
Subthreshold Cannabidiol Potentiates Levetiracetam in the Kainic Acid Model of Temporal Lobe Epilepsy: A Pilot Study

 ,
, 
 and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
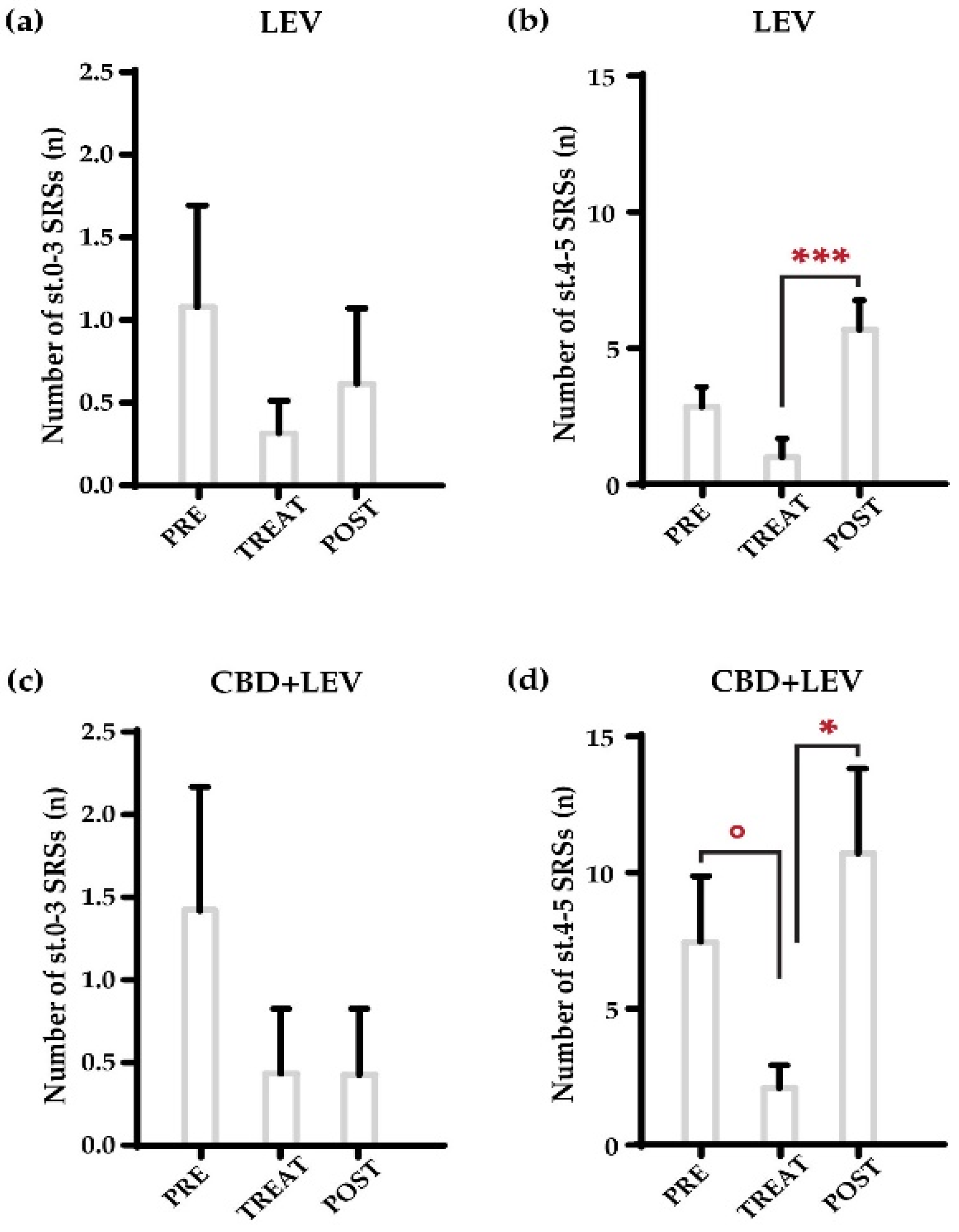
2.1. Characterization of the Overall Number of Spontaneous Recurrent Seizures (SRSs)
2.2. Characterization of the Total Duration of SRSs
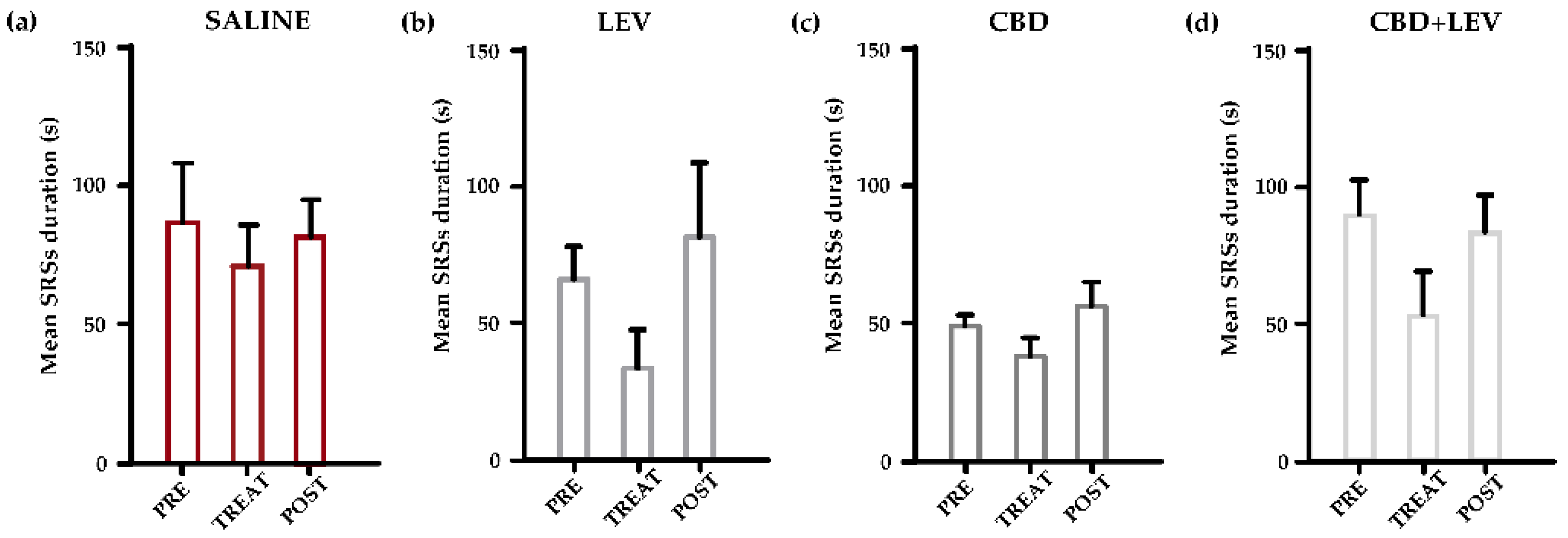
2.3. Characterization of the Mean Duration of SRSs
3. Discussion
4. Materials and Methods
4.1. Animals
4.2. Experimental Design
4.3. Electrode Implantation and Video-Electrocorticography Analysis
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Devinsky, O.; Cross, J.H.; Laux, L.; Marsh, E.; Miller, I.; Nabbout, R.; Scheffer, I.E.; Thiele, E.A.; Wright, S. Trial of Cannabidiol for Drug-Resistant Seizures in the Dravet Syndrome. N. Engl. J. Med. 2017, 376, 2011–2020. [Google Scholar] [CrossRef] [PubMed]
- Miller, I.; Scheffer, I.E.; Gunning, B.; Sanchez-Carpintero, R.; Gil-Nagel, A.; Perry, M.S.; Saneto, R.P.; Checketts, D.; Dunayevich, E.; Knappertz, V.; et al. Dose-Ranging Effect of Adjunctive Oral Cannabidiol vs Placebo on Convulsive Seizure Frequency in Dravet Syndrome: A Randomized Clinical Trial. JAMA Neurol. 2020, 77, 613. [Google Scholar] [CrossRef] [PubMed]
- Devinsky, O.; Patel, A.D.; Cross, J.H.; Villanueva, V.; Wirrell, E.C.; Privitera, M.; Greenwood, S.M.; Roberts, C.; Checketts, D.; VanLandingham, K.E.; et al. Effect of Cannabidiol on Drop Seizures in the Lennox–Gastaut Syndrome. N. Engl. J. Med. 2018, 378, 1888–1897. [Google Scholar] [CrossRef] [PubMed]
- Thiele, E.A.; Marsh, E.D.; French, J.A.; Mazurkiewicz-Beldzinska, M.; Benbadis, S.R.; Joshi, C.; Lyons, P.D.; Taylor, A.; Roberts, C.; Sommerville, K.; et al. Cannabidiol in Patients with Seizures Associated with Lennox-Gastaut Syndrome (GWPCARE4): A Randomised, Double-Blind, Placebo-Controlled Phase 3 Trial. Lancet 2018, 391, 1085–1096. [Google Scholar] [CrossRef] [PubMed]
- Thiele, E.A.; Bebin, E.M.; Bhathal, H.; Jansen, F.E.; Kotulska, K.; Lawson, J.A.; O’Callaghan, F.J.; Wong, M.; Sahebkar, F.; Checketts, D.; et al. Add-on Cannabidiol Treatment for Drug-Resistant Seizures in Tuberous Sclerosis Complex: A Placebo-Controlled Randomized Clinical Trial. JAMA Neurol. 2021, 78, 285. [Google Scholar] [CrossRef]
