
The Effects of Prolonged Treatment with Cemtirestat on Bone Parameters Reflecting Bone Quality in Non-Diabetic and Streptozotocin-Induced Diabetic Rats
 , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
2.1. Blood Biochemistry
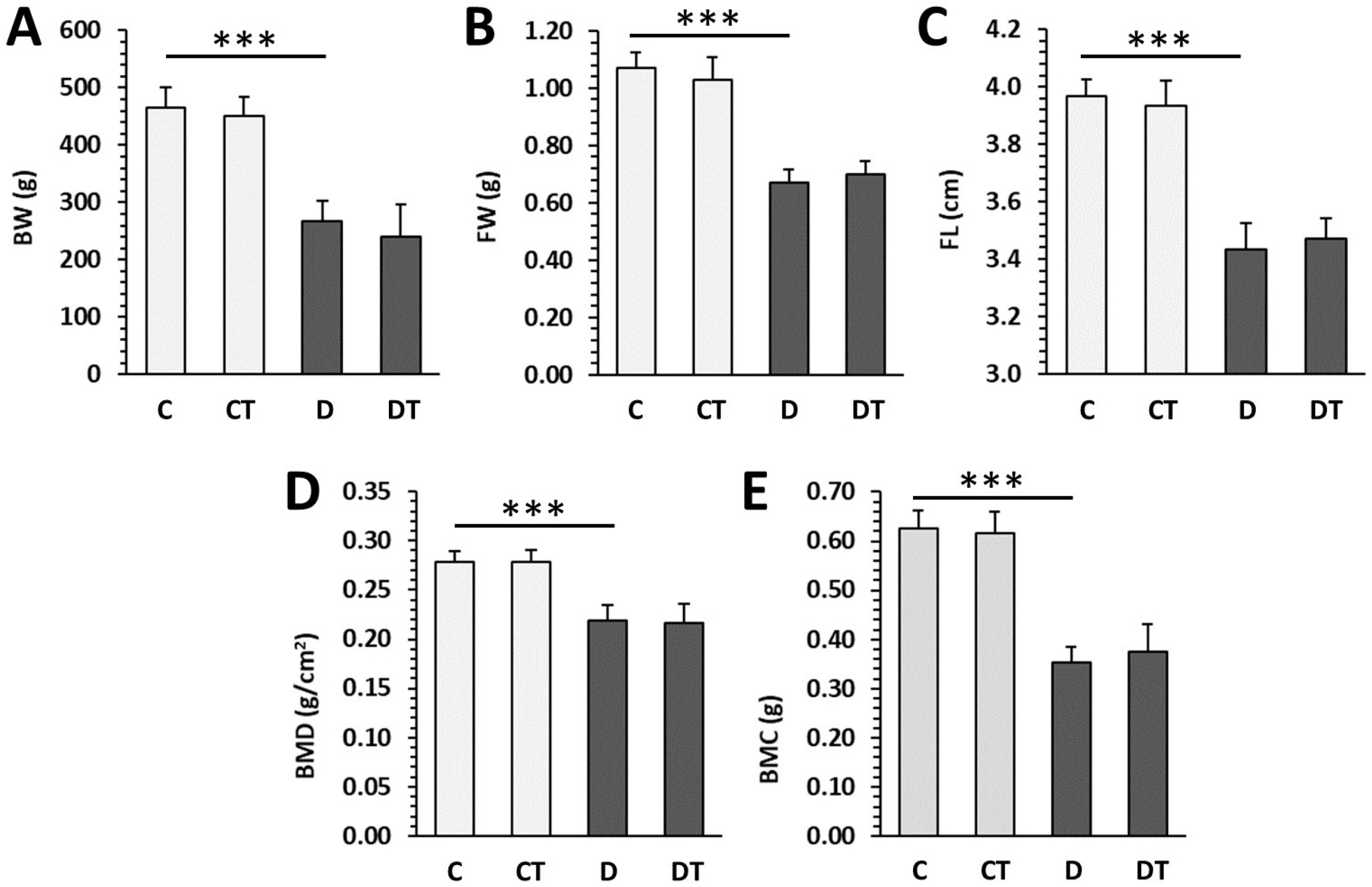
2.2. Macroscopic and Densitometric Indicators
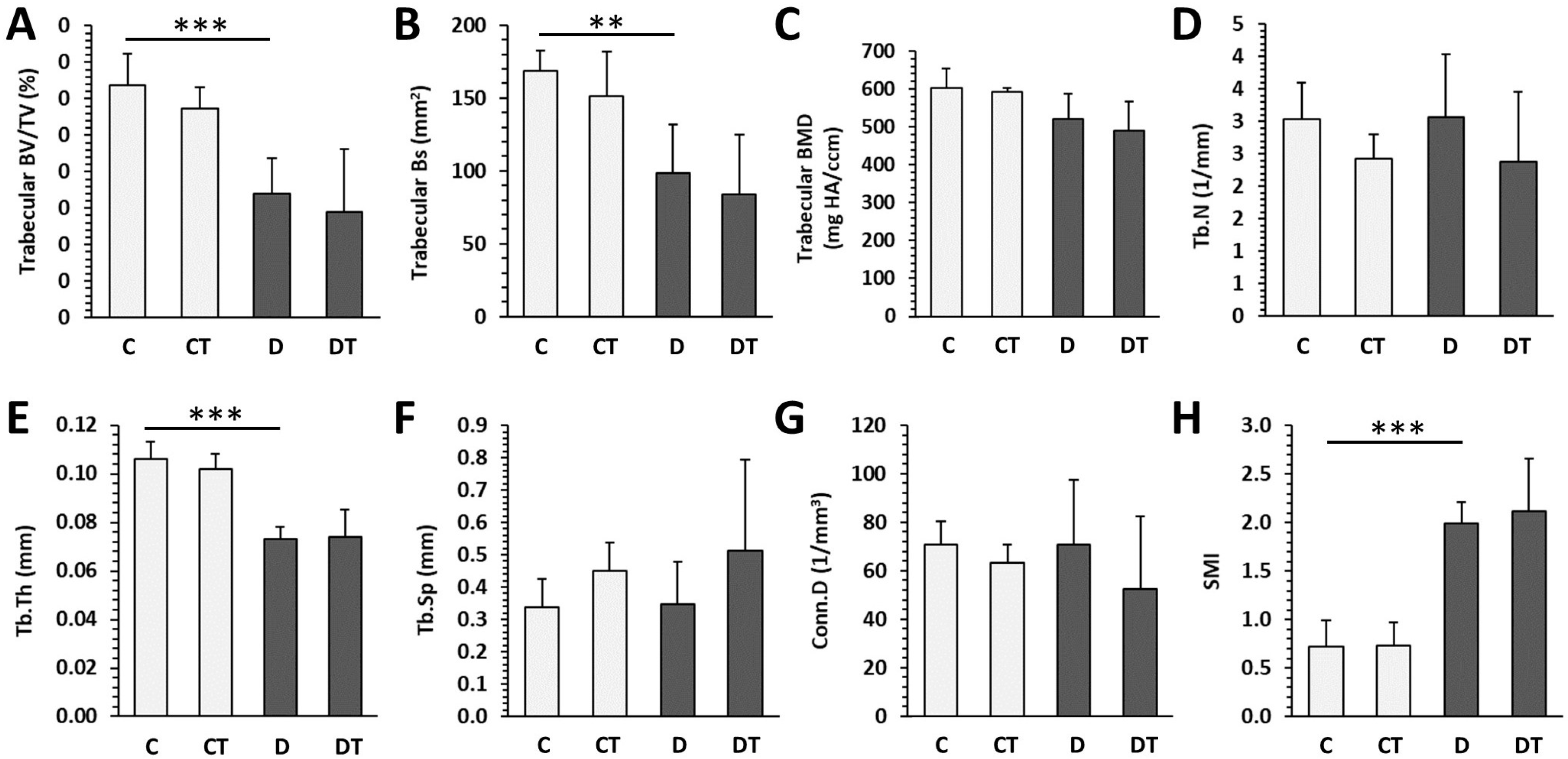
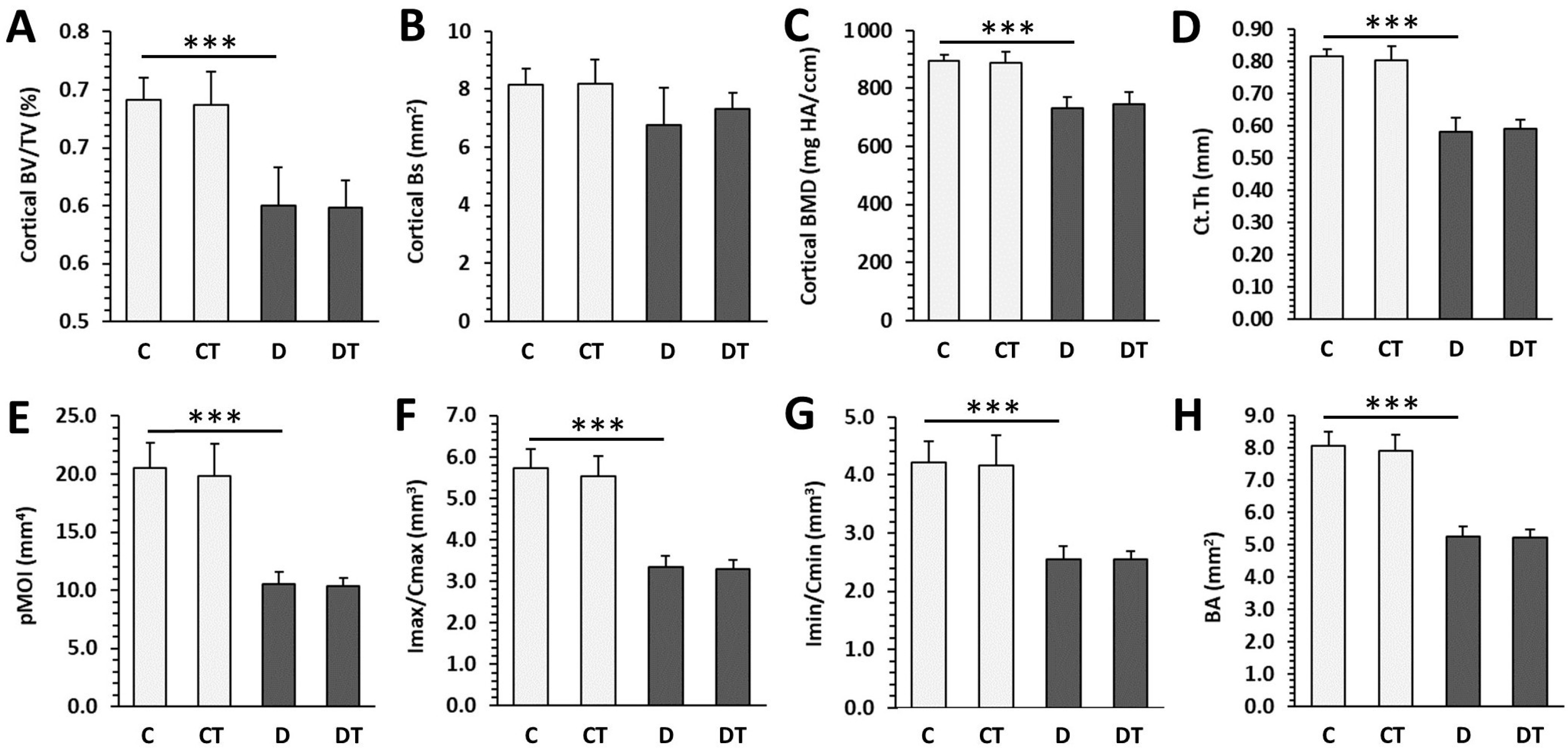
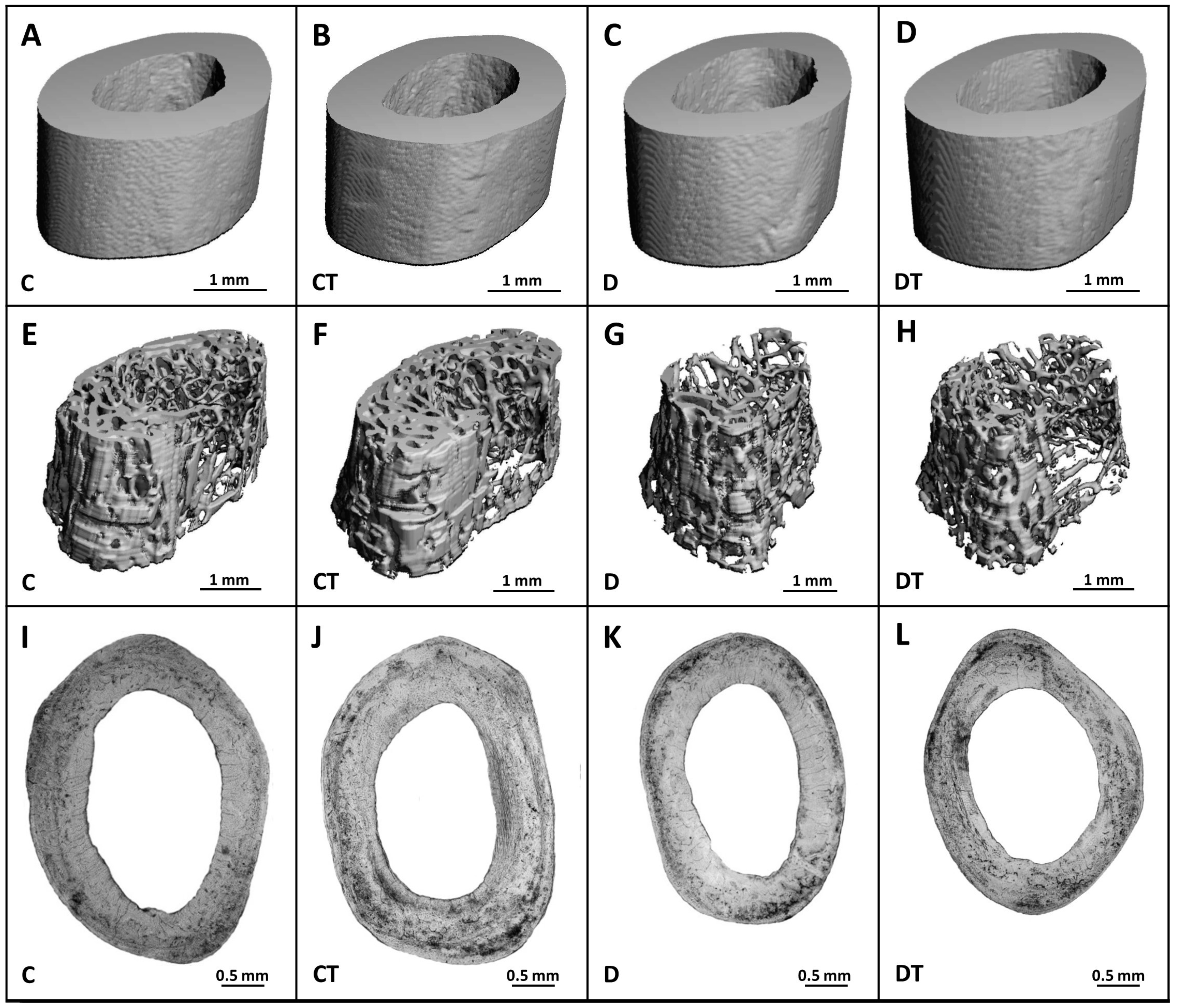
2.3. Microcomputed Tomography
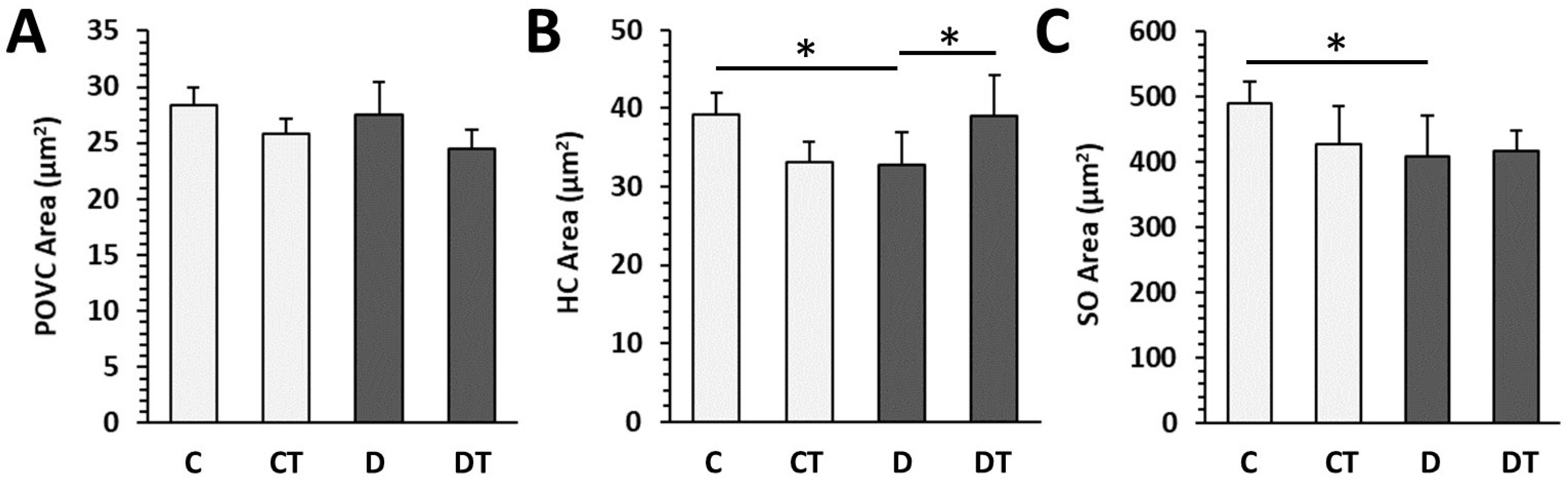
2.4. Histomorphometry
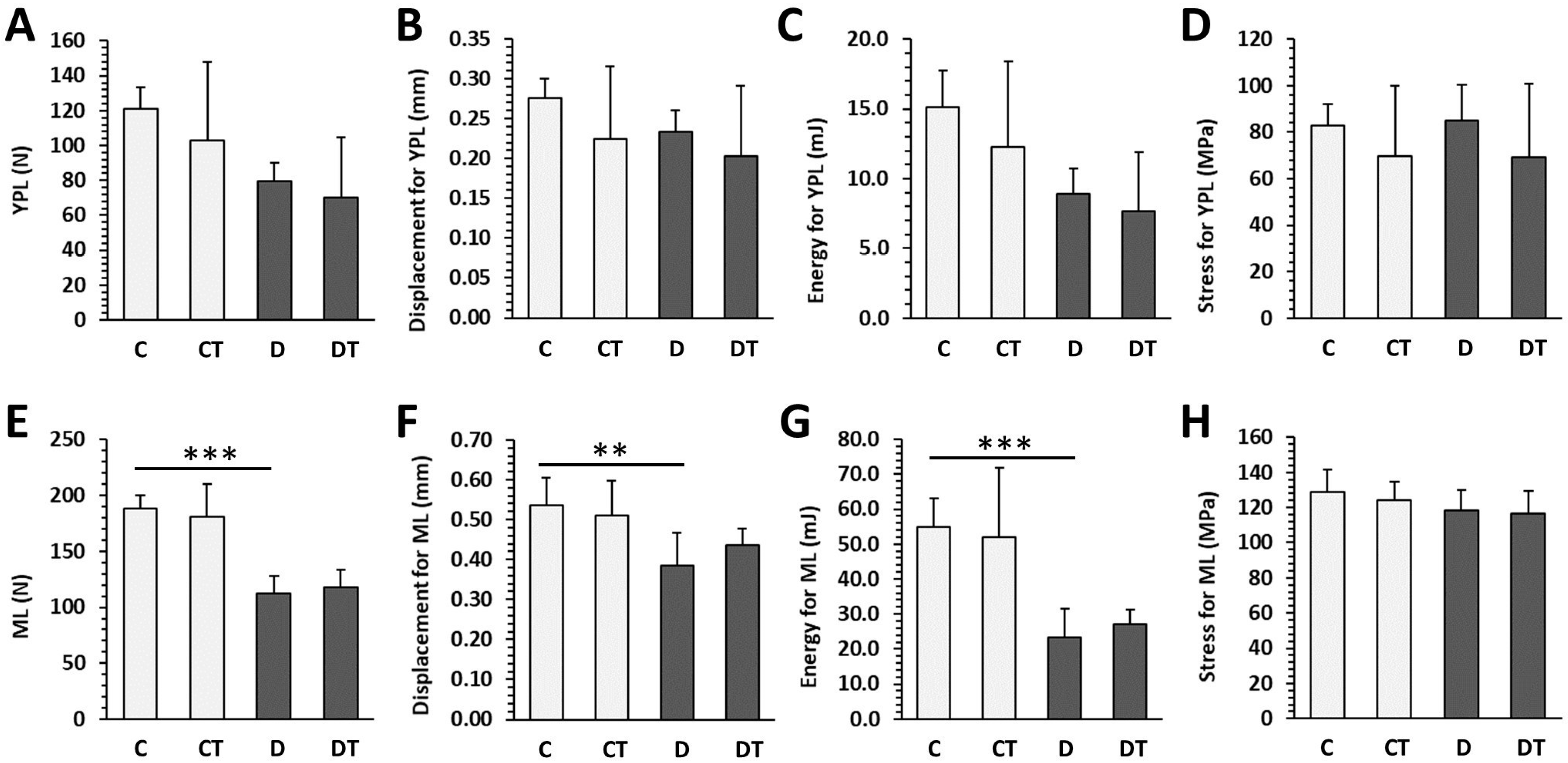
2.5. Bone Mechanical Properties
3. Discussion
4. Materials and Methods
4.1. Animals and Experimental Procedures
4.2. Blood Biochemistry
4.3. Macroscopic and Densitometric Indicators
4.4. Microcomputed Tomography
4.5. Histomorphometry
4.6. Bone Mechanical Properties
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Solis-Herrera, C.; Triplitt, C.; Reasner, C.; DeFronzo, R.A.; Cersosimo, E. Classification of Diabetes Mellitus. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Blahova, J.; Martiniakova, M.; Babikova, M.; Kovacova, V.; Mondockova, V.; Omelka, R. Pharmaceutical Drugs and Natural Therapeutic Products for the Treatment of Type 2 Diabetes Mellitus. Pharmaceuticals 2021, 14, 806. [Google Scholar] [CrossRef]
- Forbes, J.M.; Cooper, M.E. Mechanisms of Diabetic Complications. Physiol. Rev. 2013, 93, 137–188. [Google Scholar] [CrossRef]
- Costantini, S.; Conte, C. Bone Health in Diabetes and Prediabetes. World J. Diabetes 2019, 10, 421–445. [Google Scholar] [CrossRef]
- Kharroubi, A.T.; Darwish, H.M. Diabetes Mellitus: The Epidemic of the Century. World J. Diabetes 2015, 6, 850–867. [Google Scholar] [CrossRef]
- Aikaeli, F.; Njim, T.; Gissing, S.; Moyo, F.; Alam, U.; Mfinanga, S.G.; Okebe, J.; Ramaiya, K.; Webb, E.L.; Jaffar, S.; et al. Prevalence of Microvascular and Macrovascular Complications of Diabetes in Newly Diagnosed Type 2 Diabetes in Low-and-Middle-Income Countries: A Systematic Review and Meta-Analysis. PLOS Glob. Public Health 2022, 2, e0000599. [Google Scholar] [CrossRef]
