef] [PubMed]
- Naylor, R.J.; Olley, J.E. Modification of the behavioural changes induced by amphetamine in the rat by lesions in the caudate nucleus, the caudate-putamen and globus pallidus. Neuropharmacology 1972, 11, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Rung, J.P.; Carlsson, A.; Rydén Markinhuhta, K.; Carlsson, M.L. (+)-MK-801 induced social withdrawal in rats; a model for negative symptoms of schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2005, 29, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Tenn, C.C.; Kapur, S.; Fletcher, P.J. Sensitization to amphetamine, but not phencyclidine, disrupts prepulse inhibition and latent inhibition. Psychopharmacology 2005, 180, 366–376. [Google Scholar] [CrossRef] [PubMed]
- Morelli, M.; DiChiara, G. Catalepsy induced by SCH 23390 in rats. Eur. J. Pharmacol. 1985, 117, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Medvidovic-Grubisic, M.; Stambolija, V.; Kolenc, D.; Katancic, J.; Murselovic, T.; Plestina-Borjan, I.; Strbe, S.; Drmic, D.; Barisic, I.; Sindic, A.; et al. Hypermagnesemia disturbances in rats, NO-related: Pentadecapeptide BPC 157 abrogates, L-NAME and L-arginine worsen. Inflammopharmacology 2017, 25, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Guo, A.W. The search for a magic bullet to fight multiple organ failure secondary to ischemia/reperfusion injury and abdominal compartment syndrome. J. Surg. Res. 2013, 184, 792–793. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Dawson, V.L.; Dawson, T.M. Role of nitric oxide in Parkinson’s disease. Pharmacol. Ther. 2006, 109, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.K.; Dawson, T.M.; Dawson, V.L. Nitric oxide, S-nitrosylation and neurodegeneration. Cell Mol. Biol. 2005, 51, 247–254. [Google Scholar] [PubMed]
- Chung, K.K.; Dawson, V.L.; Dawson, T.M. S-nitrosylation in Parkinson’s disease and related neurodegenerative disorders. Methods Enzymol. 2005, 396, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Lu, D.; Wang, X.; Wang, Z.; Li, W.; Chen, G. The effects of nitric oxide in Alzheimer’s disease. Med. Gas. Res. 2023, 14, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Azargoonjahromi, A. Dual role of nitric oxide in Alzheimer’s disease. Nitric Oxide Vol. 2023, 134–135, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Togo, T.; Katsuse, O.; Iseki, E. Nitric oxide pathways in Alzheimer’s disease and other neurodegenerative dementias. Neurol. Res. 2004, 26, 563–566. [Google Scholar] [CrossRef] [PubMed]
- Lal, R.; Singh, A.; Watts, S.; Chopra, K. Experimental models of Parkinson’s disease: Challenges and opportunities. Eur. J. Pharmacol. 2024, 980, 176819. [Google Scholar] [CrossRef] [PubMed]
- Langston, J.W.; Ballard, P.; Tetrud, J.; Irwin, I. Chronic parkinsonism in humans due to a product of meperidine-analog synthesis. Science 1983, 219, 979–980. [Google Scholar] [CrossRef] [PubMed]
- Tohyama, Y.; Sikirić, P.; Diksic, M. Effects of pentadecapeptide BPC157 on regional serotonin synthesis in the rat brain: Alpha-methyl-L-tryptophan autoradiographic measurements. Life Sci. 2004, 76, 345–357. [Google Scholar] [CrossRef] [PubMed]
- Stambolija, V.; Stambolija, T.P.; Holjevac, J.K.; Murselovic, T.; Radonic, J.; Duzel, V.; Duplancic, B.; Uzun, S.; Zivanovic-Posilovic, G.; Kolenc, D.; et al. BPC 157: The counteraction of succinylcholine, hyperkalemia, and arrhythmias. Eur. J. Pharmacol. 2016, 781, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Hrelec, M.; Klicek, R.; Brcic, L.; Brcic, I.; Cvjetko, I.; Seiwerth, S.; Sikiric, P. Abdominal aorta anastomosis in rats and stable gastric pentadecapeptide BPC 157, prophylaxis and therapy. J. Physiol. Pharmacol. 2009, 60 (Suppl. S7), 161–165. [Google Scholar] [PubMed]
- Barisic, I.; Balenovic, D.; Klicek, R.; Radic, B.; Nikitovic, B.; Drmic, D.; Udovicic, M.; Strinic, D.; Bardak, D.; Berkopic, L.; et al. Mortal hyperkalemia disturbances in rats are NO-system related. The life saving effect of pentadecapeptide BPC 157. Regul. Pept. 2013, 181, 50–66. [Google Scholar] [CrossRef] [PubMed]
- Perovic, D.; Kolenc, D.; Bilic, V.; Somun, N.; Drmic, D.; Elabjer, E.; Buljat, G.; Seiwerth, S.; Sikiric, P. Stable gastric pentadecapeptide BPC 157 can improve the healing course of spinal cord injury and lead to functional recovery in rats. J. Orthop. Surg. Res. 2019, 14, 199. [Google Scholar] [CrossRef] [PubMed]
- Tudor, M.; Jandric, I.; Marovic, A.; Gjurasin, M.; Perovic, D.; Radic, B.; Blagaic, A.B.; Kolenc, D.; Brcic, L.; Zarkovic, K.; et al. Traumatic brain injury in mice and pentadecapeptide BPC 157 effect. Regul. Pept. 2010, 160, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Klicek, R.; Kolenc, D.; Suran, J.; Drmic, D.; Brcic, L.; Aralica, G.; Sever, M.; Holjevac, J.; Radic, B.; Turudic, T.; et al. Stable gastric pentadecapeptide BPC 157 heals cysteamine-colitis and colon-colon-anastomosis and counteracts cuprizone brain injuries and motor disability. J. Physiol. Pharmacol. 2013, 64, 597–612. [Google Scholar] [PubMed]
- Jelovac, N.; Sikirić, P.; Rucman, R.; Petek, M.; Perović, D.; Konjevoda, P.; Marović, A.; Seiwerth, S.; Grabarević, Z.; Sumajstorcić, J.; et al. A novel pentadecapeptide.; BPC 157.; blocks the stereotypy produced acutely by amphetamine and the development of haloperidol-induced supersensitivity to amphetamine. Biol. Psychiatry 1998, 43, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Blagaic, A.B.; Blagaic, V.; Romic, Z.; Sikiric, P. The influence of gastric pentadecapeptide BPC 157 on acute and chronic ethanol administration in mice. Eur. J. Pharmacol. 2004, 499, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Boban Blagaic, A.; Blagaic, V.; Mirt, M.; Jelovac, N.; Dodig, G.; Rucman, R.; Petek, M.; Turkovic, B.; Anic, T.; Dubovecak, M.; et al. Gastric pentadecapeptide BPC 157 effective against serotonin syndrome in rats. Eur. J. Pharmacol. 2005, 512, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, K.; Mishima, K.; Egashira, N.; Al-Khatib, I.H.; Ishibashi, D.; Irie, K.; Kobayashi, H.; Egawa, T.; Fujiwara, M. Effect of nilvadipine on the cerebral ischemia-induced impairment of spatial memory and hippocampal apoptosis in rats. J. Pharmacol. Sci. 2003, 93, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Vorhees, C.V.; Williams, M.T. Morris water maze: Procedures for assessing spatial and related forms of learning and memory. Nat. Protoc. 2006, 1, 848–858. [Google Scholar] [CrossRef] [PubMed]
- Ilic, S.; Drmic, D.; Zarkovic, K.; Kolenc, D.; Brcic, L.; Radic, B.; Djuzel, V.; Blagaic, A.B.; Romic, Z.; Dzidic, S.; et al. Ibuprofen hepatic encephalopathy, hepatomegaly, gastric lesion and gastric pentadecapeptide BPC 157 in rats. Eur. J. Pharmacol. 2011, 667, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Ilic, S.; Drmic, D.; Zarkovic, K.; Kolenc, D.; Coric, M.; Brcic, L.; Klicek, R.; Radic, B.; Sever, M.; Djuzel, V.; et al. High hepatotoxic dose of paracetamol produces generalized convulsions and brain damage in rats. A counteraction with the stable gastric pentadecapeptide BPC 157 (PL 14736). J. Physiol. Pharmacol. 2010, 61, 241–250. [Google Scholar] [PubMed]
