
The Potential of Artificial Intelligence in Pharmaceutical Innovation: From Drug Discovery to Clinical Trials



Abstract

1. Introduction
2. Artificial Intelligence
2.1. From the Beginning of AI to the Present Day

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Progress Information | References |
|---|---|---|
| 1955 | Allen Newell, J.C. Shaw, and Herbert A. Simon created a program called the “Logic Theorist”, the first program capable of performing automated reasoning—the first AI software in operation. In the following year, the program was demonstrated for the first time in Pittsburgh. | [7] |
| 1956 | John McCarthy first introduced the term AI at a conference on the subject. Later, in 1958, McCarthy developed the programming language Lisp, which became fundamental to the advancement of computer science and AI. Alongside Marvin Minsky, in 1959, he founded the AI laboratories. | [7,12] |
| 1958 | Arthur Samuel coined the term “Machine Learning” when he wrote about teaching a machine to play chess better than the humans who created it. | [7] |
| 1965 | Edward Feigenbaum initiated DENDRAL, the first “expert system”, capable of extracting molecular structures from organic compounds using scientific data. | [7] |
| 1966 | Joseph Weizenbaum developed the first “chatterbot”, ELIZA, a computer program designed to simulate a fictional psychotherapist. ELIZA used natural language processing to communicate with humans. | [7] |
| 1979 | The first American Association for AI was founded, currently known as the Association for the Advancement of AI (AAAI). | [7] |
| 1980s | The beginning of this decade became known as the “AI Boom”, as rapid growth and interest in AI emerged. John Hopfield and David Rumelhart introduced deep learning techniques, enabling computers to learn from experiences. Edward Feigenbaum developed specialized systems to imitate human decision-making processes. These systems were widely adopted in industry. The year 1984 became known as the “AI winter” because consumer, public, and private sectors began to show little interest in AI, leading to a decline in funding and research. | [7] |
| 1995 | Stuart Russell and Peter Norvig published “AI: A Modern Approach”, which became one of the key textbooks in the field. Richard Wallace developed the chatbot ALICE, which established more natural conversations with users. | [7] |
| 1997 | IBM’s specialized chess-playing system, Deep Blue, defeated Garry Kasparov, the reigning world chess champion and grandmaster, in a historic chess match. Dragon Systems developed voice recognition software, which was implemented in Windows. | [7,13] |
| 2000 | Cynthia Breazeal developed Kismet, the first robot capable of simulating human emotions, mimicking human facial expressions. | [7] |
| 2002 | iRobot introduced the Roomba, the first robotic vacuum cleaner that revolutionized the way homes were cleaned. Equipped with intelligent sensors, the Roomba navigates autonomously, detecting and avoiding obstacles, making cleaning easier and more efficient. | [7] |
| 2010 | Microsoft introduced Kinect for the Xbox 360, the first gaming device capable of tracking body movements and converting them into commands within the game. | [7] |
| 2011 | Apple launched Siri, the first virtual assistant. | [7] |
| 2014 | Amazon created the virtual assistant Alexa, allowing users to interact with electronic devices using voice commands. | [7] |
| 2016 | Hanson Robotics developed Sophia, the first humanoid robot with a realistic appearance, capable of communicating, seeing, and replicating human emotions. | [7] |
| 2020 | DeepMind released an updated version of AlphaFold, a program capable of deciphering the three-dimensional structure of any protein. | [7] |
| 2022 | OpenAI launched the chatbot ChatGPT | [7] |
2.2. Machine Learning
Common AI Models in Pharmaceutical Applications