- Shanbhogue, V.V.; Hansen, S.; Frost, M.; Brixen, K.; Hermann, A.P. Bone Disease in Diabetes: Another Manifestation of Microvascular Disease? Lancet Diabetes Endocrinol. 2017, 5, 827–838. [Google Scholar] [CrossRef]
- Omelka, R.; Blahova, J.; Kovacova, V.; Babikova, M.; Mondockova, V.; Kalafova, A.; Capcarova, M.; Martiniakova, M. Cornelian Cherry Pulp Has Beneficial Impact on Dyslipidemia and Reduced Bone Quality in Zucker Diabetic Fatty Rats. Animals 2020, 10, 2435. [Google Scholar] [CrossRef]
- Conte, C.; Bouillon, R.; Napoli, N. Chapter 40—Diabetes and Bone. In Principles of Bone Biology, 4th ed.; Bilezikian, J.P., Martin, T.J., Clemens, T.L., Rosen, C.J., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 941–969. ISBN 978-0-12-814841-9. [Google Scholar]
- Hygum, K.; Starup-Linde, J.; Langdahl, B.L. Diabetes and Bone. Osteoporos. Sarcopenia 2019, 5, 29–37. [Google Scholar] [CrossRef]
- Martiniakova, M.; Blahova, J.; Kovacova, V.; Babikova, M.; Mondockova, V.; Kalafova, A.; Capcarova, M.; Omelka, R. Bee Bread Can Alleviate Lipid Abnormalities and Impaired Bone Morphology in Obese Zucker Diabetic Rats. Molecules 2021, 26, 2616. [Google Scholar] [CrossRef]
- Moldogazieva, N.T.; Mokhosoev, I.M.; Mel’nikova, T.I.; Porozov, Y.B.; Terentiev, A.A. Oxidative Stress and Advanced Lipoxidation and Glycation End Products (ALEs and AGEs) in Aging and Age-Related Diseases. Oxidative Med. Cell. Longev. 2019, 2019, e3085756. [Google Scholar] [CrossRef]
- Yang, H.-J.; Zhang, T.; Wu, X.-G.; Kim, M.-J.; Kim, Y.-H.; Yang, E.-S.; Yoon, Y.-S.; Park, S. Aqueous Blackcurrant Extract Improves Insulin Sensitivity and Secretion and Modulates the Gut Microbiome in Non-Obese Type 2 Diabetic Rats. Antioxidants 2021, 10, 756. [Google Scholar] [CrossRef]
- Tanaka, K.; Yamaguchi, T.; Kanazawa, I.; Sugimoto, T. Effects of High Glucose and Advanced Glycation End Products on the Expressions of Sclerostin and RANKL as Well as Apoptosis in Osteocyte-like MLO-Y4-A2 Cells. Biochem. Biophys. Res. Commun. 2015, 461, 193–199. [Google Scholar] [CrossRef]