- Lojo, N.; Rasic, Z.; Zenko Sever, A.; Kolenc, D.; Vukusic, D.; Drmic, D.; Zoricic, I.; Sever, M.; Seiwerth, S.; Sikiric, P. Effect of diclofenac, L-NAME, L-arginine, and pentadecapeptide BPC 157 on gastrointestinal, liver and brain lesions, failed anastomosis, and intestinal adaptation deterioration in 24 h-short-bowel rats. PLoS ONE 2016, 11, e0162590. [Google Scholar] [CrossRef] [PubMed]
- Ilic, S.; Drmic, D.; Franjic, S.; Kolenc, D.; Coric, M.; Brcic, L.; Klicek, R.; Radic, B.; Sever, M.; Djuzel, V.; et al. Pentadecapeptide BPC 157 and its effects on a NSAID toxicity model: Diclofenac-induced gastrointestinal, liver, and encephalopathy lesions. Life Sci. 2011, 88, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Ilic, S.; Brcic, I.; Mester, M.; Filipovic, M.; Sever, M.; Klicek, R.; Barisic, I.; Radic, B.; Zoricic, Z.; Bilic, V.; et al. Over-dose insulin and stable gastric pentadecapeptide BPC 157. Attenuated gastric ulcers, seizures, brain lesions, hepatomegaly, fatty liver, breakdown of liver glycogen, profound hypoglycemia and calcification in rats. J. Physiol. Pharmacol. 2009, 60 (Suppl. S7), 107–114. [Google Scholar] [PubMed]
- Franco, P.G.; Silvestroff, L.; Soto, E.F.; Pasquini, J.M. Thyroid hormones promote differentiation of oligodendrocyte progenitor cells and improve remyelination after cuprizone-induced demyelination. Exp. Neurol. 2008, 212, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Guyenet, S.J.; Furrer, S.A.; Damian, V.M.; Baughan, T.D.; La Spada, A.R.; Garden, G.A. A simple composite phenotype scoring system for evaluating mouse models of cerebellar ataxia. J. Vis. Exp. 2010, 39, 1787. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M. Leaky gut: Mechanisms, measurement and clinical implications in humans. Gut. 2019, 68, 1516–1526. [Google Scholar] [CrossRef] [PubMed]
- Meijers, B.; Jouret, F.; Evenepoel, P. Linking gut microbiota to cardiovascular disease and hypertension: Lessons from chronic kidney disease. Pharmacol. Res. 2018, 133, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Obrenovich, M.E.M. Leaky gut, leaky brain? Microorganisms 2018, 6, 107. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.; Seo, M.; Berk, M.; Carvalho, A.; Maes, M. Gut permeability and microbiota in Parkinson’s disease: Role of depression, tryptophan catabolites, oxidative and nitrosative stress and melatonergic pathways. Curr. Pharm. Des. 2016, 22, 6142–6151. [Google Scholar] [CrossRef] [PubMed]
- Aleman, R.S.; Moncada, M.; Aryana, K.J. Leaky gut and the ingredients that help treat it: A review. Molecules 2023, 28, 619. [Google Scholar] [CrossRef] [PubMed]
- Ilan, Y. Leaky gut and the liver: A role for bacterial translocation in nonalcoholic steatohepatitis. World J. Gastroenterol. 2012, 18, 2609–2618. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.L.; Kalantar-Zadeh, K.; Vaziri, N.D. The gut as a source of inflammation in chronic kidney disease. Nephron J. 2015, 130, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Fändriks, L. Roles of the gut in the metabolic syndrome: An overview. J. Intern. Med. 2017, 281, 319–336. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Atkinson, M.A. The role for gut permeability in the pathogenesis of type 1 diabetes—A solid or leaky concept? Pediatr. Diabetes. 2015, 16, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Gupta, H.; Youn, G.S.; Shin, M.J.; Suk, K.T. Role of gut microbiota in hepatocarcinogenesis. Microorganisms 2019, 7, 121. [Google Scholar] [CrossRef] [PubMed]
- Saggioro, A. Leaky gut, microbiota, and cancer: An incoming hypothesis. J. Clin. Gastroenterol. 2014, 48 (Suppl. S1), S62–S66. [Google Scholar] [CrossRef] [PubMed]
- Demirtaş, H.; Özer, A.; Yıldırım, A.K.; Dursun, A.D.; Sezen, Ş.C.; Arslan, M. Protective effects of BPC 157 on liver, kidney, and lung distant organ damage in rats with experimental lower-extremity ischemia-reperfusion. Medicina 2025, 61, 291. [Google Scholar] [CrossRef] [PubMed]
- Ruenzi, M.; Stolte, M.; Veljaca, M.; Oreskovic, K.; Peterson, J. Ulcerative Colitis Study Group. A multicenter, randomized, double blind, placebo-controlled phase II study of PL 14736 enema in the treatment of mild-to-moderate ulcerative colitis. Gastroenterology 2005, 128, A584. [Google Scholar] [CrossRef]
- Xu, C.; Sun, L.; Ren, F.; Huang, P.; Tian, Z.; Cui, J.; Zhang, W.; Wang, S.; Zhang, K.; He, L.; et al. Preclinical safety evaluation of body protective compound-157, a potential drug for treating various wounds. Regul. Toxicol. Pharmacol. 2020, 114, 104665. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Feng, D.; Guo, H.; Zhou, Y.; Li, Z.; Zhang, K.; Zhang, W.; Wang, S.; Wang, Z.; Hao, Q.; et al. Pharmacokinetics, distribution, metabolism, and excretion of body-protective compound 157, a potential drug for treating various wounds, in rats and dogs. Front. Pharmacol. 2022, 13, 1026182. [Google Scholar] [CrossRef] [PubMed]
- Veljaca, M.; Pavic Sladoljev, D.; Mildner, B.; Brajsa, K.; Bubenik, M.; Stipanicic, S.; Parnham, M. Safety, tolerability and pharmacokinetics of PL14736, a novel agent for treatment of ulcerative colitis, in healthy male volunteers. Gut 2003, 51 (Suppl. SIII), A309. [Google Scholar] [CrossRef]
- Lee, E.; Burgess, K. Safety of intravenous infusion of BPC157 in humans: A pilot study. Altern. Ther. Health Med. 2025, AT11513. Online ahead of print. [PubMed]
- Sikiric, P.; Krstonijevic, Z.; Sever, M.; Lojo, N.; Drmic, D.; Zenko Sever, A.; Baric, M.; Starcevic, N.; Buljan, M.; Zoricic, I.; et al. Pentadecapeptide BPC 157 given intraarticularly counteracts knee osteoarthritis in rats. FASEB J. 2014, 28 (Suppl. S1), 844.11. [Google Scholar] [CrossRef]
- Lee, E.; Padgett, B. Intra-articular injection of BPC 157 for multiple types of knee pain. Altern. Ther. Health Med. 2021, 27, 8–13. [Google Scholar] [PubMed]
- Lee, E.; Walker, C.; Ayadi, B. Effect of BPC-157 on symptoms in patients with interstitial cystitis: A pilot study. Altern. Ther. Health Med. 2024, 30, 12–17. [Google Scholar] [PubMed]
- Jandric, I.; Vrcic, H.; Jandric Balen, M.; Kolenc, D.; Brcic, L.; Radic, B.; Drmic, D.; Seiwerth, S.; Sikiric, P. Salutary effect of gastric pentadecapeptide BPC 157 in two different stress urinary incontinence models in female rats. Med. Sci. Monit. Basic Res. 2013, 19, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Rasic, D.; Zenko Sever, A.; Rasic, F.; Strbe, S.; Rasic, Z.; Djuzel, A.; Duplancic, B.; Boban Blagaic, A.; Skrtic, A.; Seiwerth, S.; et al. Stable gastric pentadecapeptide BPC 157 heals established vesicovaginal fistula and counteracts stone formation in rats. Biomedicines 2021, 9, 1206. [Google Scholar] [CrossRef] [PubMed]
- Grgic, T.; Grgic, D.; Drmic, D.; Sever, A.Z.; Petrovic, I.; Sucic, M.; Kokot, A.; Klicek, R.; Sever, M.; Seiwerth, S.; et al. Stable gastric pentadecapeptide BPC 157 heals rat colovesical fistula. Eur. J. Pharmacol. 2016, 780, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Baric, M.; Sever, A.Z.; Vuletic, L.B.; Rasic, Z.; Sever, M.; Drmic, D.; Pavelic-Turudic, T.; Sucic, M.; Vrcic, H.; Seiwerth, S.; et al. Stable gastric pentadecapeptide BPC 157 heals rectovaginal fistula in rats. Life Sci. 2016, 148, 63–70. [Google Scholar] [CrossRef] [PubMed]
- October 29, 2024: Meeting of the Pharmacy Compounding Advisory Committee. 2024. Available online: https://www.fda.gov/advisory-committees/advisory-committee-calendar/october-29-2024-meeting-pharmacy-compounding-advisory-committee-10292024 (accessed on 18 March 2025).
