


The Development of Dermal Self-Double-Emulsifying Drug Delivery Systems: Preformulation Studies as the Keys to Success




Abstract
:
1. Introduction
2. Results and Discussion
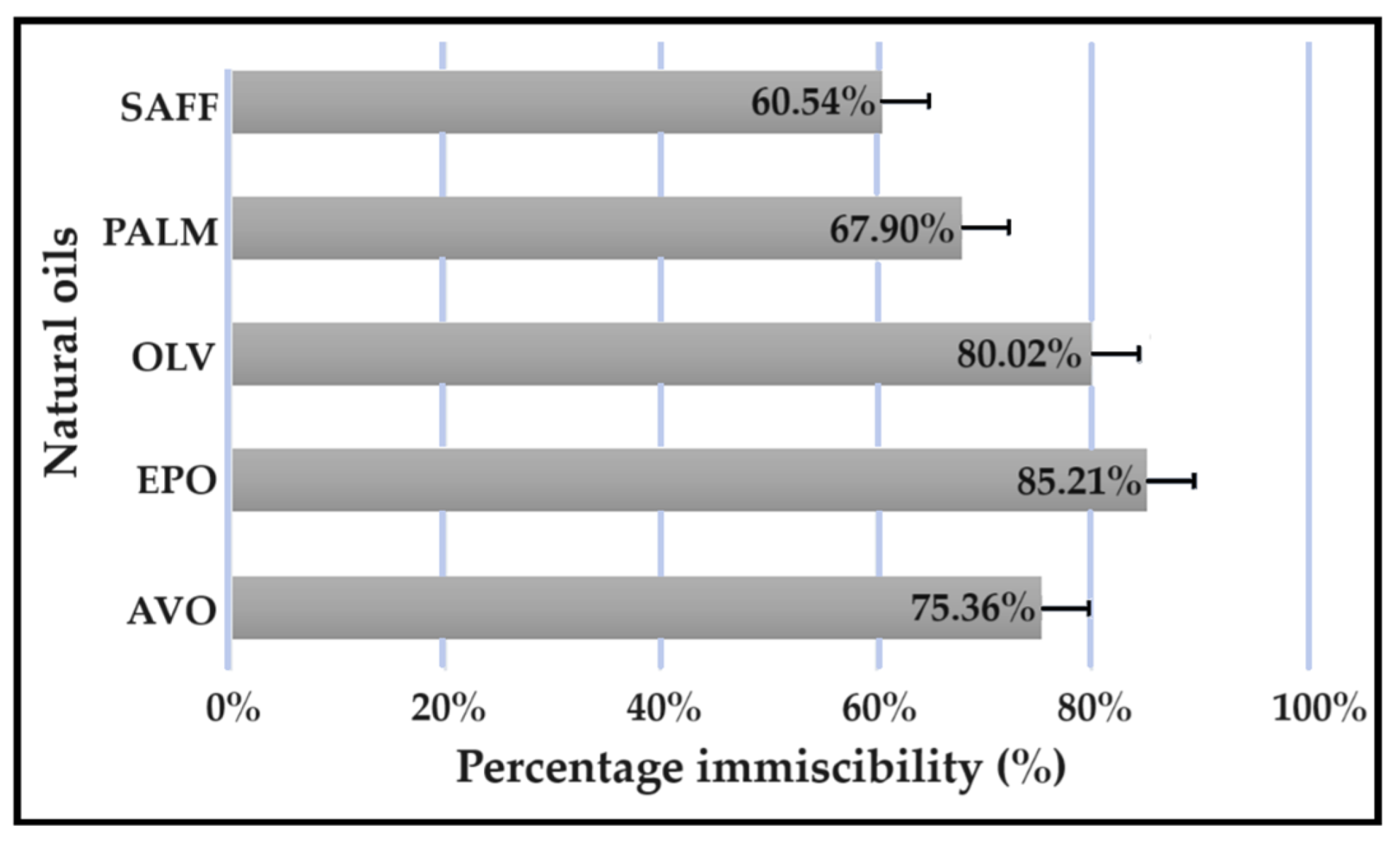
2.1. Oil Immiscibility Studies
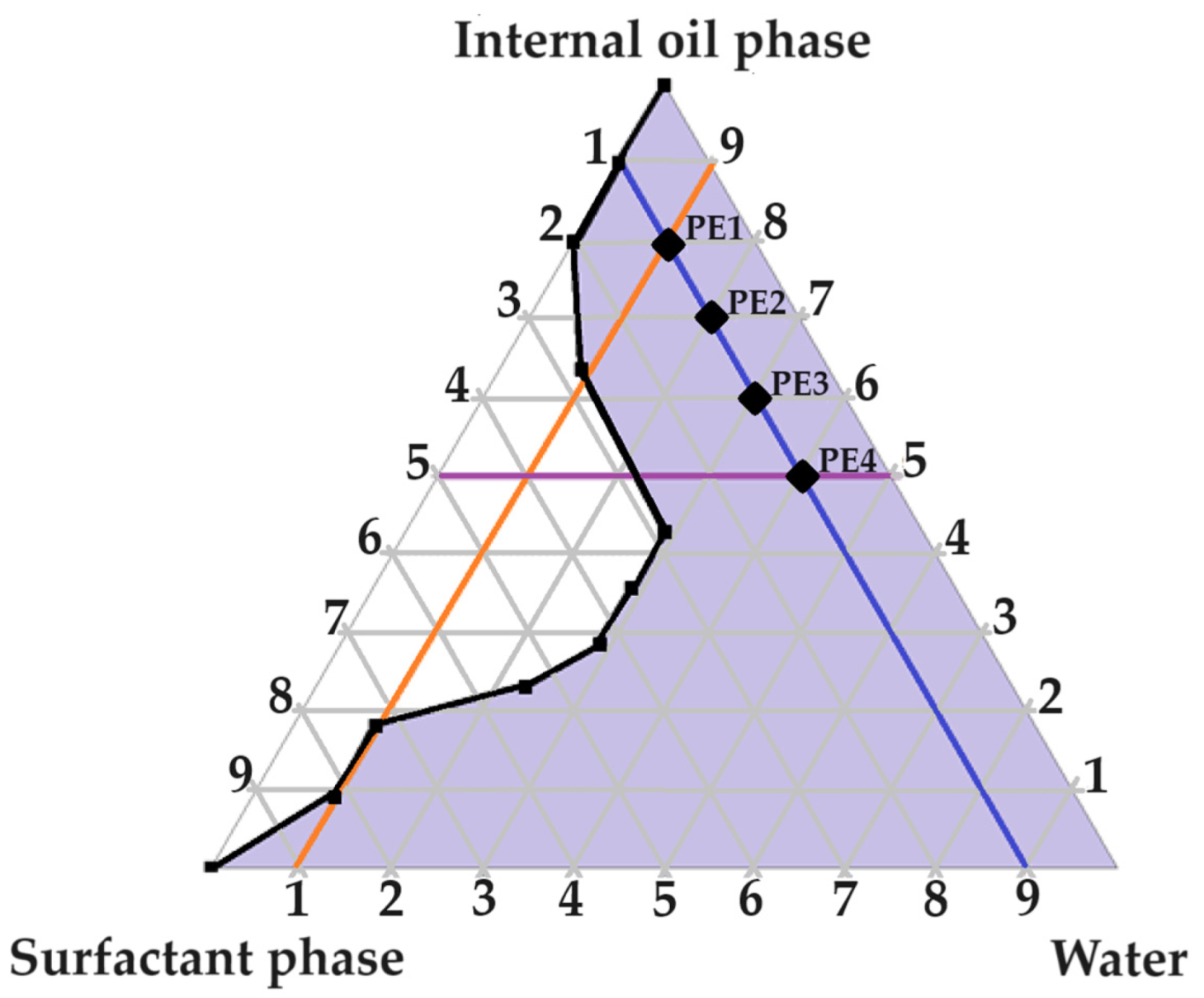
2.2. Evaluation of the Pseudoternary Phase Diagram to Find Potential Primary Emulsions
2.3. Evaluation of Primary Emulsions
2.3.1. Self-Emulsification Performance
2.3.2. Emulsion Stability Index
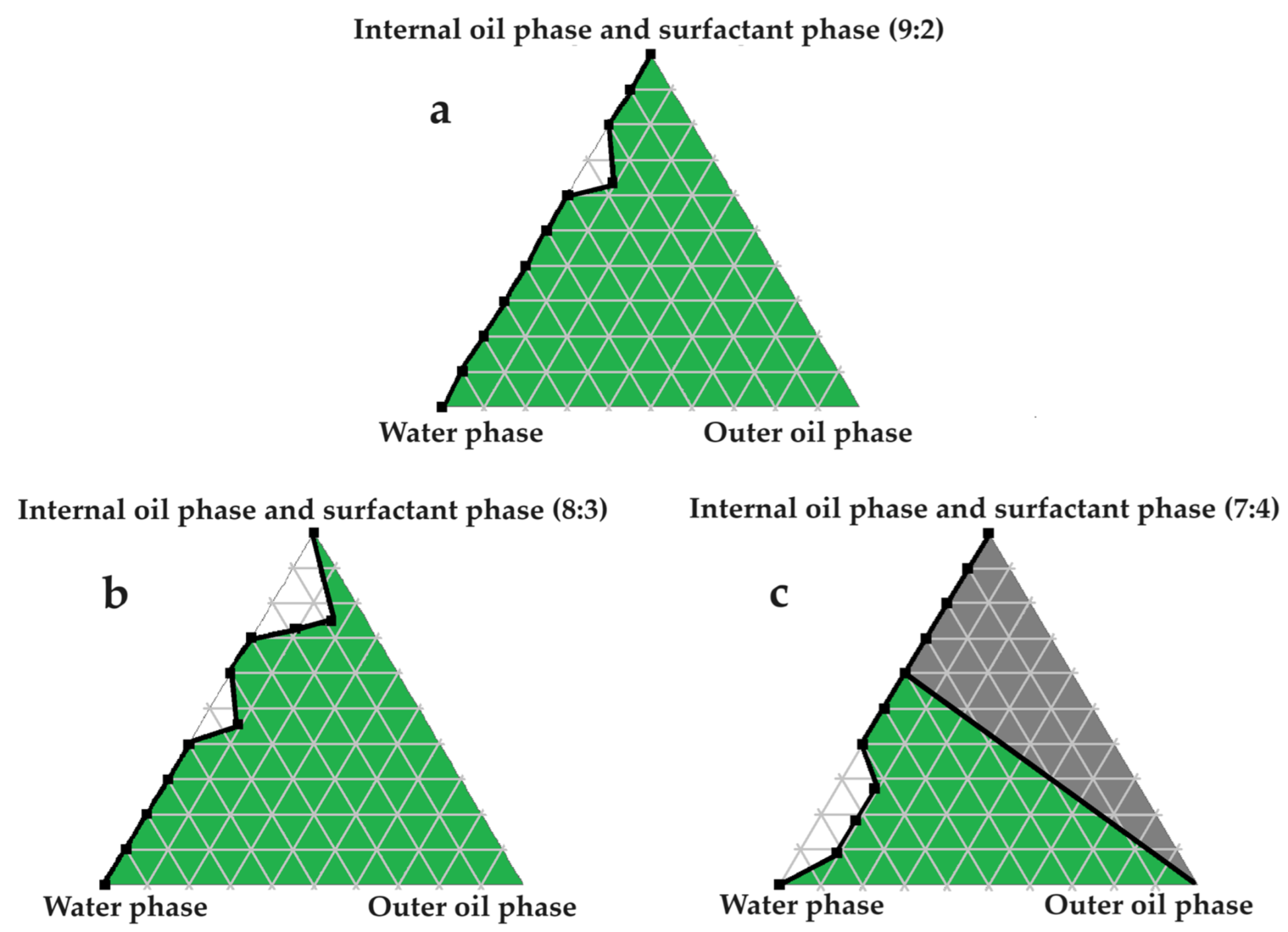
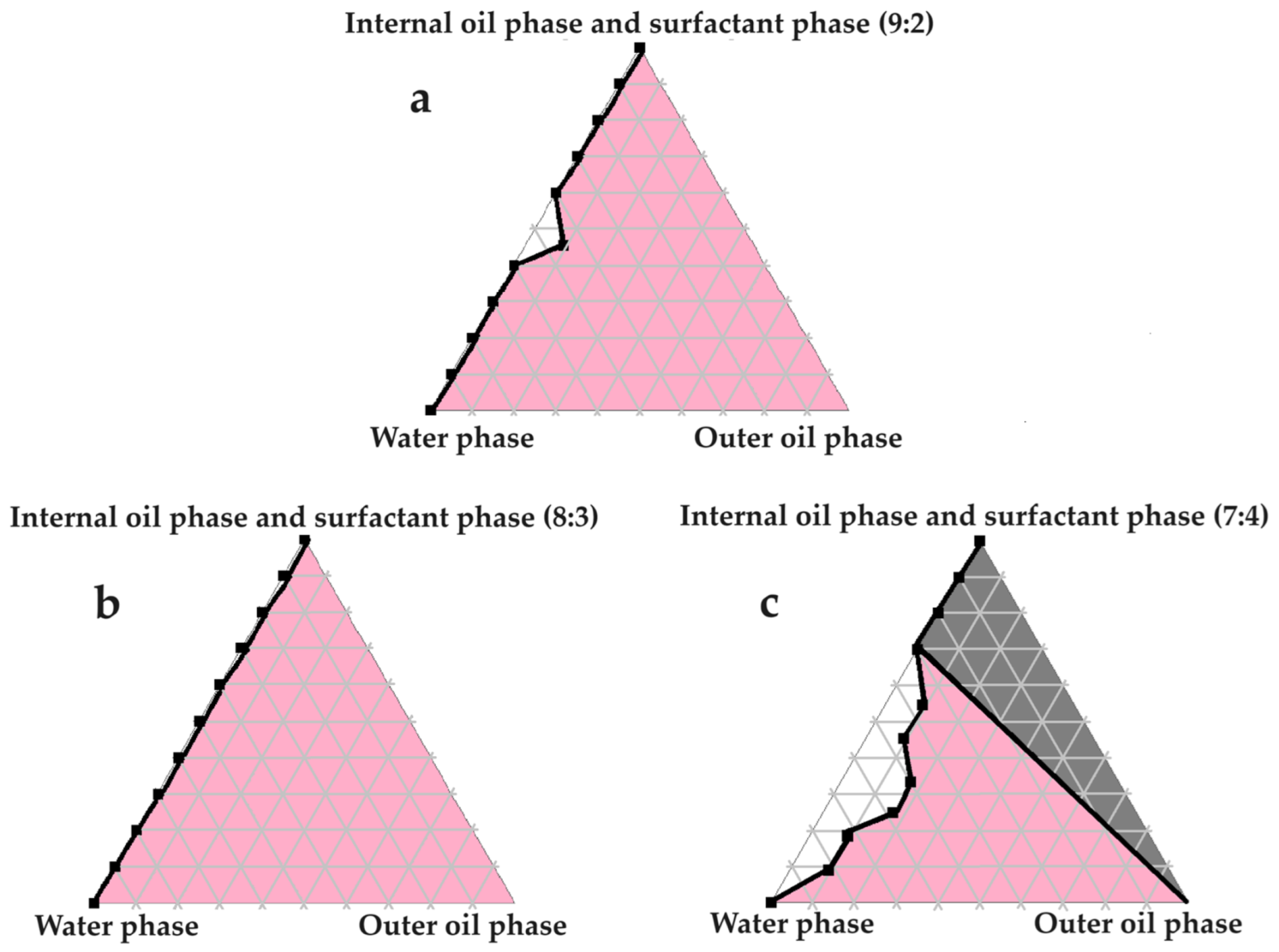
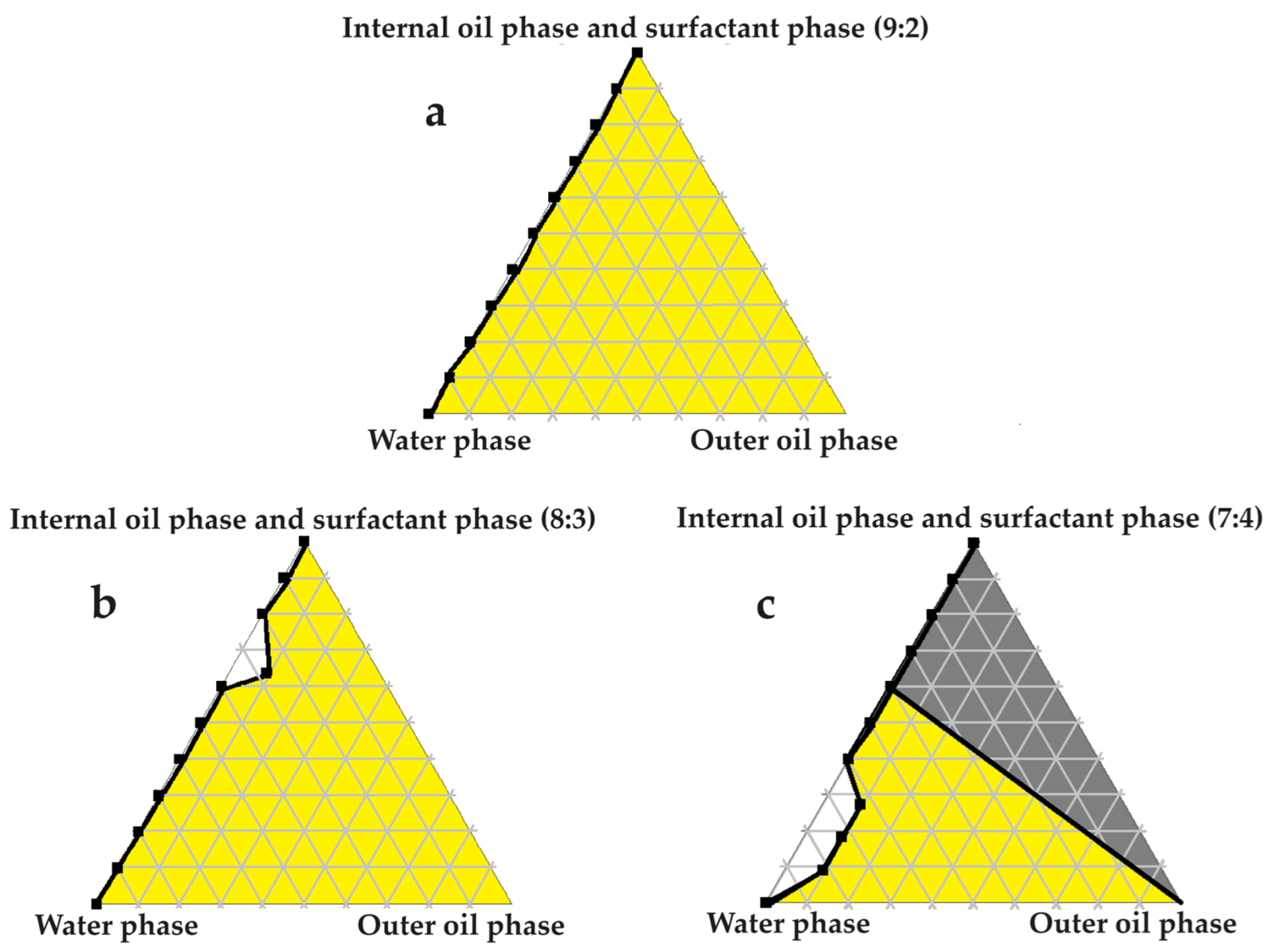
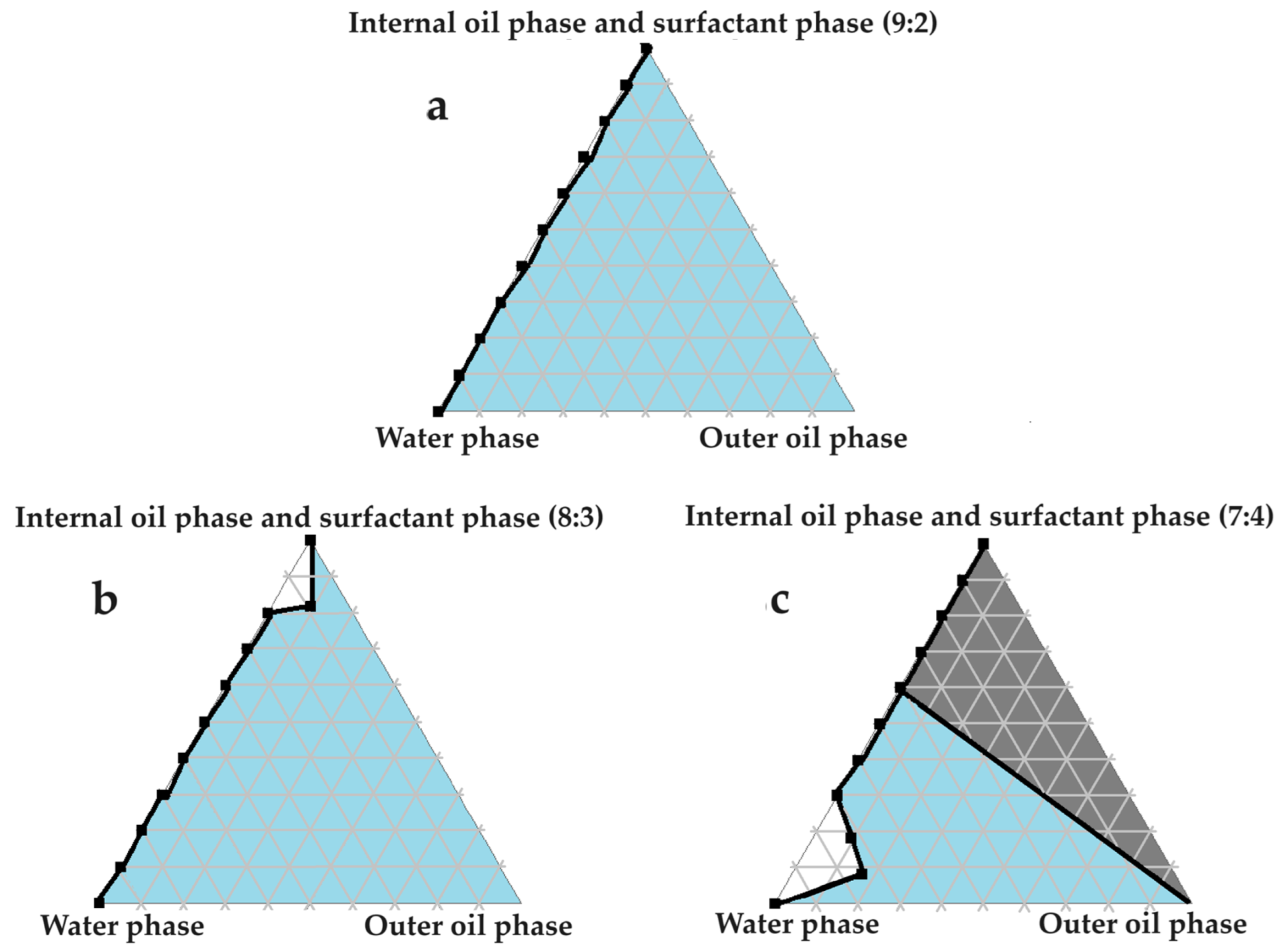
2.4. Construction of Pseudoternary Phase Diagrams for Self-Double-Emulsifying Drug Delivery Systems
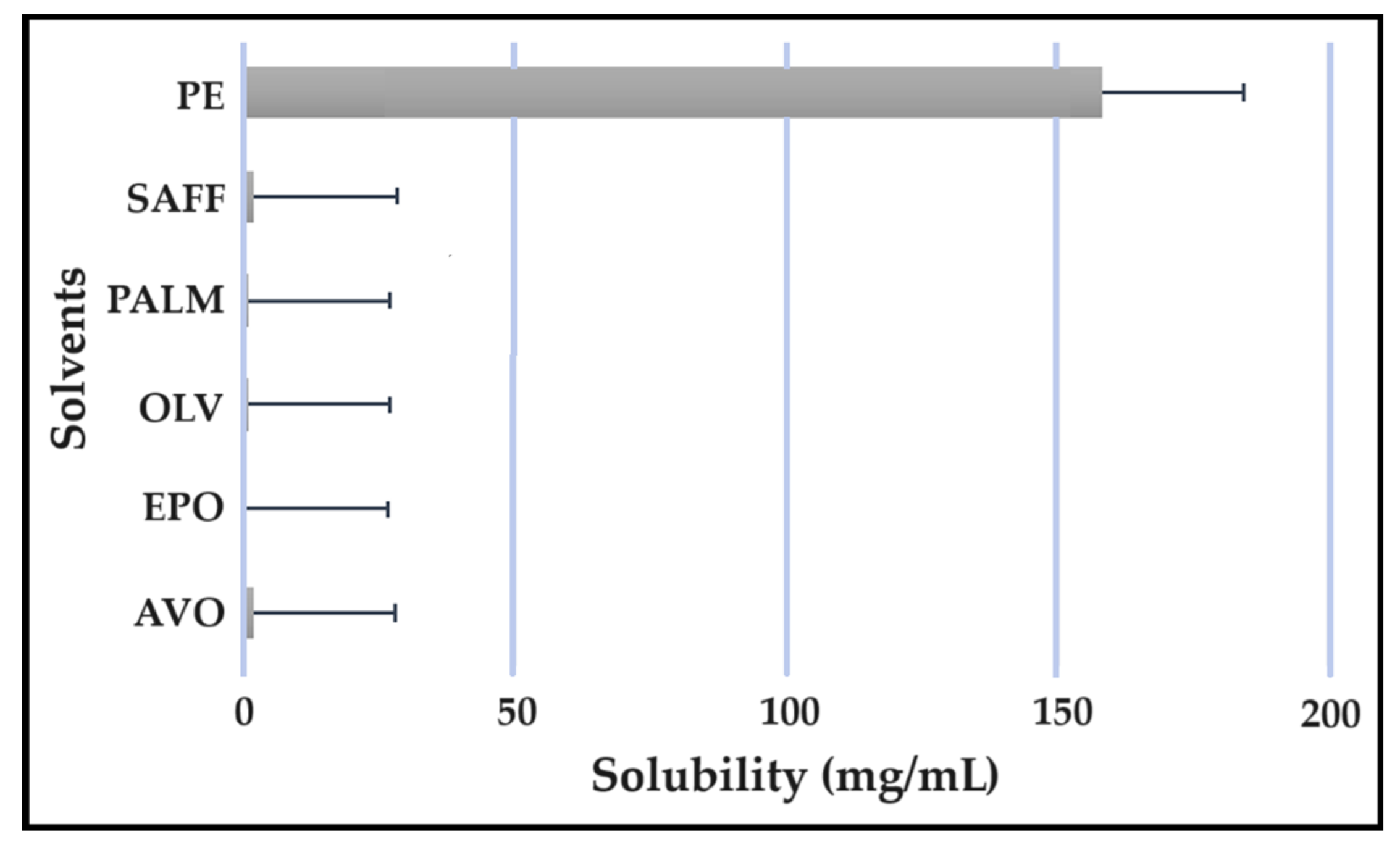
2.5. Solubility Studies
2.6. Isothermal Micro Calorimetry Compatibility Studies
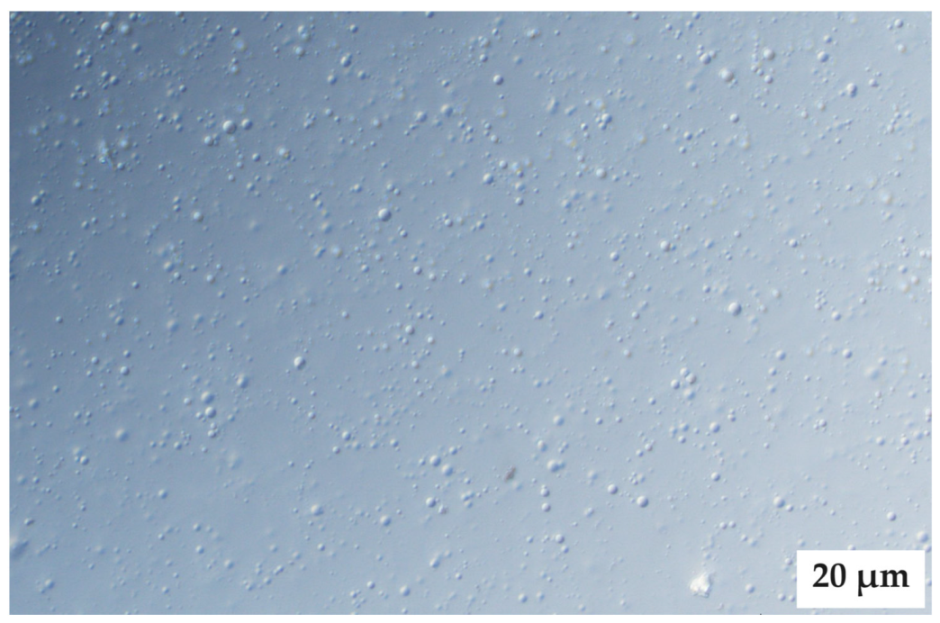
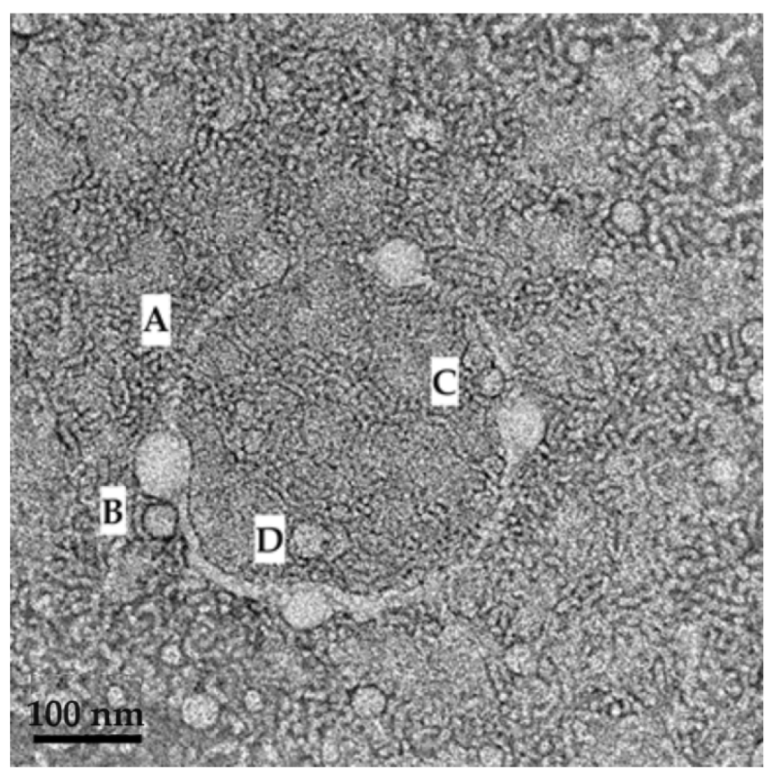
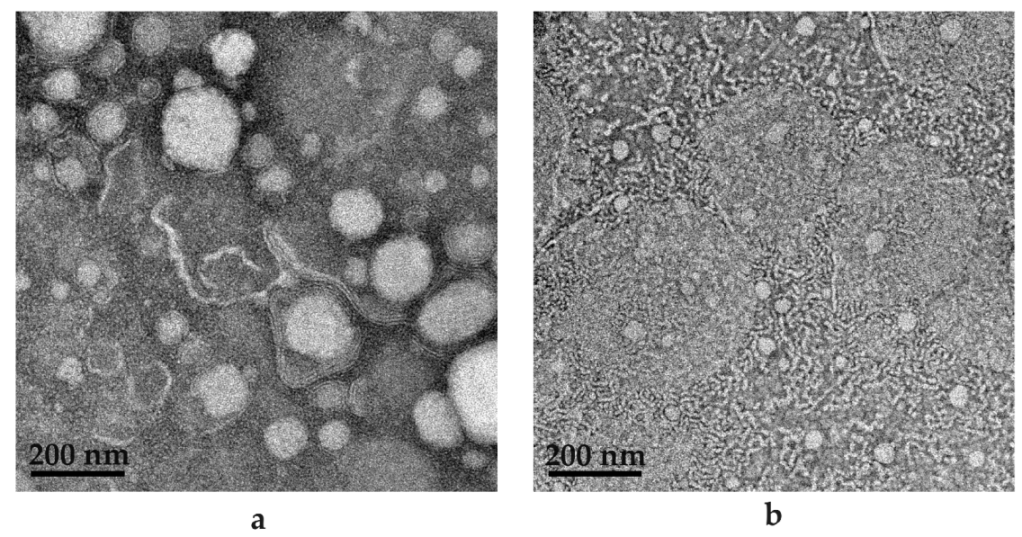
2.7. Microscope Examination
3. Materials and Methods
3.1. Materials
3.2. Methods for Drug and Excipient Selection
Considering Drug Selection
3.3. Preformulation Studies
3.3.1. Oil Immiscibility Studies
3.3.2. Hydrophilic–Lipophilic Balance Consideration
3.3.3. Construction of a Pseudoternary Phase Diagram to Find Potential Primary Emulsions
3.3.4. Evaluation of Primary Emulsions
3.3.5. Self-Emulsification Performance
- Grade A: Fast-forming emulsion (within 1 min) with a clear or bluish color;
- Grade B: Fast-forming (within 1 min) and somewhat less clear emulsion with a bluish-white color;
- Grade C: Fine murky emulsion that forms within 2 min;
- Grade D: Dull, grayish-white emulsion that displays a slightly oily appearance, which indicates slow emulsification (longer than 2 min);
- Grade E: A formulation demonstrating either poor or minimal emulsification with large oil droplets existing on the surface.
3.3.6. Emulsion Stability Index (ESI)
3.3.7. Construction of Pseudoternary Phase Diagrams for Self-Double-Emulsifying Drug Delivery Systems
3.3.8. Solubility Studies
3.3.9. Isothermal Micro Calorimetry Compatibility Studies
3.3.10. Microscope Examination
3.3.11. Droplet Size and Size Distribution
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- AboulFotouh, K.; Allam, A.A.; El-Badry, M.; El-Sayed, A.M. Role of Self-Emulsifying Drug Delivery Systems in Optimizing the Oral Delivery of Hydrophilic Macromolecules and Reducing Interindividual Variability. Colloids Surf. B Biointerfaces 2018, 167, 82–92. [Google Scholar] [CrossRef]
