

The Anti-Nociceptive Effects of Nicotine in Humans: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
- (1)
- Search strategy via PubMed:
- (2)
- Search strategy via Cochrane Library:
- (3)
- Search strategy via Embase:
2.2. Inclusion Criteria
2.3. Data Extraction and Risk of Bias
2.4. Quality Assessment
2.5. Data Analysis
3. Results
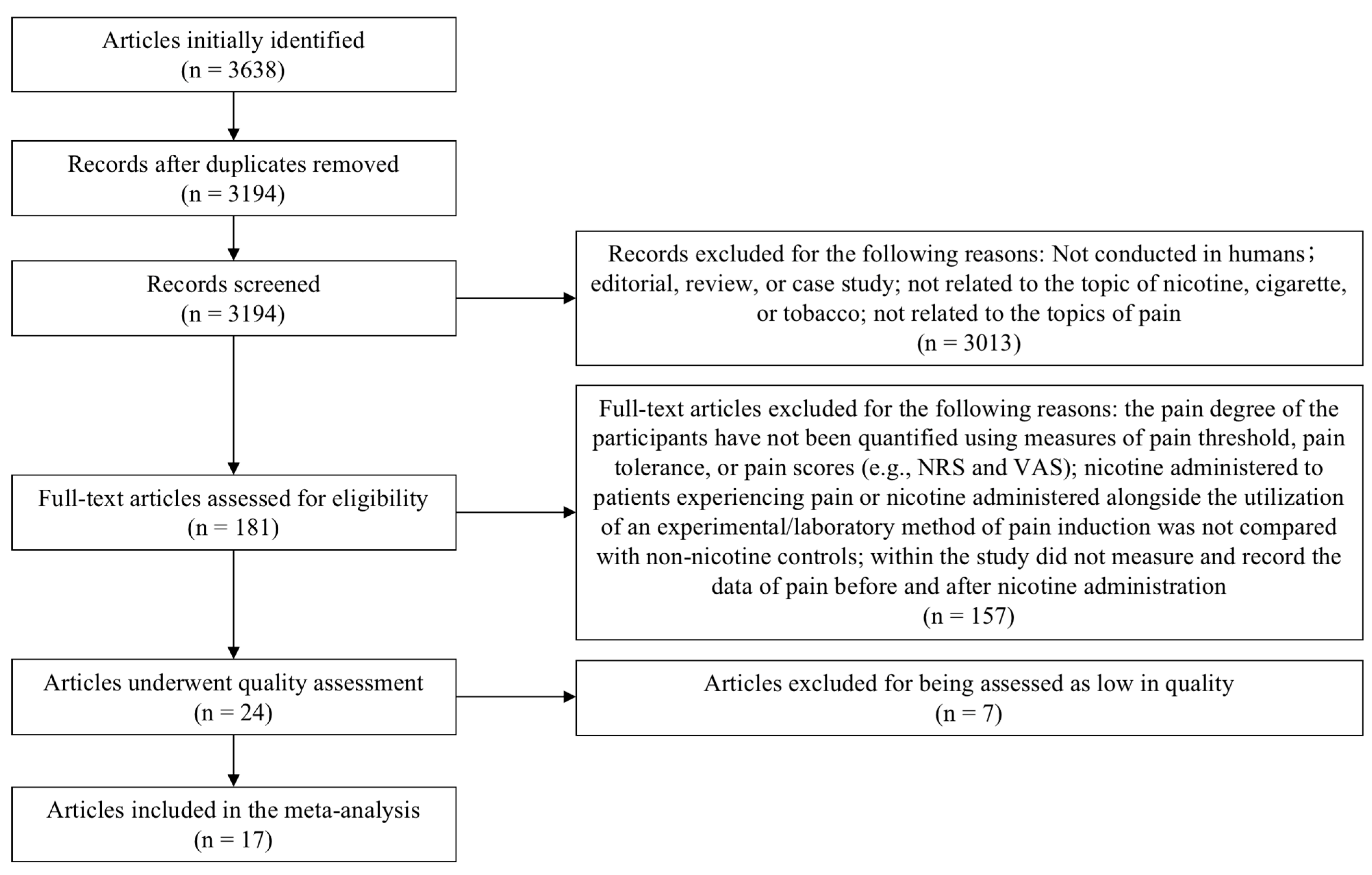
3.1. Study Selection and Characteristics of the Study Samples
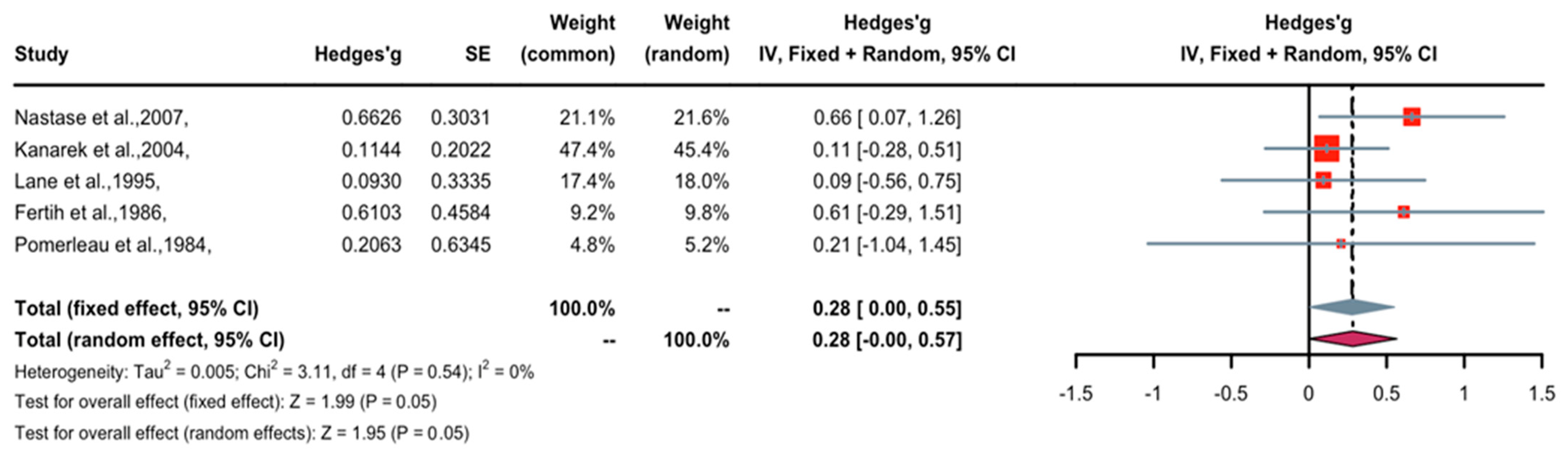
3.2. Effect of Nicotine on Pain Threshold
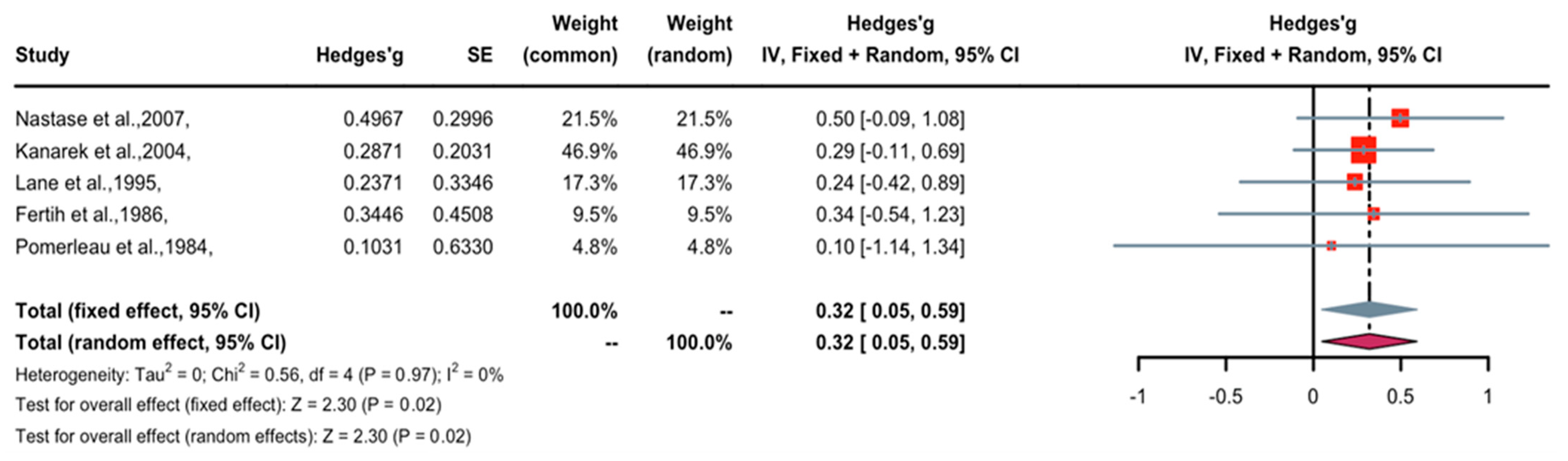
3.3. Effect of Nicotine on Pain Tolerance
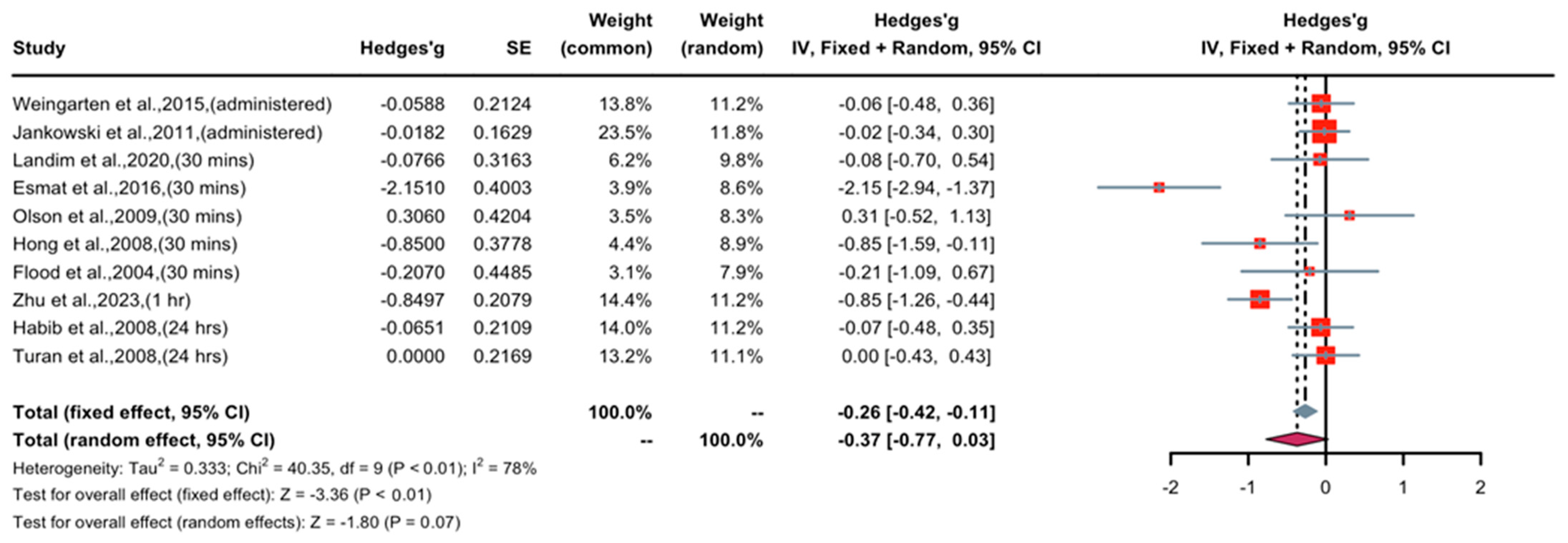
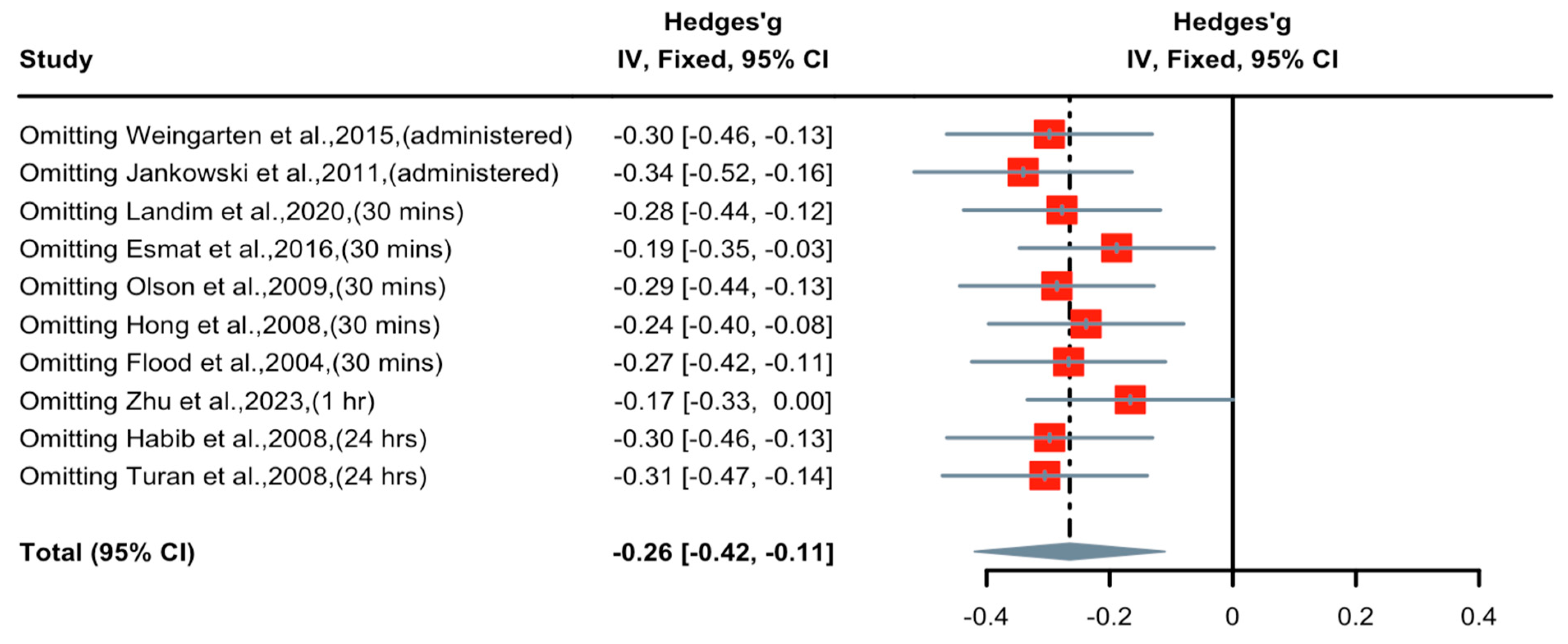
3.4. Effect of Short-Term Nicotine Application in Patients with Postoperative Pain
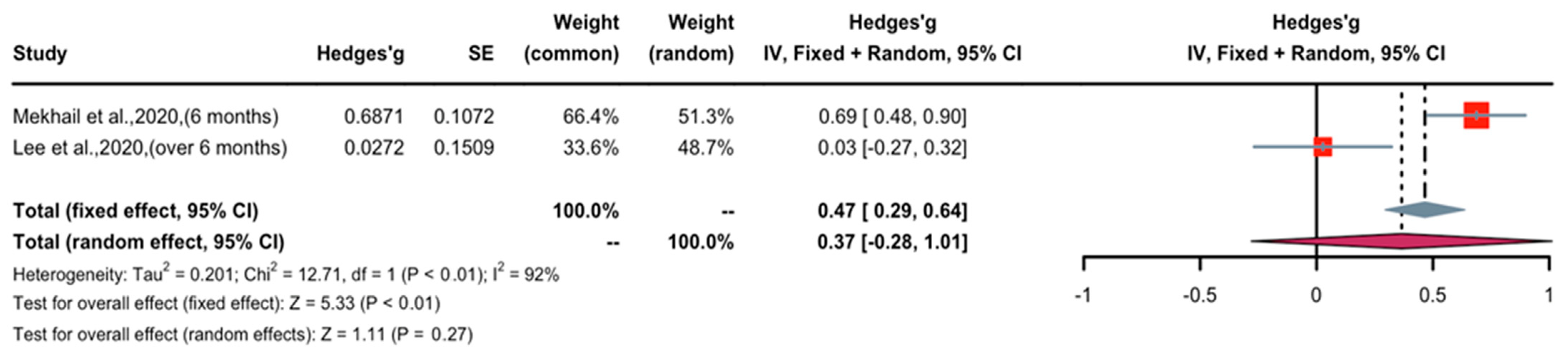
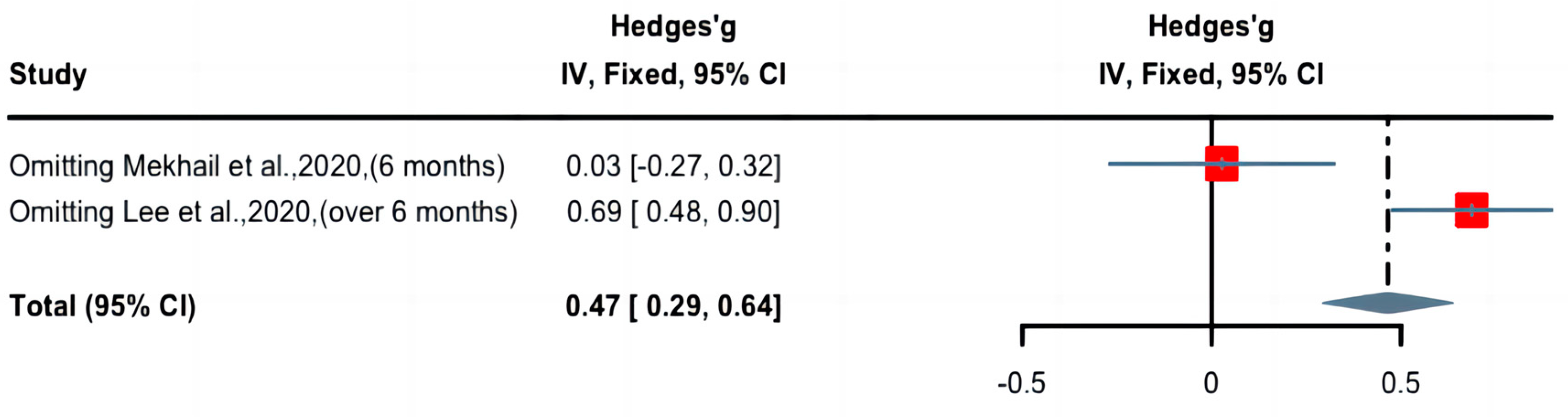
3.5. Effect of Long-Term Nicotine Application in Patients with Chronic Pain
4. Discussion and Conclusions
4.1. Summary
4.2. Potential Mechanisms of Acute Nicotine-Induced Antinociception and Long-Term Hyperalgesia
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Study Protocol Registration
References
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [PubMed]
- Phan, D.V.; Dóda, M.; Bite, A.; György, L. Antinociceptive activity of nicotine. Acta Physiol. Acad. Sci. Hung. 1973, 44, 85–93. [Google Scholar] [PubMed]