2.3. Deep Learning
2.4. Ethical Concerns in the Use of AI in Healthcare
3. Challenges and Transformations in R&D Through AI Integration
3.1. Application of AI in Formulation
3.1.1. Drug Screening
Toxicity Prediction
Bioactivity Prediction
Prediction of Physicochemical Properties
3.1.2. Drug Design
Prediction of Drug–Protein Interaction
Prediction of Target Protein 3D Structure
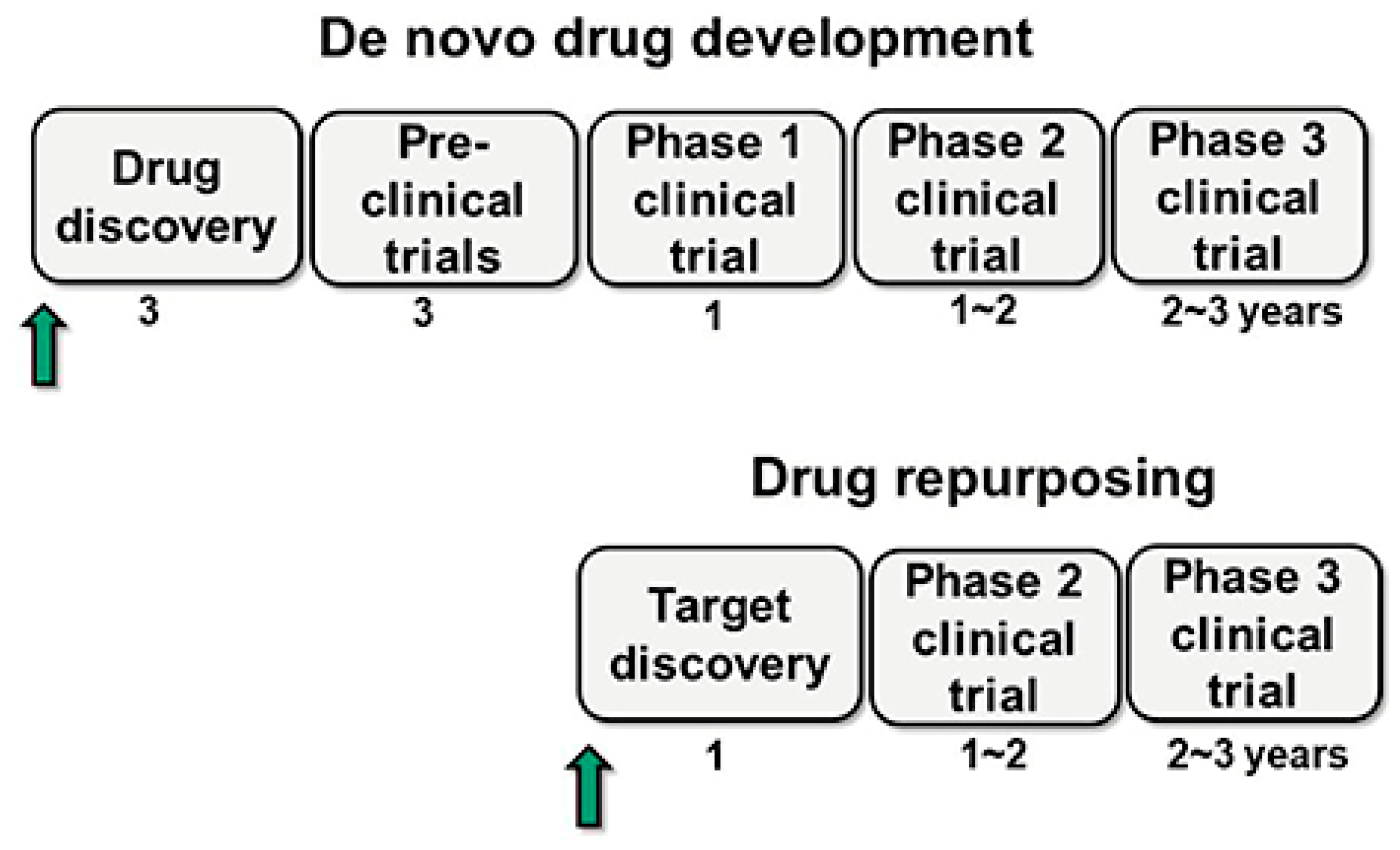
3.1.3. Drug Repurposing
3.1.4. Polypharmacology
3.1.5. Integration of AI with PBPK and Population PK Models
3.2. Integrating AI in Clinical Trials
3.3. AI-Developed Drugs: Highlighted Cases
3.4. AI in Biomedical Systems Modeling and Network Dynamics
3.5. Limitations, Risks, and Real-World Performance of AI Applications
4. Regulatory Issues
5. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADME | Absorption, Distribution, Metabolism, Excretion |
| ANN | Artificial Neural Network |
| DL | Deep Learning |
| DNNs | Deep Neural Networks |
| DTBA | Drug–Target Binding Affinity |
| EPI | Estimation Program Interface |
| FDA | Food and Drug Administration |
| R&D | Research and Development |
| AI | Artificial Intelligence |
| ML | Machine Learning |
| MMP | Matched Molecular Pair |
| NN | Neural Forest |
| QSPR | Quantitative Structure–Property Relationship |
| SaMD | Software as a Medical Device |
| SMILE | Simplified Molecular Input Line Entry System |
| SVM | Support Vector Machine |
| WHO | World Health Organization |
References
- Deng, J.; Yang, Z.; Ojima, I.; Samaras, D.; Wang, F. Artificial intelligence in drug discovery: Applications and techniques. Brief. Bioinform. 2021, 23, bbab430. [Google Scholar] [CrossRef] [PubMed]
- Kaul, V.; Enslin, S.; Gross, S.A. History of artificial intelligence in medicine. Gastrointest. Endosc. 2020, 92, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J. Artificial intelligence in radiology. Nat. Rev. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Denecke, K.; Baudoin, C.R. A Review of Artificial Intelligence and Robotics in Transformed Health Ecosystems. Front. Med. 2022, 9, 795957. [Google Scholar] [CrossRef]
- Paul, D.; Sanap, G.; Shenoy, S.; Kalyane, D.; Kalia, K.; Tekade, R.K. Artificial intelligence in drug discovery and development. Drug Discov. Today 2021, 26, 80–93. [Google Scholar] [CrossRef]
- Wang, L.; Ding, J.; Pan, L.; Cao, D.; Jiang, H.; Ding, X. Artificial intelligence facilitates drug design in the big data era. Chemom. Intell. Lab. Syst. 2019, 194, 103850. [Google Scholar] [CrossRef]
- Grzybowski, A.; Pawlikowska-Łagód, K.; Lambert, W.C. A History of Artificial Intelligence. Clin. Dermatol. 2024, 42, 221–229. [Google Scholar] [CrossRef]
- Bredt, S. Artificial Intelligence (AI) in the Financial Sector—Potential and Public Strategies. Front. Artif. Intell. 2019, 2, 16. [Google Scholar] [CrossRef]
- Stahl, B.C.; Antoniou, J.; Ryan, M.; Macnish, K.; Jiya, T. Organisational responses to the ethical issues of artificial intelligence. AI Soc. 2022, 37, 23–37. [Google Scholar] [CrossRef]
- Theodosiou, A.A.; Read, R.C. Artificial intelligence, machine learning and deep learning: Potential resources for the infection clinician. J. Infect. 2023, 87, 287–294. [Google Scholar] [CrossRef]
- Gawehn, E.; Hiss, J.A.; Schneider, G. Deep Learning in Drug Discovery. Mol. Inform. 2016, 35, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Mak, K.-K.; Pichika, M.R. Artificial intelligence in drug development: Present status and future prospects. Drug Discov. Today 2019, 24, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Vora, L.K.; Gholap, A.D.; Jetha, K.; Thakur, R.R.S.; Solanki, H.K.; Chavda, V.P. Artificial Intelligence in Pharmaceutical Technology and Drug Delivery Design. Pharmaceutics 2023, 15, 1916. [Google Scholar] [CrossRef] [PubMed]