- Updated Meeting Time and Public Participation Information. December 4, 2024: Meeting of the Pharmacy Compounding Advisory Committee. 2024. Available online: https://www.fda.gov/advisory-committees/advisory-committee-calendar/updated-meeting-time-and-public-participation-information-december-4-2024-meeting-pharmacy (accessed on 18 March 2025).
- Leenaars, C.H.C.; Teerenstra, S.; Meijboom, F.L.B.; Bleich, A. Methodical advances in reproducibility research: A proof of concept qualitative comparative analysis of reproducing animal data in humans. J. Neurosci. Methods 2023, 397, 109931. [Google Scholar] [CrossRef] [PubMed]
- Dirven, H.; Vist, G.E.; Bandhakavi, S.; Mehta, J.; Fitch, S.E.; Pound, P.; Ram, R.; Kincaid, B.; Leenaars, C.H.C.; Chen, M.; et al. Performance of preclinical models in predicting drug-induced liver injury in humans: A systematic review. Sci Rep. 2021, 11, 6403. [Google Scholar] [CrossRef] [PubMed]
- Leenaars, C.H.C.; Kouwenaar, C.; Stafleu, F.R.; Bleich, A.; Ritskes-Hoitinga, M.; De Vries, R.B.-M.; Meijboom, F.L.B. Animal to human translation: A systematic scoping review of reported concordance rates. J. Transl. Med. 2019, 17, 223. [Google Scholar] [CrossRef] [PubMed]
- Litchfield, J.T., Jr. Symposium on clinical drug evaluation and human pharmacology. XVI. Evaluation of the safety of new drugs by means of tests in animals. Clin. Pharmacol. Ther. 1962, 3, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Schooler, N.R. Negative symptoms in schizophrenia: A review and clinical guide for recognition, assessment, and treatment. Neuropsychiatr. Dis. Treat. 2020, 16, 519–534. [Google Scholar] [CrossRef] [PubMed]
- Krystal, J.H.; Karper, L.P.; Seibyl, J.P.; Freeman, G.K.; Delaney, R.; Bremner, J.D.; Heninger, G.R.; Bowers, M.B., Jr.; Charney, D.S. Subanesthetic effects of the noncompetitive NMDA antagonist, ketamine, in humans: Psychotomimetic, perceptual, cognitive, and neuroendocrine responses. Arch. Gen. Psychiatry 1994, 51, 199–214. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, A. The flaws and human harms of animal experimentation. Camb. Q. Healthc. Ethics 2015, 24, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Udovicic, M.; Sever, M.; Kavur, L.; Loncaric, K.; Barisic, I.; Balenovic, D.; Zivanovic Posilovic, G.; Strinic, D.; Uzun, S.; Batelja Vuletic, L.; et al. Stable gastric pentadecapeptide BPC 157 therapy for monocrotaline-induced pulmonary hypertension in rats leads to prevention and reversal. Biomedicines 2021, 9, 822. [Google Scholar] [CrossRef] [PubMed]
- Vitaic, S.; Stupnisek, M.; Drmic, D.; Bauk, L.; Kokot, A.; Klicek, R.; Vcev, A.; Luetic, K.; Seiwerth, S.; Sikiric, P. Nonsteroidal anti-inflammatory drugs-induced failure of lower esophageal and pyloric sphincter and counteraction of sphincters failure with stable gastric pentadecapeptide BPC 157 in rats. J. Physiol. Pharmacol. 2017, 68, 265–272. [Google Scholar] [PubMed]
- Skorjanec, S.; Kokot, A.; Drmic, D.; Radic, B.; Sever, M.; Klicek, R.; Kolenc, D.; Zenko, A.; Lovric Bencic, M.; Belosic Halle, Z.; et al. Duodenocutaneous fistula in rats as a model for “wound healing-therapy” in ulcer healing: The effect of pentadecapeptide BPC 157, L-nitro-arginine methyl ester and L-arginine. J. Physiol. Pharmacol. 2015, 66, 581–590. [Google Scholar] [PubMed]
- Cesarec, V.; Becejac, T.; Misic, M.; Djakovic, Z.; Olujic, D.; Drmic, D.; Brcic, L.; Rokotov, D.S.; Seiwerth, S.; Sikiric, P. Pentadecapeptide BPC 157 and the esophagocutaneous fistula healing therapy. Eur. J. Pharmacol. 2013, 701, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, I.; Dobric, I.; Drmic, D.; Sever, M.; Klicek, R.; Radic, B.; Brcic, L.; Kolenc, D.; Zlatar, M.; Kunjko, K.; et al. BPC 157 therapy to detriment sphincters failure-esophagitis-pancreatitis in rat and acute pancreatitis patients low sphincters pressure. J. Physiol. Pharmacol. 2011, 62, 527–534. [Google Scholar] [PubMed]