- Reddy, S.D. Therapeutic and clinical foundations of cannabidiol therapy for difficult-to-treat seizures in children and adults with refractory epilepsies. Exp. Neurol. 2023, 359, 114237. [Google Scholar] [CrossRef]
- Rozental, A.J.; Weisbeck, B.G.; Corsato Alvarenga, I.; Gustafson, D.L.; Kusick, B.R.; Rao, S.; Bartner, L.R.; McGrath, S. The Efficacy and Safety of Cannabidiol as Adjunct Treatment for Drug-resistant Idiopathic Epilepsy in 51 Dogs: A Double-blinded Crossover Study. J. Vet. Intern. Med. 2023, 37, 2291–2300. [Google Scholar] [CrossRef]
- Szaflarski, J.P.; Devinsky, O.; Lopez, M.; Park, Y.D.; Zentil, P.P.; Patel, A.D.; Thiele, E.A.; Wechsler, R.T.; Checketts, D.; Sahebkar, F. Long-term Efficacy and Safety of Cannabidiol in Patients with Treatment-resistant Epilepsies: Four-year Results from the Expanded Access Program. Epilepsia 2023, 64, 619–629. [Google Scholar] [CrossRef]
- Téllez-Zenteno, J.F.; Hernández-Ronquillo, L. A Review of the Epidemiology of Temporal Lobe Epilepsy. Epilepsy Res. Treat. 2012, 2012, 630853. [Google Scholar] [CrossRef]
- Fallah, M.S.; Dlugosz, L.; Scott, B.W.; Thompson, M.D.; Burnham, W.M. Antiseizure Effects of the Cannabinoids in the Amygdala-kindling Model. Epilepsia 2021, 62, 2274–2282. [Google Scholar] [CrossRef]
- Patra, P.H.; Barker-Haliski, M.; White, H.S.; Whalley, B.J.; Glyn, S.; Sandhu, H.; Jones, N.; Bazelot, M.; Williams, C.M.; McNeish, A.J. Cannabidiol Reduces Seizures and Associated Behavioral Comorbidities in a Range of Animal Seizure and Epilepsy Models. Epilepsia 2019, 60, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Thomson, K.E.; Metcalf, C.S.; Newell, T.G.; Huff, J.; Edwards, S.F.; West, P.J.; Wilcox, K.S. Evaluation of Subchronic Administration of Antiseizure Drugs in Spontaneously Seizing Rats. Epilepsia 2020, 61, 1301–1311. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.-M.; Russo, F.; Senn, L.; Ibatici, D.; Cannazza, G.; Biagini, G. Antiseizure Effects of Cannabidiol Leading to Increased Peroxisome Proliferator-Activated Receptor Gamma Levels in the Hippocampal CA3 Subfield of Epileptic Rats. Pharmaceuticals 2022, 15, 495. [Google Scholar] [CrossRef] [PubMed]