- Kishioka, S.; Kiguchi, N.; Kobayashi, Y.; Saika, F. Nicotine effects and the endogenous opioid system. J. Pharmacol. Sci. 2014, 125, 117–124. [Google Scholar] [CrossRef]
- Rowley, T.J.; Payappilly, J.; Lu, J.; Flood, P. The antinociceptive response to nicotinic agonists in a mouse model of postoperative pain. Anesth. Analg. 2008, 107, 1052–1057. [Google Scholar] [CrossRef]
- Yamamoto, A.; Kiguchi, N.; Kobayashi, Y.; Maeda, T.; Ueno, K.; Yamamoto, C.; Kishioka, S. Pharmacological relationship between nicotinic and opioid systems in analgesia and corticosterone elevation. Life Sci. 2011, 89, 956–961. [Google Scholar] [CrossRef]
- Umana, I.C.; Daniele, C.A.; Miller, B.A.; Abburi, C.; Gallagher, K.; Brown, M.A.; Mason, P.; McGehee, D.S. Nicotinic modulation of descending pain control circuitry. Pain 2017, 158, 1938–1950. [Google Scholar] [CrossRef]
- Flood, P.; Daniel, D. Intranasal nicotine for postoperative pain treatment. Anesthesiology 2004, 101, 1417–1421. [Google Scholar] [CrossRef]
- Turan, A.; White, P.F.; Koyuncu, O.; Karamanliodlu, B.; Kaya, G.; Apfel, C.C. Transdermal nicotine patch failed to improve postoperative pain management. Anesth. Analg. 2008, 107, 1011–1017. [Google Scholar] [CrossRef]
- Nastase, A.; Ioan, S.; Braga, R.I.; Zagrean, L.; Moldovan, M. Coffee drinking enhances the analgesic effect of cigarette smoking. Neuroreport 2007, 18, 921–924. [Google Scholar] [CrossRef]