- Vincent, A.M.; Callaghan, B.C.; Smith, A.L.; Feldman, E.L. Diabetic Neuropathy: Cellular Mechanisms as Therapeutic Targets. Nat. Rev. Neurol. 2011, 7, 573–583. [Google Scholar] [CrossRef]
- Feldman, E.L.; Nave, K.-A.; Jensen, T.S.; Bennett, D.L.H. New Horizons in Diabetic Neuropathy: Mechanisms, Bioenergetics, and Pain. Neuron 2017, 93, 1296–1313. [Google Scholar] [CrossRef]
- Oates, P.J. Aldose Reductase, Still a Compelling Target for Diabetic Neuropathy. Curr. Drug Targets 2008, 9, 14–36. [Google Scholar] [CrossRef]
- Alexiou, P.; Pegklidou, K.; Chatzopoulou, M.; Nicolaou, I.; Demopoulos, V.J. Aldose Reductase Enzyme and Its Implication to Major Health Problems of the 21st Century. Curr. Med. Chem. 2009, 16, 734–752. [Google Scholar] [CrossRef]
- Schemmel, K.E.; Padiyara, R.S.; D’Souza, J.J. Aldose Reductase Inhibitors in the Treatment of Diabetic Peripheral Neuropathy: A Review. J. Diabetes Complicat. 2010, 24, 354–360. [Google Scholar] [CrossRef]
- Maccari, R.; Ottanà, R. Targeting Aldose Reductase for the Treatment of Diabetes Complications and Inflammatory Diseases: New Insights and Future Directions. J. Med. Chem. 2015, 58, 2047–2067. [Google Scholar] [CrossRef]
- Singh Grewal, A.; Bhardwaj, S.; Pandita, D.; Lather, V.; Singh Sekhon, B. Updates on Aldose Reductase Inhibitors for Management of Diabetic Complications and Non-Diabetic Diseases. MRMC 2015, 16, 120–162. [Google Scholar] [CrossRef]
- Zhan, J.-Y.; Ma, K.; Zheng, Q.-C.; Yang, G.-H.; Zhang, H.-X. Exploring the Interactional Details between Aldose Reductase (AKR1B1) and 3-Mercapto-5H-1,2,4-Triazino[5,6-b]Indole-5-Acetic Acid through Molecular Dynamics Simulations. J. Biomol. Struct. Dyn. 2019, 37, 1724–1735. [Google Scholar] [CrossRef]
- Stefek, M.; Prnova, M.S.; Ballekova, J.; Majekova, M. Cemtirestat, a Novel Aldose Reductase Inhibitor and Antioxidant, in Multitarget Pharmacology of Diabetic Complications. Int. J. Adv. Sci. Eng. Technol. 2016, 4, 41–44. [Google Scholar]