- Klicek, R.; Sever, M.; Radic, B.; Drmic, D.; Kocman, I.; Zoricic, I.; Vuksic, T.; Ivica, M.; Barisic, I.; Ilic, S.; et al. Pentadecapeptide BPC 157, in clinical trials as a therapy for inflammatory bowel disease (PL14736), is effective in the healing of colocutaneous fistulas in rats: Role of the nitric oxide-system. J. Pharmacol. Sci. 2008, 108, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Dobric, I.; Drvis, P.; Petrovic, I.; Shejbal, D.; Brcic, L.; Blagaic, A.B.; Batelja, L.; Sever, M.; Kokic, N.; Tonkic, A.; et al. Prolonged esophagitis after primary dysfunction of the pyloric sphincter in the rat and therapeutic potential of the gastric pentadecapeptide BPC 157. J. Pharmacol. Sci. 2007, 104, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, I.; Dobric, I.; Drvis, P.; Shejbal, D.; Brcic, L.; Blagaic, A.B.; Batelja, L.; Kokic, N.; Tonkic, A.; Mise, S.; et al. An experimental model of prolonged esophagitis with sphincter failure in the rat and the therapeutic potential of gastric pentadecapeptide BPC 157. J. Pharmacol. Sci. 2006, 102, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Prkacin, I.; Separovic, J.; Aralicia, G.; Perovic, D.; Gjurasin, M.; Lovric-Bencic, M.; Stancic-Rokotov, D.; Staresinic, M.; Anic, T.; Mikus, D.; et al. Portal hypertension and liver lesions in chronically alcohol drinking rats prevented and reversed by stable gastric pentadecapeptide BPC 157 (PL-10.; PLD-116), and propranolol, but not ranitidine. J. Physiol. Paris. 2001, 95, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Mikus, D.; Sikiric, P.; Seiwerth, S.; Petricevic, A.; Aralica, G.; Druzijancic, N.; Rucman, R.; Petek, M.; Pigac, B.; Perovic, D.; et al. Pentadecapeptide BPC 157 cream improves burn-wound healing and attenuates burn-gastric lesions in mice. Burns 2001, 27, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Gjurasin, M.; Miklic, P.; Zupancic, B.; Perovic, D.; Zarkovic, K.; Brcic, L.; Kolenc, D.; Radic, B.; Seiwerth, S.; Sikiric, P. Peptide therapy with pentadecapeptide BPC 157 in traumatic nerve injury. Regul. Pept. 2010, 160, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Seiwerth, S.; Aralica, G.; Perovic, D.; Staresinic, M.; Anic, T.; Gjurasin, M.; Prkacin, I.; Separovic, J.; Stancic-Rokotov, D.; et al. Therapy effect of antiulcer agents on new chronic cysteamine colon lesion in rat. J. Physiol. Paris 2001, 95, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Sikiric, P.; Seiwerth, S.; Grabarevic, Z.; Balen, I.; Aralica, G.; Gjurasin, M.; Komericki, L.; Perovic, D.; Ziger, T.; Anic, T.; et al. Cysteamine-colon and cysteamine-duodenum lesions in rats. Attenuation by gastric pentadecapeptide BPC 157, cimetidine, ranitidine, atropine, omeprazole, sulphasalazine and methylprednisolone. J. Physiol. Paris 2001, 95, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Sebecić, B.; Nikolić, V.; Sikirić, P.; Seiwerth, S.; Sosa, T.; Patrlj, L.; Grabarević, Z.; Rucman, R.; Petek, M.; Konjevoda, P.; et al. Osteogenic effect of a gastric pentadecapeptide, BPC-157, on the healing of segmental bone defect in rabbits: A comparison with bone marrow and autologous cortical bone implantation. Bone 1999, 24, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Xue, X.C.; Wu, Y.J.; Gao, M.T.; Li, W.G.; Zhao, N.; Wang, Z.L.; Bao, C.J.; Yan, Z.; Zhang, Y.Q. Protective effects of pentadecapeptide BPC 157 on gastric ulcer in rats. World J. Gastroenterol. 2004, 10, 1032–1036. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.W. A historical view of the stress field. J. Human Stress 1975, 1, 22–36. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.W. A historical view of the stress field. J. Human Stress 1975, 1, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.T. The pituitary-adrenal axis. In Discoveries in Pharmacology, Volume 2: Hemodynamics, Hormones & Inflammation; Parnham, M.J., Bruinvels, J., Eds.; Elsevier Science Publisher: Amsterdam, The Netherlands, 1984; pp. 285–305. [Google Scholar]
- Grabarevic, Z.; Tisljar, M.; Artukovic, B.; Bratulic, M.; Dzaja, P.; Seiwerth, S.; Sikiric, P.; Peric, J.; Geres, D.; Kos, J. The influence of BPC 157 on nitric oxide agonist and antagonist induced lesions in broiler chicken. J. Physiol. Paris 1997, 91, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Tlak Gajger, I.; Smodiš Škerl, M.I.; Šoštarić, P.; Šuran, J.; Sikirić, P.; Vlainić, J. Physiological and immunological status of adult honeybees (Apis mellifera) fed sugar syrup supplemented with pentadecapeptide BPC 157. Biology 2021, 10, 891. [Google Scholar] [CrossRef] [PubMed]
