

Effect of Acute Ketamine Treatment on Sympathetic Regulation Indexed by Electrodermal Activity in Adolescent Major Depression
 , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. Characteristics of the Studied Group
2.2. The EDA and Hemodynamic Parameters
2.3. Depressive Symptomatology
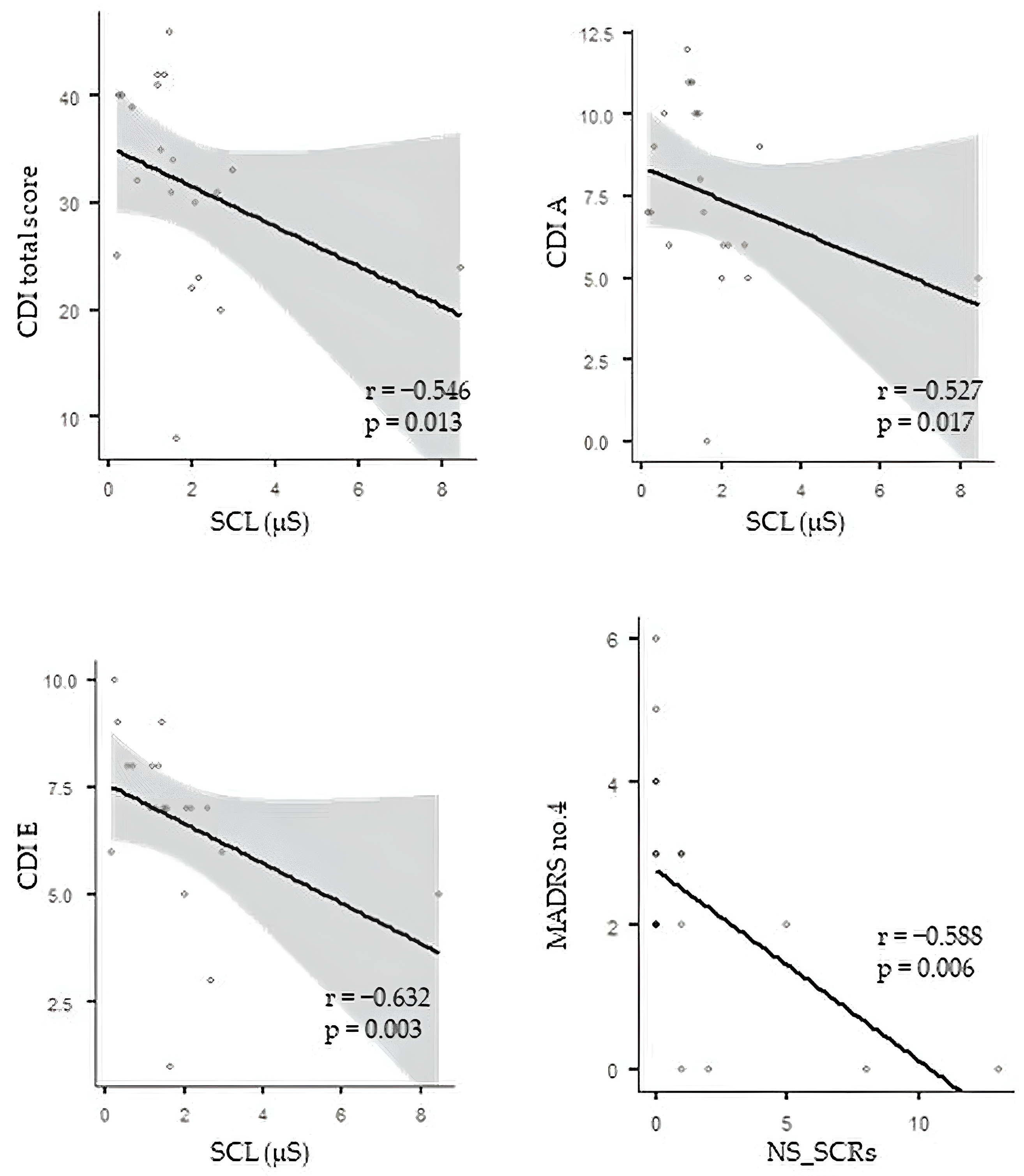
2.4. Correlation Analysis between EDA and Depressive Symptoms
2.5. Correlation Analysis between Hemodynamic Measures and Depressive Symptoms
3. Discussion
Limitations of the Study
4. Materials and Methods
4.1. Ethics Statement
4.2. Subjects
4.3. Continual Recording of Electrodermal Activity
EDA Evaluated Parameters
4.4. Assessment of Depressive Symptomatology
4.4.1. The Montgomery–Asberg Depression Rating Scale
4.4.2. The Children’s Depression Inventory
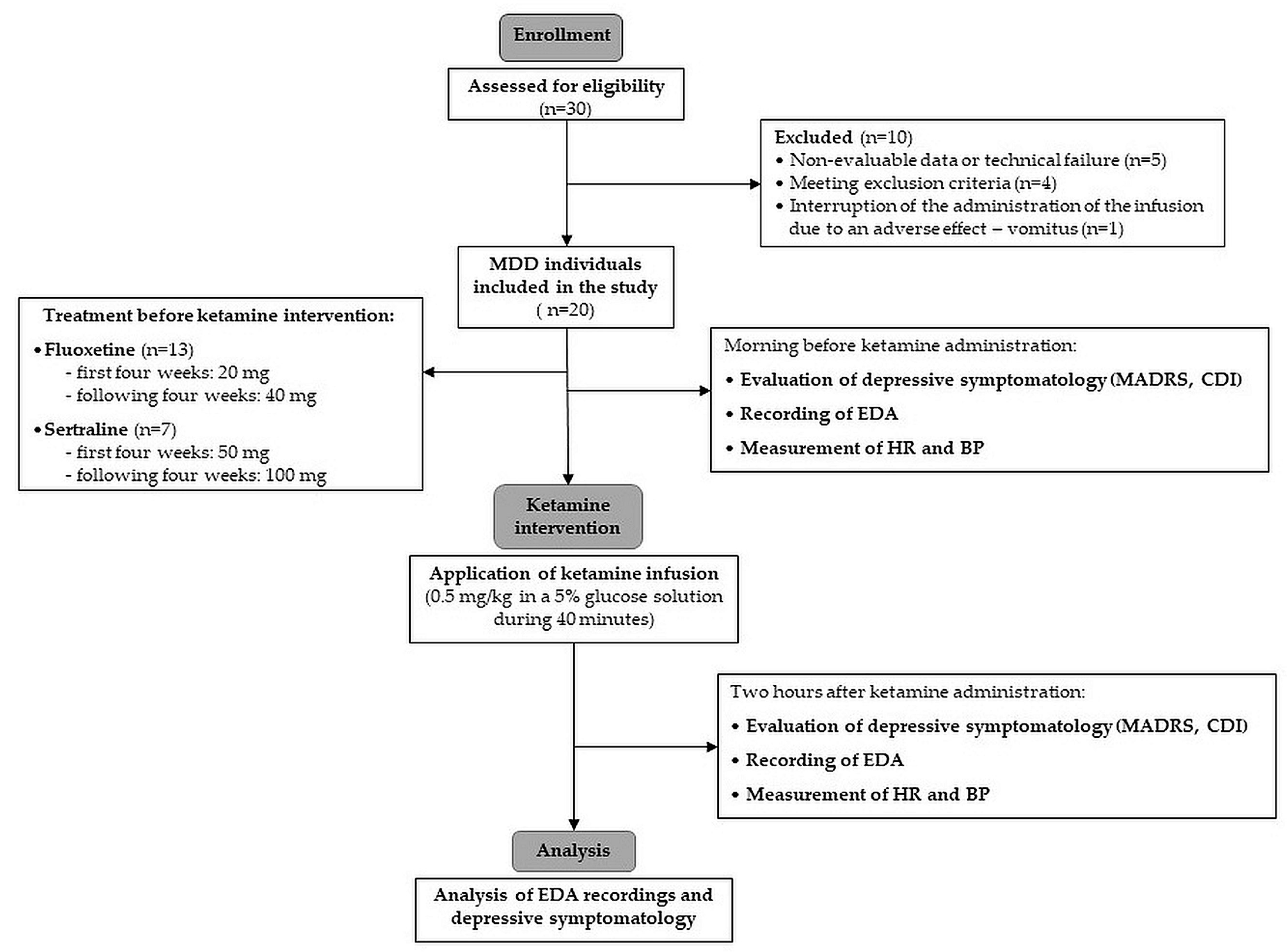
4.5. Study Protocol
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shorey, S.; Ng, E.D.; Wong, C.H.J. Global Prevalence of Depression and Elevated Depressive Symptoms among Adolescents: A Systematic Review and Meta-analysis. Br. J. Clin. Psychol. 2022, 61, 287–305. [Google Scholar] [CrossRef]
- Dwyer, J.B.; Landeros-Weisenberger, A.; Johnson, J.A.; Londono Tobon, A.; Flores, J.M.; Nasir, M.; Couloures, K.; Sanacora, G.; Bloch, M.H. Efficacy of Intravenous Ketamine in Adolescent Treatment-Resistant Depression: A Randomized Midazolam-Controlled Trial. Am. J. Psychiatry 2021, 178, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Fergusson, D.M.; Woodward, L.J. Mental Health, Educational, and Social Role Outcomes of Adolescents with Depression. Arch. Gen. Psychiatry 2002, 59, 225–231. [Google Scholar] [CrossRef] [PubMed]
- NICE. NICE Recommendations. Depression in Children and Young People: Identification and Management. Guidance. Available online: https://www.nice.org.uk/guidance/ng134/chapter/Recommendations (accessed on 10 February 2024).
