1. Introduction
Heart failure has become an increasingly common problem with a mortality rate higher than most cancers. Part of the difficulty associated with treating HF is its multifactorial and variable pathophysiology. However, a common theme in the pathogenesis of HF is mitochondrial dysfunction with altered bioenergetics and impaired ATP production in the myocardium [
1,
2,
3,
4]. Heart muscles require the greatest amounts of energy not only for muscle contraction but also for left ventricle relaxation, which are both highly energy-demanding processes [
5]. Cardiac energetics become altered when the mitochondria are unable to supply sufficient ATP to meet demand due to pathologic conditions such as ischemia and hypoperfusion. The cardiomyocyte itself is quickly injured without adequate ATP to maintain cell homeostasis. The lack of high-energy phosphates has multiple pathological downstream harmful events including vascular dysfunction, cardiac inflammation, cytokines, apoptosis, remodeling (fibrosis and collagen deposition), and cardiac dysfunction, which adversely impact patients’ quality of life [
6,
7,
8]. Clearly, there is a major need for therapies that can address this problem both prophylactically and therapeutically.
Although a variety of current therapies have been proven to benefit heart failure patients such as beta-blockers, ACE inhibitors, Aldactone, and Entresto, there are no drugs in development to specifically target abnormal bioenergetics in the creatine phosphate system and their adverse effects on cardiac muscle function in HF patients. Brown et al. [
3] indicated that the current treatments for HF patients (beta-blockers, ACE inhibitors, Aldactone, and Entresto) are aimed at developing a reduction in myocardial demand sufficient enough to improve muscle bioenergetics. Our approach, on the other hand, is to improve energy reserves in cardiac muscle under ischemia or hypoperfusion using the synthetic analog of creatine phosphate, CCrP, in order to yield clinically meaningful improvements in muscle function. Accordingly, based on our previous studies [
6], CCrP constitutes a new therapeutic strategy by compensating for mitochondrial dysfunction by supplying ATP to restore the adequate ATP levels needed for the appropriate function and homeostasis of cardiac tissues.
