
Complement System as a New Target for Hematopoietic Stem Cell Transplantation-Related Thrombotic Microangiopathy

 and
and
Abstract
:1. Introduction
2. Literature Search
3. Complement System Involvement
3.1. Functional Aspects
3.2. Genetic Aspects
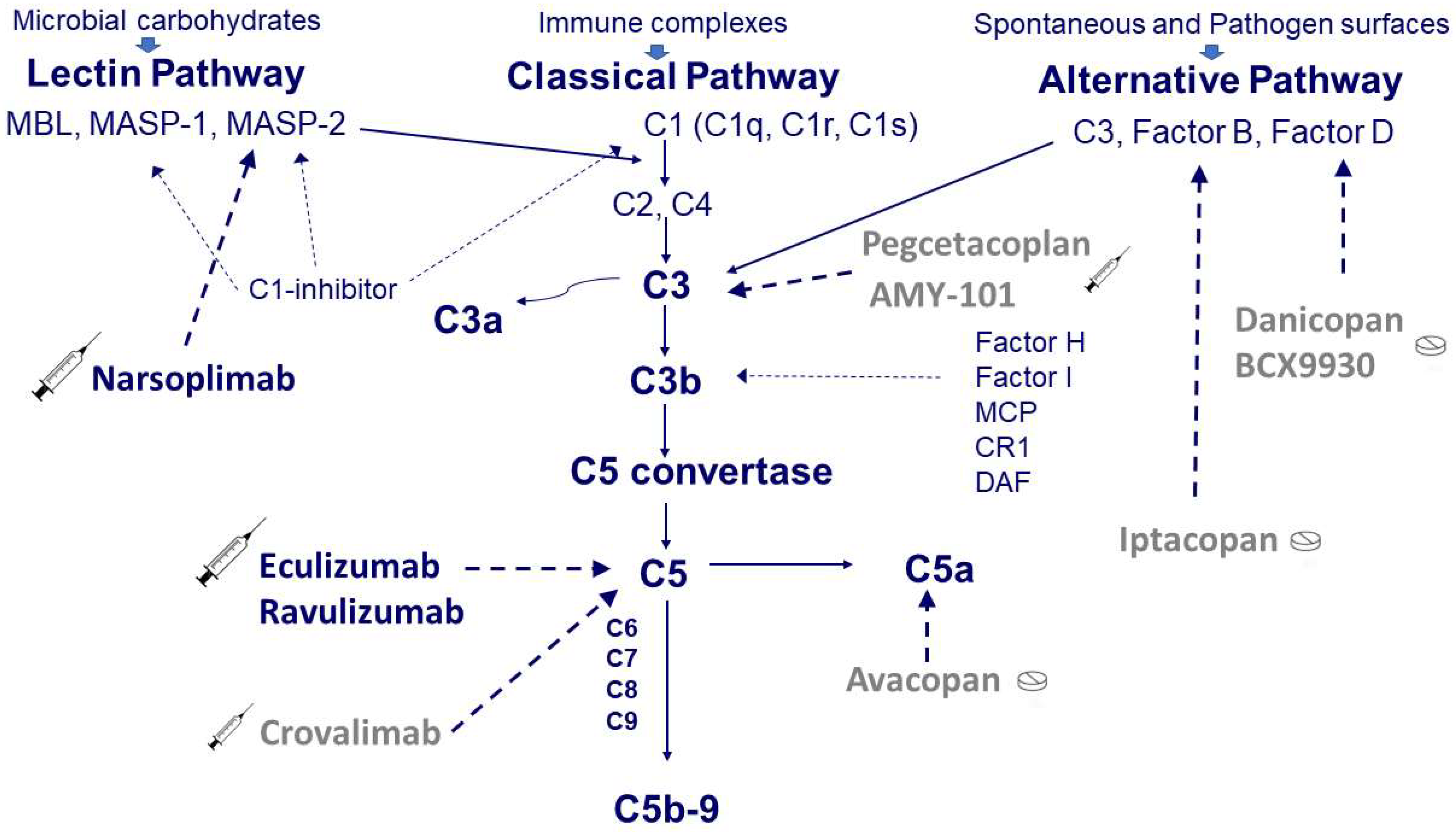
3.3. Therapeutic Aspects
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goodship, T.H.; Cook, H.T.; Fakhouri, F.; Fervenza, F.C.; Frémeaux-Bacchi, V.; Kavanagh, D.; Nester, C.M.; Noris, M.; Pickering, M.C.; de Córdoba, S.R.; et al. Atypical hemolytic uremic syndrome and C3 glomerulopathy: Conclusions from a “Kidney Disease: Improving Global Outcomes” (KDIGO) Controversies Conference. Kidney Int. 2017, 91, 539–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavriilaki, E.; Sakellari, I.; Batsis, I.; Mallouri, D.; Bousiou, Z.; Vardi, A.; Yannaki, E.; Constantinou, V.; Tsompanakou, A.; Vadikoliou, C.; et al. Transplant-associated thrombotic microangiopathy: Incidence, prognostic factors, morbidity, and mortality in allogeneic hematopoietic cell transplantation. Clin. Transplant. 2018, 32, e13371. [Google Scholar] [CrossRef] [PubMed]
- Sakellari, I.; Gavriilaki, E.; Boussiou, Z.; Batsis, I.; Mallouri, D.; Constantinou, V.; Kaloyannidis, K.; Yannaki, E.; Bamihas, G.; Anagnostopoulos, A. Transplant-associated thrombotic microangiopathy: An unresolved complication of unrelated allogeneic transplant for hematologic diseases. Hematol. Oncol. 2016, 35, 932–934. [Google Scholar] [CrossRef]
- Van Benschoten, V.; Roy, C.; Gupta, R.; Ouellette, L.; Hingorani, S.; Li, A. Incidence and Risk Factors of Transplantation-Associated Thrombotic Microangiopathy: A Systematic Review and Meta-Analysis. Transplant. Cell. Ther. 2022, 28, 266.e1–266.e8. [Google Scholar] [CrossRef] [PubMed]
- Ho, V.T.; Cutler, C.; Carter, S.; Martin, P.; Adams, R.; Horowitz, M.; Ferrara, J.; Soiffer, R.; Giralt, S. Blood and Marrow Transplant Clinical Trials Network Toxicity Committee Consensus Summary: Thrombotic Microangiopathy after Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2005, 11, 571–575. [Google Scholar] [CrossRef] [Green Version]
- Ruutu, T.; Barosi, G.; Benjamin, R.J.; Clark, R.E.; George, J.N.; Gratwohl, A.; Holler, E.; Iacobelli, M.; Kentouche, K.; Lämmle, B.; et al. Diagnostic criteria for hematopoietic stem cell transplant-associated microangiopathy: Results of a consensus process by an International Working Group. Haematologica 2007, 92, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Shayani, S.; Palmer, J.; Stiller, T.; Liu, X.; Thomas, S.; Khuu, T.; Parker, P.M.; Khaled, S.K.; Forman, S.J.; Nakamura, R. Thrombotic Microangiopathy Associated with Sirolimus Level after Allogeneic Hematopoietic Cell Transplantation with Tacrolimus/Sirolimus-Based Graft-versus-Host Disease Prophylaxis. Biol. Blood Marrow Transplant. 2013, 19, 298–304. [Google Scholar] [CrossRef] [Green Version]
- Cho, B.-S.; Yahng, S.-A.; Lee, S.-E.; Eom, K.-S.; Kim, Y.-J.; Kim, H.-J.; Lee, S.; Min, C.-K.; Cho, S.-G.; Kim, D.-W.; et al. Validation of Recently Proposed Consensus Criteria for Thrombotic Microangiopathy After Allogeneic Hematopoietic Stem-Cell Transplantation. Transplantation 2010, 90, 918–926. [Google Scholar] [CrossRef]
