


Vitamin D and Osteogenesis Imperfecta in Pediatrics
 , , , and
, , , and
Abstract
1. Introduction
2. Results
2.1. Vitamin D and BMD

{kind=link}
| Studies | Type | Patients n; M%; -F%; Age Range (years) | 25(OH)D Basal Level nmol/L (±SD) | Bone Mineral Density: LS-aBMD (±z-Score) | Results |
|---|---|---|---|---|---|
| Edouard et al. 2011 [21] | Retrospective Cross-sectional Study | n: 315; (M: 51% -F: 49%) 1–18 years | 64 (±23) | −3.9 (± 1.6) | Serum 25OH D levels are positively associated with LS-aBMD z-scores |
| Edouard et al. 2011 [22] | Retrospective study | n: 71 (M: 51%; F 49%) 3–13 years | 50 (±18) | −4.6 (±1.3) | No evidence that serum 25(OH)D level was associated with measures of bone mineralization, metabolism or mass in children with OI |
| Edouard et al. 2012 [23] | Retrospective study | n: 132 (M:52%; F: 48%) 1–18 years | 60 (±23) | −4.9 (±1.2) | OI patients with the most severe skeletal phenotype have higher serum 24,25(OH)2D levels and higher serum 24,25(OH)2D to 25OHD ratios, independently of bone mass or bone metabolism |
| Chagas et al. 2012 [24] | Cross-sectional Study | n: 26 (M: NR%; F: NR%) 13–39 years | 65 (±22) | −2.7 (±0.8) | 69% and 77% of patients with type I OI and patients with type III OI, presented insufficient vitamin D serum concentrations, whereas 8% of patients with type III OI were considered vitamin D deficient |
| Wilsford et al. 2013 [19] | Retrospective study | n: 44 (M: 41%; F: 59%) 0–18 years | 57 (±27) | Not reported | Almost 80% of children with OI have insufficient or deficient levels of 25OHD |
| Zambrano et al. 2016 [20] | Cross-sectional study | n: 52 (M: 44%; F: 56%) 0–19 years | 54.2 (±11.0) | −1.3 (±0.5) | 88.4% of individuals had insufficient or deficient serum 25-OHD levels. Positive association between the BMD z-score of the lumbar spine and serum 25-OHD levels, even after adjusting for sex, age, and OI type |
| Plante et al. 2016 [26] | double-blind randomized controlled trial | n: 60 (M: 50%; F: 50%) 6–19 years | 65.5 (±20.5) | −2 (±1.1) | One-year of RCT children with OI showed that supplementation of either 400 IU or 2000 IU of vitamin D translated into significant increases in serum 25OHD concentrations. However, increases in serum 25OHD concentrations did not have a detectable effect on LS-aBMD z-scores |
| Bian et al. 2018 [25] | Retrospective | n: 90 (M 50%; F 50%) 4–14 years | 82.6 (±29.2) | −0.9 (±1.4) | About 40% of patients with OI have vitamin D insufficiency |
| Maines et al. 2020 [27] | Prospective | n: 37 (M 54%; F% 46%) 2–20 years | 85 (±25) | Not Reported | Low vitamin D levels are to be considered a significant risk factor for post-infusion hypocalcemia after neridronate treatment |
| Diacinti et al. 2021 [10] | Prospective | n: 60 (M: 58%; F: 42%) 1–16 years | 77.3 (±40) | −2.46 (±1.25) | VFA as a safe and alternative methodology in the follow-up of children and adolescents with OI |