- Hu, C.; Wang, Q.; Ma, C.; Xia, Q. Non-Aqueous Self-Double-Emulsifying Drug Delivery System: A New Approach to Enhance Resveratrol Solubility for Effective Transdermal Delivery. Colloids Surf. A Physicochem. Eng. Asp. 2016, 489, 360–369. [Google Scholar] [CrossRef]
- Echeverry, S.M.; Rey, D.; Valderrama, I.H.; de Araujo, B.V.; Aragón, D.M. Development of a Self-Emulsifying Drug Delivery System (SEDDS) to Improve the Hypoglycemic Activity of Passiflora Ligularis Leaves Extract. J. Drug Deliv. Sci. Technol. 2021, 64, 102604. [Google Scholar] [CrossRef]
- Van Staden, D.; du Plessis, J.; Viljoen, J. Development of Topical/Transdermal Self-Emulsifying Drug Delivery Systems, Not as Simple as Expected. Sci. Pharm. 2020, 88, 17. [Google Scholar] [CrossRef]
- Lam, H.T.; Le, N.M.N.; Phan, T.N.Q.; Bernkop-Schnürch, A. Mucolytic Self-Emulsifying Drug Delivery Systems (SEDDS) Containing a Hydrophobic Ion-Pair of Proteinase. Eur. J. Pharm. Sci. 2021, 162, 105658. [Google Scholar] [CrossRef]
- Van Staden, D.; du Plessis, J.; Viljoen, J. Development of a Self-Emulsifying Drug Delivery System for Optimized Topical Delivery of Clofazimine. Pharmaceutics 2020, 12, 523. [Google Scholar] [CrossRef]
- Efiana, N.A.; Phan, T.N.Q.; Wicaksono, A.J.; Bernkop-Schnürch, A. Mucus Permeating Self-Emulsifying Drug Delivery Systems (SEDDS): About the Impact of Mucolytic Enzymes. Colloids Surf. B Biointerfaces 2018, 161, 228–235. [Google Scholar] [CrossRef]
- Moshikur, R.M.; Ali, M.K.; Moniruzzaman, M.; Goto, M. Recent Advances in Surface-Active Ionic Liquid-Assisted Self-Assembly Systems for Drug Delivery. Curr. Opin. Colloid Interface Sci. 2021, 56, 101515. [Google Scholar] [CrossRef]
- Cholakova, D.; Vinarov, Z.; Tcholakova, S.; Denkov, N.D. Self-Emulsification in Chemical and Pharmaceutical Technologies. Curr. Opin. Colloid Interface Sci. 2022, 59, 101576. [Google Scholar] [CrossRef]
- Callender, S.P.; Mathews, J.A.; Kobernyk, K.; Wettig, S.D. Microemulsion Utility in Pharmaceuticals: Implications for Multi-Drug Delivery. Int. J. Pharm. 2017, 526, 425–442. [Google Scholar] [CrossRef]
- Van Staden, D.; Haynes, R.K.; Viljoen, J.M. The Science of Selecting Excipients for Dermal Self-Emulsifying Drug Delivery Systems. Pharmaceutics 2023, 15, 1293. [Google Scholar] [CrossRef]
- Osborne, D.W.; Musakhanian, J. Skin Penetration and Permeation Properties of Transcutol®—Neat or Diluted Mixtures. AAPS PharmSciTech 2018, 19, 3512–3533. [Google Scholar] [CrossRef]
- Dragicevic, N.; Maibach, H.I. (Eds.) Percutaneous Penetration Enhancers Chemical Methods in Penetration Enhancement; Springer: Berlin/Heidelberg, Germany, 2015; ISBN 978-3-662-47038-1. [Google Scholar]
