
Medication Dosage Impact on Mortality in Old-Age Individuals with Schizophrenia: A National Cohort Study

Abstract
1. Introduction
2. Results
3. Discussions
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. World Social Report 2023: Leaving No One behind in an Ageing World; United Nations: New York, NY, USA, 2023. [Google Scholar]
- Tampi, R.R.; Young, J.; Hoq, R.; Resnick, K.; Tampi, D.J. Psychotic disorders in late life: A narrative review. Ther. Adv. Psychopharmacol. 2019, 9, 2045125319882798. [Google Scholar] [CrossRef] [PubMed]
- Van Assche, L.; Morrens, M.; Luyten, P.; Van de Ven, L.; Vandenbulcke, M. The neuropsychology and neurobiology of late-onset schizophrenia and very-late-onset schizophrenia-like psychosis: A critical review. Neurosci. Biobehav. Rev. 2017, 83, 604–621. [Google Scholar] [CrossRef] [PubMed]
- Karim, S.; Overshott, R.; Burns, A. Older people with chronic schizophrenia. Aging Ment. Health 2005, 9, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Jagsch, C.; Hofer, A. Diseases of the schizophrenia spectrum disorder in old age: Diagnostic and therapeutic challenges. Z. Gerontol. Geriatr. 2018, 51, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Bačar Bole, C.; Nagode, K.; Pišlar, M.; Mrhar, A.; Grabnar, I.; Vovk, T. Potential Drug-Drug Interactions among Patients with Schizophrenia Spectrum Disorders: Prevalence, Association with Risk Factors, and Replicate Analysis in 2021. Medicina 2023, 59, 284. [Google Scholar] [CrossRef] [PubMed]
- Van Assche, L.; Van Aubel, E.; Van de Ven, L.; Bouckaert, F.; Luyten, P.; Vandenbulcke, M. The Neuropsychological Profile and Phenomenology of Late Onset Psychosis: A Cross-sectional Study on the Differential Diagnosis of Very-Late-Onset Schizophrenia-Like Psychosis, Dementia with Lewy Bodies and Alzheimer’s Type Dementia with Psychosis. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 2019, 34, 183–199. [Google Scholar] [CrossRef] [PubMed]
- Bertol, E.; Vaiano, F.; Argo, A.; Zerbo, S.; Trignano, C.; Protani, S.; Favretto, D. Overdose of Quetiapine—A Case Report with QT Prolongation. Toxics 2021, 9, 339. [Google Scholar] [CrossRef]
- Folsom, D.P.; Lebowitz, B.D.; Lindamer, L.A.; Palmer, B.W.; Patterson, T.L.; Jeste, D.V. Schizophrenia in late life: Emerging issues. Dialogues Clin. Neurosci. 2006, 8, 45–52. [Google Scholar] [CrossRef]
- Vermeulen, J.; van Rooijen, G.; Doedens, P.; Numminen, E.; van Tricht, M.; de Haan, L. Antipsychotic medication and long-term mortality risk in patients with schizophrenia; a systematic review and meta-analysis. Psychol. Med. 2017, 47, 2217–2228. [Google Scholar] [CrossRef]
- Ray, W.A.; Fuchs, D.C.; Olfson, M.; Patrick, S.W.; Stein, C.M.; Murray, K.T.; Daugherty, J.; Cooper, W.O. Antipsychotic Medications and Mortality in Children and Young Adults. JAMA Psychiatry, 2023; online ahead of print. [Google Scholar] [CrossRef]
- Tiihonen, J.; Mittendorfer-Rutz, E.; Torniainen, M.; Alexanderson, K.; Tanskanen, A. Mortality and Cumulative Exposure to Antipsychotics, Antidepressants, and Benzodiazepines in Patients with Schizophrenia: An Observational Follow-Up Study. Am. J. Psychiatry 2016, 173, 600–606. [Google Scholar] [CrossRef]
- Lin, J.-Y.; Yeh, L.-L.; Pan, Y.-J. Exposure to psychotropic medications and mortality in schizophrenia: A 5-year national cohort study. Psychol. Med. 2023, 53, 5528–5537. [Google Scholar] [CrossRef] [PubMed]