- Soltesova Prnova, M.; Medina-Campos, O.N.; Pedraza-Chaverri, J.; Colín-González, A.L.; Piedra-García, F.; Rangel-López, E.; Kovacikova, L.; Ceylan, A.; Karasu, C.; Santamaria, A.; et al. Antioxidant Mechanisms in the Neuroprotective Action of Cemtirestat: Studies in Chemical Models, Liposomes and Rat Brain Cortical Slices. Neuroscience 2020, 443, 206–217. [Google Scholar] [CrossRef]
- Prnova, M.S.; Kovacikova, L.; Svik, K.; Bezek, S.; Elmazoğlu, Z.; Karasu, C.; Stefek, M. Triglyceride-Lowering Effect of the Aldose Reductase Inhibitor Cemtirestat—Another Factor That May Contribute to Attenuation of Symptoms of Peripheral Neuropathy in STZ-Diabetic Rats. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2020, 393, 651–661. [Google Scholar] [CrossRef]
- Soltesova Prnova, M.; Svik, K.; Bezek, S.; Kovacikova, L.; Karasu, C.; Stefek, M. 3-Mercapto-5H-1,2,4-Triazino[5,6-b]Indole-5-Acetic Acid (Cemtirestat) Alleviates Symptoms of Peripheral Diabetic Neuropathy in Zucker Diabetic Fatty (ZDF) Rats: A Role of Aldose Reductase. Neurochem. Res. 2019, 44, 1056–1064. [Google Scholar] [CrossRef]
- Pournaghi, P.; Sadrkhanlou, R.-A.; Hasanzadeh, S.; Foroughi, A. An Investigation on Body Weights, Blood Glucose Levels and Pituitary-Gonadal Axis Hormones in Diabetic and Metformin-Treated Diabetic Female Rats. Vet. Res. Forum 2012, 3, 79–84. [Google Scholar]
- Rivoira, M.; Rodríguez, V.; Picotto, G.; Battaglino, R.; Tolosa de Talamoni, N. Naringin Prevents Bone Loss in a Rat Model of Type 1 Diabetes Mellitus. Arch. Biochem. Biophys. 2018, 637, 56–63. [Google Scholar] [CrossRef]
- Vergès, B. Lipid Disorders in Type 1 Diabetes; IntechOpen: Rijeka, Croatia, 2011; ISBN 978-953-307-756-7. [Google Scholar]
- Murase, T.; Tanaka, K.; Iwamoto, Y.; Akanuma, Y.; Kosaka, K. Reciprocal Changes, Caused by Insulin and Glucagon, of Adipose Tissue Lipoprotein Lipase in Rats in Vitro. Horm. Metab. Res. 1981, 13, 212–213. [Google Scholar] [CrossRef]