- Nasr, A.; Gardouh, A.; Ghorab, M. Novel Solid Self-Nanoemulsifying Drug Delivery System (S-SNEDDS) for Oral Delivery of Olmesartan Medoxomil: Design, Formulation, Pharmacokinetic and Bioavailability Evaluation. Pharmaceutics 2016, 8, 20. [Google Scholar] [CrossRef]
- Wang, Q.; Sun, R.; Huang, J.; Xia, Q. Development and Characterization of a New Non-Aqueous Self-Double-Emulsifying Drug Delivery System for Topical Application of Rutin. J. Drug Deliv. Sci. Technol. 2021, 61, 101243. [Google Scholar] [CrossRef]
- Sarheed, O.; Dibi, M.; Ramesh, K.V.R.N.S. Studies on the Effect of Oil and Surfactant on the Formation of Alginate-Based O/W Lidocaine Nanocarriers Using Nanoemulsion Template. Pharmaceutics 2020, 12, 1223. [Google Scholar] [CrossRef]
- Zhang, J.; Ge, D.; Wang, X.; Wang, W.; Cui, D.; Yuan, G.; Wang, K.; Zhang, W. Influence of Surfactant and Weak-Alkali Concentrations on the Stability of O/W Emulsion in an Alkali-Surfactant-Polymer Compound System. ACS Omega 2021, 6, 5001–5008. [Google Scholar] [CrossRef]
- Hosny, K.M.; Alhakamy, N.A.; Al Nahyah, K.S. The Relevance of Nanotechnology, Hepato-Protective Agents in Reducing the Toxicity and Augmenting the Bioavailability of Isotretinoin. Drug Deliv. 2021, 28, 123–133. [Google Scholar] [CrossRef]
- Van Staden, D.; Haynes, R.K.; Viljoen, J.M. Adapting Clofazimine for Treatment of Cutaneous Tuberculosis by Using Self-Double-Emulsifying Drug Delivery Systems. Antibiotics 2022, 11, 806. [Google Scholar] [CrossRef]
- Chaudhari, S.P.; Dugar, R.P. Application of Surfactants in Solid Dispersion Technology for Improving Solubility of Poorly Water Soluble Drugs. J. Drug Deliv. Sci. Technol. 2017, 41, 68–77. [Google Scholar] [CrossRef]
- Becker, C.; Dressman, J.B.; Amidon, G.L.; Junginger, H.E.; Kopp, S.; Midha, K.K.; Shah, V.P.; Stavchansky, S.; Barends, D.M. Biowaiver Monographs for Immediate Release Solid Oral Dosage Forms: Isoniazid. J. Pharm. Sci. 2007, 96, 522–531. [Google Scholar] [CrossRef]
- Henwood, S.Q.; De Villiers, M.M.; Liebenberg, W.; Lötter, A.P. Solubility and Dissolution Properties of Generic Rifampicin Raw Materials. Drug Dev. Ind. Pharm. 2000, 26, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.K.; Jindal, N. Formulation of Tyloxapol Niosomes for Encapsulation, Stabilization and Dissolution of Anti-Tubercular Drugs. Colloids Surf. B Biointerfaces 2013, 101, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Trousil, J.; Pavliš, O.; Kubíčková, P.; Škorič, M.; Marešová, V.; Pavlova, E.; Knudsen, K.D.; Dai, Y.S.; Zimmerman, M.; Dartois, V.; et al. Antitubercular Nanocarrier Monotherapy: Study of In Vivo Efficacy and Pharmacokinetics for Rifampicin. J. Control. Release 2020, 321, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Sutradhar, I.; Zaman, M.H. Evaluation of the Effect of Temperature on the Stability and Antimicrobial Activity of Rifampicin Quinone. J. Pharm. Biomed. Anal. 2021, 197, 113941. [Google Scholar] [CrossRef]