CCrP is an FDA orphan drug for heart transplantation, with the designation of “Prevention of Ischemic Injury to Enhance Cardiac Graft Recovery and Survival in Heart Transplantation” (DRU-2015-4951). CCrP is a synthetic analog of the naturally occurring creatine phosphate (CrP). We have previously demonstrated that CCrP is a potent high-energy phosphate donor that is taken up into cardiac tissue and is able to directly phosphorylate adenosine diphosphate (ADP), thereby generating ATP under conditions of limited oxygen supply [
6]. CCrP is a long-acting phosphagen with more favorable enzyme kinetics under acidic/anaerobic conditions than CrP [
9]. CCrP possesses a substantially less negative Gibbs standard free energy of hydrolysis than CrP and, therefore, it continues to thermodynamically buffer the adenylate system at lower pH values and cytosolic phosphorylation potentials that occur during the later stages of ischemia, conditions in which CrP is no longer effective [
9]. Furthermore, Elgebaly SA et al. have previously demonstrated that CCrP preserved high levels of myocardial ATP during ischemia, prevented ischemic injury, reduced cardiac inflammation and apoptosis, and restored normal cardiac function in a variety of animal models of warm and cold ischemia/reperfusion including AMI, global warm cardiac arrest, cardiopulmonary bypass, heart preservation, and heart transplantation [
6].
The purpose of this study was to evaluate the cardioprotective benefits of CCrP in the standard ISO rat model of ischemia-induced HF [
10,
11,
12,
13,
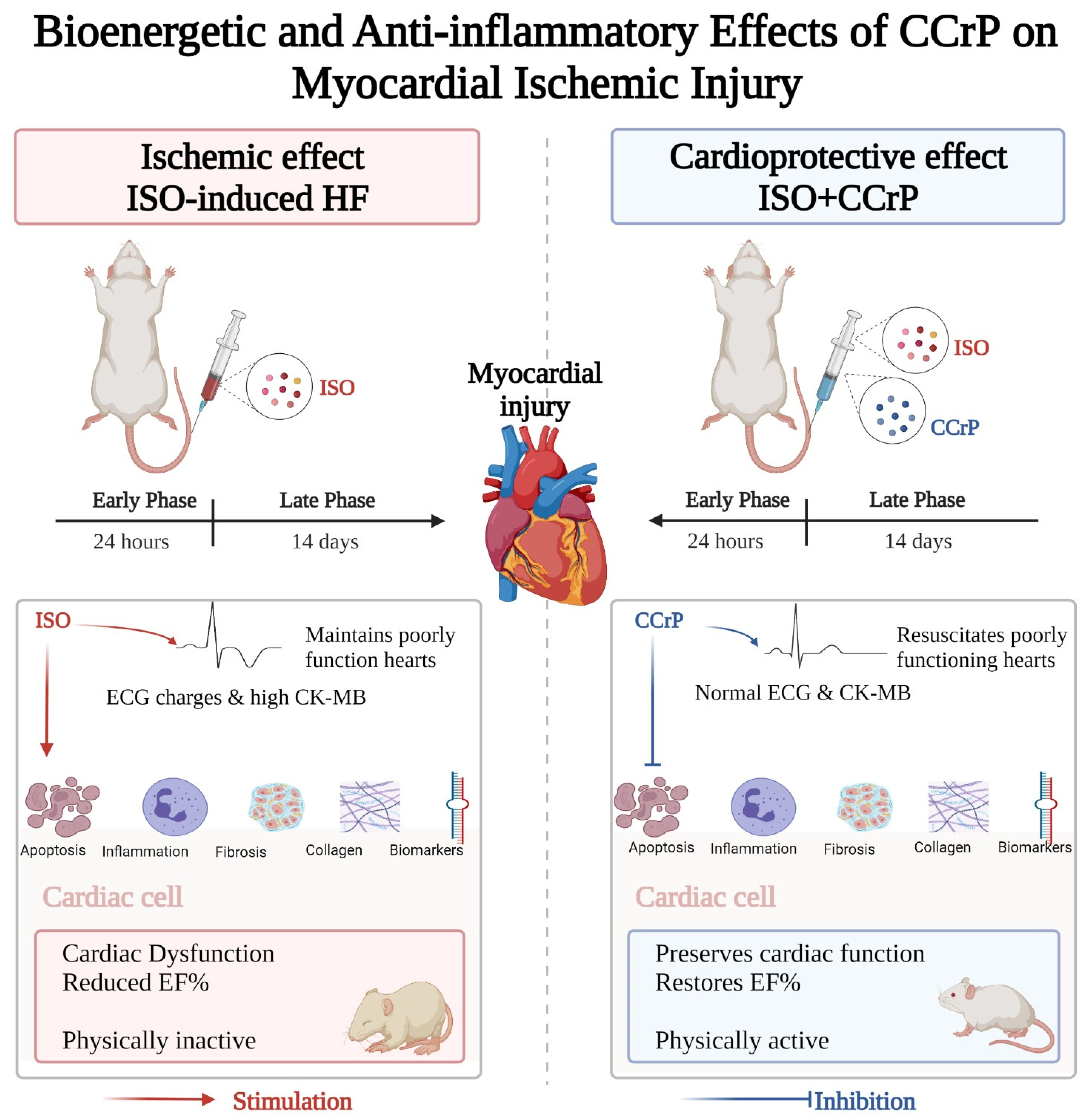
14]. We tested the hypothesis that CCrP treatment will prevent ischemic injury and the development of HF when administered prophylactically and will salvage poorly functioning hearts when administered therapeutically. As described in
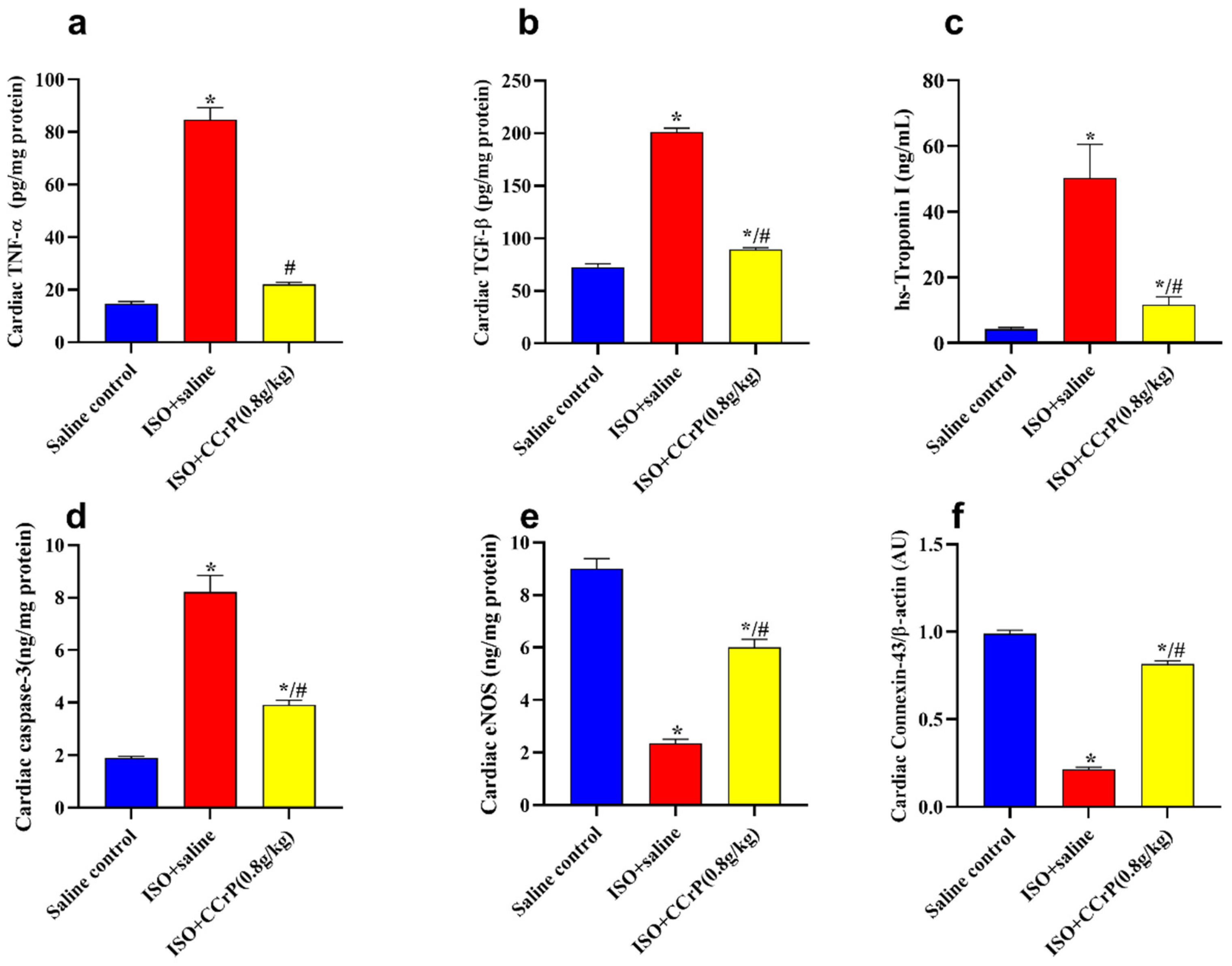
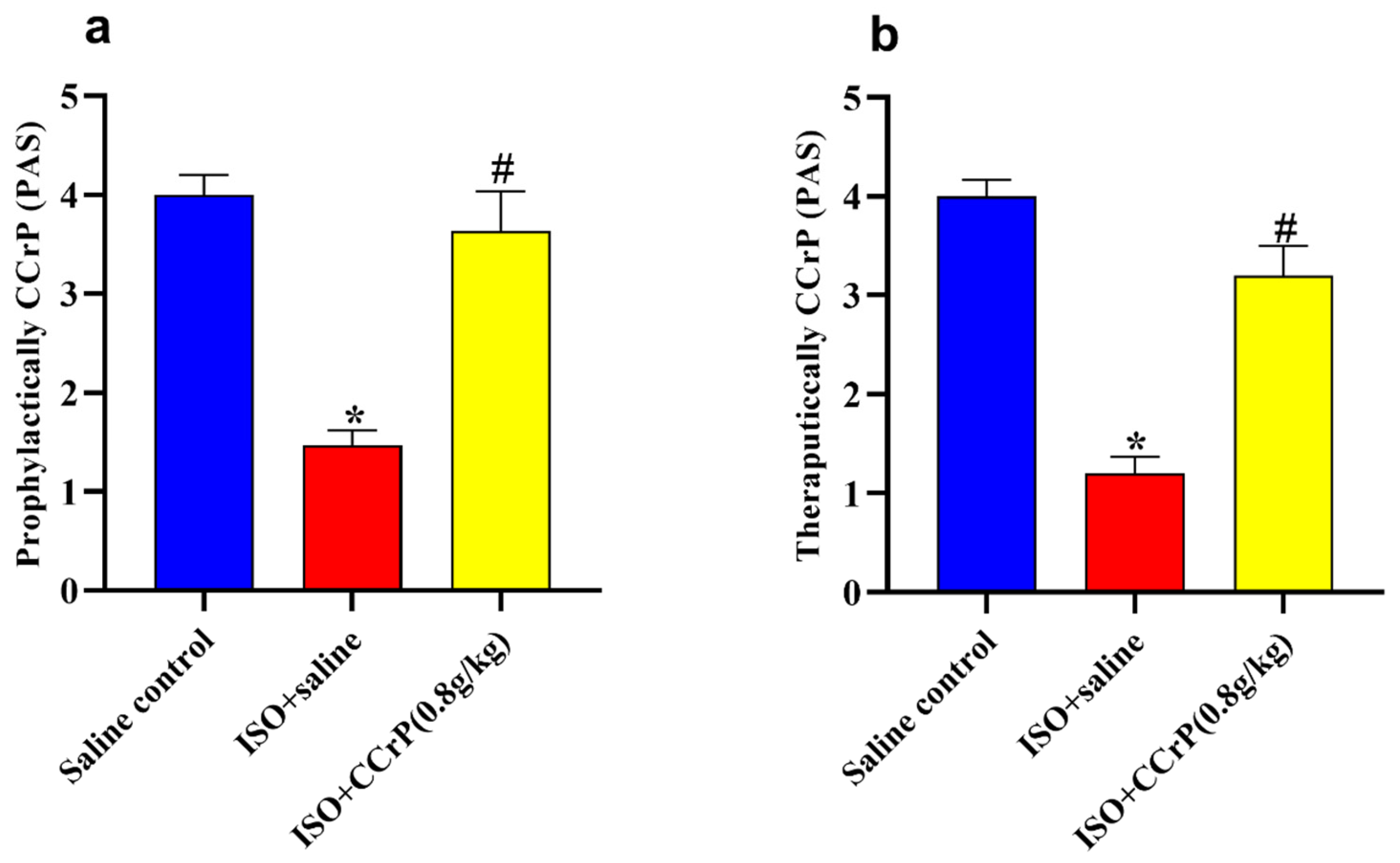
Figure 1, CCrP administered prophylactically (1) prevented ischemic injury in the acute phase of 24 h after the second ISO injection, as shown by normal ECG/ST and CK-MB levels, and (2) significantly protected against the development of HF after 14 days by reducing the downstream harmful events through a marked reduction in cardiac inflammation, apoptosis, biomarkers (hs-TnI, BNP, TNF-α, and TGF-β), remodeling (fibrosis/collagen deposition), and heart weight, but increased expression of eNOS and the cardiac conduction and function, connexin-43 β-actin with the restoration of the normal ejection fraction, cardiac function, and physical activity. When administered therapeutically, CCrP resuscitates poorly functioning hearts in the acute phase of 24 h after the second ISO injection, and the observed normal cardiac function was sustained for an additional 14 days, with the restoration of normal physical activity.