- Tlak Gajger, I.; Ribarić, J.; Smodiš Škerl, M.; Vlainić, J.; Sikirić, P. Stable gastric pentadecapeptide BPC 157 in honeybee (Apis mellifera) therapy, to control Nosema ceranae invasions in apiary conditions. J. Vet. Pharmacol. Ther. 2018, 41, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Filosevic, A.; Andretic Waldowski, R.; Sikiric, P.; Drmic, D. Stable gastric pentadecapeptide BPC 157 antagonizes hydrogen peroxide induced oxidative stress in Drosophila melanogaster. FASEB J. 2018, 31 (Suppl. S1), 667.14. [Google Scholar] [CrossRef]
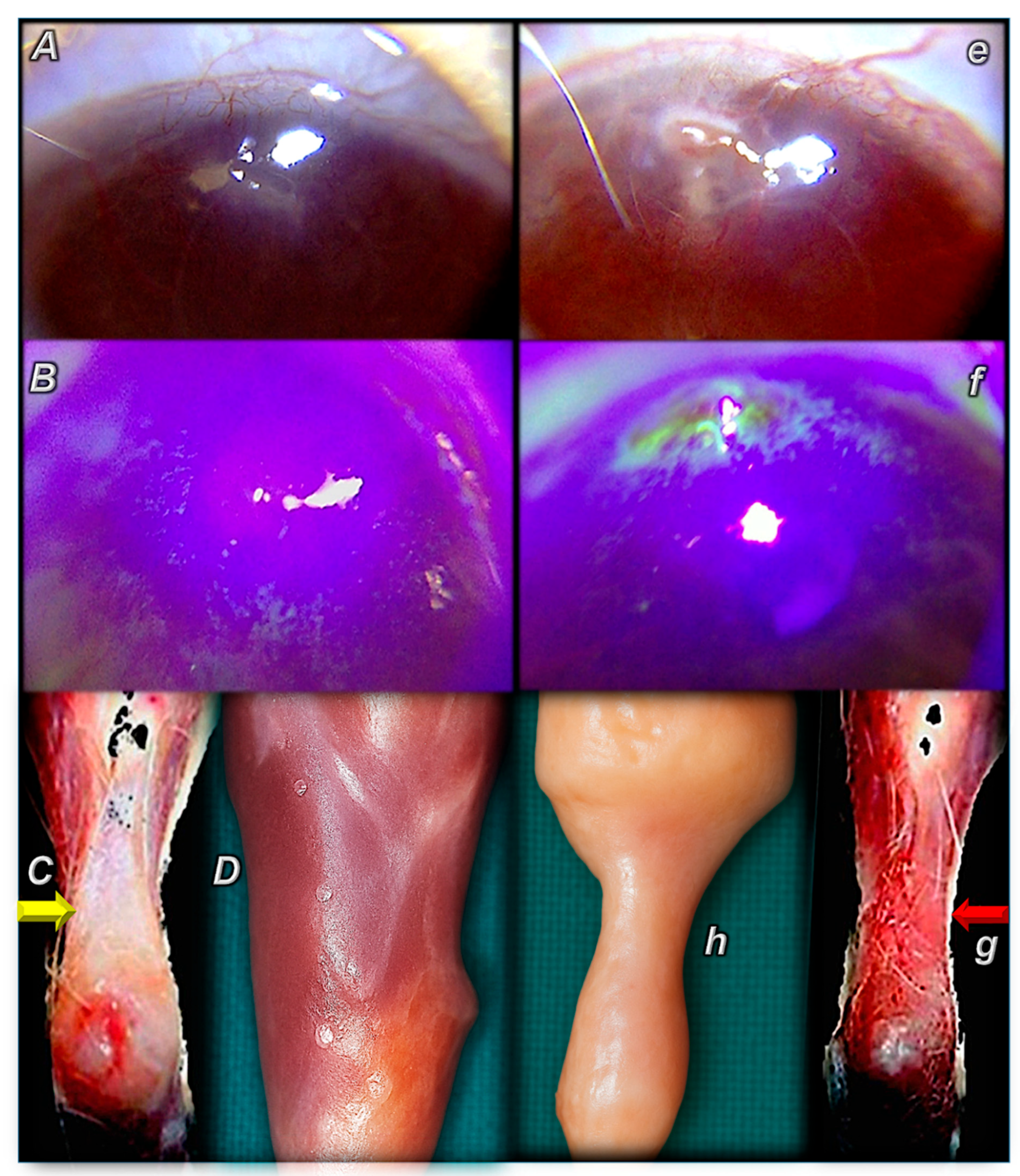
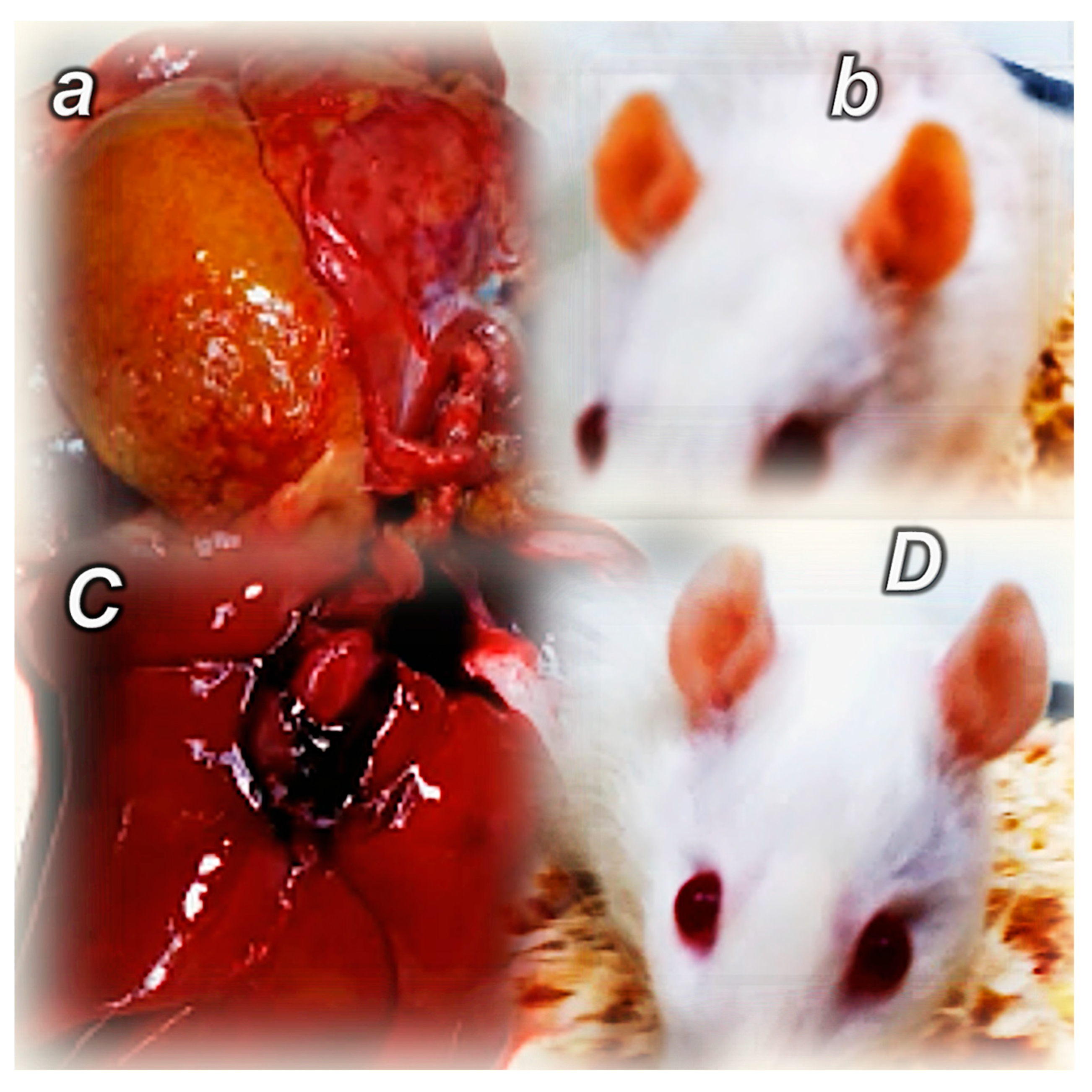
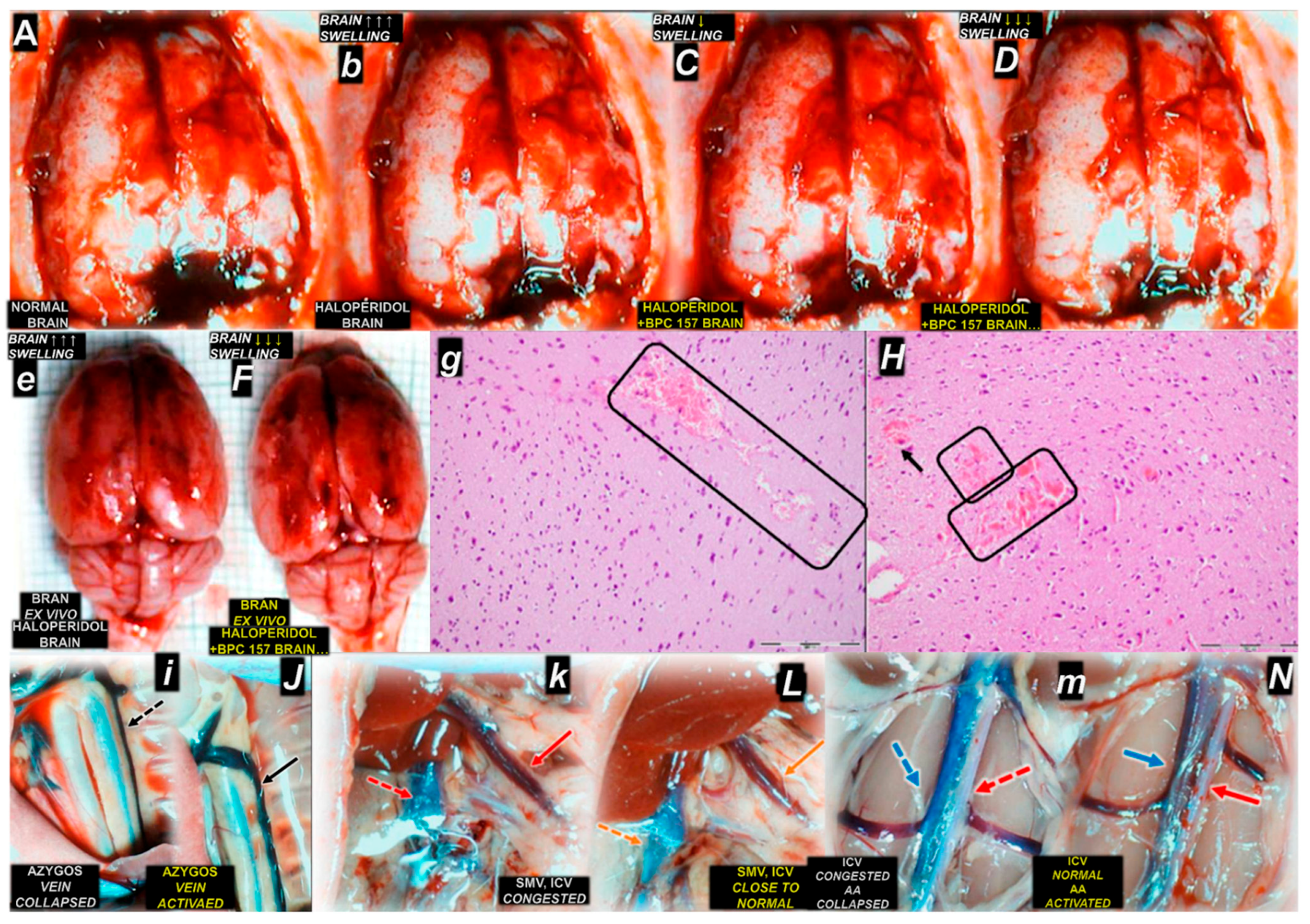
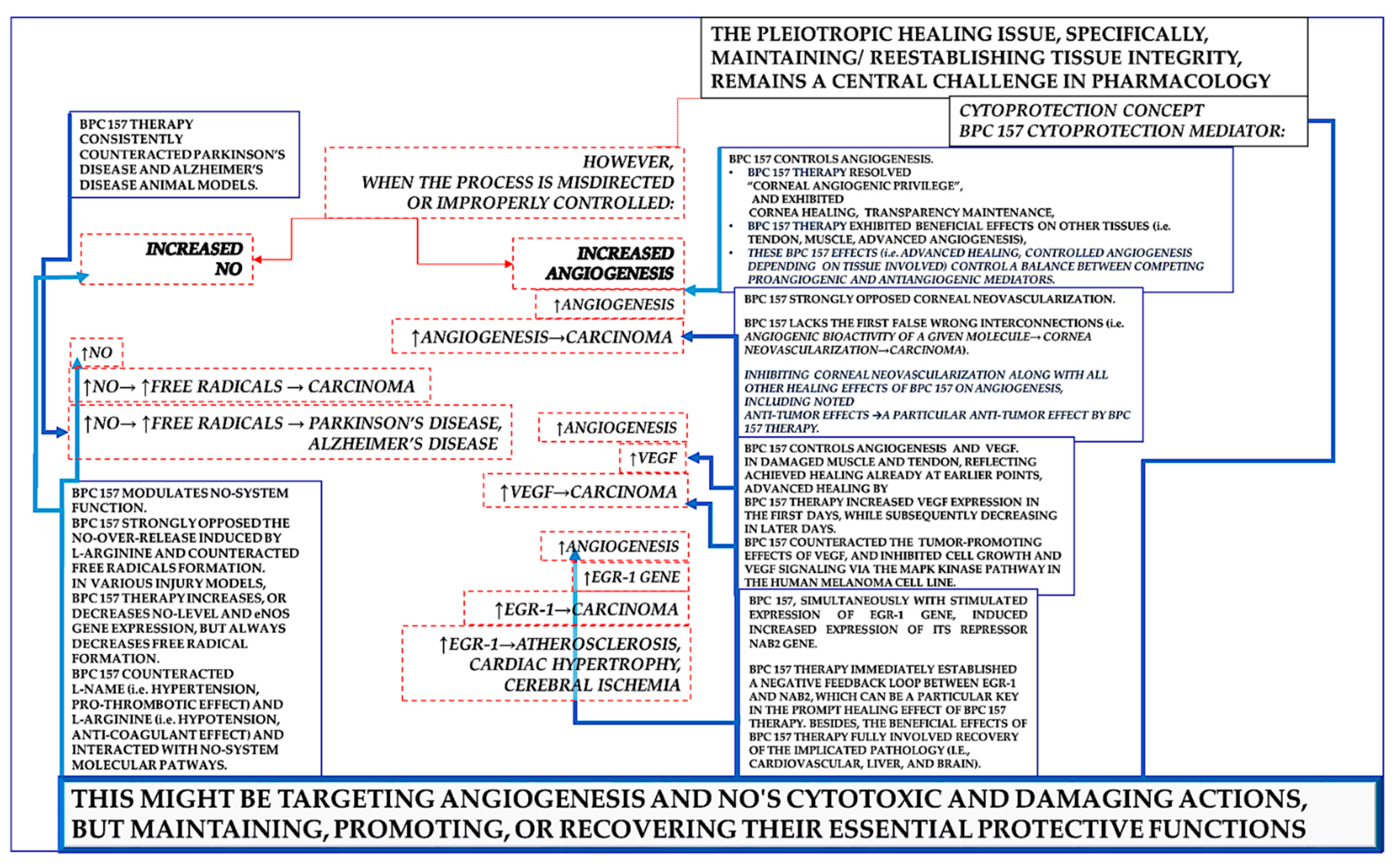

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Multifunctionality and Possible Medical Application of Stable Gastric Pentadecapeptide BPC 157, as Seen in the Presented Reviews [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40] | |
|---|---|
| Józwiak et al. Multifunctionality and possible medical application of the BPC 157 peptide-literature and patent review. doi: 10.3390/ph18020185. PMID: 40005999 [1] | Pharmaceuticals (Basel). 2025;18(2):185. |
| DeFoor and Dekker. Injectable therapeutic peptides—an adjunct to regenerative medicine and sports performance? [2] | Arthroscopy. 2025 Feb;41(2):150–152. |
| Grubisic et al. Stable gastric pentadecapeptide BPC 157 as a therapy of severe electrolyte disturbances in rats. [3] | Curr Neuropharmacol. 2025 Jan 24. doi: 10.2174/011570159X349612241205065330. Online ahead of print. PMID: 39865815 |
| Sikiric et al. New studies with stable gastric pentadecapeptide protecting gastrointestinal tract. Significance of counteraction of vascular and multiorgan failure of occlusion/occlusion-like syndrome in cytoprotection/organoprotection. [4] | Inflammopharmacology. 2024 Oct;32(5):3119–3161. |
| Bajramagic et al. Stable gastric pentadecapeptide BPC 157 and intestinal anastomoses therapy in rats—a review. [5] | Pharmaceuticals (Basel). 2024 Aug 17;17(8):1081. |
| Sikiric et al. The stable gastric pentadecapeptide BPC 157 pleiotropic beneficial activity and possible relations with neurotransmitter activity. [6] | Pharmaceuticals (Basel). 2024 Apr 3;17(4):461. |
| Sikiric et al. From Selye’s and Szabo’s cysteamine-duodenal ulcer in rats to dopamine in the stomach: Therapy significance and possibilities. [7] | Pharmaceuticals (Basel). 2023 Dec 7;16(12):1699. |
| Sikiric et al. Stable gastric pentadecapeptide BPC 157—possible novel therapy of glaucoma and other ocular conditions. [8] | Pharmaceuticals (Basel). 2023 Jul 24;16(7):1052. |
| Sikiric et al. Stable gastric pentadecapeptide BPC 157 may recover brain-gut axis and gut-brain axis function. [9] | Pharmaceuticals (Basel). 2023 Apr 30;16(5):676. |
| Sikiric et al. Stable gastric pentadecapeptide BPC 157: Prompt particular activation of collateral pathways. [10] | Curr Med Chem. 2023;30(13):1568–1573. |
| Sikiric; et al. Stable gastric pentadecapeptide BPC 157 and NO-system [11] | In: Nitric Oxide: From Research to Therapeutics, Advances in Biochemistry in Health and Disease 22; Ray, A., Gulati, K., Eds.; Springer Nature: Cham, Switzerland, 2023; pp. 349–375. |
| Staresinic et al. Stable gastric pentadecapeptide BPC 157 and striated, smooth, and heart muscle. [12] | Biomedicines. 2022 Dec 12;10(12):3221. |
| Sikiric et al. Stable gastric pentadecapeptide BPC 157 as useful cytoprotective peptide therapy in the heart disturbances, myocardial infarction, heart failure, pulmonary hypertension, arrhythmias, and thrombosis presentation. [13] | Biomedicines. 2022 Oct 25;10(11):2696. |
| Vukojevic et al. Pentadecapeptide BPC 157 and the central nervous system. [14] | Neural Regen Res. 2022 Mar;17(3):482–487. |
| Deek. BPC 157 as potential treatment for COVID-19. [15] | Med Hypotheses. 2021 Nov 9;158:110736. |
| Seiwerth et al. Stable gastric pentadecapeptide BPC 157 and wound healing. [16] | Front Pharmacol. 2021 Jun 29;12:627533. |
| Sikiric et al. Stable gastric pentadecapeptide BPC 157, Robert’s stomach cytoprotection/adaptive cytoprotection/organoprotection, and Selye’s stress coping response: Progress, achievements, and the future. [17] | Gut Liver. 2020 Mar 15;14(2):153–167. |