- Hussain, A.; Altamimi, M.A.; Alshehri, S.; Imam, S.S. Assessment of Solubility and Hansen Solubility Parameters of Rifampicin in Various Permeation Enhancers: Experimental and Computational Approach. J. Mol. Liq. 2021, 328, 115432. [Google Scholar] [CrossRef]
- Ammerman, N.C.; Swanson, R.V.; Bautista, E.M.; Almeida, D.V.; Saini, V.; Omansen, T.F.; Guo, H.; Chang, Y.S.; Li, S.Y.; Tapley, A.; et al. Impact of Clofazimine Dosing on Treatment Shortening of the First-Line Regimen in a Mouse Model of Tuberculosis. Antimicrob. Agents Chemother. 2018, 62, 1128. [Google Scholar] [CrossRef]
- Mashele, S.A.; Steel, H.C.; Matjokotja, M.T.; Rasehlo, S.S.M.; Anderson, R.; Cholo, M.C. Assessment of the Efficacy of Clofazimine Alone and in Combination with Primary Agents against Mycobacterium Tuberculosis in Vitro. J. Glob. Antimicrob. Resist. 2022, 29, 343–352. [Google Scholar] [CrossRef]
- Genina, N.; Boetker, J.P.; Colombo, S.; Harmankaya, N.; Rantanen, J.; Bohr, A. Anti-Tuberculosis Drug Combination for Controlled Oral Delivery Using 3D Printed Compartmental Dosage Forms: From Drug Product Design to in Vivo Testing. J. Control. Release 2017, 268, 40–48. [Google Scholar] [CrossRef]
- Pizzino, A.; Molinier, V.; Catté, M.; Ontiveros, J.F.; Salager, J.L.; Aubry, J.M. Relationship between Phase Behavior and Emulsion Inversion for a Well-Defined Surfactant (C10E4)/n-Octane/Water Ternary System at Different Temperatures and Water/Oil Ratios. Ind. Eng. Chem. Res. 2013, 52, 4527–4538. [Google Scholar] [CrossRef]
- Seguin, C.; Eastoe, J.; Heenan, R.K.; Grillo, I. Controlling Aggregation of Nonionic Surfactants Using Mixed Glycol Media. Langmuir 2007, 23, 4199–4202. [Google Scholar] [CrossRef]
- Villanueva-Martínez, A.; Merino, V.; Ganem-Rondero, A. Transdermal Formulations and Strategies for the Treatment of Osteoporosis. J. Drug Deliv. Sci. Technol. 2022, 69, 103111. [Google Scholar] [CrossRef]
- Nagarkar, R.; Singh, M.; Nguyen, H.X.; Jonnalagadda, S. A Review of Recent Advances in Microneedle Technology for Transdermal Drug Delivery. J. Drug Deliv. Sci. Technol. 2020, 59, 101923. [Google Scholar] [CrossRef]