- Lynch, J.M.; Tate, S.K.; Kinirons, P.; Weale, M.E.; Cavalleri, G.L.; Depondt, C.; Murphy, K.; O’Rourke, D.; Doherty, C.P.; Shianna, K.V.; et al. No Major Role of Common SV2A Variation for Predisposition or Levetiracetam Response in Epilepsy. Epilepsy Res. 2009, 83, 44–51. [Google Scholar] [CrossRef]
- Costa, A.-M.; Lucchi, C.; Malkoç, A.; Rustichelli, C.; Biagini, G. Relationship between Delta Rhythm, Seizure Occurrence and Allopregnanolone Hippocampal Levels in Epileptic Rats Exposed to the Rebound Effect. Pharmaceuticals 2021, 14, 127. [Google Scholar] [CrossRef]
- Racine, R.J. Modification of Seizure Activity by Electrical Stimulation: II. Motor Seizure. Electroencephalogr. Clin. Neurophysiol. 1972, 32, 281–294. [Google Scholar] [CrossRef]
- Biagini, G.; Panuccio, G.; Avoli, M. Neurosteroids and Epilepsy. Curr. Opin. Neurol. 2010, 23, 170–176. [Google Scholar] [CrossRef]
- Lévesque, M.; Biagini, G.; Avoli, M. Neurosteroids and Focal Epileptic Disorders. Int. J. Mol. Sci. 2020, 21, 9391. [Google Scholar] [CrossRef]
- Reddy, D.S. Neurosteroids as Novel Anticonvulsants for Refractory Status Epilepticus and Medical Countermeasures for Nerve Agents: A 15-Year Journey to Bring Ganaxolone from Bench to Clinic. J. Pharmacol. Exp. Ther. 2024, 388, 273–300. [Google Scholar] [CrossRef]
- Knight, E.M.P.; Amin, S.; Bahi-Buisson, N.; Benke, T.A.; Cross, J.H.; Demarest, S.T.; Olson, H.E.; Specchio, N.; Fleming, T.R.; Aimetti, A.A.; et al. Safety and Efficacy of Ganaxolone in Patients with CDKL5 Deficiency Disorder: Results from the Double-Blind Phase of a Randomised, Placebo-Controlled, Phase 3 Trial. Lancet Neurol. 2022, 21, 417–427. [Google Scholar] [CrossRef]
- Olson, H.E.; Amin, S.; Bahi-Buisson, N.; Devinsky, O.; Marsh, E.D.; Pestana-Knight, E.; Rajaraman, R.R.; Aimetti, A.A.; Rybak, E.; Kong, F.; et al. Long-term Treatment with Ganaxolone for Seizures Associated with Cyclin-dependent Kinase-like 5 Deficiency Disorder: Two-year Open-label Extension Follow-up. Epilepsia 2024, 65, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Bakas, T.; Van Nieuwenhuijzen, P.S.; Devenish, S.O.; McGregor, I.S.; Arnold, J.C.; Chebib, M. The Direct Actions of Cannabidiol and 2-Arachidonoyl Glycerol at GABAA Receptors. Pharmacol. Res. 2017, 119, 358–370. [Google Scholar] [CrossRef] [PubMed]