- Uderzo, C.; Jodele, S.; El Missiry, M.; Ciceri, F.; Bacigalupo, A.; Corbacioglu, S. Transplant-Associated Thrombotic Microangiopathy (TA-TMA) and Consensus Based Diagnostic and Therapeutic Recommendations: Which TA-TMA Patients to Treat and When? J. Bone Marrow Res. 2014, 2, 152. [Google Scholar] [CrossRef]
- Jodele, S.; Davies, S.M.; Lane, A.; Khoury, J.; Dandoy, C.; Goebel, J.; Myers, K.; Grimley, M.; Bleesing, J.; El-Bietar, J.; et al. Diagnostic and risk criteria for HSCT-associated thrombotic microangiopathy: A study in children and young adults. Blood 2014, 124, 645–653. [Google Scholar] [CrossRef] [Green Version]
- George, J.N.; Li, X.; McMinn, J.R.; Terrell, D.; Vesely, S.; Selby, G.B. Thrombotic thrombocytopenic purpura-hemolytic uremic syndrome following allogeneic HPC transplantation: A diagnostic dilemma. Transfusion 2004, 44, 294–304. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt, G.C.; Chao, N. Endothelial cell function and endothelial-related disorders following haematopoietic cell transplantation. Br. J. Haematol. 2020, 190, 508–519. [Google Scholar] [CrossRef] [PubMed]
- Pagliuca, S.; Michonneau, D.; De Fontbrune, F.S.; Del Galy, A.S.; Xhaard, A.; Robin, M.; De Latour, R.P.; Socie, G. Allogeneic reactivity–mediated endothelial cell complications after HSCT: A plea for consensual definitions. Blood Adv. 2019, 3, 2424–2435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, J.A.; Pallas, C.R.; Knovich, M.A. Transplant-associated thrombotic microangiopathy: Theoretical considerations and a practical approach to an unrefined diagnosis. Bone Marrow Transplant. 2021, 56, 1805–1817. [Google Scholar] [CrossRef]
- Reis, E.S.; Mastellos, D.; Hajishengallis, G.; Lambris, J.D. New insights into the immune functions of complement. Nat. Rev. Immunol. 2019, 19, 503–516. [Google Scholar] [CrossRef] [PubMed]
- Holers, V.M. Complement and Its Receptors: New Insights into Human Disease. Annu. Rev. Immunol. 2014, 32, 433–459. [Google Scholar] [CrossRef]
- Oikonomopoulou, K.; Ricklin, D.; Ward, P.A.; Lambris, J.D. Interactions between coagulation and complement—their role in inflammation. In Seminars in Immunopathology; Springer: Berlin/Heidelberg, Germany, 2012; pp. 151–165. [Google Scholar]
- Ballow, M.; Good, R.A.; Day, N.K. Complement in Graft Versus Host Disease: I. Depletion of Complement Components during a Systemic Graft Versus Host Reaction in the Rat. Exp. Biol. Med. 1975, 148, 170–176. [Google Scholar] [CrossRef]
- Kourilsky, O.; Vandewalle, A.; Smith, M.; Stühlinger, W.; Verroust, P.J.; Gonzalo, A.; Neuilly, G.; Kanfer, A.; Sraer, J.D.; Morel-Maroger, L. Persistent intravascular C3 activation after bilateral nephrectomy in patients with thrombotic microangiopathy. Clin. Nephrol. 1976, 6, 437–439. [Google Scholar]
- George, J.N.; Nester, C.M. Syndromes of Thrombotic Microangiopathy. N. Engl. J. Med. 2014, 371, 654–666. [Google Scholar] [CrossRef] [Green Version]
- Gruppo, R.A.; Rother, R.P. Eculizumab for Congenital Atypical Hemolytic–Uremic Syndrome. N. Engl. J. Med. 2009, 360, 544–546. [Google Scholar] [CrossRef]