- Gareri, P.; Segura-García, C.; Manfredi, V.G.; Bruni, A.; Ciambrone, P.; Cerminara, G.; De Sarro, G.; De Fazio, P. Use of atypical antipsychotics in the elderly: A clinical review. Clin. Interv. Aging 2014, 9, 1363–1373. [Google Scholar] [CrossRef] [PubMed]
- Talaslahti, T.; Alanen, H.M.; Hakko, H.; Isohanni, M.; Häkkinen, U.; Leinonen, E. Patients with very-late-onset schizoprhenia-like psychosis have higher mortality rates than elderly patients with earlier onset schizophrenia. Int. J. Geriatr. Psychiatry 2015, 30, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Torniainen, M.; Mittendorfer-Rutz, E.; Tanskanen, A.; Björkenstam, C.; Suvisaari, J.; Alexanderson, K.; Tiihonen, J. Antipsychotic treatment and mortality in schizophrenia. Schizophr. Bull. 2015, 41, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Nam, H.; Park, S.; Chae, J.H.; Kim, T.S. Decreased cardiovascular death in schizophrenia patients treated with antipsychotics: A Korean national cohort study. Schizophr. Res. 2021, 228, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, D.; Gissler, M.; Hällgren, J.; Ösby, U.; Westman, J.; Bobo, W.V. The overall and sex- and age-group specific incidence rates of cancer in people with schizophrenia: A population-based cohort study. Epidemiol. Psychiatr. Sci. 2020, 29, e132. [Google Scholar] [CrossRef] [PubMed]
- Ying, J.; Chew, Q.H.; Wang, Y.; Sim, K. Global Neuropsychopharmacological Prescription Trends in Adults with Schizophrenia, Clinical Correlates and Implications for Practice: A Scoping Review. Brain Sci. 2024, 14, 6. [Google Scholar] [CrossRef]
- Correll, C.U.; Rubio, J.M.; Inczedy-Farkas, G.; Birnbaum, M.L.; Kane, J.M.; Leucht, S. Efficacy of 42 Pharmacologic Cotreatment Strategies Added to Antipsychotic Monotherapy in Schizophrenia: Systematic Overview and Quality Appraisal of the Meta-analytic Evidence. JAMA Psychiatry 2017, 74, 675–684. [Google Scholar] [CrossRef]
- Möller, H.J. Management of the negative symptoms of schizophrenia: New treatment options. CNS Drugs 2003, 17, 793–823. [Google Scholar] [CrossRef]
- Li, Q.; Su, Y.A.; Xiang, Y.T.; Shu, L.; Yu, X.; Ungvari, G.S.; Ng, C.H.; Chiu, H.F.; Ning, Y.P.; Wang, G.H.; et al. Adjunctive antidepressant use in schizophrenia in China: A national survey (2002–2012). Hum. Psychopharmacol. 2017, 32, e2571. [Google Scholar] [CrossRef]
- Baandrup, L. Polypharmacy in schizophrenia. Basic Clin. Pharmacol. Toxicol. 2020, 126, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Coupland, C.; Dhiman, P.; Morriss, R.; Arthur, A.; Barton, G.; Hippisley-Cox, J. Antidepressant use and risk of adverse outcomes in older people: Population based cohort study. BMJ 2011, 343, d4551. [Google Scholar] [CrossRef] [PubMed]
- Pizzi, C.; Mancini, S.; Angeloni, L.; Fontana, F.; Manzoli, L.; Costa, G.M. Effects of selective serotonin reuptake inhibitor therapy on endothelial function and inflammatory markers in patients with coronary heart disease. Clin. Pharmacol. Ther. 2009, 86, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Detraux, J.; De Lepeleire, J.; De Hert, M. Effects of antipsychotics, antidepressants and mood stabilizers on risk for physical diseases in people with schizophrenia, depression and bipolar disorder. World Psychiatry Off. J. World Psychiatr. Assoc. (WPA) 2015, 14, 119–136. [Google Scholar] [CrossRef] [PubMed]