- Kanarek, R.B.; Carrington, C. Sucrose consumption enhances the analgesic effects of cigarette smoking in male and female smokers. Psychopharmacology 2004, 173, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Lane, J.D.; Lefebvre, J.C.; Rose, J.E.; Keefe, F.J. Effects of cigarette smoking on perception of thermal pain. Exp. Clin. Psychopharmacol. 1995, 3, 140–147. [Google Scholar] [CrossRef]
- Fertig, J.B.; Pomerleau, O.F.; Sanders, B. Nicotine-produced antinociception in minimally deprived smokers and ex-smokers. Addict. Behav. 1986, 11, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Pomerleau, O.F.; Turk, D.C.; Fertig, J.B. The effects of cigarette smoking on pain and anxiety. Addict. Behav. 1984, 9, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Esmat, I.M.; Kassim, D.Y. Comparative study between transdermal nicotine and melatonin patches on postoperative pain relief after laparoscopic cholecystectomy, a double-blind, placebo-controlled trial. Egypt. J. Anaesth. 2016, 32, 299–307. [Google Scholar] [CrossRef]
- Hong, D.; Conell-Price, J.; Cheng, S.; Flood, P. Transdermal nicotine patch for postoperative pain management: A pilot dose-ranging study. Anesth. Analg. 2008, 107, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Landim, F.S.; Laureano Filho, J.R.; Nascimento, J.; do Egito Vasconcelos, B.C. Effectiveness of nicotine patch for the control of pain, oedema, and trismus following third molar surgery: A randomized clinical trial. Int. J. Oral. Maxillofac. Surg. 2020, 49, 1508–1517. [Google Scholar] [CrossRef]
