
Pembrolizumab-Associated Cardiotoxicity: A Retrospective Analysis of the FDA Adverse Events Reporting System

 ,
,  , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Data Source and Extraction Criteria
4.2. Data Analysis—Descriptive Analysis
4.3. Data Analysis—Disproportionality Analysis
- ROR025 (lower limit of the 95% confidence interval of ROR) > 1 and adverse events > 3;
- IC025 (lower limit of the 95% credibility interval of IC) > 0.
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Teixidó, C.; Vilariño, N.; Reyes, R.; Reguart, N. PD-L1 Expression Testing in Non-Small Cell Lung Cancer. Ther. Adv. Med. Oncol. 2018, 10, 1758835918763493. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, V.; Workman, C.J.; Vignali, D.A.A. LAG-3 as the Third Checkpoint Inhibitor. Nat. Immunol. 2023, 24, 1415–1422. [Google Scholar] [CrossRef] [PubMed]
- Laenens, D.; Yu, Y.; Santens, B.; Jacobs, J.; Beuselinck, B.; Bechter, O.; Wauters, E.; Staessen, J.; Janssens, S.; Van Aelst, L. Incidence of Cardiovascular Events in Patients Treated With Immune Checkpoint Inhibitors. J. Clin. Oncol. 2022, 40, 3430–3438. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Wu, X. Cardiovascular Toxicities Associated with Immune Checkpoint Inhibitors: An Updated Comprehensive Disproportionality Analysis of the FDA Adverse Event Reporting System. J. Clin. Pharm. Ther. 2022, 47, 1576–1584. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; Ernstoff, M.S.; Gardner, J.M.; Ginex, P.; et al. Management of Immune-Related Adverse Events in Patients Treated with Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1714–1768. [Google Scholar] [CrossRef]
- Wang, D.Y.; Salem, J.-E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L.; et al. Fatal Toxic Effects Associated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef]
- Salem, J.-E.; Manouchehri, A.; Moey, M.; Lebrun-Vignes, B.; Bastarache, L.; Pariente, A.; Gobert, A.; Spano, J.-P.; Balko, J.M.; Bonaca, M.P.; et al. Cardiovascular Toxicities Associated with Immune Checkpoint Inhibitors: An Observational, Retrospective, Pharmacovigilance Study. Lancet Oncol. 2018, 19, 1579–1589. [Google Scholar] [CrossRef]
- Michel, L.; Rassaf, T.; Totzeck, M. Cardiotoxicity from Immune Checkpoint Inhibitors. Int. J. Cardiol. Heart Vasc. 2019, 25, 100420. [Google Scholar] [CrossRef] [PubMed]
- Lal, J.C.; Brown, S.-A.; Collier, P.; Cheng, F. A Retrospective Analysis of Cardiovascular Adverse Events Associated with Immune Checkpoint Inhibitors. Cardiooncology 2021, 7, 19. [Google Scholar] [CrossRef]