- Nezafati, M.H.; Vojdanparast, M.; Nezafati, P. Antidepressants and cardiovascular adverse events: A narrative review. ARYA Atheroscler. 2015, 11, 295–304. [Google Scholar] [PubMed]
- Yekehtaz, H.; Farokhnia, M.; Akhondzadeh, S. Cardiovascular considerations in antidepressant therapy: An evidence-based review. J. Tehran Heart Cent. 2013, 8, 169–176. [Google Scholar] [PubMed]
- Mazereel, V.; Detraux, J.; Vancampfort, D.; van Winkel, R.; De Hert, M. Impact of Psychotropic Medication Effects on Obesity and the Metabolic Syndrome in People with Serious Mental Illness. Front. Endocrinol. 2020, 11, 573479. [Google Scholar] [CrossRef]
- Zelena, D.; Filaretova, L.; Mergl, Z.; Barna, I.; Tóth, Z.E.; Makara, G.B. Hypothalamic paraventricular nucleus, but not vasopressin, participates in chronic hyperactivity of the HPA axis in diabetic rats. Am. J. Physiol. Endocrinol. Metab. 2006, 290, E243–E250. [Google Scholar] [CrossRef]
- Wolkowitz, O.M.; Pickar, D. Benzodiazepines in the treatment of schizophrenia: A review and reappraisal. Am. J. Psychiatry 1991, 148, 714–726. [Google Scholar] [CrossRef]
- Dold, M.; Li, C.; Tardy, M.; Khorsand, V.; Gillies, D.; Leucht, S. Benzodiazepines for schizophrenia. Cochrane Database Syst. Rev. 2012, 11, CD006391. [Google Scholar] [CrossRef]
- Miron, A.A.; Petric, P.S.; Teodorescu, A.; Ifteni, P.; Chele, G.; Szalontay, A.S. Benzodiazepines and Mood Stabilizers in Schizophrenia Patients Treated with Oral versus Long-Acting Injectable Antipsychotics—An Observational Study. Brain Sci. 2023, 13, 173. [Google Scholar] [PubMed]
- Xiang, Y.T.; Dickerson, F.; Kreyenbuhl, J.; Ungvari, G.S.; Wang, C.Y.; Si, T.M.; Lee, E.H.; He, Y.L.; Chiu, H.F.; Yang, S.Y.; et al. Adjunctive mood stabilizer and benzodiazepine use in older Asian patients with schizophrenia, 2001–2009. Pharmacopsychiatry 2012, 45, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.S.; Lin, Y.J.; Liu, S.K. Benzodiazepine use among patients with schizophrenia in Taiwan: A nationwide population-based survey. Psychiatr. Serv. 2011, 62, 908–914. [Google Scholar] [CrossRef] [PubMed]
- Izza, M.A.D.; Lunt, E.; Gordon, A.L.; Gladman, J.R.F.; Armstrong, S.; Logan, P. Polypharmacy, benzodiazepines, and antidepressants, but not antipsychotics, are associated with increased falls risk in UK care home residents: A prospective multi-centre study. Eur. Geriatr. Med. 2020, 11, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Richardson, K.; Bennett, K.; Kenny, R.A. Polypharmacy including falls risk-increasing medications and subsequent falls in community-dwelling middle-aged and older adults. Age Ageing 2015, 44, 90–96. [Google Scholar] [CrossRef]
- Chen, P.L.; Lee, W.J.; Sun, W.Z.; Oyang, Y.J.; Fuh, J.L. Risk of dementia in patients with insomnia and long-term use of hypnotics: A population-based retrospective cohort study. PLoS ONE 2012, 7, e49113. [Google Scholar] [CrossRef]
- Tenback, D.; Pijl, B.; Smeets, H.; Os, J.; Harten, P. All-cause mortality and medication risk factors in schizophrenia: A prospective cohort study. J. Clin. Psychopharmacol. 2012, 32, 31–35. [Google Scholar] [CrossRef]
- National Health Insurance Administration. National Health Insurance Annual Statistical Report 2018; National Health Insurance Administration, Ministry of Health and Welfare: Taipei City, Taiwan, 2019; ISSN 1680-5496.