- Holler, E.; Kolb, H.J.; Hiller, E.; Mraz, W.; Lehmacher, W.; Gleixner, B.; Seeber, C.; Jehn, U.; Gerhartz, H.H.; Brehm, G. Microangiopathy in patients on cyclosporine prophylaxis who developed acute graft-versus-host disease after HLA-identical bone marrow transplantation. Blood 1989, 73, 2018–2024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mii, A.; Shimizu, A.; Kaneko, T.; Fujita, E.; Fukui, M.; Fujino, T.; Utsumi, K.; Yamaguchi, H.; Tajika, K.; Tsuchiya, S.-I.; et al. Renal thrombotic microangiopathy associated with chronic graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. Pathol. Int. 2011, 61, 518–527. [Google Scholar] [CrossRef] [PubMed]
- Laskin, B.L.; Maisel, J.; Goebel, J.; Yin, H.J.; Luo, G.; Khoury, J.C.; Davies, S.M.; Jodele, S. Renal arteriolar C4d deposition: A novel characteristic of hematopoietic stem cell transplantation-associated thrombotic microangiopathy. Transplantation 2013, 96, 217–223. [Google Scholar] [CrossRef] [Green Version]
- Jodele, S.; Fukuda, T.; Vinks, A.; Mizuno, K.; Laskin, B.L.; Goebel, J.; Dixon, B.; Teusink, A.; Pluthero, F.; Lu, L.; et al. Eculizumab Therapy in Children with Severe Hematopoietic Stem Cell Transplantation–Associated Thrombotic Microangiopathy. Biol. Blood Marrow Transplant. 2013, 20, 518–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, J.; Hu, S.; He, X.; Pan, T.; Yang, L.; Zhang, R.; Tang, Y.; Wu, D.; Han, Y. N-Acetyl-L-Cysteine Potentially Inhibits Complement Activation in Transplantation-Associated Thrombotic Microangiopathy. Transplant. Cell. Ther. 2021, 28, 216.e1–216.e5. [Google Scholar] [CrossRef]
- Mezö, B.; Horváth, O.; Sinkovits, G.; Veszeli, N.; Kriván, G.; Prohászka, Z. Validation of Early Increase in Complement Activation Marker sC5b-9 as a Predictive Biomarker for the Development of Thrombotic Microangiopathy After Stem Cell Transplantation. Front. Med. (Lausanne) 2020, 7, 569291. [Google Scholar] [CrossRef]
- Gavriilaki, E.; Sakellari, I.; Chatzikonstantinou, T.; Mallouri, D.; Batsis, I.; Vardi, A.; Bousiou, Z.; Koravou, E.-E.; Masmanidou, M.; Touloumenidou, T.; et al. Endothelial and Complement Activation as Predictors of Survival in Adult Allogeneic Hematopoietic Cell Transplantation. HemaSphere 2020, 5, e487. [Google Scholar] [CrossRef]
- Okamura, H.; Nakamae, H.; Shindo, T.; Ohtani, K.; Hidaka, Y.; Ohtsuka, Y.; Makuuchi, Y.; Kuno, M.; Takakuwa, T.; Harada, N.; et al. Early Elevation of Complement Factor Ba Is a Predictive Biomarker for Transplant-Associated Thrombotic Microangiopathy. Front. Immunol. 2021, 12, 695037. [Google Scholar] [CrossRef]
- Jodele, S.; Licht, C.; Goebel, J.; Dixon, B.; Zhang, K.; Sivakumaran, T.A.; Davies, S.M.; Pluthero, F.; Lu, L.; Laskin, B.L. Abnormalities in the alternative pathway of complement in children with hematopoietic stem cell transplant-associated thrombotic microangiopathy. Blood 2013, 122, 2003–2007. [Google Scholar] [CrossRef] [PubMed]
- Cugno, M.; Berra, S.; Depetri, F.; Tedeschi, S.; Griffini, S.; Grovetti, E.; Caccia, S.; Cresseri, D.; Messa, P.; Testa, S.; et al. IgM Autoantibodies to Complement Factor H in Atypical Hemolytic Uremic Syndrome. J. Am. Soc. Nephrol. 2021, 32, 1227–1235. [Google Scholar] [CrossRef]
- Jodele, S.; Zhang, K.; Zou, F.; Laskin, B.; Dandoy, C.; Myers, K.C.; Lane, A.; Meller, J.; Medvedovic, M.; Chen, J.; et al. The genetic fingerprint of susceptibility for transplant-associated thrombotic microangiopathy. Blood 2016, 127, 989–996. [Google Scholar] [CrossRef] [Green Version]