- Chen, C.; Chen, T.; Liang, J.; Guo, X.; Xu, J.; Zheng, Y.; Guo, Z.; Chi, L.; Wei, L.; Chen, X.; et al. Cardiotoxicity Induced by Immune Checkpoint Inhibitors: A Pharmacovigilance Study from 2014 to 2019 Based on FAERS. Front. Pharmacol. 2021, 12, 616505. [Google Scholar] [CrossRef]
- Dolladille, C.; Akroun, J.; Morice, P.-M.; Dompmartin, A.; Ezine, E.; Sassier, M.; Da-Silva, A.; Plane, A.-F.; Legallois, D.; L’Orphelin, J.-M.; et al. Cardiovascular Immunotoxicities Associated with Immune Checkpoint Inhibitors: A Safety Meta-Analysis. Eur. Heart J. 2021, 42, 4964–4977. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, M.A.; Sorbara, E.E.; Cicala, G.; Santoro, V.; Cutroneo, P.M.; Franchina, T.; Spina, E. Adverse Drug Reactions with HER2-Positive Breast Cancer Treatment: An Analysis from the Italian Pharmacovigilance Database. Drugs Real World Outcomes 2022, 9, 91–107. [Google Scholar] [CrossRef] [PubMed]
- Wittayanukorn, S.; Qian, J.; Johnson, B.S.; Hansen, R.A. Cardiotoxicity in Targeted Therapy for Breast Cancer: A Study of the FDA Adverse Event Reporting System (FAERS). J. Oncol. Pharm. Pract. 2017, 23, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Long, P.; Li, S.; Pan, L.; Wang, Y.; Chen, W.; Wang, X. Cardiovascular Adverse Events Associated with Antibody-Drug Conjugates (ADCs): A Pharmacovigilance Study Based on the FAERS Database. Front. Pharmacol. 2024, 15, 1378010. [Google Scholar] [CrossRef] [PubMed]
- Center for Drug Evaluation and Research. FDA Adverse Event Reporting System (FAERS); FDA: Silver Spring, MD, USA, 2021. [Google Scholar]
- Lee, L.; Gupta, M.; Sahasranaman, S. Immune Checkpoint Inhibitors: An Introduction to the next-Generation Cancer Immunotherapy. J. Clin. Pharmacol. 2016, 56, 157–169. [Google Scholar] [CrossRef] [PubMed]
- Darvin, P.; Toor, S.M.; Sasidharan Nair, V.; Elkord, E. Immune Checkpoint Inhibitors: Recent Progress and Potential Biomarkers. Exp. Mol. Med. 2018, 50, 1–11. [Google Scholar] [CrossRef]
- Abou Alaiwi, S.; Xie, W.; Nassar, A.H.; Dudani, S.; Martini, D.; Bakouny, Z.; Steinharter, J.A.; Nuzzo, P.V.; Flippot, R.; Martinez-Chanza, N.; et al. Safety and Efficacy of Restarting Immune Checkpoint Inhibitors after Clinically Significant Immune-Related Adverse Events in Metastatic Renal Cell Carcinoma. J. Immunother. Cancer 2020, 8, e000144. [Google Scholar] [CrossRef]
- Lee, D.J.; Lee, H.J.; Farmer, J.R.; Reynolds, K.L. Mechanisms Driving Immune-Related Adverse Events in Cancer Patients Treated with Immune Checkpoint Inhibitors. Curr. Cardiol. Rep. 2021, 23, 98. [Google Scholar] [CrossRef]