3. Discussion
CCrP is a synthetic analog of CrP which is a potent high-energy phosphate donor that is taken up into the heart tissue and is able to directly phosphorylate adenosine diphosphate, thereby generating ATP under conditions of limited oxygen supply [
6,
9]. It has a longer half-life and more favorable enzyme kinetics under acidic/anaerobic conditions than creatine phosphate [
9]. We have demonstrated that CCrP administration improves myocardial energetics by preserving high levels of myocardial ATP during ischemia and restoring cardiac function in a variety of animal models of ischemia/reperfusion including AMI, global warm cardiac arrest, cardiopulmonary bypass, heart preservation, and heart transplantation [
6].
There is growing recognition that the next generation of therapeutics for HF must address the problem of bioenergetic failure [
3]. Currently, there are two ways to improve ATP stores in cardiomyopathy: reduce utilization or increase supply. Efforts to reduce ATP utilization in the myocyte of cardiomyopathy patients using Mavacamten or Ranolazine have shown mixed results [
15,
16]. Elamipretide is a cell-permeable peptide that enhances mitochondrial ATP production through the interaction with cardiolipin to promote electron transportation. Recently approved anti-hyperglycemic drugs, sodium–glucose co-transporter-2 (SGLT2) inhibitors, improve mitochondrial efficiency by favoring B-hydroxybutyrate oxidation of the heart over fatty acids. This improves the efficiency of ATP production under conditions of limited oxygen supply. Elamipretide and SCLT2 inhibitors showed successful results for preserving mitochondrial function in pre-clinical studies and in patients with heart failure and reduced ejection fraction [
3]. However, their effect on HF is still undergoing trials. Another target for the treatment of HF is the abnormal cardiac remodeling and increasing of stiffness and fibrosis that characterize this disorder. Alterations in intracellular nitrogen mono-oxide signal cascade secondary to oxidative stress are key steps in this process. Vericiguat is an oral soluble guanylate cyclase stimulator that directly generates cyclic guanosine monophosphate and restores the sensitivity of soluble guanylate cyclase to endogenous nitric oxide. Despite the promising primary trials that showed a favorable effect of the drug in improving physical activity when administered to HF patients, large RCTs failed to confirm these findings [
17].