- Tsutsumi, K.; Inoue, Y.; Shima, A.; Murase, T. Correction of Hypertriglyceridemia with Low High-Density Lipoprotein Cholesterol by the Novel Compound NO-1886, a Lipoprotein Lipase-Promoting Agent, in STZ-Induced Diabetic Rats. Diabetes 1995, 44, 414–417. [Google Scholar] [CrossRef]
- Chi, J.H.; Shin, M.S.; Lee, B.J. Identification of Hypertriglyceridemia Based on Bone Density, Body Fat Mass, and Anthropometry in a Korean Population. BMC Cardiovasc. Disord. 2019, 19, 66. [Google Scholar] [CrossRef]
- Sha, N.-N.; Zhao, Y.-J.; Zhao, D.-F.; Mok, D.K.-W.; Shi, Q.; Wang, Y.-J.; Zhang, Y. Effect of the Water Fraction Isolated from Fructus Ligustri Lucidi Extract on Bone Metabolism via Antagonizing a Calcium-Sensing Receptor in Experimental Type 1 Diabetic Rats. Food Funct. 2017, 8, 4703–4712. [Google Scholar] [CrossRef]
- Locatto, M.E.; Abranzon, H.; Caferra, D.; Fernandez, M.D.C.; Alloatti, R.; Puche, R.C. Growth and Development of Bone Mass in Untreated Alloxan Diabetic Rats. Effects of Collagen Glycosylation and Parathyroid Activity on Bone Turnover. Bone Miner. 1993, 23, 129–144. [Google Scholar] [CrossRef] [PubMed]
- Lucas, P.D. Reversible Reduction in Bone Blood Flow in Streptozotocin-Diabetic Rats. Experientia 1987, 43, 894–895. [Google Scholar] [CrossRef] [PubMed]
- Lekkala, S.; Taylor, E.A.; Hunt, H.B.; Donnelly, E. Effects of Diabetes on Bone Material Properties. Curr. Osteoporos. Rep. 2019, 17, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Londzin, P.; Kocik, S.; Kisiel-Nawrot, E.; Janas, A.; Skoczyńska, A.; Krivošíková, Z.; Štefíková, K.; Gajdoš, M.; Cegieła, U.; Folwarczna, J. Lack of Berberine Effect on Bone Mechanical Properties in Rats with Experimentally Induced Diabetes. Biomed. Pharmacother. 2022, 146, 112562. [Google Scholar] [CrossRef] [PubMed]