| Mohsenzade et al. 2021 [17] | Case control study | n: 23 (M: 39%; F: 61%) 8 ± 4 years | 65 (± 34) | 0.47 ± 0.10 | Vitamin D deficiency is prevalent amongst OI children in southern Iran |
2.2. Vitamin D and Calcemia
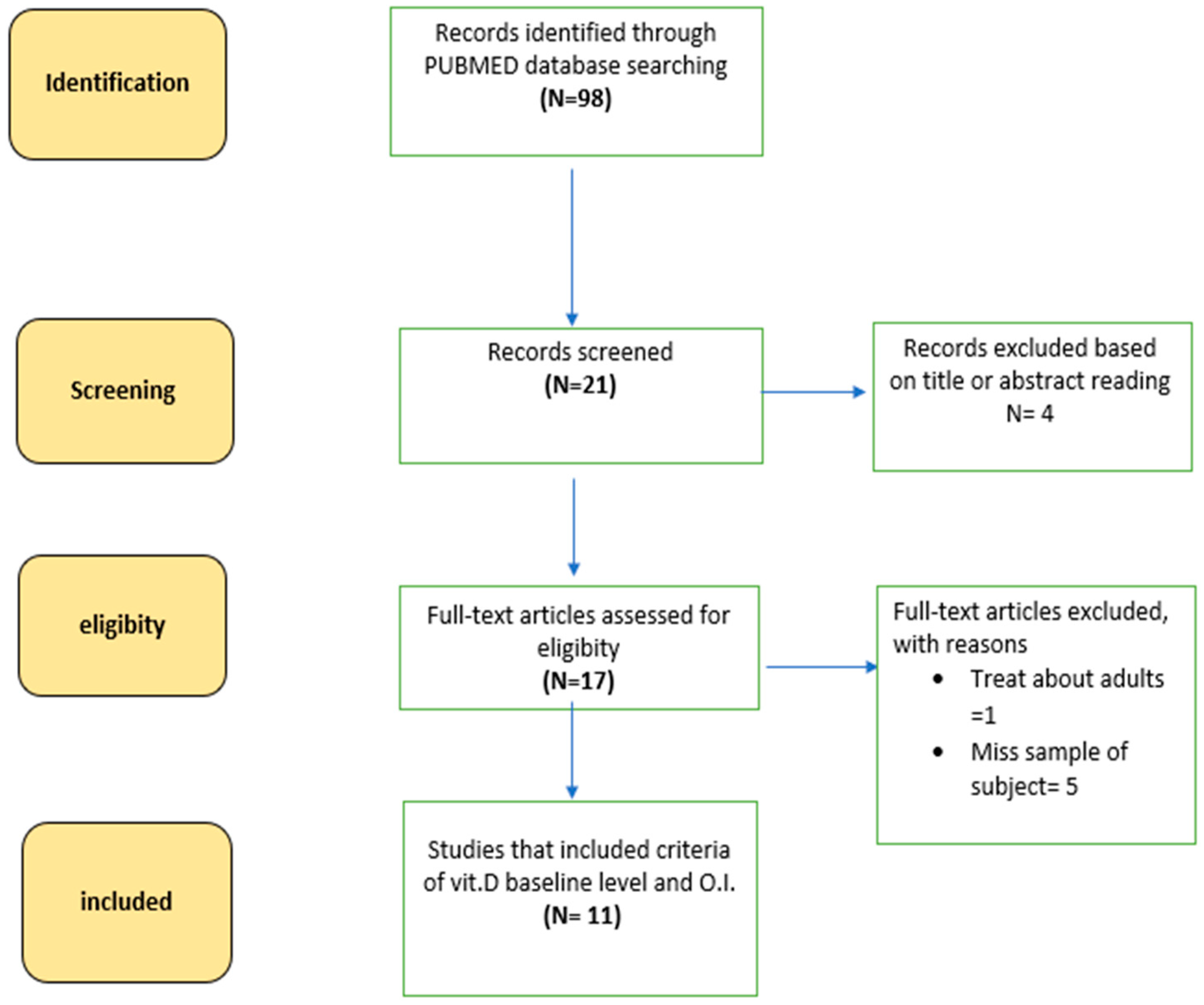
3. Materials and Methods
- -
- Study in OI patients in pediatric age,
- -
- Dosing of 25 OH Vitamin D levels,
- -
- Assessment of bone mineral density levels or bone metabolism markers.
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| OI | Osteogenesis imperfecta |
| BP | bisphosphonate |
| ALP | alkaline phosphatase |
| CTX | terminal c telopeptide |
| PTH | parathyroid hormone |
| 25OHD | 25OH vitamin D |
| RCT | randomized controlled trials |
References
- Marini, J.C.; Forlino, A.; Bächinger, H.P.; Bishop, N.J.; Byers, P.H.; Paepe, A.; Fassier, F.; Fratzl-Zelman, N.; Kozloff, K.M.; Krakow, D.; et al. Osteogenesis imperfecta. Nat. Rev. Dis. Primers 2017, 3, 17052. [Google Scholar] [CrossRef] [PubMed]
- Marom, R.; Rabenhorst, B.M.; Morello, R. Osteogenesis imperfecta: An update on clinical features and therapies. Eur. J. Endocrinol. 2020, 183, R95–R106. [Google Scholar] [CrossRef] [PubMed]
- Garibaldi, N.; Besio, R.; Dalgleish, R.; Villani, S.; Barnes, A.M.; Marini, J.C.; Forlino, A. Dissecting the phenotypic variability of osteogenesis imperfecta. Dis. Model. Mech. 2022, 15, dmm049398. [Google Scholar] [CrossRef]
- Monti, E.; Mottes, M.; Fraschini, P.; Brunelli, P.; Forlino, A.; Venturi, G.; Doro, F.; Perlini, S.; Cavarzere, P.; Antoniazzi, F. Current and emerging treatments for the management of osteogenesis imperfecta. Ther. Clin. Risk Manag. 2010, 6, 367–381. [Google Scholar] [CrossRef]
- Bishop, N. Bone Material Properties in Osteogenesis Imperfecta. J. Bone Miner. Res. 2016, 31, 699–708. [Google Scholar] [CrossRef]
- Braga, V.; Gatti, D.; Rossini, M.; Colapietro, F.; Battaglia, E.; Viapiana, O.; Adami, S. Bone turnover markers in patients with osteogenesis imperfecta. Bone 2004, 34, 1013–1016. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, J.; Takeda, T.; Ichimura, S. Increased bone resorption with decreased activity and increased recruitment of osteoblasts in osteogenesis imperfecta type I. J. Bone Miner. Metab. 2002, 20, 174–179. [Google Scholar] [CrossRef]
- D’Eufemia, P.; Finocchiaro, R.; Zambrano, A.; Lodato, V.; Celli, L.; Finocchiaro, S.; Persiani, P.; Turchetti, A.; Celli, M. Serum creatine kinase isoenzymes in children with osteogenesis imperfecta. Osteoporos. Int. 2017, 28, 339–346. [Google Scholar] [CrossRef]
- Idolazzi, L.; Fassio, A.; Viapiana, O.; Rossini, M.; Adami, G.; Bertoldo, F.; Antoniazzi, F.; Gatti, D. Treatment with neridronate in children and adolescents with osteogenesis imperfecta: Data from open-label, not controlled, three-year Italian study. Bone 2017, 103, 144–149. [Google Scholar] [CrossRef]
- Diacinti, D.; Pisani, D.; Cipriani, C.; Celli, M.; Zambrano, A.; Diacinti, D.; Kripa, E.; Iannacone, A.; Colangelo, L.; Nieddu, L.; et al. Vertebral fracture assessment (VFA) for monitoring vertebral reshaping in children and adolescents with osteogenesis imperfecta treated with intravenous neridronate. Bone 2021, 143, 115608. [Google Scholar] [CrossRef]