- National Health Insurance Administration. Introduction of the System of the Tenth Edition of the International Classification of Diseases for National Health Insurance (ICD-10-CM/PCS); Ministry of Health and Welfare: Taipei City, Taiwan, 2016.
- WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC Classification and DDD Assignment 2013, 16th ed.; WHO Collaborating Centre for Drug Statistics Methodology: Oslo, Norway, 2012. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
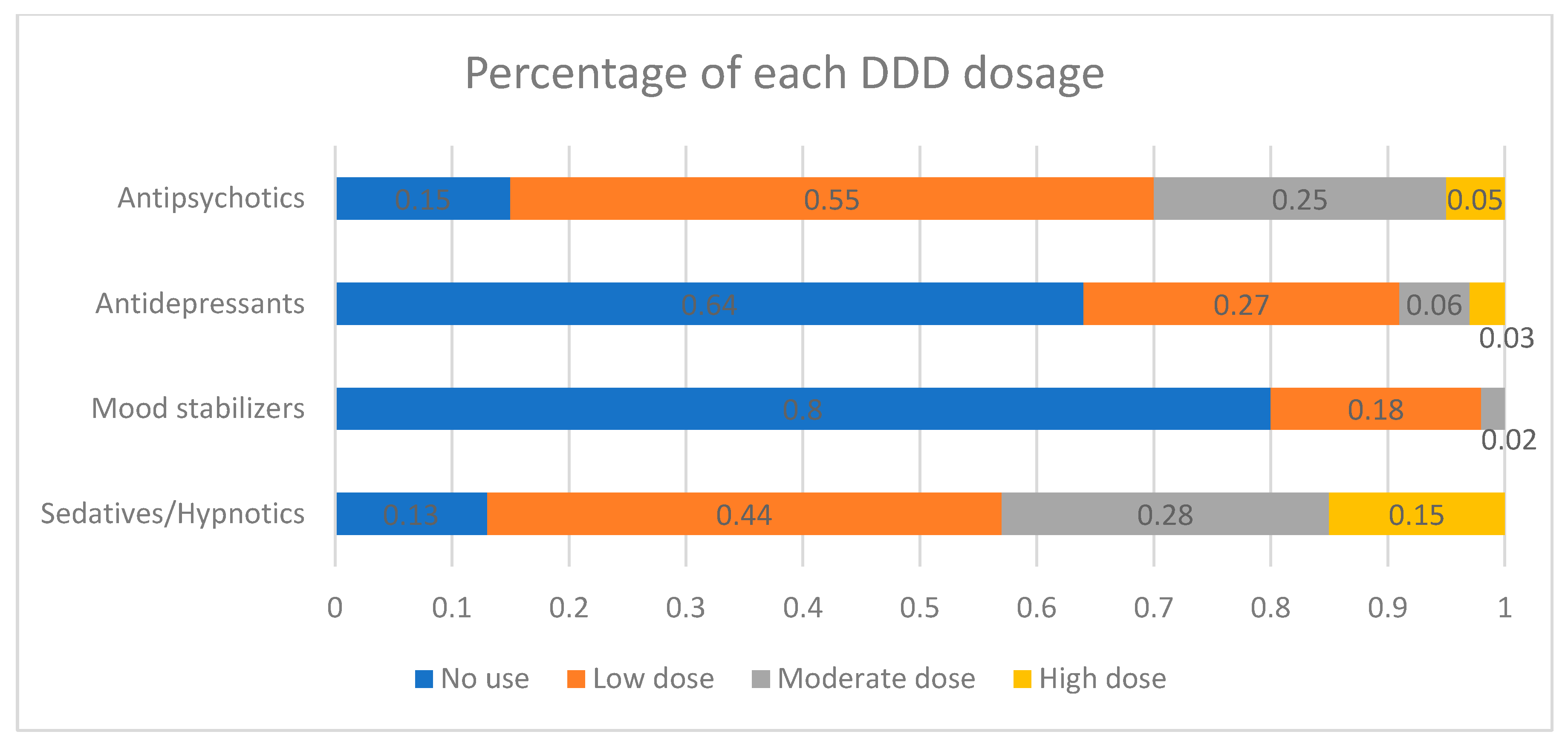
| Total (n = 6433) | No Antipsychotic Exposure (n = 944, 14.7%) | Low Antipsychotic Exposure (n = 3520, 54.7%) | Moderate Antipsychotic Exposure (n = 1636, 25.4%) | High Antipsychotic Exposure (n = 333, 5.2%) | Significance | |
|---|---|---|---|---|---|---|
| Age (years old) [mean (SD)] | 73.23 (6.6) | 74.6 (7.0) | 74.6 (7.0) | 71.5 (5.4) | 70.0 (4.2) | F = 126.75 |
| Gender [n (%)] | χ² = 10.049 * | |||||
| Female | 3843 (59.9) | 531 (56.3) | 2117 (60.1) | 976 (59.7) | 219 (65.7) | |