- Gavriilaki, E.; Touloumenidou, T.; Sakellari, I.; Batsis, I.; Mallouri, D.; Psomopoulos, F.; Tsagiopoulou, M.; Koutra, M.; Yannaki, E.; Papalexandri, A.; et al. Pretransplant Genetic Susceptibility: Clinical Relevance in Transplant-Associated Thrombotic Microangiopathy. Thromb. Haemost. 2020, 120, 638–646. [Google Scholar] [CrossRef]
- Zheng, L.; Zhang, D.; Cao, W.; Song, W.-C.; Zheng, X.L. Synergistic effects of ADAMTS13 deficiency and complement activation in pathogenesis of thrombotic microangiopathy. Blood 2019, 134, 1095–1105. [Google Scholar] [CrossRef] [PubMed]
- Ardissino, G.; Salardi, S.; Berra, S.; Colussi, G.; Cugno, M.; Zecca, M.; Giglio, F.; Peccatori, I.; Diral, E.; Tel, F.; et al. Acquired Complement Regulatory Gene Mutations and Hematopoietic Stem Cell Transplant–Related Thrombotic Microangiopathy. Biol. Blood Marrow Transplant. 2017, 23, 1580–1582. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, E.M.; Ardissino, G.; Pintarelli, G.; Capone, V.; Mariotti, J.; Verna, M.; Bernardo, M.E.; Faraci, M.; Tozzi, M.; Bucalossi, A.; et al. Gene Abnormalities in Transplant Associated-Thrombotic Microangiopathy: Comparison between Recipient and Donor’s DNA. Thromb. Haemost. 2021. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Wu, Q.V.; Amos, C.I.; Liu, Y.; Wei, H.; Cheng, C.; Tsavachidis, S.; Bryce, A.; Sartain, S.E.; Martinez, C.A.; et al. Rare Variant Genetic Association Study for Transplant-Associated Thrombotic Microangiopathy (TA-TMA) Via Whole Exome Sequencing. Blood 2021, 138 (Suppl. S1), 745. [Google Scholar] [CrossRef]
- Jodele, S.; Sabulski, A. Transplant-associated thrombotic microangiopathy: Elucidating prevention strategies and identifying high-risk patients. Expert Rev. Hematol. 2021, 14, 751–763. [Google Scholar] [CrossRef] [PubMed]
- Rathbone, J.; Kaltenthaler, E.; Richards, A.; Tappenden, P.; Bessey, A.; Cantrell, A. A systematic review of eculizumab for atypical haemolytic uraemic syndrome (aHUS). BMJ Open 2013, 3, e003573. [Google Scholar] [CrossRef]
- Jodele, S. Complement in Pathophysiology and Treatment of Transplant-Associated Thrombotic Microangiopathies. Semin. Hematol. 2018, 55, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.S.; Patel, M.; Yum, K.; Keyzner, A. Hematopoietic stem cell transplant-associated thrombotic microangiopathy: Review of pharmacologic treatment options. Transfusion 2014, 55, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Jodele, S.; Laskin, B.L.; Goebel, J.; Khoury, J.C.; Pinkard, S.L.; Carey, P.; Davies, S.M. Does early initiation of therapeutic plasma exchange improve outcome in pediatric stem cell transplant-associated thrombotic microangiopathy? Transfusion 2012, 53, 661–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulay, S.; Kreuter, J.D.; Bryant, S.C.; Elliott, M.A.; Hogan, W.J.; Winters, J.L.; Gastineau, D.A. Outcomes of plasma exchange in patients with transplant-associated thrombotic microangiopathy based on time of presentation since transplant. J. Clin. Apher. 2014, 30, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhan, A.; Connelly-Smith, L.; Aqui, N.; Balogun, R.A.; Klingel, R.; Meyer, E.; Pham, H.P.; Schneiderman, J.; Witt, V.; Wu, Y.; et al. Guidelines on the Use of Therapeutic Apheresis in Clinical Practice—Evidence-Based Approach from the Writing Committee of the American Society for Apheresis: The Eighth Special Issue. J. Clin. Apher. 2019, 34, 171–354. [Google Scholar] [CrossRef] [PubMed]