- De Velasco, G.; Je, Y.; Bossé, D.; Awad, M.M.; Ott, P.A.; Moreira, R.B.; Schutz, F.; Bellmunt, J.; Sonpavde, G.P.; Hodi, F.S.; et al. Comprehensive Meta-Analysis of Key Immune-Related Adverse Events from CTLA-4 and PD-1/PD-L1 Inhibitors in Cancer Patients. Cancer Immunol. Res. 2017, 5, 312–318. [Google Scholar] [CrossRef]
- Tachibana, M.; Imagawa, A. Type 1 Diabetes Related to Immune Checkpoint Inhibitors. Best. Pract. Res. Clin. Endocrinol. Metab. 2022, 36, 101657. [Google Scholar] [CrossRef]
- Barroso-Sousa, R.; Barry, W.T.; Garrido-Castro, A.C.; Hodi, F.S.; Min, L.; Krop, I.E.; Tolaney, S.M. Incidence of Endocrine Dysfunction Following the Use of Different Immune Checkpoint Inhibitor Regimens: A Systematic Review and Meta-Analysis. JAMA Oncol. 2018, 4, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Vandiver, J.W.; Singer, Z.; Harshberger, C. Severe Hyponatremia and Immune Nephritis Following an Initial Infusion of Nivolumab. Target. Oncol. 2016, 11, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Ganatra, S.; Neilan, T.G. Immune Checkpoint Inhibitor-Associated Myocarditis. Oncologist 2018, 23, 879–886. [Google Scholar] [CrossRef]
- Totzeck, M.; Lutgens, E.; Neilan, T.G. Are We Underestimating the Potential for Cardiotoxicity Related to Immune Checkpoint Inhibitors? Eur. Heart J. 2021, 42, 1632–1635. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in Patients Treated with Immune Checkpoint Inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. [Google Scholar] [CrossRef]
- Johnson, D.B.; Balko, J.M.; Compton, M.L.; Chalkias, S.; Gorham, J.; Xu, Y.; Hicks, M.; Puzanov, I.; Alexander, M.R.; Bloomer, T.L.; et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N. Engl. J. Med. 2016, 375, 1749–1755. [Google Scholar] [CrossRef]
- Tarrio, M.L.; Grabie, N.; Bu, D.; Sharpe, A.H.; Lichtman, A.H. PD-1 Protects against Inflammation and Myocyte Damage in T Cell-Mediated Myocarditis. J. Immunol. 2012, 188, 4876–4884. [Google Scholar] [CrossRef]
- Nishimura, H.; Okazaki, T.; Tanaka, Y.; Nakatani, K.; Hara, M.; Matsumori, A.; Sasayama, S.; Mizoguchi, A.; Hiai, H.; Minato, N.; et al. Autoimmune Dilated Cardiomyopathy in PD-1 Receptor-Deficient Mice. Science 2001, 291, 319–322. [Google Scholar] [CrossRef]
- Okazaki, T.; Tanaka, Y.; Nishio, R.; Mitsuiye, T.; Mizoguchi, A.; Wang, J.; Ishida, M.; Hiai, H.; Matsumori, A.; Minato, N.; et al. Autoantibodies against Cardiac Troponin I Are Responsible for Dilated Cardiomyopathy in PD-1-Deficient Mice. Nat. Med. 2003, 9, 1477–1483. [Google Scholar] [CrossRef]