| Male | 2590 (40.1) | 413 (43.7) | 1403 (39.9) | 660 (40.3) | 114 (34.3) | |
| Lower-income household [n (%)] | 948 (14.7) | 141 (14.9) | 473 (13.4) | 288 (17.6) | 46 (13.8) | χ² = 15.688 |
| With catastrophic illness card a [n (%)] | 4049 (62.9) | 559 (59.2) | 2012 (57.2) | 1217 (74.4) | 261 (78.4) | χ² = 182.005 |
| Psychiatric healthcare cost [mean (SD)] | 45,228 (88,433) | 11,856 (38,399) | 32,440 (70,199) | 79,285 (112,981) | 107,770 (133,018) | F = 227.33 * |
| Non-psychiatric healthcare cost b [mean (SD)] | 79,421 (161,005) | 100,910 (208,438) | 87,048 (169,539) | 53,863 (99,821) | 63,449 (140,242) | F = 23.31 * |
| Psychiatric ward admission c in the 1st year [n (%)] | 853 (13.3) | 35 (3.7) | 387 (11.0) | 345 (21.1) | 86 (25.8) | χ² = 223.482 |
| Death [n (%)] | ||||||
| All causes | 2053 (31.9) | 379 (40.1) | 1179 (33.5) | 396 (24.2) | 99 (29.7) | χ² = 78.974 |
| Natural causes | 1992 (31.0) | 368 (39.0) | 1154 (32.8) | 377 (23.0) | 93 (27.9) | χ² = 687.98 * |
| Cancer | 258 (4.0) | 51 (5.4) | 139 (3.9) | 53 (3.2) | 15 (4.5) | |