- Eller-Vainicher, C.; Zhukouskaya, V.V.; Tolkachev, Y.V.; Koritko, S.S.; Cairoli, E.; Grossi, E.; Beck-Peccoz, P.; Chiodini, I.; Shepelkevich, A.P. Low Bone Mineral Density and Its Predictors in Type 1 Diabetic Patients Evaluated by the Classic Statistics and Artificial Neural Network Analysis. Diabetes Care 2011, 34, 2186–2191. [Google Scholar] [CrossRef]
- Thrailkill, K.; Bunn, R.C.; Lumpkin, C.; Wahl, E.; Cockrell, G.; Morris, L.; Kahn, C.R.; Fowlkes, J.; Nyman, J.S. Loss of Insulin Receptor in Osteoprogenitor Cells Impairs Structural Strength of Bone. J. Diabetes Res. 2014, 2014, 703589. [Google Scholar] [CrossRef]
- Shah, V.N.; Sippl, R.; Joshee, P.; Pyle, L.; Kohrt, W.M.; Schauer, I.E.; Snell-Bergeon, J.K. Trabecular Bone Quality Is Lower in Adults with Type 1 Diabetes and Is Negatively Associated with Insulin Resistance. Osteoporos. Int. 2018, 29, 733–739. [Google Scholar] [CrossRef]
- Shanbhogue, V.V.; Hansen, S.; Frost, M.; Jørgensen, N.R.; Hermann, A.P.; Henriksen, J.E.; Brixen, K. Bone Geometry, Volumetric Density, Microarchitecture, and Estimated Bone Strength Assessed by HR-PQCT in Adult Patients With Type 1 Diabetes Mellitus. J. Bone Miner. Res. 2015, 30, 2188–2199. [Google Scholar] [CrossRef]
- Piemontese, M.; Almeida, M.; Robling, A.G.; Kim, H.-N.; Xiong, J.; Thostenson, J.D.; Weinstein, R.S.; Manolagas, S.C.; O’Brien, C.A.; Jilka, R.L. Old Age Causes de Novo Intracortical Bone Remodeling and Porosity in Mice. JCI Insight 2017, 2, e93771. [Google Scholar] [CrossRef]
- Vidal, B.; Cascão, R.; Finnilä, M.A.J.; Lopes, I.P.; Saarakkala, S.; Zioupos, P.; Canhão, H.; Fonseca, J.E. Early Arthritis Induces Disturbances at Bone Nanostructural Level Reflected in Decreased Tissue Hardness in an Animal Model of Arthritis. PLoS ONE 2018, 13, e0190920. [Google Scholar] [CrossRef]
- Jafri, S.; Hendrix, K.; Cuevas, P.; Pilawski, I.; Helms, J. Examining the Morphological and Physiological Comparisons of OVX Murine Bone vs. Mini Pigs, Rats, and Humans. J. Stud. Res. 2021, 10. [Google Scholar] [CrossRef]