- Dwyer, J.B.; Stringaris, A.; Brent, D.A.; Bloch, M.H. Annual Research Review: Defining and Treating Pediatric Treatment-resistant Depression. J. Child Psychol. Psychiatry 2020, 61, 312–332. [Google Scholar] [CrossRef] [PubMed]
- Brent, D.; Emslie, G.; Clarke, G.; Wagner, K.D.; Asarnow, J.R.; Keller, M.; Vitiello, B.; Ritz, L.; Iyengar, S.; Abebe, K.; et al. Switching to Another SSRI or to Venlafaxine with or without Cognitive Behavioral Therapy for Adolescents With SSRI-Resistant Depression. JAMA J. Am. Med. Assoc. 2008, 299, 901–913. [Google Scholar] [CrossRef]
- March, J.; Silva, S.; Petrycki, S.; Curry, J.; Wells, K.; Fairbank, J.; Burns, B.; Domino, M.; McNulty, S.; Vitiello, B.; et al. Fluoxetine, Cognitive-Behavioral Therapy, and Their Combination for Adolescents with Depression: Treatment for Adolescents with Depression Study (TADS) Randomized Controlled Trial. JAMA 2004, 292, 807–820. [Google Scholar] [CrossRef] [PubMed]
- Maalouf, F.T.; Atwi, M.; Brent, D.A. Treatment-Resistant Depression in Adolescents: Review and Updates on Clinical Management. Depress. Anxiety 2011, 28, 946–954. [Google Scholar] [CrossRef] [PubMed]
- Berman, R.M.; Cappiello, A.; Anand, A.; Oren, D.A.; Heninger, G.R.; Charney, D.S.; Krystal, J.H. Antidepressant Effects of Ketamine in Depressed Patients. Biol. Psychiatry 2000, 47, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Maina, G.; Adami, M.; Ascione, G.; Bondi, E.; De Berardis, D.; Delmonte, D.; Maffezzoli, S.; Martinotti, G.; Nivoli, A.; Ottavianelli, E.; et al. Nationwide Consensus on the Clinical Management of Treatment-Resistant Depression in Italy: A Delphi Panel. Ann. Gen. Psychiatry 2023, 22, 48. [Google Scholar] [CrossRef]
- Correia-Melo, F.S.; Leal, G.C.; Carvalho, M.S.; Jesus-Nunes, A.P.; Ferreira, C.B.N.; Vieira, F.; Magnavita, G.; Vale, L.A.S.; Mello, R.P.; Nakahira, C.; et al. Comparative Study of Esketamine and Racemic Ketamine in Treatment-Resistant Depression. Medicine 2018, 97, e12414. [Google Scholar] [CrossRef]
- Schatzberg, A.F. A Word to the Wise About Intranasal Esketamine. Am. J. Psychiatry 2019, 176, 422–424. [Google Scholar] [CrossRef]
- Vlerick, L.; Devreese, M.; Peremans, K.; Dockx, R.; Croubels, S.; Duchateau, L.; Polis, I. Pharmacokinetics, Absolute Bioavailability and Tolerability of Ketamine after Intranasal Administration to Dexmedetomidine Sedated Dogs. PLoS ONE 2020, 15, e0227762. [Google Scholar] [CrossRef]
- Singh, B.; Kung, S.; Pazdernik, V.; Schak, K.M.; Geske, J.; Schulte, P.J.; Frye, M.A.; Vande Voort, J.L. Comparative Effectiveness of Intravenous Ketamine and Intranasal Esketamine in Clinical Practice Among Patients with Treatment-Refractory Depression: An Observational Study. J. Clin. Psychiatry 2023, 84, 22m14548. [Google Scholar] [CrossRef]
- Wilkinson, S.T.; Ballard, E.D.; Bloch, M.H.; Mathew, S.J.; Murrough, J.W.; Feder, A.; Sos, P.; Wang, G.; Zarate, C.A.; Sanacora, G. The Effect of a Single Dose of Intravenous Ketamine on Suicidal Ideation: A Systematic Review and Individual Participant Data Meta-Analysis. Am. J. Psychiatry 2018, 175, 150–158. [Google Scholar] [CrossRef]
- Grunebaum, M.F.; Galfalvy, H.C.; Choo, T.-H.; Keilp, J.G.; Moitra, V.K.; Parris, M.S.; Marver, J.E.; Burke, A.K.; Milak, M.S.; Sublette, M.E.; et al. Ketamine for Rapid Reduction of Suicidal Thoughts in Major Depression: A Midazolam-Controlled Randomized Clinical Trial. Am. J. Psychiatry 2018, 175, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Zanos, P.; Moaddel, R.; Morris, P.J.; Riggs, L.M.; Highland, J.N.; Georgiou, P.; Pereira, E.F.R.; Albuquerque, E.X.; Thomas, C.J.; Zarate, C.A.; et al. Ketamine and Ketamine Metabolite Pharmacology: Insights into Therapeutic Mechanisms. Pharmacol. Rev. 2018, 70, 621–660. [Google Scholar] [CrossRef] [PubMed]
- Pettorruso, M.; d’Andrea, G.; Di Carlo, F.; De Risio, L.; Zoratto, F.; Miuli, A.; Benatti, B.; Vismara, M.; Pompili, E.; Nicolò, G.; et al. Comparing Fast-Acting Interventions for Treatment-Resistant Depression: An Explorative Study of Accelerated HF-rTMS versus Intranasal Esketamine. Brain Stimulat. 2023, 16, 1041–1043. [Google Scholar] [CrossRef] [PubMed]
- Meshkat, S.; Rosenblat, J.D.; Ho, R.C.; Rhee, T.G.; Cao, B.; Ceban, F.; Danayan, K.; Chisamore, N.; Vincenzo, J.D.D.; McIntyre, R.S. Ketamine Use in Pediatric Depression: A Systematic Review. Psychiatry Res. 2022, 317, 114911. [Google Scholar] [CrossRef] [PubMed]