- Axelrod, M.L.; Meijers, W.C.; Screever, E.M.; Qin, J.; Carroll, M.G.; Sun, X.; Tannous, E.; Zhang, Y.; Sugiura, A.; Taylor, B.C.; et al. T Cells Specific for α-Myosin Drive Immunotherapy-Related Myocarditis. Nature 2022, 611, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Tay, W.T.; Fang, Y.-H.; Beh, S.T.; Liu, Y.-W.; Hsu, L.-W.; Yen, C.-J.; Liu, P.-Y. Programmed Cell Death-1: Programmed Cell Death-Ligand 1 Interaction Protects Human Cardiomyocytes Against T-Cell Mediated Inflammation and Apoptosis Response In Vitro. Int. J. Mol. Sci. 2020, 21, 2399. [Google Scholar] [CrossRef] [PubMed]
- Pirozzi, F.; Poto, R.; Aran, L.; Cuomo, A.; Galdiero, M.R.; Spadaro, G.; Abete, P.; Bonaduce, D.; Marone, G.; Tocchetti, C.G.; et al. Cardiovascular Toxicity of Immune Checkpoint Inhibitors: Clinical Risk Factors. Curr. Oncol. Rep. 2021, 23, 13. [Google Scholar] [CrossRef]
- Rubio-Infante, N.; Ramírez-Flores, Y.A.; Castillo, E.C.; Lozano, O.; García-Rivas, G.; Torre-Amione, G. Cardiotoxicity Associated with Immune Checkpoint Inhibitor Therapy: A Meta-Analysis. Eur. J. Heart Fail. 2021, 23, 1739–1747. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Drobni, Z.D.; Zafar, A.; Gongora, C.A.; Zlotoff, D.A.; Alvi, R.M.; Taron, J.; Rambarat, P.K.; Schoenfeld, S.; Mosarla, R.C.; et al. Pre-Existing Autoimmune Disease Increases the Risk of Cardiovascular and Noncardiovascular Events After Immunotherapy. JACC CardioOncol. 2022, 4, 660–669. [Google Scholar] [CrossRef]
- Xie, W.; Huang, H.; Xiao, S.; Fan, Y.; Deng, X.; Zhang, Z. Immune Checkpoint Inhibitors Therapies in Patients with Cancer and Preexisting Autoimmune Diseases: A Meta-Analysis of Observational Studies. Autoimmun. Rev. 2020, 19, 102687. [Google Scholar] [CrossRef]
- Grabie, N.; Lichtman, A.H.; Padera, R. T Cell Checkpoint Regulators in the Heart. Cardiovasc. Res. 2019, 115, 869–877. [Google Scholar] [CrossRef]
- Knudsen, B.; Prasad, V. COVID-19 Vaccine Induced Myocarditis in Young Males: A Systematic Review. Eur. J. Clin. Investig. 2023, 53, e13947. [Google Scholar] [CrossRef]
- Oster, M.E.; Shay, D.K.; Su, J.R.; Gee, J.; Creech, C.B.; Broder, K.R.; Edwards, K.; Soslow, J.H.; Dendy, J.M.; Schlaudecker, E.; et al. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US from December 2020 to August 2021. JAMA 2022, 327, 331–340. [Google Scholar] [CrossRef]
- Patel, R.P.; Parikh, R.; Gunturu, K.S.; Tariq, R.Z.; Dani, S.S.; Ganatra, S.; Nohria, A. Cardiotoxicity of Immune Checkpoint Inhibitors. Curr. Oncol. Rep. 2021, 23, 79. [Google Scholar] [CrossRef]