- Nguyen, J.T.; Barak, M.M. Secondary Osteon Structural Heterogeneity between the Cranial and Caudal Cortices of the Proximal Humerus in White-Tailed Deer. J. Exp. Biol. 2020, 223, jeb225482. [Google Scholar] [CrossRef] [PubMed]
- Ascenzi, M.-G.; Chin, J.; Lappe, J.; Recker, R. Non-Osteoporotic Women with Low-Trauma Fracture Present Altered Birefringence in Cortical Bone. Bone 2016, 84, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Romero, M.J.; Platt, D.H.; Tawfik, H.E.; Labazi, M.; El-Remessy, A.B.; Bartoli, M.; Caldwell, R.B.; Caldwell, R.W. Diabetes-Induced Coronary Vascular Dysfunction Involves Increased Arginase Activity. Circ. Res. 2008, 102, 95–102. [Google Scholar] [CrossRef]
- Peng, J.; Qu, H.; Peng, J.; Luo, T.-Y.; Lv, F.-J.; Chen, L.; Wang, Z.-N.; Ouyang, Y.; Cheng, Q.-F. Abnormal Spontaneous Brain Activity in Type 2 Diabetes with and without Microangiopathy Revealed by Regional Homogeneity. Eur. J. Radiol. 2016, 85, 607–615. [Google Scholar] [CrossRef]
- Jannapureddy, S.; Sharma, M.; Yepuri, G.; Schmidt, A.M.; Ramasamy, R. Aldose Reductase: An Emerging Target for Development of Interventions for Diabetic Cardiovascular Complications. Front. Endocrinol. 2021, 12, 636267. [Google Scholar] [CrossRef]
- Gasser, J.A.; Kneissel, M. Bone Physiology and Biology. In Bone Toxicology; Smith, S.Y., Varela, A., Samadfam, R., Eds.; Molecular and Integrative Toxicology; Springer International Publishing: Cham, Switzerland, 2017; pp. 27–94. ISBN 978-3-319-56192-9. [Google Scholar]
- Quattrini, L.; La Motta, C. Aldose Reductase Inhibitors: 2013-Present. Expert Opin. Ther. Pat. 2019, 29, 199–213. [Google Scholar] [CrossRef]
- Balestri, F.; Moschini, R.; Mura, U.; Cappiello, M.; Del Corso, A. In Search of Differential Inhibitors of Aldose Reductase. Biomolecules 2022, 12, 485. [Google Scholar] [CrossRef]
- Inaba, M.; Terada, M.; Nishizawa, Y.; Shioi, A.; Ishimura, E.; Otani, S.; Morii, H. Protective Effect of an Aldose Reductase Inhibitor against Bone Loss in Galactose-Fed Rats: Possible Involvement of the Polyol Pathway in Bone Metabolism. Metabolism 1999, 48, 904–909. [Google Scholar] [CrossRef]