No prior studies have addressed the problem of inefficient production of ATP within the myocytes by directly increasing ATP supply via the phosphocreatine system. Additionally, the therapeutic benefits of CCrP in animal models of heart failure have not been reported. Therefore, based on our previous studies [
6], we believe that the ability of CCrP to preserve high levels of cellular ATP with anti-inflammatory properties makes it a promising novel target for early therapeutic intervention in those with HF. The advantage of CCrP over other therapies designed for this purpose is the simplicity of its mechanism; it merely augments a natural physiological process via CrP so that more ATP is available under conditions where the normal means of supplying ATP are unable to meet demand. Unlike any other drug in development, CCrP does not interfere with normal metabolism. No other agents proposed to treat HF work through a similar mechanism of effect on the phosphocreatine system. Instead, other therapies that attempt to improve ATP supply do so by altering the mitochondrial function.
In the present study, we used the standard ISO rat model of ischemia-induced HF [
13,
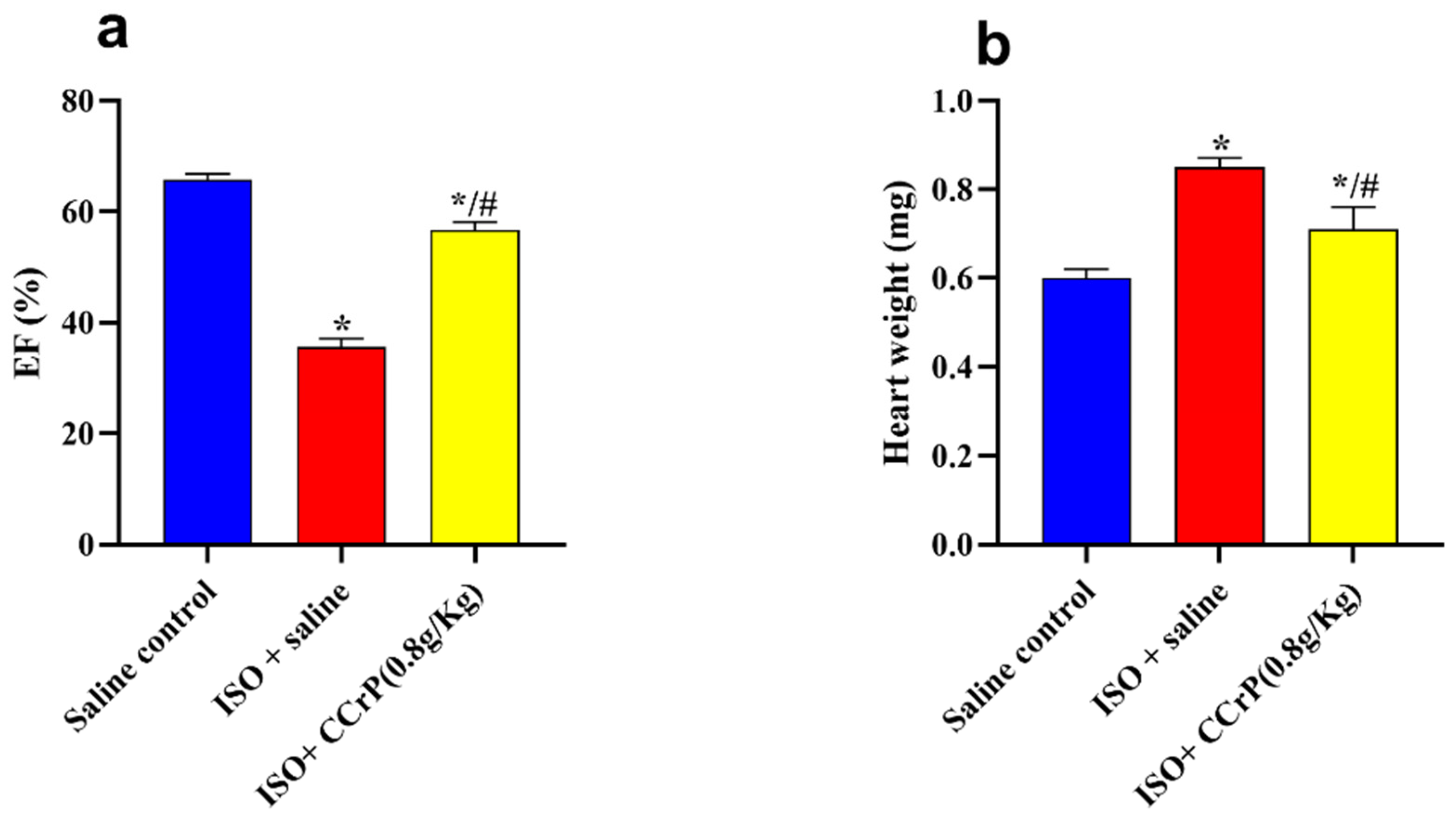
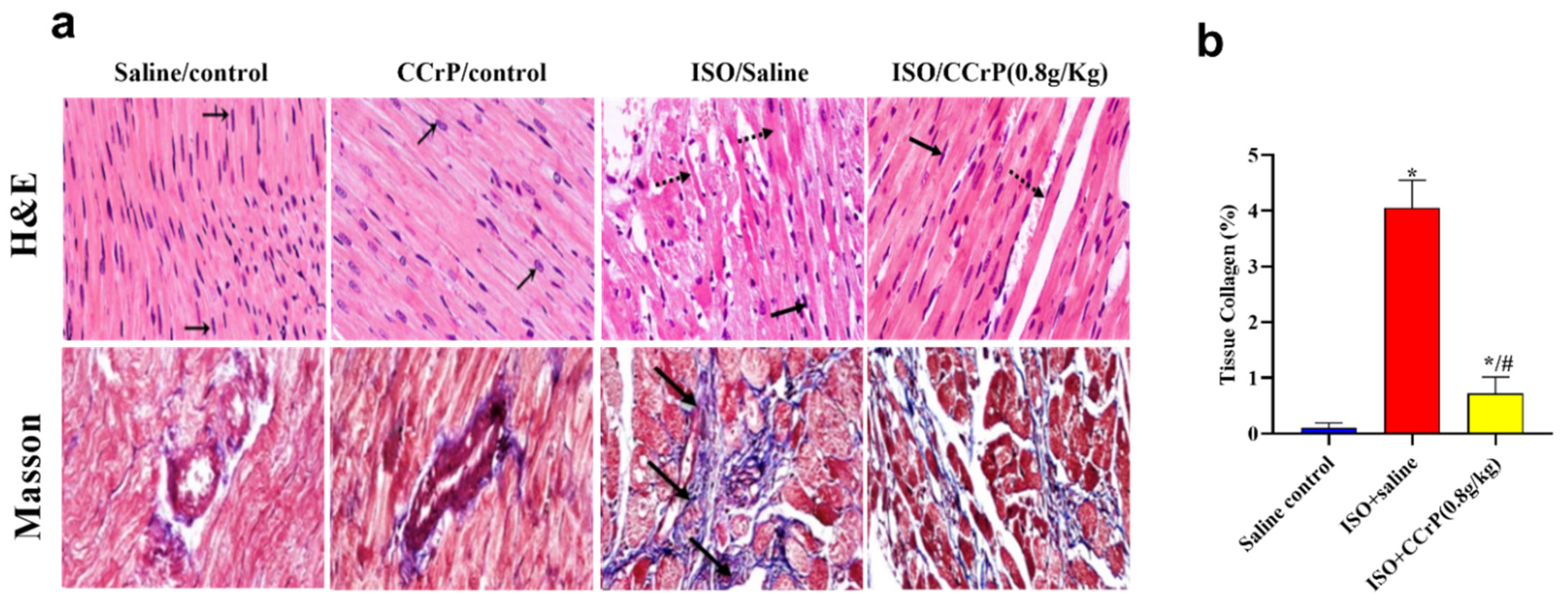
14] and demonstrated that the prophylactic administration of CCrP at the effective dose of 0.8 g/kg/day protected hearts against ischemic injury in the acute phase of 24 h after the last ISO injection, and prevented the subsequent development of HF after 14 days. Similarly, CCrP administered therapeutically after the completion of the second ISO injection resuscitated poorly functioning hearts in the acute phase and continued to preserve normal cardiac function and physical activity for an additional 14 days. Specifically, CCrP significantly altered the underlying mechanism involved in the pathogenesis of HF by (1) maintaining normal heart weight, cardiac function (EF%), and normal physical activity; (2) resuscitating poorly functioning hearts with sustained preservation of normal physical activity after 14 days; (3) significantly reducing the levels of cardiac biomarkers including hs-TnI, BNP, TNF-α, TGF-β, and caspase-3 contents; (4) markedly inhibiting cardiac inflammation and apoptosis; (5) significantly increasing the levels of eNOS and connexin-43 β-actin; and (6) markedly reducing cardiac remodeling (fibrosis and collagen deposition) by over 83%. Furthermore, CCrP at a lower dose of 0.4 g/kg/day and a higher dose of 1.2 g/kg/day continued to show cardioprotection. Thus, the administration of CCrP significantly protected hearts against ischemic injury and the development of HF, as well as resuscitated poorly functioning hearts by reducing the number of downstream harmful events, including cardiac inflammation, apoptosis, and remodeling resulting in the restoration of normal cardiac function and the physical activity of rats. These results support our hypothesis that CCrP treatment prevents ischemic injury and the development of HF when administered prophylactically, and salvages poorly functioning hearts when administered therapeutically.