- Chaturvedi, S.; Garg, A. An Insight of Techniques for the Assessment of Permeation Flux across the Skin for Optimization of Topical and Transdermal Drug Delivery Systems: “Modelling the Topical and Transdermal Drug Delivery Systems”. J. Drug Deliv. Sci. Technol. 2021, 62, 102355. [Google Scholar] [CrossRef]
- Gowda, B.H.J.; Ahmed, M.G.; Husain, A. Transferosomal in Situ Gel Administered through Umbilical Skin Tissues for Improved Systemic Bioavailability of Drugs: A Novel Strategy to Replace Conventional Transdermal Route. Med. Hypotheses 2022, 161, 110805. [Google Scholar] [CrossRef]
- Despotopoulou, D.; Lagopati, N.; Pispas, S.; Gazouli, M.; Demetzos, C.; Pippa, N. The Technology of Transdermal Delivery Nanosystems: From Design and Development to Preclinical Studies. Int. J. Pharm. 2022, 611, 121290. [Google Scholar] [CrossRef]
- Fernandes, G.F.S.; Thompson, A.M.; Castagnolo, D.; Denny, W.A.; Dos Santos, J.L. Tuberculosis Drug Discovery: Challenges and New Horizons. J. Med. Chem. 2022, 65, 7489–7531. [Google Scholar] [CrossRef]
- Warnken, Z.; Trementozzi, A.; Martins, P.P.; Parekh, J.; Koleng, J.J.; Smyth, H.D.C.; Brunaugh, A. Development of Low-Cost, Weight-Adjustable Clofazimine Mini-Tablets for Treatment of Tuberculosis in Pediatrics. Eur. J. Pharm. Sci. 2023, 187, 106470. [Google Scholar] [CrossRef]
- Wang, M.-G.; Liu, X.-M.; Wu, S.-Q.; He, J.-Q. Impacts of Clofazimine on the Treatment Outcomes of Drug-Resistant Tuberculosis. Microbes Infect. 2023, 25, 105020. [Google Scholar] [CrossRef]
- Dey, T.; Brigden, G.; Cox, H.; Shubber, Z.; Cooke, G.; Ford, N. Outcomes of Clofazimine for the Treatment of Drug-Resistant Tuberculosis: A Systematic Review and Meta-Analysis. J. Antimicrob. Chemother. 2013, 68, 284–293. [Google Scholar] [CrossRef]
- Ndjeka, N.; Schnippel, K.; Master, I.; Meintjes, G.; Maartens, G.; Romero, R.; Padanilam, X.; Enwerem, M.; Chotoo, S.; Singh, N.; et al. High Treatment Success Rate for Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis Using a Bedaquiline-Containing Treatment Regimen. Eur. Respir. J. 2018, 52, 1801528. [Google Scholar] [CrossRef]
- Du, Y.; Qiu, C.; Chen, X.; Wang, J.; Jing, W.; Pan, H.; Chen, W.; Liu, Y.; Li, C.; Xi, X.; et al. Treatment Outcome of a Shorter Regimen Containing Clofazimine for Multidrug-Resistant Tuberculosis: A Randomized Control Trial in China. Clin. Infect. Dis. 2020, 71, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Van Zyl, L.; Du Plessis, J.; Viljoen, J. Cutaneous Tuberculosis Overview and Current Treatment Regimens. Tuberculosis 2015, 95, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-Y.; Jia, Q.-N.; Li, J. Treatment of Non-Tuberculosis Mycobacteria Skin Infections. Front. Pharmacol. 2023, 14, 2156. [Google Scholar] [CrossRef]