- Marom, R.; Lee, Y.C.; Grafe, I.; Lee, B. Pharmacological and biological therapeutic strategies for osteogenesis imperfecta. Am. J. Med. Genet. C Semin. Med. Genet. 2016, 172, 367–383. [Google Scholar] [CrossRef] [PubMed]
- Yao, P.; Bennett, D.; Mafham, M.; Lin, X.; Chen, Z.; Armitage, J.; Clarke, R. Vitamin D and Calcium for the Prevention of Fracture: A Systematic Review and Meta-analysis. JAMA Netw. Open. 2019, 2, e1917789. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Pike, J.W.; Christakos, S. Biology and Mechanisms of Action of the Vitamin D Hormone. Endocrinol. Metab. Clin. N. Am. 2017, 46, 815–843. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930, Erratum in J. Clin. Endocrinol. Metab. 2011, 96, 3908. [Google Scholar] [CrossRef]
- Pilz, S.; Trummer, C.; Theiler-Schwetz, V.; Grübler, M.R.; Verheyen, N.D.; Odler, B.; Karras, S.N.; Zittermann, A.; März, W. Critical Appraisal of Large Vitamin D Randomized Controlled Trials. Nutrients 2022, 14, 303. [Google Scholar] [CrossRef]
- Mohsenzade, P.; Amirhakimi, A.; Honar, N.; Saki, F.; Omrani, G.H.R.; Dabbaghmanesh, M. Bone density, fractures and the associated factors in iranian children and adolescent with Osteogenesis Imperfecta. BMC Pediatr. 2021, 21, 37. [Google Scholar] [CrossRef]
- Kadhim, M.; Holmes, L.; Bober, M.B.; Rogers, K.J.; Kallur, A.; Davey, L.; Kruse, R. Vitamin D Status in Pediatric Patients with Osteogenesis Imperfecta. Pediatr. Therapeut. 2011, 1, 2. [Google Scholar] [CrossRef]
- Wilsford, L.D.; Sullivan, E.; Mazur, L.J. Risk factors for vitamin D deficiency in children with osteogenesis imperfecta. J. Pediatr. Orthop. 2013, 33, 575–579. [Google Scholar] [CrossRef]
- Zambrano, M.B.; Brizola, E.; Pinheiro, B.; Vanz, A.P.; Mello, E.D.; Félix, T.M. Study of the Determinants of Vitamin D Status in Pediatric Patients With Osteogenesis Imperfecta. J. Am. Coll. Nutr. 2016, 35, 339–345. [Google Scholar] [CrossRef]
- Edouard, T.; Glorieux, F.H.; Rauch, F. Predictors and correlates of vitamin D status in children and adolescents with osteoge esis imperfecta. J. Clin. Endocrinol. Metab. 2011, 96, 3193–3198. [Google Scholar] [CrossRef]
- Edouard, T.; Glorieux, F.H.; Rauch, F. Relationship between vitamin D status and bone mineralization, mass, and metabolism in children with osteogenesis imperfecta: Histomorphometric study. J. Bone Miner. Res. 2011, 26, 2245–2251. [Google Scholar] [CrossRef] [PubMed]
- Edouard, T.; Husseini, A.; Glorieux, F.H.; Rauch, F. Serum 24,25-dihydroxyvitamin D concentrations in osteogenesis imperfecta: Relationship to bone parameters. J. Clin. Endocrinol. Metab. 2012, 97, 1243–1249. [Google Scholar] [CrossRef] [PubMed]
- Chagas, C.E.; Roque, J.P.; Santarosa Emo Peters, B.; Lazaretti-Castro, M.; Martini, L.A. Do patients with osteogenesis imperfecta need individualized nutritional support? Nutrition 2012, 28, 138–142. [Google Scholar] [CrossRef]