- Choi, R.Y.; Coyner, A.S.; Kalpathy-Cramer, J.; Chiang, M.F.; Campbell, J.P. Introduction to Machine Learning, Neural Networks, and Deep Learning. Transl. Vis. Sci. Technol. 2020, 9, 14. [Google Scholar]
- Cabrera, A.; Bouterse, A.; Nelson, M.; Razzouk, J.; Ramos, O.; Chung, D.; Cheng, W.; Danisa, O. Use of random forest machine learning algorithm to predict short term outcomes following posterior cervical decompression with instrumented fusion. J. Clin. Neurosci. 2023, 107, 167–171. [Google Scholar] [CrossRef]
- Rebollo, R.; Oyoun, F.; Corvis, Y.; El-Hammadi, M.M.; Saubamea, B.; Andrieux, K.; Mignet, N.; Alhareth, K. Microfluidic Manufacturing of Liposomes: Development and Optimization by Design of Experiment and Machine Learning. ACS Appl. Mater. Interfaces 2022, 14, 39736–39745. [Google Scholar] [CrossRef]
- Lin, E.; Lin, C.-H.; Lane, H.-Y. De Novo Peptide and Protein Design Using Generative Adversarial Networks: An Update. J. Chem. Inf. Model. 2022, 62, 761–774. [Google Scholar] [CrossRef]
- Gupta, R.R. Application of Artificial Intelligence and Machine Learning in Drug Discovery. In Artificial Intelligence in Drug Design; Heifetz, A., Ed.; Springer: New York, NY, USA, 2022; pp. 113–124. [Google Scholar]
- Svensson, H.G.; Tyrchan, C.; Engkvist, O.; Chehreghani, M.H. Utilizing reinforcement learning for de novo drug design. Mach. Learn. 2024, 113, 4811–4843. [Google Scholar] [CrossRef]
- Pearson, G.S. Artificial Intelligence and Publication Ethics. J. Am. Psychiatr. Nurses Assoc. 2024, 30, 453–455. [Google Scholar] [CrossRef]
- Rogers, W.A.; Draper, H.; Carter, S.M. Evaluation of artificial intelligence clinical applications: Detailed case analyses show value of healthcare ethics approach in identifying patient care issues. Bioethics 2021, 35, 623–633. [Google Scholar] [CrossRef]
- Nagarajan, N.; Yapp, E.K.Y.; Le, N.Q.K.; Kamaraj, B.; Al-Subaie, A.M.; Yeh, H.-Y. Application of Computational Biology and Artificial Intelligence Technologies in Cancer Precision Drug Discovery. BioMed Res. Int. 2019, 2019, 8427042. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Luo, M.; Wu, P.; Wu, S.; Lee, T.-Y.; Bai, C. Application of Computational Biology and Artificial Intelligence in Drug Design. Int. J. Mol. Sci. 2022, 23, 13568. [Google Scholar] [CrossRef]
- Deore, A.B.; Dhumane, J.R.; Wagh, R.; Sonawane, R. The Stages of Drug Discovery and Development Process. Asian J. Pharm. Res. Dev. 2019, 7, 62–67. [Google Scholar] [CrossRef]
- Parvathaneni, V.; Kulkarni, N.S.; Muth, A.; Gupta, V. Drug repurposing: A promising tool to accelerate the drug discovery process. Drug Discov. Today 2019, 24, 2076–2085. [Google Scholar] [CrossRef]
- Dana, D.; Gadhiya, S.V.; St. Surin, L.G.; Li, D.; Naaz, F.; Ali, Q.; Paka, L.; Yamin, M.A.; Narayan, M.; Goldberg, I.D.; et al. Deep Learning in Drug Discovery and Medicine; Scratching the Surface. Molecules 2018, 23, 2384. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, C.; Das, B.; Rawat, V.S.; Wahlang, J.B.; Nongpiur, A.; Tiewsoh, I.; Lyngdoh, N.M.; Das, D.; Bidarolli, M.; Sony, H.T. Artificial Intelligence and Machine Learning Technology Driven Modern Drug Discovery and Development. Int. J. Mol. Sci. 2023, 24, 2026. [Google Scholar] [CrossRef] [PubMed]
- Ciallella, H.L.; Zhu, H. Advancing Computational Toxicology in the Big Data Era by Artificial Intelligence: Data-Driven and Mechanism-Driven Modeling for Chemical Toxicity. Chem. Res. Toxicol. 2019, 32, 536–547. [Google Scholar] [CrossRef]
- Parvatikar, P.P.; Patil, S.; Khaparkhuntikar, K.; Patil, S.; Singh, P.K.; Sahana, R.; Kulkarni, R.V.; Raghu, A.V. Artificial intelligence: Machine learning approach for screening large database and drug discovery. Antivir. Res. 2023, 220, 105740. [Google Scholar] [CrossRef]
- Singh, S.; Gupta, H.; Sharma, P.; Sahi, S. Advances in Artificial Intelligence (AI)-assisted approaches in drug screening. Artif. Intell. Chem. 2024, 2, 100039. [Google Scholar] [CrossRef]