- Glajchen, N.; Epstein, S.; Ismail, F.; Thomas, S.; Fallon, M.; Chakrabarti, S. Bone Mineral Metabolism in Experimental Diabetes Mellitus: Osteocalcin as a Measure of Bone Remodeling. Endocrinology 1988, 123, 290–295. [Google Scholar] [CrossRef]
- Martiniaková, M.; Boboňová, I.; Omelka, R.; Grosskopf, B.; Stawarz, R.; Toman, R. Structural Changes in Femoral Bone Tissue of Rats after Subchronic Peroral Exposure to Selenium. Acta Vet. Scand. 2013, 55, 8. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martiniakova, M.; Kovacova, V.; Mondockova, V.; Svik, K.; Londzin, P.; Folwarczna, J.; Soltesova Prnova, M.; Stefek, M.; Omelka, R. The Effects of Prolonged Treatment with Cemtirestat on Bone Parameters Reflecting Bone Quality in Non-Diabetic and Streptozotocin-Induced Diabetic Rats. Pharmaceuticals 2023, 16, 628. https://doi.org/10.3390/ph16040628
Martiniakova M, Kovacova V, Mondockova V, Svik K, Londzin P, Folwarczna J, Soltesova Prnova M, Stefek M, Omelka R. The Effects of Prolonged Treatment with Cemtirestat on Bone Parameters Reflecting Bone Quality in Non-Diabetic and Streptozotocin-Induced Diabetic Rats. Pharmaceuticals. 2023; 16(4):628. https://doi.org/10.3390/ph16040628
Chicago/Turabian StyleMartiniakova, Monika, Veronika Kovacova, Vladimira Mondockova, Karol Svik, Piotr Londzin, Joanna Folwarczna, Marta Soltesova Prnova, Milan Stefek, and Radoslav Omelka. 2023. "The Effects of Prolonged Treatment with Cemtirestat on Bone Parameters Reflecting Bone Quality in Non-Diabetic and Streptozotocin-Induced Diabetic Rats" Pharmaceuticals 16, no. 4: 628. https://doi.org/10.3390/ph16040628
APA StyleMartiniakova, M., Kovacova, V., Mondockova, V., Svik, K., Londzin, P., Folwarczna, J., Soltesova Prnova, M., Stefek, M., & Omelka, R. (2023). The Effects of Prolonged Treatment with Cemtirestat on Bone Parameters Reflecting Bone Quality in Non-Diabetic and Streptozotocin-Induced Diabetic Rats. Pharmaceuticals, 16(4), 628. https://doi.org/10.3390/ph16040628