- Ruffolo, G.; Gaeta, A.; Cannata, B.; Pinzaglia, C.; Aronica, E.; Morano, A.; Cifelli, P.; Palma, E. GABAergic Neurotransmission in Human Tissues Is Modulated by Cannabidiol. Life 2022, 12, 2042. [Google Scholar] [CrossRef] [PubMed]
- Gunn, B.G.; Cunningham, L.; Mitchell, S.G.; Swinny, J.D.; Lambert, J.J.; Belelli, D. GABAA Receptor-Acting Neurosteroids: A Role in the Development and Regulation of the Stress Response. Front. Neuroendocrinol. 2015, 36, 28–48. [Google Scholar] [CrossRef] [PubMed]
- Chintala, S.M.; Tateiwa, H.; Qian, M.; Xu, Y.; Amtashar, F.; Chen, Z.; Kirkpatrick, C.C.; Bracamontes, J.; Germann, A.L.; Akk, G.; et al. Direct Measurements of Neurosteroid Binding to Specific Sites on GABAA Receptors. Br. J. Pharmacol. 2024. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Golub, V.; Ramakrishnan, S.; Reddy, D.S. Isobolographic Analysis of Adjunct Antiseizure Activity of the FDA-Approved Cannabidiol with Neurosteroids and Benzodiazepines in Adult Refractory Focal Onset Epilepsy. Exp. Neurol. 2023, 360, 114294. [Google Scholar] [CrossRef] [PubMed]
- Gilmartin, C.G.S.; Dowd, Z.; Parker, A.P.J.; Harijan, P. Interaction of cannabidiol with other antiseizure medications: A narrative review. Seizure 2021, 86, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Socała, K.; Wyska, E.; Szafarz, M.; Nieoczym, D.; Wlaź, P. Acute effect of cannabidiol on the activity of various novel antiepileptic drugs in the maximal electroshock- and 6 Hz-induced seizures in mice: Pharmacodynamic and pharmacokinetic studies. Neuropharmacology 2019, 158, 107733. [Google Scholar] [CrossRef]
- Gaston, T.E.; Bebin, E.M.; Cutter, G.R.; Grayson, L.; Szaflarski, J.P. Final analysis of potential drug-drug interactions between highly purified cannabidiol and anti-seizure medications in an open-label expanded access program. Epilepsia Open 2023, 8, 1405–1412. [Google Scholar] [CrossRef]
- Bertram, E.H.; Dudek, F.E. Addressing the problems of treatment failure in epilepsy: You cannot fix what you do not understand. Epilepsia 2024, 65, 2248–2254. [Google Scholar] [CrossRef]