- Spanakis, M.; Tzamali, E.; Tzedakis, G.; Koumpouzi, C.; Pediaditis, M.; Tsatsakis, A.; Sakkalis, V. Artificial Intelligence Models and Tools for the Assessment of Drug–Herb Interactions. Pharmaceuticals 2025, 18, 282. [Google Scholar] [CrossRef]
- Li, X.; Liang, J.; Hu, J.; Ma, L.; Yang, J.; Zhang, A.; Jing, Y.; Song, Y.; Yang, Y.; Feng, Z.; et al. Screening for primary aldosteronism on and off interfering medications. Endocrine 2024, 83, 178–187. [Google Scholar] [CrossRef]
- Rocco, P.; Musazzi, U.M.; Franzè, S.; Minghetti, P. Copies of nonbiological complex drugs: Generic, hybrid or biosimilar? Drug Discov Today 2019, 24, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Zagalo, D.M.; Sousa, J.; Simões, S. Quality by design (QbD) approach in marketing authorization procedures of Non-Biological Complex Drugs: A critical evaluation. Eur. J. Pharm. Biopharm. 2022, 178, 1–24. [Google Scholar] [CrossRef]
- Saha, E.; Rathore, P.; Parida, R.; Rana, N.P. The interplay of emerging technologies in pharmaceutical supply chain performance: An empirical investigation for the rise of Pharma 4.0. Technol. Forecast. Soc. Change 2022, 181, 121768. [Google Scholar] [CrossRef]
- Malheiro, V.; Duarte, J.; Veiga, F.; Mascarenhas-Melo, F. Exploiting Pharma 4.0 Technologies in the Non-Biological Complex Drugs Manufacturing: Innovations and Implications. Pharmaceutics 2023, 15, 2545. [Google Scholar] [CrossRef]
- Chan, H.C.S.; Shan, H.; Dahoun, T.; Vogel, H.; Yuan, S. Advancing Drug Discovery via Artificial Intelligence. Trends Pharmacol. Sci. 2019, 40, 592–604. [Google Scholar] [CrossRef]
- Shiammala, P.N.; Duraimutharasan, N.K.B.; Vaseeharan, B.; Alothaim, A.S.; Al-Malki, E.S.; Snekaa, B.; Safi, S.Z.; Singh, S.K.; Velmurugan, D.; Selvaraj, C. Exploring the artificial intelligence and machine learning models in the context of drug design difficulties and future potential for the pharmaceutical sectors. Methods 2023, 219, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Kaur, N.; Gehlot, A. Application of artificial intelligence in drug design: A review. Comput. Biol. Med. 2024, 179, 108810. [Google Scholar] [CrossRef]
- Rashid, M.B.M.A. Artificial Intelligence Effecting a Paradigm Shift in Drug Development. SLAS Technol. 2021, 26, 3–15. [Google Scholar] [CrossRef]
- Doytchinova, I. Drug Design—Past, Present, Future. Molecules 2022, 27, 1496. [Google Scholar] [CrossRef]
- Gholap, A.D.; Uddin, J.; Faiyazuddin; Omri, A.; Gowri, S.; Khalid, M. Advances in artificial intelligence for drug delivery and development: A comprehensive review. Comput. Biol. Med. 2024, 178, 108702. [Google Scholar] [CrossRef] [PubMed]
- Jumper, J.; Evans, R.; Pritzel, A.; Green, T.; Figurnov, M.; Ronneberger, O.; Tunyasuvunakool, K.; Bates, R.; Žídek, A.; Potapenko, A.; et al. Highly accurate protein structure prediction with AlphaFold. Nature 2021, 596, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; Ohue, M. SpatialPPI: Three-dimensional space protein-protein interaction prediction with AlphaFold Multimer. Comput. Struct. Biotechnol. J. 2024, 23, 1214–1225. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Samantasinghar, A.; Soomro, A.M.; Kim, S.; Choi, K.H. A systematic review of computational approaches to understand cancer biology for informed drug repurposing. J. Biomed. Inform. 2023, 142, 104373. [Google Scholar] [CrossRef]
- Park, K. A review of computational drug repurposing. Transl. Clin. Pharmacol. 2019, 27, 59–63. [Google Scholar] [CrossRef]
- Issa, N.T.; Stathias, V.; Schürer, S.; Dakshanamurthy, S. Machine and deep learning approaches for cancer drug repurposing. Semin. Cancer Biol. 2021, 68, 132–142. [Google Scholar] [CrossRef]
- Bajorath, J. Origins and progression of the polypharmacology concept in drug discovery. Artif. Intell. Life Sci. 2024, 5, 100094. [Google Scholar] [CrossRef]