| CVD | 384 (6.0) | 73 (7.7) | 227 (6.4) | 64 (3.9) | 20 (6.0) | |
| DM | 111 (1.7) | 12 (1.3) | 72 (2.0) | 23 (1.4) | 4 (1.2) | |
| Unnatural causes | 61 (0.9) | 11 (1.2) | 25 (0.7) | 19 (1.2) | 6 (1.8) | χ² = 45.19 * |
| Suicide | 15 (0.2) | 1 (0.1) | 9 (0.3) | 4 (0.2) | 1 (0.3) | |
| Unknown | 13 (0.2) | 3 (0.3) | 3 (0.1) | 7 (0.4) | 0 (0.0) | |
| Follow-up days [mean (SD)] | 1585.69 (456.0) | 1350.44 (635.2) | 1508.32 (500.5) | 1580.90 (465.3) | 1524.81 (515.6) | F = 40.42 |
| Low Exposure | Moderate Exposure | High Exposure | ||||
|---|---|---|---|---|---|---|
| Adjusted Hazard Ratio | 95% CI | Adjusted Hazard Ratio | 95% CI | Adjusted Hazard Ratio | 95% CI | |
| Overall mortality | ||||||
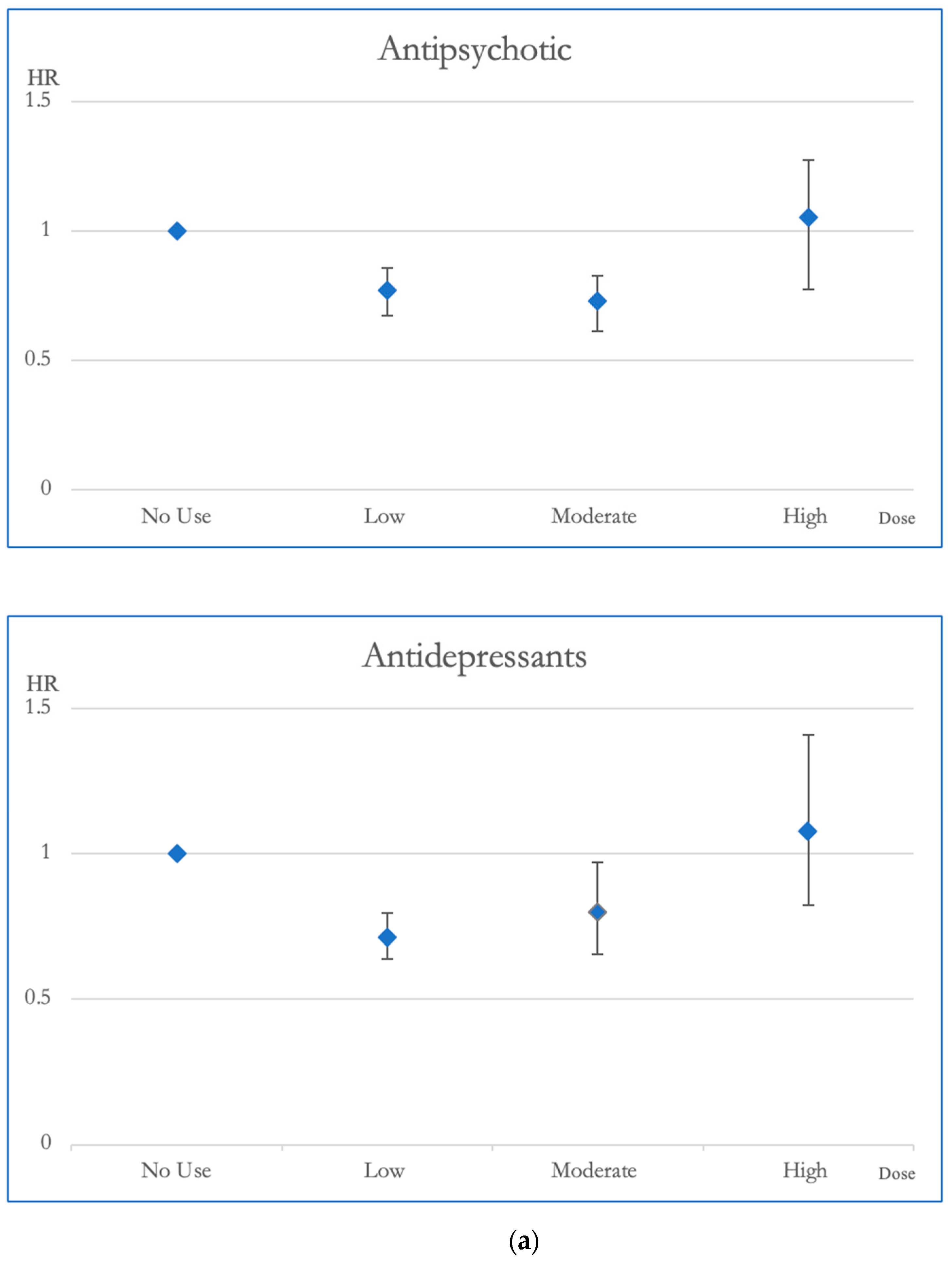
| Antipsychotics | 0.773 ** | 0.687–0.896 | 0.729 ** | 0.629–0.846 | 1.054 | 0.834–1.333 |
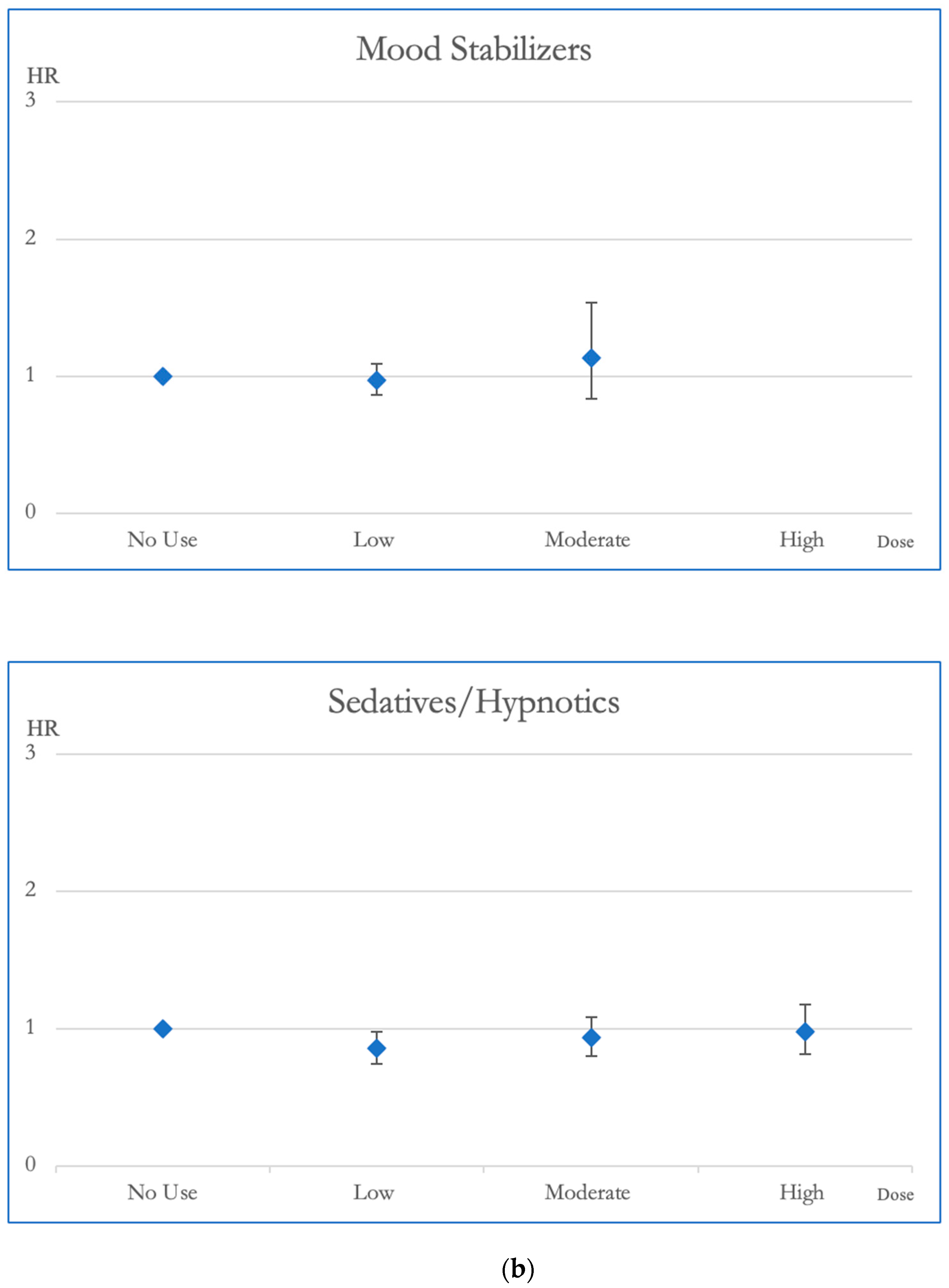
| Mood stabilizers | 0.973 | 0.866–1.093 | 1.134 | 0.835–1.539 | ||
| Antidepressants | 0.714 ** | 0.640–0.797 | 0.797 * | 0.656–0.970 | 1.077 | 0.823–1.410 |