- Hijazi, Y.; Boulieu, R. Contribution of CYP3A4, CYP2B6, and CYP2C9 Isoforms to N-Demethylation of Ketamine in Human Liver Microsomes. Drug Metab. Dispos. 2002, 30, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Fanta, S.; Kinnunen, M.; Backman, J.T.; Kalso, E. Population Pharmacokinetics of S-Ketamine and Norketamine in Healthy Volunteers after Intravenous and Oral Dosing. Eur. J. Clin. Pharmacol. 2015, 71, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, A.; Theurillat, R.; Lassahn, P.; Mevissen, M.; Thormann, W. CE Provides Evidence of the Stereoselective Hydroxylation of Norketamine in Equines. Electrophoresis 2009, 30, 2912–2921. [Google Scholar] [CrossRef]
- Dinis-Oliveira, R.J. Metabolism and Metabolomics of Ketamine: A Toxicological Approach. Forensic Sci. Res. 2017, 2, 2–10. [Google Scholar] [CrossRef]
- Mion, G.; Villevieille, T. Ketamine Pharmacology: An Update (Pharmacodynamics and Molecular Aspects, Recent Findings). CNS Neurosci. Ther. 2013, 19, 370–380. [Google Scholar] [CrossRef]
- Edginton, A.N.; Schmitt, W.; Voith, B.; Willmann, S. A Mechanistic Approach for the Scaling of Clearance in Children. Clin. Pharmacokinet. 2006, 45, 683–704. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, C.H.; Nelson, W.L. The Relationship of Ketamine Requirement to Age in Pediatric Patients. Anesthesiology 1974, 40, 507–508. [Google Scholar] [CrossRef]
- White, P.F.; Schüttler, J.; Shafer, A.; Stanski, D.R.; Horai, Y.; Trevor, A.J. Comparative Pharmacology of the Ketamine Isomers. Br. J. Anaesth. 1985, 57, 197–203. [Google Scholar] [CrossRef]
- Adamowicz, P.; Kala, M. Urinary Excretion Rates of Ketamine and Norketamine Following Therapeutic Ketamine Administration: Method and Detection Window Considerations. J. Anal. Toxicol. 2005, 29, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Cook, D.R.; Stiller, R.; Dayton, P. Pharmacokinetics of Ketamine (K) in Infants and Small Children. Anesthesiology 1982, 57, A428. [Google Scholar] [CrossRef]
- Kamp, J.; Olofsen, E.; Henthorn, T.K.; Van Velzen, M.; Niesters, M.; Dahan, A.; for the Ketamine Pharmacokinetic Study Group. Ketamine Pharmacokinetics: A Systematic Review of the Literature, Meta-analysis, and Population Analysis. Anesthesiology 2020, 133, 1192–1213. [Google Scholar] [CrossRef]
- Herd, D.; Anderson, B.J. Ketamine Disposition in Children Presenting for Procedural Sedation and Analgesia in a Children’s Emergency Department. Pediatr. Anesth. 2007, 17, 622–629. [Google Scholar] [CrossRef]
- Sleigh, J.; Harvey, M.; Voss, L.; Denny, B. Ketamine—More Mechanisms of Action than Just NMDA Blockade. Trends Anaesth. Crit. Care 2014, 4, 76–81. [Google Scholar] [CrossRef]
- Abdallah, C.G.; Adams, T.G.; Kelmendi, B.; Esterlis, I.; Sanacora, G.; Krystal, J.H. Ketamine’s mechanism of action: A path to rapid-acting antidepressants. Depress. Anxiety 2016, 33, 689–697. [Google Scholar] [CrossRef]
- Li, N.; Lee, B.; Liu, R.-J.; Banasr, M.; Dwyer, J.M.; Iwata, M.; Li, X.-Y.; Aghajanian, G.; Duman, R.S. mTOR-Dependent Synapse Formation Underlies the Rapid Antidepressant Effects of NMDA Antagonists. Science 2010, 329, 959–964. [Google Scholar] [CrossRef]
- Anand, A.; Li, Y.; Wang, Y.; Wu, J.; Gao, S.; Bukhari, L.; Mathews, V.P.; Kalnin, A.; Lowe, M.J. Antidepressant Effect on Connectivity of the Mood-Regulating Circuit: An fMRI Study. Neuropsychopharmacology 2005, 30, 1334–1344. [Google Scholar] [CrossRef]
- Bellato, A.; Sesso, G.; Milone, A.; Masi, G.; Cortese, S. Systematic Review and Meta-Analysis: Altered Autonomic Functioning in Youths With Emotional Dysregulation. J. Am. Acad. Child Adolesc. Psychiatry 2023, 63, 216–230. [Google Scholar] [CrossRef]
- Charkoudian, N.; Rabbitts, J.A. Sympathetic Neural Mechanisms in Human Cardiovascular Health and Disease. Mayo Clin. Proc. 2009, 84, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Braithwaite, J.; Watson, D.; Jones, R.; Rowe, M.A. Guide for Analysing Electrodermal Activity & Skin Conductance Responses for Psychological Experiments; CTIT Technical Report Series; Behavioural Brain Sciences Centre, University of Birmingham: Birmingham, UK, 2013. [Google Scholar]
- Andreassi, J.L. Psychophysiology: Human Behavior and Physiological Response, 4th ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2000; pp. xxvi, 458. ISBN 978-0-8058-2832-0. [Google Scholar]
- Dawson, M.E.; Schell, A.M.; Filion, D.L.; Berntson, G.G. The Electrodermal System; Cacioppo, J.T., Tassinary, L.G., Berntson, G., Eds.; Cambridge University Press: Cambridge, UK, 2007; pp. 157–181. [Google Scholar]