Previously, we have reported that CCrP treatment inhibited a cardiac molecular mechanism involved in the pathogenesis of HF via the autophagy-related Nourin-dependent
miR-137 (a marker of myocardial ischemic damage which promotes cardiac remodeling in HF) and Nourin-dependent
miR-106b (a marker of inflammation which promotes cardiac inflammation) [
12]. Specifically, the Nourin-associated miR-137 and miR-106b were significantly upregulated in the ISO/saline rats, but not in the ISO/CCrP rats that did not develop HF [
12], further supporting the anti-inflammatory property of CCrP.
The results of the limited safety study, where healthy rats were treated with CCrP at a dose of 0.8 g/kg/day for 14 consecutive days (CCrP control), showed no toxicity in rat hearts as evidenced by the absence of cardiac inflammation, apoptosis, biomarkers, and remodeling, and that these rats continued to exhibit normal cardiac function and physical activity similar to the saline control rats. The lack of cardiac toxicity further confirms our recently reported studies that the administration of CCrP did not alter liver and renal function, suggesting that CCrP is a safe drug [
12].
We believe that CCrP can potentially have a number of clinical applications as a bioenergetic/anti-inflammatory cardioprotective drug in heart transplantation, high-risk cardiac surgery, intervention cardiology, delayed AMI patients, and patients with Takotsubo cardiomyopathy.
A. Heart transplantation—The number of heart transplants performed each year in the U.S. has significantly lagged behind liver and kidney placement, with 3902 heart transplants in 2021 compared to 8896 liver transplants and 23,401 kidney transplants [
18,
19]. In this regard, the percentage of hearts donated in 2021 was only 28% of organ donors as 6 hearts from every 10 organ donors are unutilized. This happens due to the following two important factors: (1) donors with poor heart function, and (2) ischemic injury caused by harvesting and ex vivo cold static storage, particularly transport periods that exceed 4 h. As an FDA orphan designated drug for the “Prevention of Ischemic Injury to Enhance Cardiac Graft Recovery and Survival in Heart Transplantation” (DRU-2015-4951), CCrP can improve donor heart bioenergetics which will allow for prolonged transport times (e.g., >6 h compared to the current 4 h) [
6] and salvage poorly functioning donors’ hearts. Thus, CCrP can potentially increase donor heart utilization and the safety of heart transplantation beyond what is possible with current methods.