- Moey, M.Y.Y.; Tomdio, A.N.; McCallen, J.D.; Vaughan, L.M.; O’Brien, K.; Naqash, A.R.; Cherry, C.; Walker, P.R.; Carabello, B.A. Characterization of Immune Checkpoint Inhibitor-Related Cardiotoxicity in Lung Cancer Patients from a Rural Setting. JACC CardioOncol. 2020, 2, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Ndjana Lessomo, F.Y.; Wang, Z.; Mukuka, C. Comparative Cardiotoxicity Risk of Pembrolizumab versus Nivolumab in Cancer Patients Undergoing Immune Checkpoint Inhibitor Therapy: A Meta-Analysis. Front. Oncol. 2023, 13, 1080998. [Google Scholar] [CrossRef] [PubMed]
- O’Gara, P.T.; Kushner, F.G.; Ascheim, D.D.; Casey, D.E.; Chung, M.K.; de Lemos, J.A.; Ettinger, S.M.; Fang, J.C.; Fesmire, F.M.; Franklin, B.A.; et al. 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 61, e78–e140. [Google Scholar] [CrossRef] [PubMed]
- Triggianese, P.; Novelli, L.; Galdiero, M.R.; Chimenti, M.S.; Conigliaro, P.; Perricone, R.; Perricone, C.; Gerli, R. Immune Checkpoint Inhibitors-Induced Autoimmunity: The Impact of Gender. Autoimmun. Rev. 2020, 19, 102590. [Google Scholar] [CrossRef] [PubMed]
- da Silva, J.S.; Montagnoli, T.L.; Rocha, B.S.; Tacco, M.L.C.A.; Marinho, S.C.P.; Zapata-Sudo, G. Estrogen Receptors: Therapeutic Perspectives for the Treatment of Cardiac Dysfunction after Myocardial Infarction. Int. J. Mol. Sci. 2021, 22, 525. [Google Scholar] [CrossRef]
- Ortona, E.; Pierdominici, M.; Rider, V. Editorial: Sex Hormones and Gender Differences in Immune Responses. Front. Immunol. 2019, 10, 1076. [Google Scholar] [CrossRef]
- Wang, F.; Wei, Q.; Wu, X. Cardiac Arrhythmias Associated with Immune Checkpoint Inhibitors: A Comprehensive Disproportionality Analysis of the FDA Adverse Event Reporting System. Front. Pharmacol. 2022, 13, 986357. [Google Scholar] [CrossRef]
- Escudier, M.; Cautela, J.; Malissen, N.; Ancedy, Y.; Orabona, M.; Pinto, J.; Monestier, S.; Grob, J.-J.; Scemama, U.; Jacquier, A.; et al. Clinical Features, Management, and Outcomes of Immune Checkpoint Inhibitor–Related Cardiotoxicity. Circulation 2017, 136, 2085–2087. [Google Scholar] [CrossRef]
- Fradley, M.G.; Brown, A.C.; Shields, B.; Viganego, F.; Damrongwatanasuk, R.; Patel, A.A.; Hartlage, G.; Roper, N.; Jaunese, J.; Roy, L.; et al. Developing a Comprehensive Cardio-Oncology Program at a Cancer Institute: The Moffitt Cancer Center Experience. Oncol. Rev. 2017, 11, 340. [Google Scholar] [CrossRef]
- Lyon, A.R.; Yousaf, N.; Battisti, N.M.L.; Moslehi, J.; Larkin, J. Immune Checkpoint Inhibitors and Cardiovascular Toxicity. Lancet Oncol. 2018, 19, e447–e458. [Google Scholar] [CrossRef]