- Weingarten, T.N.; McGlinch, B.P.; Liedl, L.; Kendrick, M.L.; Kellogg, T.A.; Schroeder, D.R.; Sprung, J. Intranasal nicotine increases postoperative nausea and is ineffective in reducing pain following laparoscopic bariatric surgery in tobacco-Naïve females: A randomized, double blind trial. Obes. Surg. 2015, 25, 506–513. [Google Scholar] [CrossRef]
- Jankowski, C.J.; Weingarten, T.N.; Martin, D.P.; Whalen, F.X.; Gebhart, J.B.; Liedl, L.M.; Danielson, D.R.; Nadeau, A.M.; Schroeder, D.R.; Warner, D.O.; et al. Randomised trial of intranasal nicotine and postoperative pain, nausea and vomiting in non-smoking women. Eur. J. Anaesthesiol. 2011, 28, 585–591. [Google Scholar] [CrossRef]
- Habib, A.S.; White, W.D.; El Gasim, M.A.; Saleh, G.; Polascik, T.J.; Moul, J.W.; Gan, T.J. Transdermal nicotine for analgesia after radical retropubic prostatectomy. Anesth. Analg. 2008, 107, 999–1004. [Google Scholar] [CrossRef]
- Olson, L.C.; Hong, D.; Conell-Price, J.S.; Cheng, S.; Flood, P. A transdermal nicotine patch is not effective for postoperative pain management in smokers: A pilot dose-ranging study. Anesth. Analg. 2009, 109, 1987–1991. [Google Scholar] [CrossRef] [PubMed]
- Mekhail, N.; Costandi, S.; Mehanny, D.S.; Armanyous, S.; Saied, O.; Taco-Vasquez, E.; Saweris, Y. The Impact of Tobacco Smoking on Spinal Cord Stimulation Effectiveness in Complex Regional Pain Syndrome Patients. Neuromodulation 2020, 23, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J. Correlations among pain, depressive symptoms, constipation, and serotonin levels in smokers and non smokers. Perspect. Psychiatr. Care 2020, 56, 864–870. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Zhu, C.; Bi, Y.; Wei, K.; Tao, K.; Hu, L.; Lu, Z. Effect of perioperative high-dose transdermal nicotine patch on pain sensitivity among male abstinent tobacco smokers undergoing abdominal surgery: A randomized controlled pilot study. Addiction 2023, 118, 1579–1585. [Google Scholar] [CrossRef]
- Iida, H.; Yamaguchi, S.; Goyagi, T.; Sugiyama, Y.; Taniguchi, C.; Matsubara, T.; Yamada, N.; Yonekura, H.; Iida, M. Consensus statement on smoking cessation in patients with pain. J. Anesth. 2022, 36, 671–687. [Google Scholar] [CrossRef] [PubMed]
- Seyedsadeghi, M.; Arabzadeh, A.; Entezariasl, M.; Shahbazzadegan, B.; Dindar, S.; Isazadehfar, K. The Effect of Nicotine Patch on Reducing Nausea, Vomiting, and Pain Following Laparoscopic Cholecystectomy: A Randomized Clinical Trial. Addict. Health 2023, 15, 39–44. [Google Scholar] [CrossRef]
- da Silva Barbirato, D.; de Melo Vasconcelos, A.F.; Dantas de Moraes, S.L.; Pellizzer, E.P.; do Egito Vasconcelos, B.C. Analgesic potential of transdermal nicotine patch in surgery: A systematic review and meta-analysis of randomised placebo-controlled trials. Eur. J. Clin. Pharmacol. 2023, 79, 589–607. [Google Scholar] [CrossRef]
- Dreyer, F. Acetylcholine receptor. Br. J. Anaesth. 1982, 54, 115–130. [Google Scholar] [CrossRef][Green Version]