| Park et al. BPC 157 rescued NSAID-cytotoxicity via stabilizing intestinal permeability and enhancing cytoprotection. [18] | Curr Pharm Des. 2020;26(25):2971–2981. |
| Sikiric et al. Fistulas healing. Stable gastric pentadecapeptide BPC 157 therapy. [19] | Curr Pharm Des. 2020;26(25):2991–3000. |
| Gwyer et al. Gastric pentadecapeptide body protection compound BPC 157 and its role in accelerating musculoskeletal soft tissue healing. [20] | Cell Tissue Res. 2019 Aug;377(2):153–159. |
| Seiwerth et al. BPC 157 and standard angiogenic growth factors. Gastrointestinal tract healing, lessons from tendon, ligament, muscle and bone healing. [21] | Curr Pharm Des. 2018;24(18):1972–1989. |
| Kang et al. BPC157 as potential agent rescuing from cancer cachexia. [22] | Curr Pharm Des. 2018;24(18):1947–1956. |
| Sikiric et al. Novel cytoprotective mediator, stable gastric pentadecapeptide BPC 157. Vascular recruitment and gastrointestinal tract healing. [23] | Curr Pharm Des. 2018;24(18):1990–2001. |
| Sikiric et al. Stress in gastrointestinal tract and stable gastric pentadecapeptide BPC 157. Finally, do we have a solution? [24] | Curr Pharm Des. 2017;23(27):4012–4028. |
| Szabo et al. “Stress” is 80 years old: From Hans Selye original paper in 1936 to recent advances in GI ulceration. [25] | Curr Pharm Des. 2017;23(27):4029–4041. |
| Gyires and Feher A. Stress, neuropeptides and gastric mucosa. [26] | Curr Pharm Des. 2017;23(27):3928–3940. |
| Sikiric et al. Brain-gut axis and pentadecapeptide BPC 157: Theoretical and practical implications. [27] | Curr Neuropharmacol. 2016;14(8):857–865. |
| Seiwerth et al. BPC 157 and blood vessels. [28] | Curr Pharm Des. 2014;20(7):1121–5. |
| Sikiric et al. Stable gastric pentadecapeptide BPC 157-NO-system relation. [29] | Curr Pharm Des. 2014;20(7):1126–35 |
| Sikiric et al. Toxicity by NSAIDs. Counteraction by stable gastric pentadecapeptide BPC 157. [30] | Curr Pharm Des. 2013;19(1):76–83. |
| Sikiric et al. Focus on ulcerative colitis: stable gastric pentadecapeptide BPC 157. [31] | Curr Med Chem. 2012;19(1):126–32. |
| Sikiric et al. Stable gastric pentadecapeptide BPC 157: novel therapy in gastrointestinal tract. [32] | Curr Pharm Des. 2011;17(16):1612–32. |
| Mózsik et al. Approaches to gastrointestinal cytoprotection: from isolated cells, via animal experiments to healthy human subjects and patients with different gastrointestinal disorders. [33] | Curr. Pharm. Des. 2011,17(16),1556–1572. |
| Sikiric et al. Revised Robert’s cytoprotection and adaptive cytoprotection and stable gastric pentadecapeptide BPC 157. Possible significance and implications for novel mediator. [34] | Curr Pharm Des. 2010;16(10):1224–34. |
| Mózsik. Gastric cytoprotection 30 years after its discovery by Andre Robert: a personal perspective. [35] | Inflammopharmacology 2010,18(5),209–221. |
| Mózsik et al. Gastrointestinal cytoprotection: from basic science to clinical perspectives. [36] | Inflammopharmacology 2007,15(2),49–60. |
| Sikiric et al. Stable gastric pentadecapeptide BPC 157 in trials for inflammatory bowel disease (PL-10, PLD-116, PL 14736, Pliva, Croatia). Full and distended stomach, and vascular response. [37] | Inflammopharmacology. 2006 Dec;14(5–6):214–21. |
| Wood. The first Nobel prize for integrated systems physiology: Ivan Petrovich Pavlov, 1904. [38] | Physiology, 2004,19(6),326–330. |
| Sikiric The pharmacological properties of the novel peptide BPC 157 (PL-10). [39] | Inflammopharmacology. 1999;7(1):1–14. |
| Sikiric et al. A new gastric juice peptide, BPC. An overview of the stomach-stress-organoprotection hypothesis and beneficial effects of BPC. [40] | J Physiol Paris. 1993;87(5):313–27 |
| References | Organ System | Dose and Protocol | Model | Key Findings |
|---|---|---|---|---|
| Masnec et al. Perforating corneal injury in rat and pentadecapeptide BPC 157. Exp. Eye Res. 2015, 136, 9–15. [76] | Cornea | After injury induction, BPC 157 therapy successfully closed perforating corneal incisions in rats and rapidly restored corneal transparency. This effect is quite consistent given the regimens used, i.e., 2 pg/mL, 2 ng/mL, and 2 µg/mL distilled water, two eye drops/left rat eye immediately after injury induction, and then every 8 h up to 120 h. | Perforating corneal injury | BPC 157 therapy cured severe corneal lesions and maintained corneal transparency. All controls developed new vessels that grew from the limbus to the penetrated area and had no transparency. Contrarily, BPC 157-treated rats generally had no new vessels, and those that did form in the limbus did not make contact with the penetrated area. |