| Sedative-Hypnotics | 0.855 * | 0.745–0.982 | 0.934 | 0.803–1.086 | 0.979 | 0.816–1.175 |
| Cardiovascular mortality | ||||||
| Antipsychotics | 0.788 | 0.603–1.031 | 0.617 ** | 0.434–0.878 | 1.102 | 0.651–1.867 |
| Mood stabilizers | 1.103 | 0.845–1.440 | 1.342 | 0.681–2.647 | ||
| Antidepressants | 0.589 ** | 0.453–0.766 | 0.632 | 0.396–1.011 | 0.454 | 0.198–1.043 |
| Sedative-Hypnotics | 0.658 * | 0.489–0.886 | 0.763 | 0.548–1.063 | 1.062 | 0.719–1.567 |
| Cancer mortality | ||||||
| Antipsychotics | 0.688 * | 0.497–0.954 | 0.660 * | 0.440–0.989 | 1.076 | 0.585–1.982 |
| Mood stabilizers | 0.877 | 0.626–1.230 | 0.901 | 0.366–2.221 | ||
| Antidepressants | 0.827 | 0.607–1.126 | 1.170 | 0.700–1.956 | 2.194 * | 1.174–4.100 |
| Sedative-Hypnotics | 0.762 | 0.526–1.104 | 0.755 | 0.502–1.135 | 0.507 * | 0.297–0.864 |
| DM mortality | ||||||
| Antipsychotics | 1.435 | 0.776–2.655 | 0.959 | 0.466–1.973 | 0.783 | 0.243–2.528 |
| Mood stabilizers | 0.882 | 0.531–1.464 | 0.804 | 0.194–3.336 | ||
| Antidepressants | 0.599 * | 0.378–0.949 | 0.356 * | 0.127–0.994 | 0.363 | 0.086–1.535 |