- Cichońska, A.; Ravikumar, B.; Rahman, R. AI for targeted polypharmacology: The next frontier in drug discovery. Curr. Opin. Struct. Biol. 2024, 84, 102771. [Google Scholar] [CrossRef]
- Raman, K.; Kumar, R.; Musante, C.J.; Madhavan, S. Integrating Model-Informed Drug Development With AI: A Synergistic Approach to Accelerating Pharmaceutical Innovation. Clin. Transl. Sci. 2025, 18, e70124. [Google Scholar] [CrossRef]
- Peters, S.A. Applications of Physiologically Based Pharmacokinetic Models Integrated with Drug Effect models (PBPK/PD). In Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations: Principles, Methods, and Applications in the Pharmaceutical Industry, Second Edition; John Wiley & Sons: Hoboken, NJ, USA, 2021; pp. 353–374. [Google Scholar]
- Saeheng, T.; Karbwang, J.; Na-Bangchang, K. Population-pharmacokinetic/pharmacodynamic model of atractylodes lancea (Thunb.) DC. administration in patients with advanced-stage intrahepatic cholangiocarcinoma: A dosage prediction. BMC Complement. Med. Ther. 2024, 24, 384. [Google Scholar] [CrossRef]
- Chou, W.-C.; Chen, Q.; Yuan, L.; Cheng, Y.-H.; He, C.; Monteiro-Riviere, N.A.; Riviere, J.E.; Lin, Z. An artificial intelligence-assisted physiologically-based pharmacokinetic model to predict nanoparticle delivery to tumors in mice. J. Control Release 2023, 361, 53–63. [Google Scholar] [CrossRef]
- Chou, W.-C.; Lin, Z. Machine learning and artificial intelligence in physiologically based pharmacokinetic modeling. Toxicol. Sci. 2022, 191, 1–14. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Z.; Li, Y.; Du, J.; Gao, X.; Li, Y.; Lai, L. A Combination of Machine Learning and PBPK Modeling Approach for Pharmacokinetics Prediction of Small Molecules in Humans. Pharm. Res. 2024, 41, 1369–1379. [Google Scholar] [CrossRef]
- Wu, K.; Li, X.; Zhou, Z.; Zhao, Y.; Su, M.; Cheng, Z.; Wu, X.; Huang, Z.; Jin, X.; Li, J.; et al. Predicting pharmacodynamic effects through early drug discovery with artificial intelligence-physiologically based pharmacokinetic (AI-PBPK) modelling. Front. Pharmacol. 2024, 15, 1330855. [Google Scholar] [CrossRef]
- Umscheid, C.A.; Margolis, D.J.; Grossman, C.E. Key Concepts of Clinical Trials: A Narrative Review. Postgrad. Med. 2011, 123, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Fogel, D.B. Factors associated with clinical trials that fail and opportunities for improving the likelihood of success: A review. Contemp. Clin. Trials Commun. 2018, 11, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, J.W.; Abraham, W.T.; Bhatt, A.S.; Dunn, J.; Felker, G.M.; Jain, S.S.; Lindsell, C.J.; Mace, M.; Martyn, T.; Shah, R.U.; et al. Artificial Intelligence in Cardiovascular Clinical Trials. JACC 2024, 84, 2051–2062. [Google Scholar] [CrossRef] [PubMed]
- Chopra, H.; Annu; Kil Shin, D.; Munjal, K.; Priyanka; Dhama, K.; Bin Emran, T. Revolutionizing clinical trials: The role of AI in accelerating medical breakthroughs. Int. J. Surg. 2023, 109, 4211–4220. [Google Scholar] [CrossRef]
- Zhang, Y.; Mastouri, M.; Zhang, Y. Accelerating drug discovery, development, and clinical trials by artificial intelligence. Medicine 2024, 5, 1050–1070. [Google Scholar] [CrossRef]
- Goldberg, J.M.; Amin, N.P.; Zachariah, K.A.; Bhatt, A.B. The Introduction of AI Into Decentralized Clinical Trials. JACC Adv. 2024, 3, 101094. [Google Scholar] [CrossRef]
- Lu, X.; Yang, C.; Liang, L.; Hu, G.; Zhong, Z.; Jiang, Z. Artificial intelligence for optimizing recruitment and retention in clinical trials: A scoping review. J. Am. Med. Inform. Assoc. 2024, 31, 2749–2759. [Google Scholar] [CrossRef] [PubMed]
- Fountzilas, E.; Tsimberidou, A.M.; Vo, H.H.; Kurzrock, R. Clinical trial design in the era of precision medicine. Genome Med. 2022, 14, 101. [Google Scholar] [CrossRef]
- Jayatunga, M.K.; Ayers, M.; Bruens, L.; Jayanth, D.; Meier, C. How successful are AI-discovered drugs in clinical trials? A first analysis and emerging lessons. Drug Discov. Today 2024, 29, 104009. [Google Scholar] [CrossRef] [PubMed]