| Staresinic et al. Gastric pentadecapeptide BPC 157 accelerates healing of transected rat Achilles tendon and in vitro stimulates tendocytes growth. J. Orthop. Res. 2003, 21(6), 976–983. [90] | Achilles tendon | Agents (/kg b.w., i.p., once time daily) (BPC 157 (dissolved in saline, with no carrier addition) (10 microg, 10 ng or 10 pg) or saline (5.0 mL)) were firstly applied 30 min after surgery, with the last application 24 h before autopsy. | Transected Achilles tendon | Pentadecapeptide BPC 157 fully improves recovery: (i) biomechanically, increased load of failure, load of failure per area, and Young’s modulus of elasticity; (ii) functionally, significantly higher AFI values; (iii) microscopically, more mononuclears and less granulocytes, superior formation of fibroblasts, reticulin, and collagen; (iv) macroscopically, smaller size and depth of tendon defect, and, subsequently, the reestablishment of full tendon integrity. Unlike the damaged cornea [74,75,76,77], in the healing of transected Achilles tendon already at postoperative day 4, BPC 157-treated rats have large fields of dense mature collagen, illustrating well the consistent organ-specific healing effect’s cellularity, and well-formed capillaries and small vessels [88], while control rats exhibit only some young capillaries. |
| Sever et al. Stable gastric pentadecapeptide BPC 157 in the therapy of the rats with bile duct ligation. Eur. J. Pharmacol. 2019, 847, 130–142. [118] | Liver | In bile duct occluded rats, in an 8-week study, BPC 157 (10 µg/kg, 10 ng/kg) was given continuously (intraperitoneally once a day or perorally (continuously in drinking water)) or only once as a direct bath application. | Bile duct ligation- induced liver cirrhosis | Liver weight was not increased, and ascites was eliminated. Microscopy presentation documented the smaller intensity of architectural changes (fibrosis and cirrhosis); lower necroinflammatory score; smaller alpha-smooth muscle actin (α-SMA) distribution; and smaller Ki-67 distribution. Smaller were serum enzymes and bilirubin values. Normalized were MDA- and NO-levels in the liver, next to Western blot of NOS2 and NOS3 in the liver tissue and decreased IL-6, TNF-α, and IL-1β levels in liver tissues. Annihilation of portal hypertension consistently occurred. Despite bile duct ligation, portal pressure did not develop. With late application of BPC 157 therapy in bile duct ligated rats with already advanced liver cirrhosis, portal hypertension disappeared and did not reappear. |
| Response | Target |
|---|---|
| L-NAME R, L-arginine R Opposite, specific | Perforated cecum: vessel presentation, bleeding; Cyclophosphamide: hemorrhagic cystitis; short bowel: liver lesions, brain lesions; Celecoxib: gastric lesions, liver lesions; esophagogastric anastomosis: anastomosis strength, “esophageal sphincter” function, pyloric sphincter function; tail amputation: bleeding; Warfarin: bleeding; duodenocutaneous fistula: duodenal defect, skin defect, fistula, lethality; esophagocutaneous fistula: esophageal defect, skin defect, esophagocutaneous fistula leaking; Intra(per)-oral/intragastric strong alcohol in rat: tongue lesions, gastric lesions, duodenal lesions, lower esophageal pressure; mortal hyperkalemia: survival and life-saving potential, arrhythmias, hypertension, lower esophageal sphincter pressure, blood pressure; in vitro in stomach tissue homogenates: NO generation; left colic artery and vein ligation: arcade vessel; parietal peritoneum excision with an underlying superficial layer of muscle tissue in rats: increased adhesion formation; ketamine-induced: anhedonia |
| L-NAME R, L-arginine NR Opposite, specific | Short bowel: gastrointestinal lesions, failed anastomosis healing, intestinal adaptation deterioration; Cyclophosphamide: gastric lesions, duodenal lesions; colocutaneous fistula: colon defect, skin defect, fistula; mortal hyperkalemia: muscular disability |