- Puzanov, I.; Diab, A.; Abdallah, K.; Bingham, C.O.; Brogdon, C.; Dadu, R.; Hamad, L.; Kim, S.; Lacouture, M.E.; LeBoeuf, N.R.; et al. Managing Toxicities Associated with Immune Checkpoint Inhibitors: Consensus Recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J. Immunother. Cancer 2017, 5, 95. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on Cardio-Oncology Developed in Collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Bhatti, A.W.; Patel, R.; Dani, S.S.; Khadke, S.; Makwana, B.; Lessey, C.; Shah, J.; Al-Husami, Z.; Yang, E.H.; Thavendiranathan, P.; et al. SGLT2i and Primary Prevention of Cancer Therapy–Related Cardiac Dysfunction in Patients with Diabetes. JACC CardioOncol. 2024, in press. [Google Scholar] [CrossRef]
- Ha, A.; Langroudi, A.P.; Eisenberg, M.L. What Is the Validity of the Federal Adverse Event Reporting System in Contemporary Clinical Research? J. Sex. Med. 2024, 21, 744–745. [Google Scholar] [CrossRef]
- Center for Drug Evaluation and Research. Questions and Answers on FDA’s Adverse Event Reporting System (FAERS). Available online: https://www.fda.gov/drugs/surveillance/questions-and-answers-fdas-adverse-event-reporting-system-faers (accessed on 25 September 2024).
- Ye, X.; Hu, F.; Zhai, Y.; Qin, Y.; Xu, J.; Guo, X.; Zhuang, Y.; He, J. Hematological Toxicities in Immune Checkpoint Inhibitors: A Pharmacovigilance Study from 2014 to 2019. Hematol. Oncol. 2020, 38, 565–575. [Google Scholar] [CrossRef]
- van Puijenbroek, E.P.; Bate, A.; Leufkens, H.G.M.; Lindquist, M.; Orre, R.; Egberts, A.C.G. A Comparison of Measures of Disproportionality for Signal Detection in Spontaneous Reporting Systems for Adverse Drug Reactions. Pharmacoepidemiol. Drug Saf. 2002, 11, 3–10. [Google Scholar] [CrossRef]
- Evans, S.J.; Waller, P.C.; Davis, S. Use of Proportional Reporting Ratios (PRRs) for Signal Generation from Spontaneous Adverse Drug Reaction Reports. Pharmacoepidemiol. Drug Saf. 2001, 10, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Bate, A.; Lindquist, M.; Edwards, I.R.; Olsson, S.; Orre, R.; Lansner, A.; De Freitas, R.M. A Bayesian Neural Network Method for Adverse Drug Reaction Signal Generation. Eur. J. Clin. Pharmacol. 1998, 54, 315–321. [Google Scholar] [CrossRef]
- Szarfman, A.; Machado, S.G.; O’Neill, R.T. Use of Screening Algorithms and Computer Systems to Efficiently Signal Higher-than-Expected Combinations of Drugs and Events in the US FDA’s Spontaneous Reports Database. Drug Saf. 2002, 25, 381–392. [Google Scholar] [CrossRef]
- Sakaeda, T.; Tamon, A.; Kadoyama, K.; Okuno, Y. Data Mining of the Public Version of the FDA Adverse Event Reporting System. Int. J. Med. Sci. 2013, 10, 796–803. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| n (%) | Cardiac Failure | Atrial Fibrillation | Myocardial Infarction | Pericardial Disease | Myocarditis | QT Prolongation | |