- Hurst, R.; Rollema, H.; Bertrand, D. Nicotinic acetylcholine receptors: From basic science to therapeutics. Pharmacol. Ther. 2013, 137, 22–54. [Google Scholar] [CrossRef]
- Zoli, M.; Pucci, S.; Vilella, A.; Gotti, C. Neuronal and Extraneuronal Nicotinic Acetylcholine Receptors. Curr. Neuropharmacol. 2018, 16, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Brody, A.L.; Mandelkern, M.A.; London, E.D.; Olmstead, R.E.; Farahi, J.; Scheibal, D.; Jou, J.; Allen, V.; Tiongson, E.; Chefer, S.I.; et al. Cigarette smoking saturates brain alpha 4 beta 2 nicotinic acetylcholine receptors. Arch. Gen. Psychiatry 2006, 63, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Rose, J.E.; Behm, F.M.; Westman, E.C.; Coleman, R.E. Arterial nicotine kinetics during cigarette smoking and intravenous nicotine administration: Implications for addiction. Drug Alcohol Depend. 1999, 56, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Dani, J.A.; Radcliffe, K.A.; Pidoplichko, V.I. Variations in desensitization of nicotinic acetylcholine receptors from hippocampus and midbrain dopamine areas. Eur. J. Pharmacol. 2000, 393, 31–38. [Google Scholar] [CrossRef]
- Mansvelder, H.D.; McGehee, D.S. Long-term potentiation of excitatory inputs to brain reward areas by nicotine. Neuron 2000, 27, 349–357. [Google Scholar] [CrossRef]