- Szumała, P.; Macierzanka, A. Topical Delivery of Pharmaceutical and Cosmetic Macromolecules Using Microemulsion Systems. Int. J. Pharm. 2022, 615, 121488. [Google Scholar] [CrossRef]
- Takezaki, H.; Otsubo, T.; Echigo, Y.; Kamiya, H.; Okada, Y. Porous and Spherical Ethyl Cellulose Fine Particles Produced by Ternary System-Based Emulsion Castings. Powder Technol. 2022, 395, 663–668. [Google Scholar] [CrossRef]
- Finch, J.A.; Zhang, W. Frother Function–Structure Relationship: Dependence of CCC95 on HLB and the H-Ratio. Miner. Eng. 2014, 61, 1–8. [Google Scholar] [CrossRef]
- Al Achi, A.; Shrivastava, P. Preparation of Flaxseed Oil Emulsions. J. Pharm. Sci. Innov. 2015, 4, 215–216. [Google Scholar] [CrossRef]
- Leichner, C.; Baus, R.A.; Jelkmann, M.; Plautz, M.; Barthelmes, J.; Dünnhaupt, S.; Bernkop-Schnürch, A. In Vitro Evaluation of a Self-Emulsifying Drug Delivery System (SEDDS) for Nasal Administration of Dimenhydrinate. Drug Deliv. Transl. Res. 2019, 9, 945–955. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Yan, F.; Jia, Q.; Wang, Q. Norm Descriptors for Predicting the Hydrophile-Lipophile Balance (HLB) and Critical Micelle Concentration (CMC) of Anionic Surfactants. Colloids Surf. A Physicochem. Eng. Asp. 2019, 583, 123967. [Google Scholar] [CrossRef]
- Cui, H.; Cao, G.; Zhu, S.; Mu, J.; Chou, X. Study on the Preparation and Formation Factors of Frother Emulsion. Colloids Surf. A Physicochem. Eng. Asp. 2022, 636, 128155. [Google Scholar] [CrossRef]
- Pasquali, R.C.; Taurozzi, M.P.; Bregni, C. Some Considerations about the Hydrophilic–Lipophilic Balance System. Int. J. Pharm. 2008, 356, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Suñer, J.; Calpena, A.C.; Clares, B.; Cañadas, C.; Halbaut, L. Development of Clotrimazole Multiple W/O/W Emulsions as Vehicles for Drug Delivery: Effects of Additives on Emulsion Stability. AAPS PharmSciTech 2017, 18, 539–550. [Google Scholar] [CrossRef] [PubMed]
- Lima, M.T.; Spiering, V.J.; Kurt-Zerdeli, S.N.; Brüggemann, D.C.; Gradzielski, M.; Schomäcker, R. The Hydrophilic-Lipophilic Balance of Carboxylate and Carbonate Modified Nonionic Surfactants. Colloids Surf. A Physicochem. Eng. Asp. 2019, 569, 156–163. [Google Scholar] [CrossRef]
- Montillet, A.; Nedjar, S.; Tazerout, M. Continuous Production of Water-in-Oil Emulsion Using Micromixers. Fuel 2013, 106, 410–416. [Google Scholar] [CrossRef]
- Farooq, A.; Shafaghat, H.; Jae, J.; Jung, S.C.; Park, Y.K. Enhanced Stability of Bio-Oil and Diesel Fuel Emulsion Using Span 80 and Tween 60 Emulsifiers. J. Environ. Manag. 2019, 231, 694–700. [Google Scholar] [CrossRef]