- Askin, S.; Burkhalter, D.; Calado, G.; El Dakrouni, S. Artificial Intelligence Applied to clinical trials: Opportunities and challenges. Health Technol. 2023, 13, 203–213. [Google Scholar] [CrossRef]
- Wang, J.; Zeng, Z.; Li, Z.; Liu, G.; Zhang, S.; Luo, C.; Hu, S.; Wan, S.; Zhao, L. The clinical application of artificial intelligence in cancer precision treatment. J. Transl. Med. 2025, 23, 120. [Google Scholar] [CrossRef]
- Salas, M.; Petracek, J.; Yalamanchili, P.; Aimer, O.; Kasthuril, D.; Dhingra, S.; Junaid, T.; Bostic, T. The Use of Artificial Intelligence in Pharmacovigilance: A Systematic Review of the Literature. Pharm. Med. 2022, 36, 295–306. [Google Scholar] [CrossRef]
- Joshi, P.; Masilamani, V.; Mukherjee, A. A knowledge graph embedding based approach to predict the adverse drug reactions using a deep neural network. J. Biomed. Inform. 2022, 132, 104122. [Google Scholar] [CrossRef] [PubMed]
- Syrowatka, A.; Song, W.; Amato, M.G.; Foer, D.; Edrees, H.; Co, Z.; Kuznetsova, M.; Dulgarian, S.; Seger, D.L.; Simona, A.; et al. Key use cases for artificial intelligence to reduce the frequency of adverse drug events: A scoping review. Lancet Digit. Health 2022, 4, e137–e148. [Google Scholar] [CrossRef]
- Widera, P.; Welsing, P.M.; Danso, S.O.; Peelen, S.; Kloppenburg, M.; Loef, M.; Marijnissen, A.C.; van Helvoort, E.M.; Blanco, F.J.; Magalhães, J.; et al. Development and validation of a machine learning-supported strategy of patient selection for osteoarthritis clinical trials: The IMI-APPROACH study. Osteoarthr. Cartil. Open 2023, 5, 100406. [Google Scholar] [CrossRef]
- Cook, S.F.; Rhodes, T.; Schlusser, C.; Han, S.; Chen, C.; Zach, N.; Murthy, V.; Davé, S. A Descriptive Review of Global Real World Evidence Efforts to Advance Drug Discovery and Clinical Development in Amyotrophic Lateral Sclerosis. Front. Neurol. 2021, 12, 770001. [Google Scholar] [CrossRef]
- Singh, G.; Schulthess, D.; Hughes, N.; Vannieuwenhuyse, B.; Kalra, D. Real world big data for clinical research and drug development. Drug Discov. Today 2018, 23, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Dou, L.; Xu, Z.; Xu, J.; Zang, C.; Su, C.; Pieper, A.A.; Leverenz, J.B.; Wang, F.; Zhu, X.; Cummings, J.; et al. A network-based systems genetics framework identifies pathobiology and drug repurposing in Parkinson’s disease. NPJ Park. Dis. 2025, 11, 22. [Google Scholar] [CrossRef]
- Zhang, W.; Kuang, Z.; Peissig, P.; Page, D. Adverse drug reaction discovery from electronic health records with deep neural networks. In Proceedings of the ACM Conference on Health, Inference, and Learning CHIL ‘20, Toronto, ON, Canada, 2–4 April 2020; pp. 30–39. [Google Scholar]
- Denny, J.C.; Van Driest, S.L.; Wei, W.; Roden, D.M. The Influence of Big (Clinical) Data and Genomics on Precision Medicine and Drug Development. Clin. Pharmacol. Ther. 2018, 103, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Nagalakshmi, R.; Khan, S.B.; Kumar, A.V.; R, M.T.; Alojail, M.; Sangwan, S.R.; Saraee, M. Enhancing drug discovery and patient care through advanced analytics with the power of NLP and machine learning in pharmaceutical data interpretation. SLAS Technol. 2025, 31, 100238. [Google Scholar]
- Liu, Z.; Roberts, R.A.; Lal-Nag, M.; Chen, X.; Huang, R.; Tong, W. AI-based language models powering drug discovery and development. Drug Discov. Today 2021, 26, 2593–2607. [Google Scholar] [CrossRef]
- Liu, J.; Wang, X.; Ye, X.; Chen, D. Improved health outcomes of nasopharyngeal carcinoma patients 3 years after treatment by the AI-assisted home enteral nutrition management. Front. Nutr. 2025, 11, 1481073. [Google Scholar] [CrossRef]
- Śledź, P.; Caflisch, A. Protein structure-based drug design: From docking to molecular dynamics. Curr. Opin. Struct. Biol. 2018, 48, 93–102. [Google Scholar] [CrossRef]