- Boucsein, W. Electrodermal Activity; Springer: Boston, MA, USA, 2012; ISBN 978-1-4614-1125-3. [Google Scholar]
- Caruelle, D.; Gustafsson, A.; Shams, P.; Lervik-Olsen, L. The Use of Electrodermal Activity (EDA) Measurement to Understand Consumer Emotions—A Literature Review and a Call for Action. J. Bus. Res. 2019, 104, 146–160. [Google Scholar] [CrossRef]
- Mestanikova, A.; Ondrejka, I.; Mestanik, M.; Hrtanek, I.; Snircova, E.; Tonhajzerova, I. Electrodermal Activity in Adolescent Depression. In Pulmonary Infection and Inflammation; Pokorski, M., Ed.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Switzerland, 2016; Volume 935, pp. 83–88. ISBN 978-3-319-44484-0. [Google Scholar]
- Erath, S.A.; Su, S.; Tu, K.M. Electrodermal Reactivity Moderates the Prospective Association Between Peer Victimization and Depressive Symptoms in Early Adolescence. J. Clin. Child Adolesc. Psychol. 2018, 47, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- Lipsitz, O.; Di Vincenzo, J.D.; Rodrigues, N.B.; Cha, D.S.; Lee, Y.; Greenberg, D.; Teopiz, K.M.; Ho, R.C.; Cao, B.; Lin, K.; et al. Safety, Tolerability, and Real-World Effectiveness of Intravenous Ketamine in Older Adults with Treatment-Resistant Depression: A Case Series. Am. J. Geriatr. Psychiatry 2021, 29, 899–913. [Google Scholar] [CrossRef] [PubMed]
- Cullen, K.R.; Amatya, P.; Roback, M.G.; Albott, C.S.; Westlund Schreiner, M.; Ren, Y.; Eberly, L.E.; Carstedt, P.; Samikoglu, A.; Gunlicks-Stoessel, M.; et al. Intravenous Ketamine for Adolescents with Treatment-Resistant Depression: An Open-Label Study. J. Child Adolesc. Psychopharmacol. 2018, 28, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.J.; Hasassri, E. Ketamine for Adolescent Depression: An Overview and Considerations for Future Directions. Am. J. Psychiatry Resid. J. 2022, 17, 2–4. [Google Scholar] [CrossRef]
- Weber, G.; Yao, J.; Binns, S.; Namkoong, S. Case Report of Subanesthetic Intravenous Ketamine Infusion for the Treatment of Neuropathic Pain and Depression with Suicidal Features in a Pediatric Patient. Case Rep. Anesthesiol. 2018, 2018, 9375910. [Google Scholar] [CrossRef]
- Kohrs, R.; Durieux, M.E. Ketamine: Teaching an Old Drug New Tricks. Anesth. Analg. 1998, 87, 1186–1193. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Shu, S.; Bayliss, D.A. HCN1 Channel Subunits Are a Molecular Substrate for Hypnotic Actions of Ketamine. J. Neurosci. 2009, 29, 600–609. [Google Scholar] [CrossRef]
- Durieux, M.E. Inhibition by Ketamine of Muscarinic Acetylcholine Receptor Function. Anesth. Analg. 1995, 81, 57–62. [Google Scholar] [CrossRef]
- Kapur, S.; Seeman, P. NMDA Receptor Antagonists Ketamine and PCP Have Direct Effects on the Dopamine D2 and Serotonin 5-HT2 Receptors—Implications for Models of Schizophrenia. Mol. Psychiatry 2002, 7, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Seeman, P.; Ko, F.; Tallerico, T. Dopamine Receptor Contribution to the Action of PCP, LSD and Ketamine Psychotomimetics. Mol. Psychiatry 2005, 10, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Lisek, M.; Boczek, T.; Ferenc, B.; Zylinska, L. Regional Brain Dysregulation of Ca2+-Handling Systems in Ketamine-Induced Rat Model of Experimental Psychosis. Cell Tissue Res. 2016, 363, 609–620. [Google Scholar] [CrossRef] [PubMed]
- Castillo, A.; Dubois, J.; Field, R.M.; Fishburn, F.; Gundran, A.; Ho, W.C.; Jawhar, S.; Kates-Harbeck, J.; Aghajan, Z.M.; Miller, N.; et al. Measuring Acute Effects of Subanesthetic Ketamine on Cerebrovascular Hemodynamics in Humans Using TD-fNIRS. Sci. Rep. 2023, 13, 11665. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.H.; Mendez-David, I.; Defaix, C.; Guiard, B.P.; Tritschler, L.; David, D.J.; Gardier, A.M. Ketamine Treatment Involves Medial Prefrontal Cortex Serotonin to Induce a Rapid Antidepressant-like Activity in BALB/cJ Mice. Neuropharmacology 2017, 112, 198–209. [Google Scholar] [CrossRef]
- Qing-Ping, W.; Nakai, Y. The Dorsal Raphe: An Important Nucleus in Pain Modulation. Brain Res. Bull. 1994, 34, 575–585. [Google Scholar] [CrossRef]
- Williams, N.R.; Heifets, B.D.; Blasey, C.; Sudheimer, K.; Pannu, J.; Pankow, H.; Hawkins, J.; Birnbaum, J.; Lyons, D.M.; Rodriguez, C.I.; et al. Attenuation of Antidepressant Effects of Ketamine by Opioid Receptor Antagonism. Am. J. Psychiatry 2018, 175, 1205–1215. [Google Scholar] [CrossRef]