- Au, W.-Y.; Ma, E.; Lee, T.-L.; Ha, S.-Y.; Fung, A.T.; Lie, A.K.W.; Kwong, Y.-L. Successful treatment of thrombotic microangiopathy after haematopoietic stem cell transplantation with rituximab. Br. J. Haematol. 2007, 137, 475–478. [Google Scholar] [CrossRef]
- Marr, H.; McDonald, E.J.; Merriman, E.; Smith, M.; Mangos, H.; Stoddart, C.; Ganly, P. Successful treatment of transplant-associated microangiopathy with rituximab. N. Zeal. Med. J. 2009, 122, 72–74. [Google Scholar]
- Corti, P.; Uderzo, C.; Tagliabue, A.; Della Volpe, A.; Annaloro, C.; Tagliaferri, E.; Balduzzi, A. Defibrotide as a promising treatment for thrombotic thrombocytopenic purpura in patients undergoing bone marrow transplantation. Bone Marrow Transplant. 2002, 29, 542–543. [Google Scholar] [CrossRef] [Green Version]
- Yeates, L.; Slatter, M.A.; Bonanomi, S.; Lim, F.L.W.I.; Ong, S.Y.; Dalissier, A.; Barberi, W.; Shulz, A.; Duval, M.; Heilmann, C.; et al. Use of defibrotide to treat transplant-associated thrombotic microangiopathy: A retrospective study of the Paediatric Diseases and Inborn Errors Working Parties of the European Society of Blood and Marrow Transplantation. Bone Marrow Transplant. 2017, 52, 762–764. [Google Scholar] [CrossRef]
- Wolff, D.; Wilhelm, S.; Hahn, J.; Gentilini, C.; Hilgendorf, I.; Steiner, B.; Kahl, C.; Junghanss, C.; Hartung, G.; Casper, J.; et al. Replacement of calcineurin inhibitors with daclizumab in patients with transplantation-associated microangiopathy or renal insufficiency associated with graft-versus-host disease. Bone Marrow Transplant. 2006, 38, 445–451. [Google Scholar] [CrossRef] [Green Version]
- Ardissino, G.; Possenti, I.; Tel, F.; Testa, S.; Salardi, S.; Ladisa, V. Discontinuation of Eculizumab Treatment in Atypical Hemolytic Uremic Syndrome: An Update. Am. J. Kidney Dis. 2015, 66, 172–173. [Google Scholar] [CrossRef] [PubMed]
- Jodele, S.; Dandoy, C.E.; Lane, A.; Laskin, B.L.; Teusink-Cross, A.; Myers, K.C.; Wallace, G.H.; Nelson, A.; Bleesing, J.; Chima, R.S.; et al. Complement blockade for TA-TMA: Lessons learned from large pediatric cohort treated with eculizumab. Blood 2020, 135, 1049–1057. [Google Scholar] [CrossRef]
- Mizuno, K.; Dandoy, C.E.; Teusink-Cross, A.; Davies, S.M.; Vinks, A.A.; Jodele, S. Eculizumab precision-dosing algorithm for thrombotic microangiopathy in children and young adults undergoing HSCT. Blood Adv. 2022, 6, 1454–1463. [Google Scholar] [CrossRef] [PubMed]
- Jodele, S.; Fukuda, T.; Mizuno, K.; Vinks, A.; Laskin, B.L.; Goebel, J.; Dixon, B.; Chima, R.S.; Hirsch, R.; Teusink, A.; et al. Variable Eculizumab Clearance Requires Pharmacodynamic Monitoring to Optimize Therapy for Thrombotic Microangiopathy after Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2015, 22, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahimova, A.; Luebbering, N.; Abdullah, S.; Todd, K.; Duell, A.; Lake, K.E.; Mullins, E.; Palumbo, J.; Davies, S.M.; Jodele, S. Understanding the Mechanisms of Eculizumab Refractoriness in Transplant Associated Thrombotic Microangiopathy. In Proceedings of the 2021 TCT Meeting Digital Experience, 8–12 February 2022; Available online: https://tct.confex.com/tandem/2021/meetingapp.cgi/Paper/17205 (accessed on 28 April 2022).