- Farghali, H.; Kutinová Canová, N.; Arora, M. The potential applications of artificial intelligence in drug discovery and development. Physiol. Res. 2021, 70 (Suppl. S4), S715–S722. [Google Scholar] [CrossRef] [PubMed]
- Burki, T. A new paradigm for drug development. Lancet Digit. Health 2020, 2, e226–e227. [Google Scholar] [CrossRef]
- Soni, K.; Hasija, Y. Artificial Intelligence Assisted Drug Research and Development. In Proceedings of the 2022 IEEE Delhi Section Conference (DELCON), New Delhi, India, 11–13 February 2022. [Google Scholar]
- Richardson, P.; Griffin, I.; Tucker, C.; Smith, D.; Oechsle, O.; Phelan, A.; Rawling, M.; Savory, E.; Stebbing, J. Baricitinib as potential treatment for 2019-nCoV acute respiratory disease. Lancet 2020, 395, e30–e31. [Google Scholar] [CrossRef]
- Cesaro, A.; de la Fuente-Nunez, C. Antibiotic identified by AI. Nat. Chem. Biol. 2023, 19, 1296–1298. [Google Scholar] [CrossRef]
- Gupta, R.; Srivastava, D.; Sahu, M.; Tiwari, S.; Ambasta, R.K.; Kumar, P. Artificial intelligence to deep learning: Machine intelligence approach for drug discovery. Mol. Divers. 2021, 25, 1315–1360. [Google Scholar] [CrossRef]
- Ren, F.; Aliper, A.; Chen, J.; Zhao, H.; Rao, S.; Kuppe, C.; Ozerov, I.V.; Zhang, M.; Witte, K.; Kruse, C.; et al. A small-molecule TNIK inhibitor targets fibrosis in preclinical and clinical models. Nat. Biotechnol. 2025, 43, 63–75. [Google Scholar] [CrossRef]
- Stokes, J.M.; Yang, K.; Swanson, K.; Jin, W.; Cubillos-Ruiz, A.; Donghia, N.M.; Macnair, C.R.; French, S.; Carfrae, L.A.; Bloom-Ackermann, Z.; et al. A Deep Learning Approach to Antibiotic Discovery. Cell 2020, 180, 688–702.e13. [Google Scholar] [CrossRef]
- Nussinov, R.; Zhang, M.; Liu, Y.; Jang, H. AlphaFold, allosteric, and orthosteric drug discovery: Ways forward. Drug Discov. Today 2023, 28, 103551. [Google Scholar] [CrossRef]
- Guo, S.-B.; Meng, Y.; Lin, L.; Zhou, Z.-Z.; Li, H.-L.; Tian, X.-P.; Huang, W.-J. Artificial intelligence alphafold model for molecular biology and drug discovery: A machine-learning-driven informatics investigation. Mol. Cancer 2024, 23, 223. [Google Scholar] [CrossRef]
- Saber-Ayad, M.; Hammoudeh, S.; Abu-Gharbieh, E.; Hamoudi, R.; Tarazi, H.; Al-Tel, T.H.; Hamid, Q. Current Status of Baricitinib as a Repurposed Therapy for COVID-19. Pharmaceuticals 2021, 14, 680. [Google Scholar] [CrossRef]
- Saito, R.; Yano, N.; Kojima, S.; Miyoshi, F. Data-driven drug discovery for drug repurposing. Nihon Yakurigaku Zasshi 2023, 158, 10–14. [Google Scholar] [CrossRef]
- Program, T.A.A.; Wallach, I.; Bernard, D.; Nguyen, K.; Ho, G.; Morrison, A.; Stecula, A.; Rosnik, A.; O’sullivan, A.M.; Davtyan, A.; et al. AI is a viable alternative to high throughput screening: A 318-target study. Sci. Rep. 2024, 14, 7526. [Google Scholar]
- Chen, J.; Bolhuis, D.L.; Laggner, C.; Kong, D.; Yu, L.; Wang, X.; Emanuele, M.J.; Brown, N.G.; Liu, P. AtomNet-Aided OTUD7B Inhibitor Discovery and Validation. Cancers 2023, 15, 517. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, Z.-W.; Qin, Y. inite-Time Topology Identification of Delayed Complex Dynamical Networks and Its Application. Cyborg Bionic Syst. 2024, 5, 0092. [Google Scholar] [CrossRef]
- Zanca, F.; Brusasco, C.; Pesapane, F.; Kwade, Z.; Beckers, R.; Avanzo, M. Regulatory Aspects of the Use of Artificial Intelligence Medical Software. Semin. Radiat. Oncol. 2022, 32, 432–441. [Google Scholar] [CrossRef]
- Mirakhori, F.; Niazi, S.K. Harnessing the AI/ML in Drug and Biological Products Discovery and Development: The Regulatory Perspective. Pharmaceuticals 2025, 18, 47. [Google Scholar] [CrossRef]
- Da Silva, M.; Horsley, T.; Singh, D.; Da Silva, E.; Ly, V.; Thomas, B.; Daniel, R.C.; Chagal-Feferkorn, K.A.; Iantomasi, S.; White, K.; et al. Legal concerns in health-related artificial intelligence: A scoping review protocol. Syst. Rev. 2022, 11, 123. [Google Scholar] [CrossRef]