- Mineur, Y.S.; Picciotto, M.R. Nicotine Receptors and Depression: Revisiting and Revising the Cholinergic Hypothesis. Trends Pharmacol. Sci. 2010, 31, 580–586. [Google Scholar] [CrossRef]
- Moaddel, R.; Abdrakhmanova, G.; Kozak, J.; Jozwiak, K.; Toll, L.; Jimenez, L.; Rosenberg, A.; Tran, T.; Xiao, Y.; Zarate, C.A.; et al. Sub-Anesthetic Concentrations of (R,S)-Ketamine Metabolites Inhibit Acetylcholine-Evoked Currents in A7 Nicotinic Acetylcholine Receptors. Eur. J. Pharmacol. 2013, 698, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Hirota, K.; Lambert, D.G. Anaesthesia-Related Drugs and SARS-CoV-2 Infection. Br. J. Anaesth. 2021, 127, e32–e34. [Google Scholar] [CrossRef] [PubMed]
- Robson, M.J.; Elliott, M.; Seminerio, M.J.; Matsumoto, R.R. Evaluation of Sigma (σ) Receptors in the Antidepressant-like Effects of Ketamine in Vitro and in Vivo. Eur. Neuropsychopharmacol. 2012, 22, 308–317. [Google Scholar] [CrossRef]
- Wang, J.; Mack, A.L.; Coop, A.; Matsumoto, R.R. Novel Sigma (σ) Receptor Agonists Produce Antidepressant-like Effects in Mice. Eur. Neuropsychopharmacol. 2007, 17, 708–716. [Google Scholar] [CrossRef]
- Kim, C.S.; Chang, P.Y.; Johnston, D. Enhancement of Dorsal Hippocampal Activity by Knockdown of HCN1 Channels Leads to Anxiolytic- and Antidepressant-like Behaviors. Neuron 2012, 75, 503–516. [Google Scholar] [CrossRef]
- Zhang, K.; Xu, T.; Yuan, Z.; Wei, Z.; Yamaki, V.N.; Huang, M.; Huganir, R.L.; Cai, X. Essential Roles of AMPA Receptor GluA1 Phosphorylation and Presynaptic HCN Channels in Fast-Acting Antidepressant Responses of Ketamine. Sci. Signal. 2016, 9, ra123. [Google Scholar] [CrossRef]
- Han, Y.; Heuermann, R.J.; Lyman, K.A.; Fisher, D.; Ismail, Q.-A.; Chetkovich, D.M. HCN-Channel Dendritic Targeting Requires Bipartite Interaction with TRIP8b and Regulates Antidepressant-like Behavioral Effects. Mol. Psychiatry 2017, 22, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Lopez, J.P.; Lücken, M.D.; Brivio, E.; Karamihalev, S.; Kos, A.; De Donno, C.; Benjamin, A.; Yang, H.; Dick, A.L.W.; Stoffel, R.; et al. Ketamine Exerts Its Sustained Antidepressant Effects via Cell-Type-Specific Regulation of Kcnq2. Neuron 2022, 110, 2283–2298. [Google Scholar] [CrossRef] [PubMed]
- Nutt, D.; Demyttenaere, K.; Janka, Z.; Aarre, T.; Bourin, M.; Canonico, P.L.; Carrasco, J.L.; Stahl, S. The Other Face of Depression, Reduced Positive Affect: The Role of Catecholamines in Causation and Cure. J. Psychopharmacol. Oxf. Engl. 2007, 21, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Wilkowska, A.; Wiglusz, M.S.; Gałuszko-Wegielnik, M.; Włodarczyk, A.; Cubała, W.J. Antianhedonic Effect of Repeated Ketamine Infusions in Patients With Treatment Resistant Depression. Front. Psychiatry 2021, 12, 704330. [Google Scholar] [CrossRef] [PubMed]
- Lally, N.; Nugent, A.C.; Luckenbaugh, D.A.; Niciu, M.J.; Roiser, J.P.; Zarate, C.A. Neural Correlates of Change in Major Depressive Disorder Anhedonia Following Open-Label Ketamine. J. Psychopharmacol. 2015, 29, 596–607. [Google Scholar] [CrossRef] [PubMed]
- Valenza, G.; Citi, L.; Saul, J.P.; Barbieri, R. Measures of Sympathetic and Parasympathetic Autonomic Outflow from Heartbeat Dynamics. J. Appl. Physiol. 2018, 125, 19–39. [Google Scholar] [CrossRef] [PubMed]
- Valenza, G. Depression as a Cardiovascular Disorder: Central-Autonomic Network, Brain-Heart Axis, and Vagal Perspectives of Low Mood. Front. Netw. Physiol. 2023, 3, 1125495. [Google Scholar] [CrossRef] [PubMed]
- Liebe, T.; Li, S.; Lord, A.; Colic, L.; Krause, A.L.; Batra, A.; Kretzschmar, M.A.; Sweeney-Reed, C.M.; Behnisch, G.; Schott, B.H.; et al. Factors Influencing the Cardiovascular Response to Subanesthetic Ketamine: A Randomized, Placebo-Controlled Trial. Int. J. Neuropsychopharmacol. 2017, 20, 909–918. [Google Scholar] [CrossRef]
- Dowdy, E.G.; Kaya, K. Studies of the Mechanism of Cardiovascular Responses to CI-581. Anesthesiology 1968, 29, 931–942. [Google Scholar] [CrossRef]
- Okamoto, H.; Hoka, S.; Kawasaki, T.; Okuyama, T.; Takahashi, S. L-Arginine Attenuates Ketamine-Induced Increase in Renal Sympathetic Nerve Activity. Anesthesiology 1994, 81, 137–146. [Google Scholar] [CrossRef]
- Irnaten, M.; Wang, J.; Chang, K.S.K.; Andresen, M.C.; Mendelowitz, D. Ketamine Inhibits Sodium Currents in Identified Cardiac Parasympathetic Neurons in Nucleus Ambiguus. Anesthesiology 2002, 96, 659–666. [Google Scholar] [CrossRef]