| Sedative-Hypnotics | 1.408 | 0.683–2.900 | 1.842 | 0.869–3.905 | 2.866 * | 1.265–6.492 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.-R.; Yeh, L.-L.; Lin, J.-Y.; Pan, Y.-J. Medication Dosage Impact on Mortality in Old-Age Individuals with Schizophrenia: A National Cohort Study. Pharmaceuticals 2024, 17, 78. https://doi.org/10.3390/ph17010078
Li J-R, Yeh L-L, Lin J-Y, Pan Y-J. Medication Dosage Impact on Mortality in Old-Age Individuals with Schizophrenia: A National Cohort Study. Pharmaceuticals. 2024; 17(1):78. https://doi.org/10.3390/ph17010078
Chicago/Turabian StyleLi, Jia-Ru, Ling-Ling Yeh, Ji-Yu Lin, and Yi-Ju Pan. 2024. "Medication Dosage Impact on Mortality in Old-Age Individuals with Schizophrenia: A National Cohort Study" Pharmaceuticals 17, no. 1: 78. https://doi.org/10.3390/ph17010078
APA StyleLi, J.-R., Yeh, L.-L., Lin, J.-Y., & Pan, Y.-J. (2024). Medication Dosage Impact on Mortality in Old-Age Individuals with Schizophrenia: A National Cohort Study. Pharmaceuticals, 17(1), 78. https://doi.org/10.3390/ph17010078