- Kang, B.K.; Lee, J.S.; Chon, S.K.; Jeong, S.Y.; Yuk, S.H.; Khang, G.; Lee, H.B.; Cho, S.H. Development of Self-Microemulsifying Drug Delivery Systems (SMEDDS) for Oral Bioavailability Enhancement of Simvastatin in Beagle Dogs. Int. J. Pharm. 2004, 274, 65–73. [Google Scholar] [CrossRef]
- Prajapat, M.D.; Patel, N.J.; Bariya, A.; Patel, S.S.; Butani, S.B. Formulation and Evaluation of Self-Emulsifying Drug Delivery System for Nimodipine, a BCS Class II Drug. J. Drug Deliv. Sci. Technol. 2017, 39, 59–68. [Google Scholar] [CrossRef]
- Hemmati, F.; Jafari, S.M.; Taheri, R.A. Optimization of Homogenization-Sonication Technique for the Production of Cellulose Nanocrystals from Cotton Linter. Int. J. Biol. Macromol. 2019, 137, 374–381. [Google Scholar] [CrossRef]
- Rohrer, J.; Zupančič, O.; Hetényi, G.; Kurpiers, M.; Bernkop-Schnürch, A. Design and Evaluation of SEDDS Exhibiting High Emulsifying Properties. J. Drug Deliv. Sci. Technol. 2018, 44, 366–372. [Google Scholar] [CrossRef]
- Czajkowska-Kośnik, A.; Szekalska, M.; Amelian, A.; Szymańska, E.; Winnicka, K. Development and Evaluation of Liquid and Solid Self-Emulsifying Drug Delivery Systems for Atorvastatin. Molecules 2015, 20, 21010–21022. [Google Scholar] [CrossRef]
- Qi, X.; Wang, L.; Zhu, J.; Hu, Z.; Zhang, J. Self-Double-Emulsifying Drug Delivery System (SDEDDS): A New Way for Oral Delivery of Drugs with High Solubility and Low Permeability. Int. J. Pharm. 2011, 409, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Jiang, S.; Wang, X.; Liao, J.; Yin, Z. Preparation and Evaluation of Nattokinase-Loaded Self-Double-Emulsifying Drug Delivery System. Asian J. Pharm. Sci. 2015, 10, 386–395. [Google Scholar] [CrossRef]
- Van Zyl, L.; Viljoen, J.M.; Haynes, R.K.; Aucamp, M.; Ngwane, A.H.; du Plessis, J. Topical Delivery of Artemisone, Clofazimine and Decoquinate Encapsulated in Vesicles and Their In Vitro Efficacy Against Mycobacterium Tuberculosis. AAPS PharmSciTech 2019, 20, 33. [Google Scholar] [CrossRef] [PubMed]
- Oladipo, O.G.; Ezeokoli, O.T.; Maboeta, M.S.; Bezuidenhout, J.J.; Tiedt, L.R.; Jordaan, A.; Bezuidenhout, C.C. Tolerance and Growth Kinetics of Bacteria Isolated from Gold and Gemstone Mining Sites in Response to Heavy Metal Concentrations. J. Environ. Manag. 2018, 212, 357–366. [Google Scholar] [CrossRef]
- Onwudiwe, D.C.; Krüger, T.P.J.; Jordaan, A.; Strydom, C.A. Laser-Assisted Synthesis, and Structural and Thermal Properties of ZnS Nanoparticles Stabilised in Polyvinylpyrrolidone. Appl. Surf. Sci. 2014, 321, 197–204. [Google Scholar] [CrossRef]