- De Fontbrune, F.S.; Galambrun, C.; Sirvent, A.; Huynh, A.; Faguer, S.; Nguyen, S.; Bay, J.-O.; Neven, B.; Moussi, J.; Simon, L.; et al. Use of Eculizumab in Patients with Allogeneic Stem Cell Transplant-Associated Thrombotic Microangiopathy: A study from the SFGM-TC. Transplantation 2015, 99, 1953–1959. [Google Scholar] [CrossRef] [PubMed]
- Rudoni, J.; Jan, A.; Hosing, C.; Aung, F.; Yeh, J. Eculizumab for transplant-associated thrombotic microangiopathy in adult allogeneic stem cell transplant recipients. Eur. J. Haematol. 2018, 101, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Vasu, S.; Wu, H.; Satoskar, A.; Puto, M.; Roddy, J.; Blum, W.; Klisovic, R.; Andritsos, L.; Hofmeister, C.; Benson, D.M.; et al. Eculizumab therapy in adults with allogeneic hematopoietic cell transplant-associated thrombotic microangiopathy. Bone Marrow Transplant. 2016, 51, 1241–1244. [Google Scholar] [CrossRef] [Green Version]
- Bohl, S.R.; Kuchenbauer, F.; von Harsdorf, S.; Kloevekorn, N.; Schönsteiner, S.S.; Rouhi, A.; Schwarzwälder, P.; Döhner, H.; Bunjes, D.; Bommer, M. Thrombotic Microangiopathy after Allogeneic Stem Cell Transplantation: A Comparison of Eculizumab Therapy and Conventional Therapy. Biol. Blood Marrow Transplant. 2017, 23, 2172–2177. [Google Scholar] [CrossRef] [Green Version]
- Brambilla, M.; Ardissino, G.; Paglialonga, F.; Testa, S.; Capone, V.; Montini, G. Haemoglobinuria for the early identification of aHUS relapse: Data from the ItalKId-HUS Network. J. Nephrol. 2021, 35, 279–284. [Google Scholar] [CrossRef]
- Jayne, D.R.; Merkel, P.A.; Schall, T.J.; Bekker, P. Avacopan for the Treatment of ANCA-Associated Vasculitis. N. Engl. J. Med. 2021, 384, 599–609. [Google Scholar] [CrossRef]
- Fakhouri, F.; Schwotzer, N.; Golshayan, D.; Frémeaux-Bacchi, V. The Rational Use of Complement Inhibitors in Kidney Diseases. Kidney Int. Rep. 2022, 7, 1165–1178. [Google Scholar] [CrossRef]
- Brodsky, R.A.; Young, N.S.; Antonioli, E.; Risitano, A.M.; Schrezenmeier, H.; Schubert, J.; Gaya, A.; Coyle, L.; De Castro, C.; Fu, C.-L.; et al. Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria. Blood 2008, 111, 1840–1847. [Google Scholar] [CrossRef]
- Tschumi, S.; Gugger, M.; Bucher, B.S.; Riedl, M.; Simonetti, G.D. Eculizumab in atypical hemolytic uremic syndrome: Long-term clinical course and histological findings. Pediatr. Nephrol. 2011, 26, 2085–2088. [Google Scholar] [CrossRef] [PubMed]
- Cugno, M.; Gualtierotti, R.; Possenti, I.; Testa, S.; Tel, F.; Griffini, S.; Grovetti, E.; Tedeschi, S.; Salardi, S.; Cresseri, D.; et al. Complement functional tests for monitoring eculizumab treatment in patients with atypical hemolytic uremic syndrome. J. Thromb. Haemost. JTH 2014, 12, 1440–1448. [Google Scholar] [CrossRef] [PubMed]
- Ardissino, G.; Tel, F.; Sgarbanti, M.; Cresseri, D.; Giussani, A.; Griffini, S.; Grovetto, E.; Possenti, I.; Perrone, M.; Testa, S.; et al. Complement functional tests for monitoring eculizumab treatment in patients with atypical hemolytic uremic syndrome: An update. Pediatr. Nephrol. 2017, 33, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Cugno, M.; Capone, V.; Griffini, S.; Grovetti, E.; Pintarelli, G.; Porcaro, L.; Clementi, E.; Ardissino, G. Eculizumab treatment in atypical hemolytic uremic syndrome: Correlation between functional complement tests and drug levels. J. Nephrol. 2022, 35, 1205–1211. [Google Scholar] [CrossRef]
- Wetzels, J.F.; van de Kar, N.C. Discontinuation of Eculizumab Maintenance Treatment for Atypical Hemolytic Uremic Syndrome. Am. J. Kidney Dis. 2015, 65, 342. [Google Scholar] [CrossRef] [PubMed]
- de Latour, R.P.; Xhaard, A.; Fremeaux-Bacchi, V.; Coppo, P.; Fischer, A.M.; Helley, D.; Socié, G. Successful use of eculizumab in a patient with post-transplant thrombotic microangiopathy. Br. J. Haematol. 2013, 161, 279–280. [Google Scholar] [CrossRef]