| L-NAME NR, L-arginine R Opposite, specific | Celecoxib: brain lesions; heparin: bleeding; Apomorphine, MK-801, haloperidol, methamphetamine: apomorphine-induced disturbances, MK-801-induced locomotion, stereotyped sniffing, ataxia disturbances, haloperidol-induced catalepsy, methamphetamine-induced disturbances; mortal hyperkalemia: pyloric sphincter pressure; intragastric alcohol: stomach lesions; ketamine-induced: cognitive dysfunction |
| L-NAME R, L-arginine R Opposite, non-specific | Esophagogastric anastomosis: esophagitis lesions, gastric lesions, lethality; esophagocutaneous fistula: lower esophageal sphincter pressure; ketamine-induced: social withdrawal |
| L-NAME R, L-arginine NR Opposite, non-specific | Thiopental: anesthesia |
| L-NAME NR, L-arginine NR Not relevant | Perforated cecum: cecum lesion; Cyclophosphamide: leak point pressure; tail amputation: APTT-, TT- values; heparin: APTT-, TT-values; Warfarin: thrombocytopenia, PT-values; intra(per)-oral/intragastric strong alcohol in rat: pyloric sphincter pressure; mortal hyperkalemia: serum electrolyte values; superior anterior pancreaticoduodenal vein ligation: vessels |
| L-NAME R, L-arginine R¸ Parallel, specific | Superior anterior pancreaticoduodenal vein ligation: duodenal lesions; hypermagnesemia: muscle weakness, muscle lesions, brain lesions, hypermagnesemia, hyperkalemia; tail amputation: thrombocytopenia; heparin: thrombocytopenia; lidocaine: lidocaine-induced local anesthesia via intraplantar application, lidocaine-induced axillary block, lidocaine-induced spinal (L4-L5) intrathecal block; left colic artery and vein ligation: colon lesions; parietal peritoneum excision with an underlying superficial layer of muscle tissue in rats: failed vasculature; ketamine-induced: anxiety |
| L-NAME R, L-arginine R Parallel, non-specific | Normal pupil: miosis; atropine-induced: mydriasis; dopamine antagonists: lower esophageal sphincter pressure, pyloric sphincter pressure; amphetamine: amphetamine-induced disturbances; acute alcohol intoxication: behavior, temperature, alcohol level in blood; alcohol: withdrawal; broiler chicken: pulmonary hypertension syndrome |
| Parameter | Unit | Males | Females | Males +Females |
|---|---|---|---|---|
| Time of maximum concentration (tmax) | h | 8 | 3 | 3 |
| Maximum concentration (Cmax) | µg eq./mL | 10.36 | 10.90 | 10.53 |
| Area under the curve (AUC) | h·µg eq./mL | 988 | 1058 | 1023 |
| Half-life (t1/2) | h | 66 | 69 | 68 |
| Mean residence time (MRT) | h | 91 | 94 | 93 |
| Index of bioavailability (F) | - | 1.1 | 1.2 | 1.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sikiric, P.; Seiwerth, S.; Skrtic, A.; Staresinic, M.; Strbe, S.; Vuksic, A.; Sikiric, S.; Bekic, D.; Soldo, D.; Grizelj, B.; et al. Stable Gastric Pentadecapeptide BPC 157 as a Therapy and Safety Key: A Special Beneficial Pleiotropic Effect Controlling and Modulating Angiogenesis and the NO-System. Pharmaceuticals 2025, 18, 928. https://doi.org/10.3390/ph18060928
Sikiric P, Seiwerth S, Skrtic A, Staresinic M, Strbe S, Vuksic A, Sikiric S, Bekic D, Soldo D, Grizelj B, et al. Stable Gastric Pentadecapeptide BPC 157 as a Therapy and Safety Key: A Special Beneficial Pleiotropic Effect Controlling and Modulating Angiogenesis and the NO-System. Pharmaceuticals. 2025; 18(6):928. https://doi.org/10.3390/ph18060928
Chicago/Turabian StyleSikiric, Predrag, Sven Seiwerth, Anita Skrtic, Mario Staresinic, Sanja Strbe, Antonia Vuksic, Suncana Sikiric, Dinko Bekic, Dragan Soldo, Boris Grizelj, and et al. 2025. "Stable Gastric Pentadecapeptide BPC 157 as a Therapy and Safety Key: A Special Beneficial Pleiotropic Effect Controlling and Modulating Angiogenesis and the NO-System" Pharmaceuticals 18, no. 6: 928. https://doi.org/10.3390/ph18060928
APA StyleSikiric, P., Seiwerth, S., Skrtic, A., Staresinic, M., Strbe, S., Vuksic, A., Sikiric, S., Bekic, D., Soldo, D., Grizelj, B., Novosel, L., Beketic Oreskovic, L., Oreskovic, I., Stupnisek, M., Boban Blagaic, A., & Dobric, I. (2025). Stable Gastric Pentadecapeptide BPC 157 as a Therapy and Safety Key: A Special Beneficial Pleiotropic Effect Controlling and Modulating Angiogenesis and the NO-System. Pharmaceuticals, 18(6), 928. https://doi.org/10.3390/ph18060928