- Mendelowitz, D. Advances in Parasympathetic Control of Heart Rate and Cardiac Function. Physiology 1999, 14, 155–161. [Google Scholar] [CrossRef]
- Kienbaum, P.; Heuter, T.; Pavlakovic, G.; Michel, M.C.; Peters, J. S (+)-Ketamine Increases Muscle Sympathetic Activity and Maintains the Neural Response to Hypotensive Challenges in Humans. Anesthesiology 2001, 94, 252–258. [Google Scholar] [CrossRef]
- Couch, G.A.; White, M.P.; De Gray, L.E. Central Nervous System Stimulants: Basic Pharmacology and Relevance to Anaesthesia and Critical Care. Anaesth. Intensive Care Med. 2020, 21, 503–511. [Google Scholar] [CrossRef]
- Lalonde, G. Miller’s Anesthesia, Eighth Edition: Ronald D. Miller, Neal H. Cohen, Lars I. Eriksson, Lee A. Fleisher, Jeanine P. Wiener-Kronish, William L. Young. Elsevier, Philadelphia, 2015, 449$, 3576 Pages. IBSN 978-0-7020-5283-5. Can. J. Anesth. Can. Anesth. 2015, 62, 558–559. [Google Scholar] [CrossRef]
- Salt, P.J.; Barnes, P.K.; Beswick, F.J. Inhibition of Neuronal and Extraneuronal Uptake of Noradrenaline by Ketamine in the Isolated Perfused Rat Heart. Br. J. Anaesth. 1979, 51, 835–838. [Google Scholar] [CrossRef]
- Bonnet, A.; Naveteur, J. Electrodermal Activity in Low Back Pain Patients with and without Co-Morbid Depression. Int. J. Psychophysiol. 2004, 53, 37–44. [Google Scholar] [CrossRef]
- Carney, R.M.; Hong, B.A.; Kulkarni, S.; Kapila, A. A Comparison of EMG and SCL in Normal and Depressed Subjects. Pavlov. J. Biol. Sci. 1981, 16, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Miquel, M.; Fuentes, I.; Garcia-Merita, M.; Rojo, L. Habituation and Sensitization Processes in Depressive Disorders. Psychopathology 1999, 32, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Rottenberg, J.; Gross, J.J.; Wilhelm, F.H.; Najmi, S.; Gotlib, I.H. Crying Threshold and Intensity in Major Depressive Disorder. J. Abnorm. Psychol. 2002, 111, 302–312. [Google Scholar] [CrossRef]
- Tsai, J.L.; Pole, N.; Levenson, R.W.; Muñoz, R.F. The Effects of Depression on the Emotional Responses of Spanish-Speaking Latinas. Cultur. Divers. Ethnic Minor. Psychol. 2003, 9, 49–63. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.Y.; Jang, E.H.; Kim, S.; Choi, K.W.; Jeon, H.J.; Yu, H.Y.; Byun, S. Automatic Detection of Major Depressive Disorder Using Electrodermal Activity. Sci. Rep. 2018, 8, 17030. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-555-8. [Google Scholar]
- Platt, J.M.; Bates, L.; Jager, J.; McLaughlin, K.A.; Keyes, K.M. Is the US Gender Gap in Depression Changing Over Time? A Meta-Regression. Am. J. Epidemiol. 2021, 190, 1190–1206. [Google Scholar] [CrossRef]
- Harteveld, L.M.; Nederend, I.; Ten Harkel, A.D.J.; Schutte, N.M.; De Rooij, S.R.; Vrijkotte, T.G.M.; Oldenhof, H.; Popma, A.; Jansen, L.M.C.; Suurland, J.; et al. Maturation of the Cardiac Autonomic Nervous System Activity in Children and Adolescents. J. Am. Heart Assoc. 2021, 10, e017405. [Google Scholar] [CrossRef]
- Srivastava, S.; Gangwar, R.; Kumar, A. Safety and Efficacy of Ketamine Infusion in Late Onset Depression, and Conversion to Treatment Response. Indian J. Psychiatry 2015, 57, 328. [Google Scholar] [CrossRef]
- Dwyer, J.B.; Beyer, C.; Wilkinson, S.T.; Ostroff, R.B.; Qayyum, Z.; Bloch, M.H. Ketamine as a Treatment for Adolescent Depression: A Case Report. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 352–354. [Google Scholar] [CrossRef] [PubMed]
- Thought Technology Ltd. FlexComp Infiniti Hardware Manual 2003. Available online: https://thoughttechnology.com/content/docs/manual/SA7560%20rev.%204%20FlexComp%20Infiniti%20User%20Manual%20(2).pdf (accessed on 12 December 2023).
- Blain, S.; Power, S.D.; Sejdic, E.; Mihailidis, A.; Chau, T. A Cardiorespiratory Classifier of Voluntary and Involuntary Electrodermal Activity. Biomed. Eng. OnLine 2010, 9, 11. [Google Scholar] [CrossRef]
- Poh, M.; Swenson, N.C.; Picard, R.W. A Wearable Sensor for Unobtrusive, Long-Term Assessment of Electrodermal Activity. IEEE Trans. Biomed. Eng. 2010, 57, 1243–1252. [Google Scholar] [CrossRef]
- Posada-Quintero, H.F.; Florian, J.P.; Orjuela-Cañón, A.D.; Aljama-Corrales, T.; Charleston-Villalobos, S.; Chon, K.H. Power Spectral Density Analysis of Electrodermal Activity for Sympathetic Function Assessment. Ann. Biomed. Eng. 2016, 44, 3124–3135. [Google Scholar] [CrossRef]
- Turpin, G.; Grandfield, T. Electrodermal Activity. In Encyclopedia of Stress; Elsevier: Amsterdam, The Netherlands, 2007; pp. 899–902. ISBN 978-0-12-373947-6. [Google Scholar]