B. High-risk cardiac surgery and intervention cardiology—CCrP can potentially protect against complications in the following areas:
(1) Patients who have completed the high-risk transcatheter aortic valve implantation (TAVI) procedure. Significant complications of high-risk TAVI procedures include death (6–7% one-year mortality), heart failure (19–23%), and stroke (up to 5%) [
20]. During the procedure, myocardial ischemia occurs, which can cause low cardiac output syndrome (LCOS) at the end of the procedure. We believe that CCrP administration immediately prior to the TAVI procedure will significantly protect hearts against this initial ischemic injury and have a positive impact on reducing short- and long-term complications triggered by LCOS.
(2) Patients who are undergoing high-risk cardiac surgery. There are approximately 200,000 cardiac surgical procedures performed per year in the U.S. About 10% of these cases are considered to be high-risk, defined as more than 5% predicted risk of perioperative mortality. This risk can be accurately predicted based on calculations performed prior to surgery that depend on the procedure, comorbidities, and other factors available in the medical record. The main reason that high-risk patients die after surgery is due to LCOS. This clinical syndrome is often characterized by reduced cardiac ejection fraction after surgery, poor cardiac output relative to needs, hypotension, and acidosis, and it eventually leads to multiorgan failure and death. Much of this problem results from poor cardiac protection during the period of cardiac arrest required to perform the surgical procedure. Efforts to improve this protection, using CCrP, may improve cardiac function after surgery and reduce the mortality associated with LCOS.
(3) Patients who are undergoing intervention cardiology. There are approximately one million percutaneous coronary intervention (PCI) procedures performed per year in the U.S. About 10% of these procedures are considered to be high-risk. Protecting cardiac tissues during these high-risk cases will potentially reduce cardiac injury and preserve cardiac function.
C. Delayed AMI patients—Every year, about 805,000 people in the U.S. experience AMI [
21]. Currently, more than 50% of patients with AMI seek medical care late [
21]. A delay after the onset of infarction in treatment using current existing strategies leads to a higher incidence of heart failure (HF), particularly for women [
22,
23]. Based on our positive results that CCrP resuscitates poorly functioning hearts and preserves prolonged normal cardiac function, we believe that CCrP administration to patients with delayed AMI will potentially protect adjacent areas from progressing to necrotic myocardium and reduce the subsequent development of HF.
D. Takotsubo cardiomyopathy—This refers to the treatment of patients with Takotsubo cardiomyopathy to reduce death or congestive heart failure. Takotsubo cardiomyopathy (approximately 25,000 cases yearly) is due to ischemia-induced non-ST elevation myocardial infarction (non-STEMI) thought to be associated with acute physical or psychological stress. The disorder is not due to coronary artery disease and is characterized by a typical apical ballooning of the left ventricle shown via echocardiogram that usually improves over the course of several months. However, stress cardiomyopathy can lead to death or congestive heart failure with 80 to 90% of cases being women [
24,
25]. A registry has been established to record these cases and distinguish them from STEMI cases [
26]. Of note, the abnormal echocardiography findings and proposed pathophysiology in Takotsubo cardiomyopathy patients are comparable to those observed in organ donors with poor cardiac contractility [
27]. Since this cardiomyopathy is associated with acute cardiac stress, and we have demonstrated in the present study that CCrP resuscitates poorly functioning hearts, maintains prolonged normal cardiac function, and prevents the development of HF in the ischemia-induced myocardial injury rat model of Takotsubo, it appears reasonable that the acute treatment of Takotsubo patients with CCrP might speed up recovery and minimize the long-term morbidity and/or mortality from this disorder.
In conclusion, CCrP is a promising novel bioenergetic/anti-inflammatory drug that prevents ischemic injury and the development of HF by blocking key harmful downstream events of ischemia (inflammation, apoptosis, remodeling, and cardiac dysfunction). Potential future therapeutic applications of CCrP include heart transplantation, high-risk cardiac surgery, intervention cardiology, patients with Takotsubo cardiomyopathy, and patients with delayed AMI.
4. Materials and Methods
4.1. Experimental ISO Rat Model (ISO/Saline “HF Rats” and ISO/CCrP “Non-HF Rats”)
A standard ISO rat model of ischemia-induced heart failure was used to determine whether CCrP administered prophylactically prevents ischemic injury and the subsequent development of heart failure (HF) and whether the administration of CCrP therapeutically resuscitates poorly functioning hearts and sustains the preserved cardiac function over 14 days. We purchased from Cairo University Research Park’s Animal Technology Laboratory (Dokki, Cairo, Egypt) adult male Wistar rats (6–8 weeks old) weighing 180–220 g. Rats were caged under controlled temperature (20–25 °C) and humidity (45–55%) conditions with a twelve hour light/dark cycle and free access to food and water. Prior to the experiment, animals were housed for a couple of weeks to accommodate them, and then they were randomly distributed across the groups. Solutions of highly pure CCrP (>98%) (Nour Heart, Inc., Vienna, VA, USA) were freshly prepared before use.
All experimental procedures were approved by the Faculty of Pharmacy Ethics Committee at Cairo University (permit number: PT 2733), and they were carried out in accordance with the US National Institutes of Health’s Guide for Care and Use of Laboratory Animals (NIH publication no. 85-23, revised in 2011). The project began on 19 May 2019.
4.1.1. CCrP Administered Prophylactically
Rats were injected with isoproterenol hydrochloride (Sigma Aldrich; Merck KGaA, Darmstadt, Germany, Cat. # 15627) subcutaneously (s.c.) for two consecutive days at specific doses of 85 and 170 mg/kg/day (the LD50 for s.c. isoproterenol in rats = 600 mg/kg), respectively, and then left for an additional two weeks [
10,
11,
12,
13,
14]. The ISO/saline rats were treated with 1 mL saline via intraperitoneal (IP) injection both 24 h and 1 h before the first ISO administration, and then daily for two weeks. The ISO/CCrP rats were also treated via IP injection with 1 mL CCrP solution 24 h and 1 h before the first ISO administration, and then daily for an additional two weeks. Prior to use, solutions of CCrP were freshly prepared in saline. According to our previous studies, CCrP at a dose of 0.8 gm/kg/day is the most effective dose to prevent myocardial ischemic injury in intact canine and rat models of acute myocardial ischemia, global cardiac arrest, cardiopulmonary bypass, and heart transplantation [
6,
10,
11,
12].