- Bian, Q.; McAdam, L.; Grynpas, M.; Mitchell, J.; Harrington, J. Increased Rates of Vitamin D Insufficiency in Boys with Duchenne Muscular Dystrophy Despite Higher Vitamin D3 Supplementation. Glob. Pediatr Health 2019, 6, 2333794X19835661. [Google Scholar] [CrossRef] [PubMed]
- Plante, L.; Veilleux, L.N.; Glorieux, F.H.; Weiler, H.; Rauch, F. Effect of high-dose vitamin D supplementation on bone density in youth with osteogenesis imperfecta: A randomized controlled trial. Bone 2016, 86, 36–42. [Google Scholar] [CrossRef]
- Maines, E.; Tadiotto, E.; Morandi, G.; Fedrizzi, M.; Gaudino, R.; Cavarzere, P.; Guzzo, A.; Antoniazzi, F. Hypocalcemia following Neridronate Administration in Pediatric Patients with Osteogenesis Imperfecta: A Prospective Observational Study. J. Pediatr. Genet. 2020, 9, 93–100. [Google Scholar] [CrossRef]
- Dalle Carbonare, L.; Valenti, M.T.; Del Forno, F.; Caneva, E.; Pietrobelli, A. Vitamin D: Daily vs. Monthly Use in Children and Elderly—What Is Going on? Nutrients 2017, 9, 652. [Google Scholar] [CrossRef]
- Pavón de Paz, I.; Rosado Sierra, J.A.; Pérez Blanco, C.; Modroño Móstoles, N.; Guijarro de Armas, G.; Navea Aguilera, C. Acute and long-term effects of zoledronate in adult patients with osteogenesis imperfecta. An observational Spanish study with five years of follow-up. Endocrinol. Diabetes Nutr. 2019, 66, 108–116, (In English and Spanish). [Google Scholar] [CrossRef]
- Herdea, A.; Ionescu, A.; Dragomirescu, M.C.; Ulici, A. Vitamin D-A Risk Factor for Bone Fractures in Children: A Population-Based Prospective Case-Control Randomized Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 3300. [Google Scholar] [CrossRef]
- Herdea, A.; Dragomirescu, M.C.; Ulici, A.; Lungu, C.N.; Charkaoui, A. Controlling the Progression of Curvature in Children and Adolescent Idiopathic Scoliosis Following the Administration of Melatonin, Calcium, and Vitamin D. Children 2022, 9, 758. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coccia, F.; Pietrobelli, A.; Zoller, T.; Guzzo, A.; Cavarzere, P.; Fassio, A.; Flodmark, C.-E.; Gatti, D.; Antoniazzi, F. Vitamin D and Osteogenesis Imperfecta in Pediatrics. Pharmaceuticals 2023, 16, 690. https://doi.org/10.3390/ph16050690
Coccia F, Pietrobelli A, Zoller T, Guzzo A, Cavarzere P, Fassio A, Flodmark C-E, Gatti D, Antoniazzi F. Vitamin D and Osteogenesis Imperfecta in Pediatrics. Pharmaceuticals. 2023; 16(5):690. https://doi.org/10.3390/ph16050690
Chicago/Turabian StyleCoccia, Francesco, Angelo Pietrobelli, Thomas Zoller, Alessandra Guzzo, Paolo Cavarzere, Angelo Fassio, Carl-Erik Flodmark, Davide Gatti, and Franco Antoniazzi. 2023. "Vitamin D and Osteogenesis Imperfecta in Pediatrics" Pharmaceuticals 16, no. 5: 690. https://doi.org/10.3390/ph16050690
APA StyleCoccia, F., Pietrobelli, A., Zoller, T., Guzzo, A., Cavarzere, P., Fassio, A., Flodmark, C.-E., Gatti, D., & Antoniazzi, F. (2023). Vitamin D and Osteogenesis Imperfecta in Pediatrics. Pharmaceuticals, 16(5), 690. https://doi.org/10.3390/ph16050690