- Sahelijo, L.; Mujeebudin, A.; Mitchell, D.; Larouche, R.; Yu, Z.X.; Zhang, Y.; Soni, P. First in human single-ascending dose study: Safety, biomarker, pharmacokinetics and exposure-response relationships of ALXN1210, a humanized monoclonal antibody to C5, with marked half-life extension and potential for significantly longer dosing intervals. Blood 2015, 126, 4777. [Google Scholar] [CrossRef]
- Hill, A.; DeZern, A.E.; Kinoshita, T.; Brodsky, R.A. Paroxysmal nocturnal haemoglobinuria. Nat. Rev. Dis. Primers 2017, 18, 17028. [Google Scholar] [CrossRef] [Green Version]
- Sheridan, D.; Yu, Z.X.; Zhang, Y.; Patel, R.; Sun, F.; Lasaro, M.A.; Tamburini, P. Design and preclinical characterization of ALXN1210: A novel anti-C5 antibody with extended duration of action. PLoS ONE 2018, 13, e0195909. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.W.; Bachman, E.S.; Aguzzi, R.; Jang, J.H.; Kim, J.S.; Rottinghaus, S.T.; Szer, J. Immediate, complete, and sustained inhibition of C5 with ALXN1210 reduces complement-mediated hemolysis in patients with paroxysmal nocturnal hemoglobinuria (PNH): Interim analysis of a dose-escalation study. Blood 2016, 128, 2428. [Google Scholar] [CrossRef]
- Sostelly, A.; Soubret, A.; Bucher, C.; Buatois, C.; Charoin, J.E.; Jordan, G.; Klughammer, B.; Dieckmann, A.; Fukuzawa, T.; Gotanda, K.; et al. Characterizing C5 Inhibition with the SMART-Ig Anti-hC5 Antibody Crovalimab in PNH Patients Using Free Available Paratopes. Blood 2019, 134 (Suppl. S1), 1277. [Google Scholar] [CrossRef]
- Goodship, T.H.J.; Pinto, F.; Weston-Davies, W.H.; Silva, J.; Nishimura, J.-I.; Nunn, M.A.; Mackie, I.; Machin, S.J.; Palm, L.; Pryce, J.W.; et al. Use of the complement inhibitor Coversin to treat HSCT-associated TMA. Blood Adv. 2017, 1, 1254–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozarcanin, H.; Lood, C.; Munthe-Fog, L.; Sandholm, K.; Hamad, O.A.; Bengtsson, A.; Skjødt, M.-O.; Huber-Lang, M.; Garred, P.; Ekdahl, K.N.; et al. The lectin complement pathway serine proteases (MASPs) represent a possible crossroad between the coagulation and complement systems in thromboinflammation. J. Thromb. Haemost. 2015, 14, 531–545. [Google Scholar] [CrossRef] [PubMed]
- Gulla, K.C.; Gupta, K.; Krarup, A.; Gal, P.; Schwaeble, W.J.; Sim, R.B.; O’Connor, C.D.; Hajela, K. Activation of mannan-binding lectin-associated serine proteases leads to generation of a fibrin clot. Immunology 2009, 129, 482–495. [Google Scholar] [CrossRef] [PubMed]
- Krarup, A.; Wallis, R.; Presanis, J.S.; Gál, P.; Sim, R. Simultaneous Activation of Complement and Coagulation by MBL-Associated Serine Protease 2. PLoS ONE 2007, 2, e623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rambaldi, A.; Gritti, G.; Micò, M.C.; Frigeni, M.; Borleri, G.; Salvi, A.; Landi, F.; Pavoni, C.; Sonzogni, A.; Gianatti, A.; et al. Endothelial injury and thrombotic microangiopathy in COVID-19: Treatment with the lectin-pathway inhibitor narsoplimab. Immunobiology 2020, 225, 152001. [Google Scholar] [CrossRef]
- Khaled, S.K.; Claes, K.; Goh, Y.T.; Kwong, Y.L.; Leung, N.; Mendrek, W.; Nakamura, R.; Sathar, J.; Ng, E.; Nangia, N.; et al. Narsoplimab, a Mannan-Binding Lectin-Associated Serine Protease-2 Inhibitor, for the Treatment of Adult Hematopoietic Stem-Cell Transplantation–Associated Thrombotic Microangiopathy. J. Clin. Oncol. 2022, JCO2102389. [Google Scholar] [CrossRef]
- Zhang, R.; Zhou, M.; Qi, J.; Miao, W.; Zhang, Z.; Wu, D.; Han, Y. Efficacy and Safety of Eculizumab in the Treatment of Transplant-Associated Thrombotic Microangiopathy: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 11, 564647. [Google Scholar] [CrossRef]

{kind=link}
| CTN [5] | IWG [6] | COH [7] | Cho et al. [8] | Uderzo et al. [9] | Jodele et al. [10] | |
|---|---|---|---|---|---|---|
| De novo thrombocytopenia | - | yes | yes | yes | yes | yes |