|---|---|---|---|---|---|---|---|
| Sex | Female | 52 (32.70) | 39 (35.14) | 23 (23.96) | 80 (43.48) | 107 (38.77) | 0 (0.00) |
| Male | 101 (63.52) | 68 (61.26) | 69 (71.88) | 104 (56.52) | 158 (57.25) | 0 (0.00) | |
| N/A | 5 (3.14) | 4 (3.60) | 4 (4.17) | 0 (0.00) | 11 (3.99) | 0 (0.00) | |
| Age | 71.62 ± 9.69 (N/A 37) | 71.58 ± 8.05 (N/A 24) | 70.00 ± 10.55 (N/A 45) | 63.80 ± 13.22 (N/A 43) | 69.59 ± 11.55 (N/A 41) | 0.00 ± 0.00 | |
| Reaction | Serious | 158 | 111 | 96 | 184 | 276 | 0 |
| Non-serious | 0 | 0 | 0 | 0 | 0 | 0 | |
| Outcome | Died | 67 (42.14) | 27 (24.32) | 45 (46.88) | 32 (17.39) | 112 (40.58) | 0 (0.00) |
| Life-threatening | 16 (10.06) | 15 (13.51) | 9 (9.38) | 20 (10.87) | 57 (20.65) | 0 (0.00) | |
| Hospitalized | 45 (28.30) | 35 (31.53) | 27 (28.13) | 76 (41.30) | 68 (24.64) | 0 (0.00) | |
| Disabled | 0 (0.00) | 0 (0.00) | 0 (0.0) | 0 (0.0) | 1(0.36) | 0 (0.00) | |
| Other | 30 (18.87) | 34 (30.63) | 15 (15.63) | 56 (30.43) | 38 (13.77) | 0 (0.00) |
| ROR (95% CI) | IC (97.5% CI) | |
|---|---|---|
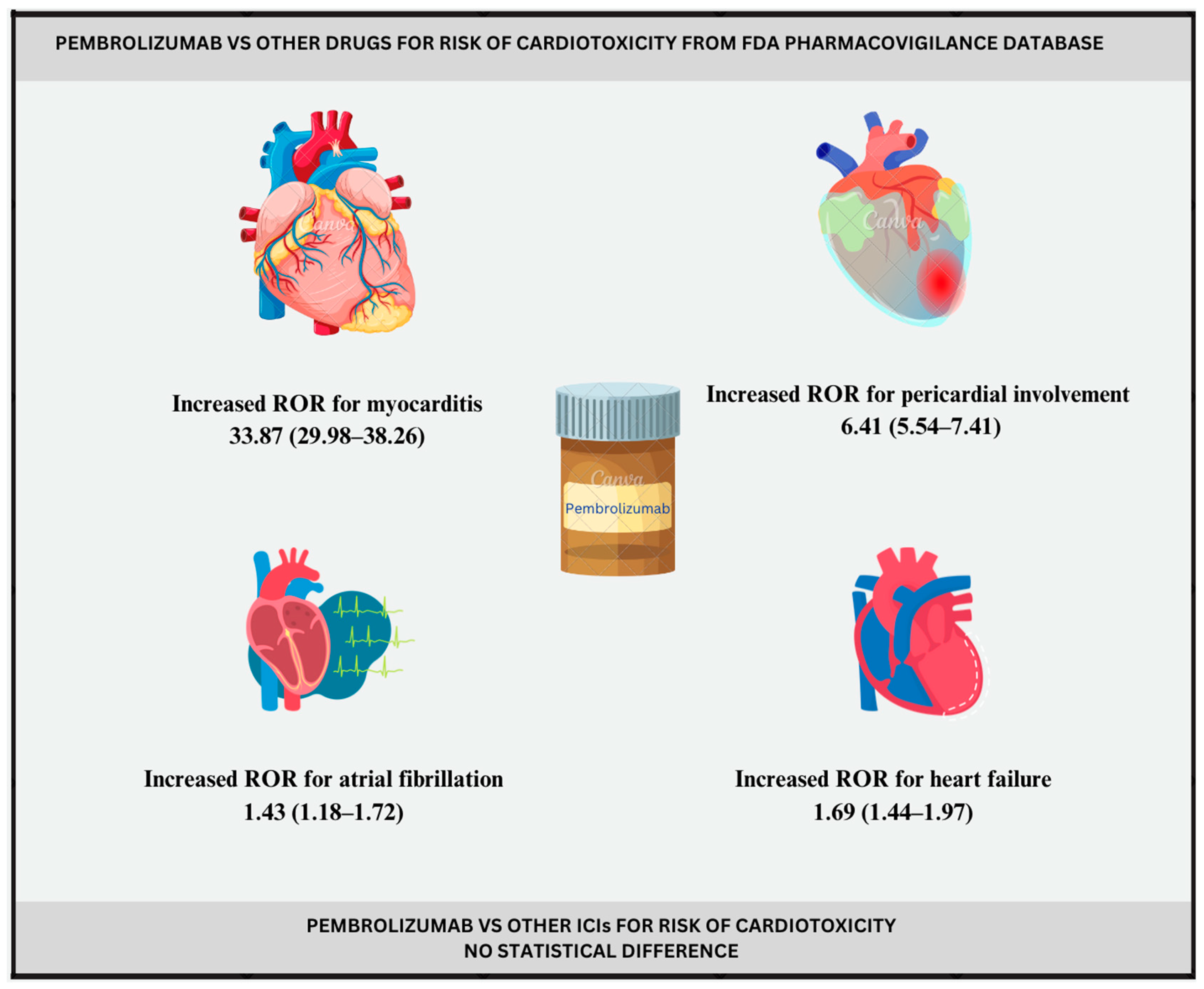
| Cardiac failure | 1.69 (1.44–1.97) | 0.75 (0.48–1.37) |
| Atrial fibrillation | 1.43 (1.18–1.72) | 0.51 (0.19–1.26) |
| Myocardial infarction | 1.22 (1.00–1.49) | 0.28 (−0.06–1.09) |
| Pericardial disease | 6.41 (5.54–7.41) | 2.64 (2.39–3.22) |
| Myocarditis | 33.87 (29.98–38.26) | 4.91 (4.71–5.39) |
| QT prolongation | / | / |
| Adverse Events | Pembrolizumab | Cemiplimab | Nivolumab | Atezolizumab | Avelumab | Durvalumab | Ipilimumab |
|---|---|---|---|---|---|---|---|
| Cardiac failure | 0.74 (0.63–0.87) | 2.05 (0.92–4.61) | 1.10 (0.97–1.26) | 0.65 (0.48–0.89) | 0.81 (0.42–1.56) | 0.74 (0.54–1.02) | 0.17 (0.07–0.40) |
| Atrial Fibrillation | 0.62 (0.51–0.75) | 0.44 (0.06–3.17) | 0.80 (0.68–0.95) | 0.86 (0.63–1.18) | 1.31 (0.72–2.38) | 0.52 (0.33–0.79) | 0.51 (0.28–0.92) |
| Myocardial infarction | 1.01 (0.81–1.26) | 1.52 (0.38–6.10) | 1.14 (0.94–1.38) | 1.18 (0.82–1.68) | 1.41 (0.67–2.97) | 1.40 (0.98–1.98) | 0.37 (0.15–0.89) |
| Pericardial disease | 1.13 (0.96–1.32) | 0.86 (0.21–3.44) | 1.14 (0.98–1.32) | 1.29 (1.00–1.66) | 0.45 (0.17–1.21) | 0.72 (0.50–1.04) | 0.17 (0.06–0.44) |
| Myocarditis | 1.01 (0.89–1.15) | 1.31 (0.54–3.16) | 0.85 (0.75–0.97) | 0.52 (0.38–0.70) | 0.97 (0.57–1.64) | 0.53 (0.38–0.74) | 0.53 (0.34–0.83) |
| QT prolongation | / | / | 0.31 (0.12–0.76) | / | / | / | 1.23 (0.3–5.02) |