- Widmann, M.; Lieb, A.; Fogli, B.; Steck, A.; Mutti, A.; Schwarzer, C. Characterization of the intrahippocampal kainic acid model in female mice with a special focus on seizure suppression by antiseizure medications. Exp. Neurol. 2024, 376, 114749. [Google Scholar] [CrossRef] [PubMed]
- Duveau, V.; Pouyatos, B.; Bressand, K.; Bouyssières, C.; Chabrol, T.; Roche, Y.; Depaulis, A.; Roucard, C. Differential Effects of Antiepileptic Drugs on Focal Seizures in the Intrahippocampal Kainate Mouse Model of Mesial Temporal Lobe Epilepsy. CNS Neurosci. Ther. 2016, 22, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Casillas-Espinosa, P.M.; Anderson, A.; Harutyunyan, A.; Li, C.; Lee, J.; Braine, E.L.; Brady, R.D.; Sun, M.; Huang, C.; Barlow, C.K.; et al. Disease-modifying effects of sodium selenate in a model of drug-resistant, temporal lobe epilepsy. eLife 2023, 12, e78877. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.; Bankstahl, M.; Löscher, W. Inter-individual variation in the effect of antiepileptic drugs in the intrahippocampal kainate model of mesial temporal lobe epilepsy in mice. Neuropharmacology 2015, 90, 53–62. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucchi, C.; Marcucci, M.; Aledresi, K.A.M.S.; Costa, A.-M.; Cannazza, G.; Biagini, G. Subthreshold Cannabidiol Potentiates Levetiracetam in the Kainic Acid Model of Temporal Lobe Epilepsy: A Pilot Study. Pharmaceuticals 2024, 17, 1187. https://doi.org/10.3390/ph17091187
Lucchi C, Marcucci M, Aledresi KAMS, Costa A-M, Cannazza G, Biagini G. Subthreshold Cannabidiol Potentiates Levetiracetam in the Kainic Acid Model of Temporal Lobe Epilepsy: A Pilot Study. Pharmaceuticals. 2024; 17(9):1187. https://doi.org/10.3390/ph17091187
Chicago/Turabian StyleLucchi, Chiara, Mattia Marcucci, Kawther Ameen Muhammed Saeed Aledresi, Anna-Maria Costa, Giuseppe Cannazza, and Giuseppe Biagini. 2024. "Subthreshold Cannabidiol Potentiates Levetiracetam in the Kainic Acid Model of Temporal Lobe Epilepsy: A Pilot Study" Pharmaceuticals 17, no. 9: 1187. https://doi.org/10.3390/ph17091187
APA StyleLucchi, C., Marcucci, M., Aledresi, K. A. M. S., Costa, A.-M., Cannazza, G., & Biagini, G. (2024). Subthreshold Cannabidiol Potentiates Levetiracetam in the Kainic Acid Model of Temporal Lobe Epilepsy: A Pilot Study. Pharmaceuticals, 17(9), 1187. https://doi.org/10.3390/ph17091187