| De novo anemia | - | yes | - | yes | yes | yes |
| Schistocytosis | yes | yes | yes | yes | yes | yes |
| Negative Coombs test | yes | - | - | yes | yes | - |
| Decreased haptoglobin | - | yes | - | yes | - | - |
| Increase in LDH | yes | yes | yes | yes | yes | yes |
| Renal or Neuro-dysfunction | yes | - | yes | - | yes | yes |
| Hypertension | - | - | - | - | yes | yes |
| Proteinuria | - | - | - | - | yes | yes |
| Increased sC5b9 | - | - | - | - | yes | yes |
| Frequency of TA-TMA (%) | - | 50 | 17 | 13 | - | 18 |
| Genetic Alterations in Complement Regulation (Positive Subjects/Investigated Subjects) | Anti-Factor H Auto-ab (Positive Subjects/Investigated Subjects) | Complement Functional Involvement | ||
|---|---|---|---|---|
| Receiver’s DNA | Donor’s DNA | |||
| Mii et al. 2011 [23] | - | - | - | C4d glomerular deposition |
| Laskin et al. 2013 [24] | - | - | - | C4d glomerular deposition |
| Jodele et al. 2013 [30] | 5/6 | 1/6 | 3/6 | - |
| Jodele et al. 2014 [25] | - | - | - | Elevated plasma levels of sC5b-9 |
| Jodele et al. 2016 [32] | 22/34 | - | - | - |
| Ardissino et al. 2017 [35] | 0/16 | 6/16 | - | - |
| Qi et al. 2017 [26] | - | - | - | Elevated plasma levels of sC5b-9 and C3b |
| Gavriilaki et al. 2020 [28] | - | - | - | Elevated plasma levels of sC5b-9 |
| Gavriilaki et al. 2020 [33] | 31 */40 | 5 */18 | - | Elevated plasma levels of sC5b-9 |
| Mezo et al. 2020 [27] | - | - | - | Elevated plasma levels of sC5b-9 |
| Cugno et al. 2021 [31] | - | 4/20 | 7/20 | - |
| Rodriguez et al. 2021 [36] | 4/33 | 11/33 | - | - |
| Okamura et al. 2021 [29] | 9/15 | - | - | Elevated plasma levels of Ba |
| Zhang et al. 2021 [37] | 9 */91 | - | - | - |
| Drug | Type | Mechanism of Action | Mode of Administration | Response Rate | References |
|---|---|---|---|---|---|
| Used in TA-TMA | |||||
| Eculizumab | mAb | Inhibition of C5 and C5b9 formation | intravenous | Children 67–78%Adults 33–60% | [25,50,51,52,53,54,55,56,57,58,59] |
| Ravulizumab | mAb | Inhibition of C5 and C5b9 formation | intravenous | Under evaluation | NCT04543591 |
| Coversin | Small protein | Inhibition of C5 and C5b9 formation | subcutaneous | Single case | [74] |
| Narsoplimab | mAb | MASP-2 inhibition | intravenous | Adults 61% | [79] NCT02222545 |
| Pegcetacoplan | Peptide | C3 inhibition | subcutaneous | Under evaluation | NCT05148299 |
| Never used in TA-TMA | |||||
| Crovalimab | mAb | Inhibition of C5 and C5b9 formation | subcutaneous | ||
| Iptacopam | Small molecule | Factor B inhibition | oral | ||
| Danicopan | Small molecule | Factor D inhibition | oral | ||
| BCX9930 | Small molecule | Factor D inhibition | oral | ||
| Avacopan | Small molecule | C5a inhibition | oral | ||
| AMY-101 | Peptide | C3 inhibition | subcutaneous | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ardissino, G.; Capone, V.; Tedeschi, S.; Porcaro, L.; Cugno, M. Complement System as a New Target for Hematopoietic Stem Cell Transplantation-Related Thrombotic Microangiopathy. Pharmaceuticals 2022, 15, 845. https://doi.org/10.3390/ph15070845
Ardissino G, Capone V, Tedeschi S, Porcaro L, Cugno M. Complement System as a New Target for Hematopoietic Stem Cell Transplantation-Related Thrombotic Microangiopathy. Pharmaceuticals. 2022; 15(7):845. https://doi.org/10.3390/ph15070845
Chicago/Turabian StyleArdissino, Gianluigi, Valentina Capone, Silvana Tedeschi, Luigi Porcaro, and Massimo Cugno. 2022. "Complement System as a New Target for Hematopoietic Stem Cell Transplantation-Related Thrombotic Microangiopathy" Pharmaceuticals 15, no. 7: 845. https://doi.org/10.3390/ph15070845
APA StyleArdissino, G., Capone, V., Tedeschi, S., Porcaro, L., & Cugno, M. (2022). Complement System as a New Target for Hematopoietic Stem Cell Transplantation-Related Thrombotic Microangiopathy. Pharmaceuticals, 15(7), 845. https://doi.org/10.3390/ph15070845