Adult male Wistar rats were divided into four groups: (1) ISO/saline (n = 6), where ISO rats were treated with IP injections of saline; (2) ISO/CCrP (n = 5), where ISO rats were treated with IP injections of CCrP at a dose of 0.8 g/kg/day; (3) saline/control (n = 5), where healthy rats were treated with IP injections of saline; and (4) CCrP/control (n = 4), where healthy rats were treated with IP injections of CCrP at a dose of 0.8 g/kg/day for 14 days to evaluate the potential drug toxicity [
12]. The cardioprotective activity of CCrP was also tested using a lower dose of 0.4 g/kg/day (n = 3) and a higher dose of 1.2 g/kg/day (n = 2). Additionally, various parameters including serum CK-MB (rat Creatine Kinase MB Isoenzyme ELISA Kit (Cat no: DEIA-FN285) Creative Diagnostics, New York, NY, USA) and ECG analysis were conducted 24 h after the first dose of ISO to confirm the development of early myocardial injury. Fourteen days after the second ISO injection, we measured the following parameters: heart weight, EF%, ECHO analysis, and physical activity, as well as cardiac fibrosis, percentage of deposited collagen, serum levels of high-sensitivity rat cardiac Troponin I, BNP, and various protein expressions in the ventricles including tumor necrosis factor-alpha (TNF-α) (inflammation marker), transforming growth factor-beta (TGF-β) (fibrogenic marker), vascular function-endothelial nitric oxide synthase (eNOS), apoptosis-caspase-3, and the cardiac conduction and function-connexin-43 β-actin.
In humans, CCrP will be used at the effective dose of 0.21 gm/kg for an average 100 kg person [
28].
4.1.2. CCrP Administered Therapeutically
For this study, a total of 18 male Wistar albino rats (170 to 190 gm) were used. Isoproterenol hydrochloride was procured from Sigma-Aldrich, St. Louis, MO, USA, Cat. # 15627. ISO was administered subcutaneously to rats over the course of two consecutive days at doses of 85 mg/kg (first day) and 170 mg/kg (second day) [
10,
11,
12,
13,
14]. Only rats (n = 10) that showed cardiac dysfunction via electrocardiographic abnormalities (ST elevation) and high serum creatine kinase-MB 24 h after the second ISO injection were allowed to proceed to complete the study for an additional 14 days. These 10 rats with poor heart function were randomized into two groups and received saline or CCrP one hour after completing the course of the second ISO injections and then daily for an additional 2 weeks. Four rats received a saline injection (1 mL/i.p.) (ISO + saline, n = 4) and six rats received CCrP at an effective dose of 0.8 g/kg/day (ISO + CCrP, n = 6) [
10]. A negative control group of healthy rats was injected with saline (saline/control, n = 4). After 14 days, evidence of stress cardiomyopathy was assessed via ECHO analysis for EF% measurements, serum levels of hs-TnI and BNP, and physical activity.
4.2. Assessment of Heart Function
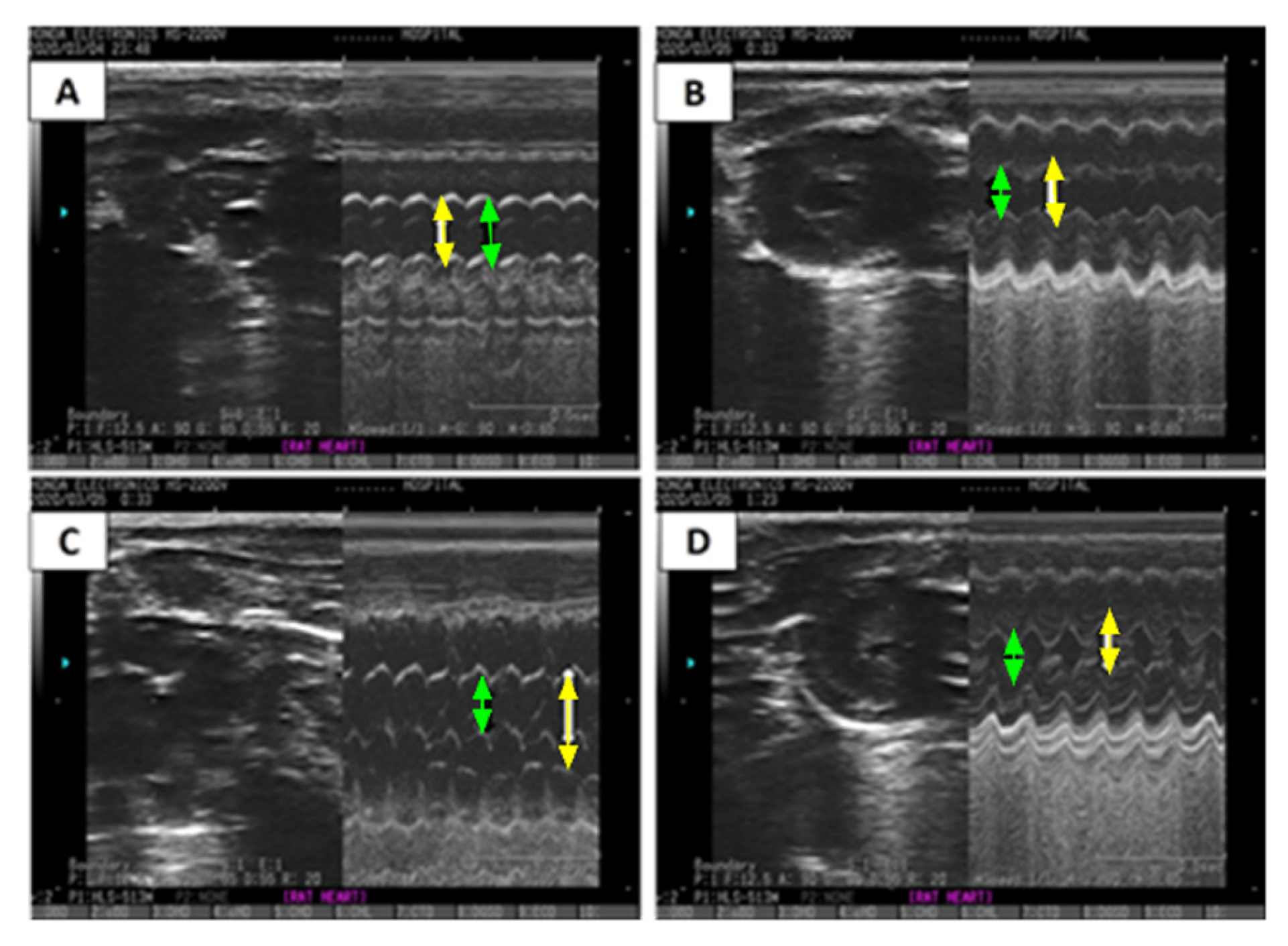
The electrical activity of the heart was measured 24 h and 14 days after the second ISO injection to evaluate the acute and long-term responses to CCrP treatment. An electrode was inserted subcutaneously into the limb under anesthesia (50 mg/kg of thiopental) to record ECGs. The ECGs were used to calculate heart rate, QT interval, and QRS duration. After 14 days, heart function was evaluated using ECHO, which used an ultrasound probe (Honda HS-2200 V, Tokyo, Japan) to measure the dimensions of the left ventricle and calculate the ejection fraction percentage. This was achieved using a 12.5-MHz probe, and the measurements were taken as an average over three cardiac cycles. The LVEDD and LVESD, as well as the EF%, were automatically calculated in the M-Mode of the long-axis parasternal view and provided by the built-in software [
11].