- Hua, S. Lipid-Based Nano-Delivery Systems for Skin Delivery of Drugs and Bioactives. Front. Pharmacol. 2015, 6, 219. [Google Scholar] [CrossRef]
- Ibrar, M.; Ayub, Y.; Nazir, R.; Irshad, M.; Hussain, N.; Saleem, Y.; Ahmad, M. Garlic and Ginger Essential Oil-Based Neomycin Nano-Emulsions as Effective and Accelerated Treatment for Skin Wounds’ Healing and Inflammation: In-Vivo and in-Vitro Studies. Saudi Pharm. J. 2022, 30, 1700–1709. [Google Scholar] [CrossRef]
- Hasan, N.; Imran, M.; Sheikh, A.; Tiwari, N.; Jaimini, A.; Kesharwani, P.; Jain, G.K.; Ahmad, F.J. Advanced Multifunctional Nano-Lipid Carrier Loaded Gel for Targeted Delivery of 5-Flurouracil and Cannabidiol against Non-Melanoma Skin Cancer. Environ. Res. 2023, 233, 116454. [Google Scholar] [CrossRef]
- Qureshi, M.; Qadir, A.; Aqil, M.; Sultana, Y.; Warsi, M.H.; Ismail, M.V.; Talegaonkar, S. Berberine Loaded Dermal Quality by Design Adapted Chemically Engineered Lipid Nano-Constructs-Gel Formulation for the Treatment of Skin Acne. J. Drug Deliv. Sci. Technol. 2021, 66, 102805. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug | Log P | Molecular Weight (Da) | Aqueous Solubility | Elimination Half-Life | Metabolized | BCS Classification |
|---|---|---|---|---|---|---|
| CFZ | 7.66 | 473.40 | <1 mg/mL | 70 days | Hepatic | Class II |
| INH | 0.64 | 137.14 | 125 mg/mL | 45–110 min 1 2–4.5 h 2 | Hepatic | Class I/III 3 |
| PZY | −1.88 | 123.11 | 15 mg/mL | 3–5 h | Hepatic | Class III |
| RIF | 3.80 | 822.90 | 1.51 mg/mL | 3–4 h | Hepatic | Class II |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Staden, D.; Haynes, R.K.; Viljoen, J.M. The Development of Dermal Self-Double-Emulsifying Drug Delivery Systems: Preformulation Studies as the Keys to Success. Pharmaceuticals 2023, 16, 1348. https://doi.org/10.3390/ph16101348
van Staden D, Haynes RK, Viljoen JM. The Development of Dermal Self-Double-Emulsifying Drug Delivery Systems: Preformulation Studies as the Keys to Success. Pharmaceuticals. 2023; 16(10):1348. https://doi.org/10.3390/ph16101348
Chicago/Turabian Stylevan Staden, Daniélle, Richard K. Haynes, and Joe M. Viljoen. 2023. "The Development of Dermal Self-Double-Emulsifying Drug Delivery Systems: Preformulation Studies as the Keys to Success" Pharmaceuticals 16, no. 10: 1348. https://doi.org/10.3390/ph16101348
APA Stylevan Staden, D., Haynes, R. K., & Viljoen, J. M. (2023). The Development of Dermal Self-Double-Emulsifying Drug Delivery Systems: Preformulation Studies as the Keys to Success. Pharmaceuticals, 16(10), 1348. https://doi.org/10.3390/ph16101348