- Zhang, T.; Zhang, L.; Liang, Y.; Siapas, A.G.; Zhou, F.M.; Dani, J.A. Dopamine signaling differences in the nucleus accumbens and dorsal striatum exploited by nicotine. J. Neurosci. 2009, 29, 4035–4043. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Intervention | Pain | Measures | Design | Sample (T/C) | Quality Assessment (RoB2) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I1 | I2 | I3 | I4 | I5 | Total | |||||||
| Zhu et al. [26] | 2023 | patch | surgery | NRS score | between | 50/51 | 1 | 1 | 1 | 1 | 1 | 5 |
| Landim et al. [17] | 2020 | patch | surgery | VAS score | between | 20/20 | 1 | 1 | 1 | 1 | 1 | 5 |
| Esmat et al. [15] | 2016 | patch | surgery | VAS score | between | 20/20 | 1 | 1 | 0 | 1 | 1 | 4 |
| Weingarten et al. [18] | 2015 | nasal spray | surgery | NRS score | between | 42/47 | 1 | 1 | 1 | 1 | 1 | 5 |
| Jankowski et al. [19] | 2011 | nasal spray | surgery | NRS score | between | 72/79 | 1 | 1 | 1 | 1 | 1 | 5 |
| Turan et al. [9] | 2008 | patch | surgery | VRS score | between | 43/42 | 1 | 1 | 0 | 1 | 1 | 4 |
| Hong et al. [16] | 2008 | patch | surgery | NRS score | between | 30/10 | 1 | 1 | 0 | 1 | 1 | 4 |
| Habib et al. [20] | 2008 | patch | surgery | VAS score | between | 44/46 | 1 | 1 | 1 | 1 | 1 | 5 |
| Flood et al. [8] | 2004 | nasal spray | surgery | NRS score | between | 10/10 | 1 | 1 | 0 | 1 | 1 | 4 |
| Mekhail et al. [22] | 2020 | tobacco | CRPS | NRS score | between | 177/192 | 1 | 1 | 1 | 1 | 1 | 5 |
| Lee et al. [23] | 2020 | tobacco | chronic | NRS score | between | 164/60 | 1 | 0 | 1 | 1 | 1 | 4 |