| Adverse Events | Pembrolizumab | Cemiplimab | Nivolumab | Atezolizumab | Avelumab | Durvalumab | Ipilimumab |
|---|---|---|---|---|---|---|---|
| Cardiac failure | −0.37 (−0.63–0.26) | 0.91 (−0.50–3.99) | 0.12 (−0.08–0.59) | −0.59 (−1.11–0.66) | −0.29 (−1.43–2.26) | −0.41 (−0.94–0.83) | −2.45 (−4.01–0.89) |
| Atrial Fibrillation | −0.60 (−0.91–0.15) | −0.87 (−4.65–5.33) | −0.26 (−0.53–0.38) | −0.20 (−0.73–1.04) | 0.37 (−0.66–2.69) | −0.91 (−1.64–0.79) | −0.92 (−1.95–1.40) |
| Myocardial infarction | 0.02 (−0.32–0.82) | 0.46 (−2.14–5.34) | 0.15 (−0.14–0.84) | 0.22 (−0.37–1.60) | 0.45 (−0.85–3.32) | 0.45 (−0.13–1.82) | −1.33 (−2.89–2.01) |
| Pericardial disease | 0.14 (−0.10–0.72) | −0.18 (−2.77–4.70) | 0.15 (−0.07–0.67) | 0.34 (−0.08–1.34) | −1.05 (−2.81–2.64) | −0.45 (−1.06–0.98) | −2.42 (−4.18–1.26) |
| Myocarditis | 0.01 (−0.19–0.49) | 0.34 (−1.22–3.68) | −0.19 (−0.38–0.27) | −0.91 (−1.42–0.29) | −0.04 (−0.95–2.03) | −0.87 (−1.42–0.42) | −0.87 (−1.62–0.87) |
| QT prolongation | −4.77 (−15.10–5.01) | −0.46 (−10.79–9.32) | −1.42 (−2.99–1.92) | −3.15 (−13.47–6.64) | −1.27 (−11.60–8.51) | −2.96 (−13.28–6.83) | 0.23 (−2.36–5.12) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milutinovic, S.; Jancic, P.; Jokic, V.; Petrovic, M.; Dumic, I.; Rodriguez, A.M.; Tanasijevic, N.; Begosh-Mayne, D.; Stanojevic, D.; Escarcega, R.O.; et al. Pembrolizumab-Associated Cardiotoxicity: A Retrospective Analysis of the FDA Adverse Events Reporting System. Pharmaceuticals 2024, 17, 1372. https://doi.org/10.3390/ph17101372
Milutinovic S, Jancic P, Jokic V, Petrovic M, Dumic I, Rodriguez AM, Tanasijevic N, Begosh-Mayne D, Stanojevic D, Escarcega RO, et al. Pembrolizumab-Associated Cardiotoxicity: A Retrospective Analysis of the FDA Adverse Events Reporting System. Pharmaceuticals. 2024; 17(10):1372. https://doi.org/10.3390/ph17101372
Chicago/Turabian StyleMilutinovic, Stefan, Predrag Jancic, Vera Jokic, Marija Petrovic, Igor Dumic, Ambar Morales Rodriguez, Nikola Tanasijevic, Dustin Begosh-Mayne, Dragana Stanojevic, Ricardo O. Escarcega, and et al. 2024. "Pembrolizumab-Associated Cardiotoxicity: A Retrospective Analysis of the FDA Adverse Events Reporting System" Pharmaceuticals 17, no. 10: 1372. https://doi.org/10.3390/ph17101372
APA StyleMilutinovic, S., Jancic, P., Jokic, V., Petrovic, M., Dumic, I., Rodriguez, A. M., Tanasijevic, N., Begosh-Mayne, D., Stanojevic, D., Escarcega, R. O., Lopez-Mattei, J., & Cao, X. (2024). Pembrolizumab-Associated Cardiotoxicity: A Retrospective Analysis of the FDA Adverse Events Reporting System. Pharmaceuticals, 17(10), 1372. https://doi.org/10.3390/ph17101372