4.3. Physical Activity
Fourteen days after the second ISO injection, the scoring of physical activity was recorded as follows: normal activity (+4); mild physical impairment (+3); moderate physical impairment (+2); and severe physical impairment (+1) [
6].
4.4. Sample Processing and Heart Weight Index (HWI) Determination
Twenty-four hours after the last ISO injection, serum samples were collected to measure the levels of CK-MB using the rat creatine kinase MB isoenzyme ELISA Kit (Cat. No. DEIA-FN285; Creative Diagnostics, USA). The instructions provided by the kit’s manufacturer were followed. At the end of the study, 14 days after the last ISO injection, rats were sacrificed via decollation under anesthesia using 30 mg/kg pentobarbital. Hearts were quickly removed and rinsed with cold phosphate-buffered saline and weighed after removing the atria, aorta, and fat. The weights of the rats were also recorded and the heart weight index (HWI, in mg/g) was calculated by dividing heart weight by rat weight. Hearts from 3 rats from each group were used for a histopathological examination. The remaining rats’ ventricles were quickly dissected, rinsed, dried, and weighed. One part was homogenized in cold phosphate-buffered saline to create a 10% homogenate, and the other part was frozen at −80 °C for later use in further analysis.
4.5. Biochemical Assessment
Enzyme-linked immunoassay (ELISA) was used to measure brain natriuretic peptide (BNP) (MyBioSource, Inc., San Diego, CA, USA, Cat. # MBS2700198) and rat Troponin I type 3 (cTn-I) in the serum as markers for HF using the rat high-sensitivity Troponin I type 3 (cTn-I) (MyBioSource, Inc., San Diego, CA, USA, Cat. # MBS765393). Additionally, ELISA was used to measure the levels of tumor necrosis factor-alpha (TNF-α) (Cat. # MBS2507393), transforming growth factor-beta (TGF-β) (Cat. # MBS260302), endothelial nitric oxide synthase (eNOS) (Cat. # MBS721860), and caspase-3 (Cat. # MBS763727) in tissue homogenates using corresponding kits (MyBioSource, Inc., San Diego, CA, USA).
Protein concentrations were assessed via Western blot analysis on a portion of the ventricle that was homogenized in lysis buffer. A connexin-43 primary antibody (Thermofisher Scientific, Waltham, MA, USA, Cat. # 71-0700) and horseradish peroxidase (HRP)-conjugated goat anti-rabbit secondary antibody (Thermofisher Scientific, USA, Cat. # 31460) were used to measure protein expression and determine protein levels using a Bicinchoninic acid (BCA) protein assay kit (Thermo Fisher Scientific Inc., USA) [
13]. Using a scanning laser densitometer from Biomed Instrument, Clinton Charter Township, MI, USA, the amount of protein was determined via densitometric analysis of the autoradiograms. The results were adjusted to beta-actin and expressed as a change from the normal levels in the saline control group.
4.6. Histopathological Assessment
The heart tissues of the rats were preserved in a 10% formalin solution and embedded in paraffin wax blocks. Five-micrometer sections were cut using an ultra-microtome and sections were stained with H&E. The slides were examined under a light microscope (Olympus, Tokyo, Japan) and the images were captured using a digital camera. Additionally, a semi-quantitative scoring system (morphometry) was used to measure the amount of cardiac collagen, with 0 indicating no collagen, 1 indicating moderate collagen, and 3 indicating intense collagen. Sections of the hearts (5 m) were stained with Masson trichrome to evaluate the extent of myocardial fibrosis and to identify collagen fibers in cardiac tissues using an image analyzer (Leica Qwin 550, Wetzlar, Hesse, Germany). The percentage of fibrosis for each group was calculated by calculating the average of 10 randomly selected fields from each section. Sections were also stained with H&E to evaluate myocardial damage and hypertrophy. A semi-quantitative grading scale of 0–5 was used to assess myocardial injury [
14]. Two independent pathologists who were blinded to the study groups and the experimental setup examined the heart morphology for each section.
4.7. Statistical Analysis
Quantitative values were expressed as the mean ± standard error of the mean (mean ± S.E.M) of 3 to 6 rats per group. The significant difference in the measured variables between different experimental groups was data analyzed using GraphPad Prism (version: 8; GraphPad Software Inc., San Diego, CA, USA). The analysis of variance test (ANOVA) followed by Dunn’s multiple comparison test were used to compare multi-group results. A p-value <0.05 was considered to be statistically significant. Normality was checked using the Shapiro–Wilk test and homogeneity was checked using Levene’s test.



 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}