- Montgomery, S.A.; Åsberg, M. A New Depression Scale Designed to Be Sensitive to Change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef]
- Müller, M.J.; Szegedi, A.; Wetzel, H.; Benkert, O. Moderate and Severe Depression. J. Affect. Disord. 2000, 60, 137–140. [Google Scholar] [CrossRef]
- Smucker, M.R.; Craighead, W.E.; Craighead, L.W.; Green, B.J. Normative and Reliability Data for the Children’s Depression Inventory. J. Abnorm. Child Psychol. 1986, 14, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, M. The Children’s Depression, Inventory (CDI). Psychopharmacol. Bull. 1985, 21, 995–998. [Google Scholar] [PubMed]
- Lee, S.; Lee, D.K. What Is the Proper Way to Apply the Multiple Comparison Test? Korean J. Anesthesiol. 2018, 71, 353–360. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Number of participants (n) | 20 |
| Average age (yrs.) | 15.0 ± 1.46 |
| Sex | Only female |
| Mean BMI (kg/m2) | 20.3 ± 2.68 |
| Current AD treatment | 0 |
| Previous AD treatment | Fluoxetine (n = 13) |
| First four weeks: 20 mg | |
| Following four weeks: 40 mg | |
| Sertraline (n = 7) | |
| First four weeks: 50 mg | |
| Following four weeks: 100 mg |
| Variable | n | Before Ketamine Treatment | Two Hours after the End of Ketamine Treatment | Adjusted p-Value |
|---|---|---|---|---|
| EDA measures | ||||
| SCL (μS) | 20 | 1.80 ± 1.77 | 1.71 ± 1.38 | 0.820 |
| NS_SCRs | 20 | 1.60 ± 3.36 | 1.85 ± 3.36 | 0.823 |
| Hemodynamic measures | ||||
| HR (bpm) | 20 | 92.6 ± 7.7 | 97.0 ± 11.9 | 0.106 |
| SBP (mmHg) | 20 | 106.6 ± 13.4 | 108.8 ± 16.6 | 0.544 |
| DBP (mmHg) | 20 | 62.9 ± 8.5 | 62.3 ± 9.0 | 0.776 |
| Depression measures | ||||
| MADRS total score | 20 | 32.30 ± 9.21 | 16.40 ± 10.80 | <0.001 |
| MADRS no. 1 (apparent sadness) | 20 | 3.95 ± 1.39 | 1.85 ± 1.35 | <0.001 |
| MADRS no. 2 (reported sadness) | 20 | 4.35 ± 1.14 | 2.30 ± 1.66 | <0.001 |
| MADRS no. 3 (inner tension) | 20 | 3.50 ± 1.05 | 1.80 ± 1.51 | <0.001 |
| MADRS no. 4 (reduced sleep) | 20 | 2.35 ± 1.63 | 1.45 ± 1.57 | 0.092 |
| MADRS no. 5 (reduced appetite) | 20 | 1.85 ± 2.08 | 1.20 ± 1.36 | 0.203 |
| MADRS no. 6 (concentration difficulties) | 20 | 3.10 ± 1.33 | 1.90 ± 1.17 | 0.003 |
| MADRS no. 7 (lassitude) | 20 | 3.30 ± 1.59 | 1.15 ± 1.35 | <0.001 |
| MADRS no. 8 (inability to feel) | 20 | 2.00 ± 1.89 | 0.70 ± 0.92 | 0.006 |
| MADRS no. 9 (pessimistic thoughts) | 20 | 3.55 ± 1.43 | 2.35 ± 1.50 | 0.001 |
| MADRS no. 10 (suicidal thoughts) | 20 | 4.35 ± 1.69 | 1.70 ± 1.38 | <0.001 |
| CDI total score | 20 | 31.90 ± 9.43 | 27.6 ± 13.4 | 0.018 |
| CDI A (negative mood) | 20 | 7.50 ± 2.84 | 6.20 ± 3.68 | 0.012 |
| CDI B (interpersonal problems) | 20 | 3.35 ± 1.31 | 2.90 ± 1.71 | 0.083 |
| CDI C (ineffectiveness) | 20 | 5.55 ± 1.96 | 5.15 ± 2.70 | 0.413 |
| CDI D (anhedonia) | 20 | 8.75 ± 3.13 | 7.95 ± 3.78 | 0.072 |
| CDI E (negative self-esteem) | 20 | 6.75 ± 2.07 | 5.35 ± 2.70 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovacova, V.; Macejova, A.; Tonhajzerova, I.; Visnovcova, Z.; Ferencova, N.; Mlyncekova, Z.; Kukucka, T.; Farsky, I.; Nosal, S.; Ondrejka, I. Effect of Acute Ketamine Treatment on Sympathetic Regulation Indexed by Electrodermal Activity in Adolescent Major Depression. Pharmaceuticals 2024, 17, 358. https://doi.org/10.3390/ph17030358
Kovacova V, Macejova A, Tonhajzerova I, Visnovcova Z, Ferencova N, Mlyncekova Z, Kukucka T, Farsky I, Nosal S, Ondrejka I. Effect of Acute Ketamine Treatment on Sympathetic Regulation Indexed by Electrodermal Activity in Adolescent Major Depression. Pharmaceuticals. 2024; 17(3):358. https://doi.org/10.3390/ph17030358
Chicago/Turabian StyleKovacova, Veronika, Andrea Macejova, Ingrid Tonhajzerova, Zuzana Visnovcova, Nikola Ferencova, Zuzana Mlyncekova, Tomas Kukucka, Ivan Farsky, Slavomir Nosal, and Igor Ondrejka. 2024. "Effect of Acute Ketamine Treatment on Sympathetic Regulation Indexed by Electrodermal Activity in Adolescent Major Depression" Pharmaceuticals 17, no. 3: 358. https://doi.org/10.3390/ph17030358
APA StyleKovacova, V., Macejova, A., Tonhajzerova, I., Visnovcova, Z., Ferencova, N., Mlyncekova, Z., Kukucka, T., Farsky, I., Nosal, S., & Ondrejka, I. (2024). Effect of Acute Ketamine Treatment on Sympathetic Regulation Indexed by Electrodermal Activity in Adolescent Major Depression. Pharmaceuticals, 17(3), 358. https://doi.org/10.3390/ph17030358