| Nastase et al. [10] | 2007 | tobacco | thermal | PTH and PTO | within | 23/23 | 1 | 1 | 1 | 1 | 1 | 5 |
| Kanarek et al. [11] | 2004 | tobacco | thermal | PTH and PTO | within | 49/49 | 1 | 1 | 1 | 1 | 1 | 5 |
| Lane et al. [12] | 1995 | tobacco | thermal | PTH and PTO | within | 18/18 | 1 | 1 | 1 | 1 | 1 | 5 |
| Fertig et al. [13] | 1986 | tobacco | thermal | PTH and PTO | within | 10/10 | 1 | 1 | 0 | 1 | 1 | 4 |
| Pomerleau et al. [14] | 1984 | tobacco | thermal | PTH and PTO | within | 5/5 | 1 | 1 | 0 | 1 | 1 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, Y.; Yang, Y.; Schneider, C.; Balle, T. The Anti-Nociceptive Effects of Nicotine in Humans: A Systematic Review and Meta-Analysis. Pharmaceuticals 2023, 16, 1665. https://doi.org/10.3390/ph16121665
Luo Y, Yang Y, Schneider C, Balle T. The Anti-Nociceptive Effects of Nicotine in Humans: A Systematic Review and Meta-Analysis. Pharmaceuticals. 2023; 16(12):1665. https://doi.org/10.3390/ph16121665
Chicago/Turabian StyleLuo, Yujia, Yating Yang, Carl Schneider, and Thomas Balle. 2023. "The Anti-Nociceptive Effects of Nicotine in Humans: A Systematic Review and Meta-Analysis" Pharmaceuticals 16, no. 12: 1665. https://doi.org/10.3390/ph16121665
APA StyleLuo, Y., Yang, Y., Schneider, C., & Balle, T. (2023). The Anti-Nociceptive Effects of Nicotine in Humans: A Systematic Review and Meta-Analysis. Pharmaceuticals, 16(12), 1665. https://doi.org/10.3390/ph16121665