- Krishnan Ganapathy, M.N. Artificial Intelligence and Healthcare Regulatory and Legal Concerns. Telehealth Med. Today 2021, 6, 252. [Google Scholar] [CrossRef]
- Gerke, S.; Babic, B.; Evgeniou, T.; Cohen, I.G. The need for a system view to regulate artificial intelligence/machine learning-based software as medical device. npj Digit. Med. 2020, 3, 53. [Google Scholar] [CrossRef]
- Lee, T.T.; Kesselheim, A.S. U.S. Food and Drug Administration Precertification Pilot Program for Digital Health Software: Weighing the Benefits and Risks. Ann. Intern. Med. 2018, 168, 730–732. [Google Scholar] [CrossRef]
- Khan, Z.; Gaidhane, A.M.; Singh, M.; Ganesan, S.; Kaur, M.; Sharma, G.C.; Rani, P.; Sharma, R.; Thapliyal, S.; Kushwaha, M.; et al. Diagnostic Accuracy of IDX-DR for Detecting Diabetic Retinopathy: A Systematic Review and Meta-Analysis. Am. J. Ophthalmol. 2025, 273, 192–204. [Google Scholar] [CrossRef]
- Cheng, J.Y.; Abel, J.T.; Balis, U.G.; McClintock, D.S.; Pantanowitz, L. Challenges in the Development, Deployment, and Regulation of Artificial Intelligence in Anatomic Pathology. Am. J. Pathol. 2021, 191, 1684–1692. [Google Scholar] [CrossRef]
- Lin, W.; Chen, Y.; Unadkat, J.D.; Zhang, X.; Wu, D.; Heimbach, T. Applications, Challenges, and Outlook for PBPK Modeling and Simulation: A Regulatory, Industrial and Academic Perspective. Pharm. Res. 2022, 39, 1701–1731. [Google Scholar] [CrossRef]
- Pappalardo, F.; Russo, G.; Tshinanu, F.M.; Viceconti, M. In silico clinical trials: Concepts and early adoptions. Brief. Bioinform. 2018, 20, 1699–1708. [Google Scholar] [CrossRef]
- Bordukova, M.; Makarov, N.; Rodriguez-Esteban, R.; Schmich, F.; Menden, M.P. Generative artificial intelligence empowers digital twins in drug discovery and clinical trials. Expert Opin. Drug Discov. 2024, 19, 33–42. [Google Scholar] [CrossRef]
- Greenleaf, G.; Mowbray, A.; Chung, P. Building sustainable free legal advisory systems: Experiences from the history of AI & law. Comput. Law Secur. Rev. 2018, 34, 314–326. [Google Scholar]
- Askr, H.; Elgeldawi, E.; Ella, H.A.; Elshaier, Y.A.M.M.; Gomaa, M.M.; Hassanien, A.E. Deep learning in drug discovery: An integrative review and future challenges. Artif. Intell. Rev. 2023, 56, 5975–6037. [Google Scholar] [CrossRef]
| Ethical Principle | Ethical Foundations |
|---|---|
| Autonomy |
|
| Public interest |
|
| Transparency |
|
| Responsibility |
|
| Inclusion and equity |
|
| Privacy |
|
| Molecule | Original Therapeutic Indication | New Therapeutic Indication |
|---|---|---|
| Ormeloxifene | Oral contraceptive | Prostate Cancer |
| Metformin | Diabetes | Cancer |
| Cimetidine | Ulcer | Lung Cancer |
| Bazedoxifene | Osteoporosis | Breast Cancer |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malheiro, V.; Santos, B.; Figueiras, A.; Mascarenhas-Melo, F. The Potential of Artificial Intelligence in Pharmaceutical Innovation: From Drug Discovery to Clinical Trials. Pharmaceuticals 2025, 18, 788. https://doi.org/10.3390/ph18060788
Malheiro V, Santos B, Figueiras A, Mascarenhas-Melo F. The Potential of Artificial Intelligence in Pharmaceutical Innovation: From Drug Discovery to Clinical Trials. Pharmaceuticals. 2025; 18(6):788. https://doi.org/10.3390/ph18060788
Chicago/Turabian StyleMalheiro, Vera, Beatriz Santos, Ana Figueiras, and Filipa Mascarenhas-Melo. 2025. "The Potential of Artificial Intelligence in Pharmaceutical Innovation: From Drug Discovery to Clinical Trials" Pharmaceuticals 18, no. 6: 788. https://doi.org/10.3390/ph18060788
APA StyleMalheiro, V., Santos, B., Figueiras, A., & Mascarenhas-Melo, F. (2025). The Potential of Artificial Intelligence in Pharmaceutical Innovation: From Drug Discovery to Clinical Trials. Pharmaceuticals, 18(6), 788. https://doi.org/10.3390/ph18060788