
Biologics in COVID-19 So Far: Systematic Review


Abstract
:1. Introduction
2. Results
2.1. Interleukin 6 Inhibitors
2.2. Interleukin 1 Inhibitors
2.3. Interferons
2.4. Mesenchymal Stem Cells
2.5. Anti-Spike Monoclonal Antibodies
3. Discussion
4. Materials and Methods
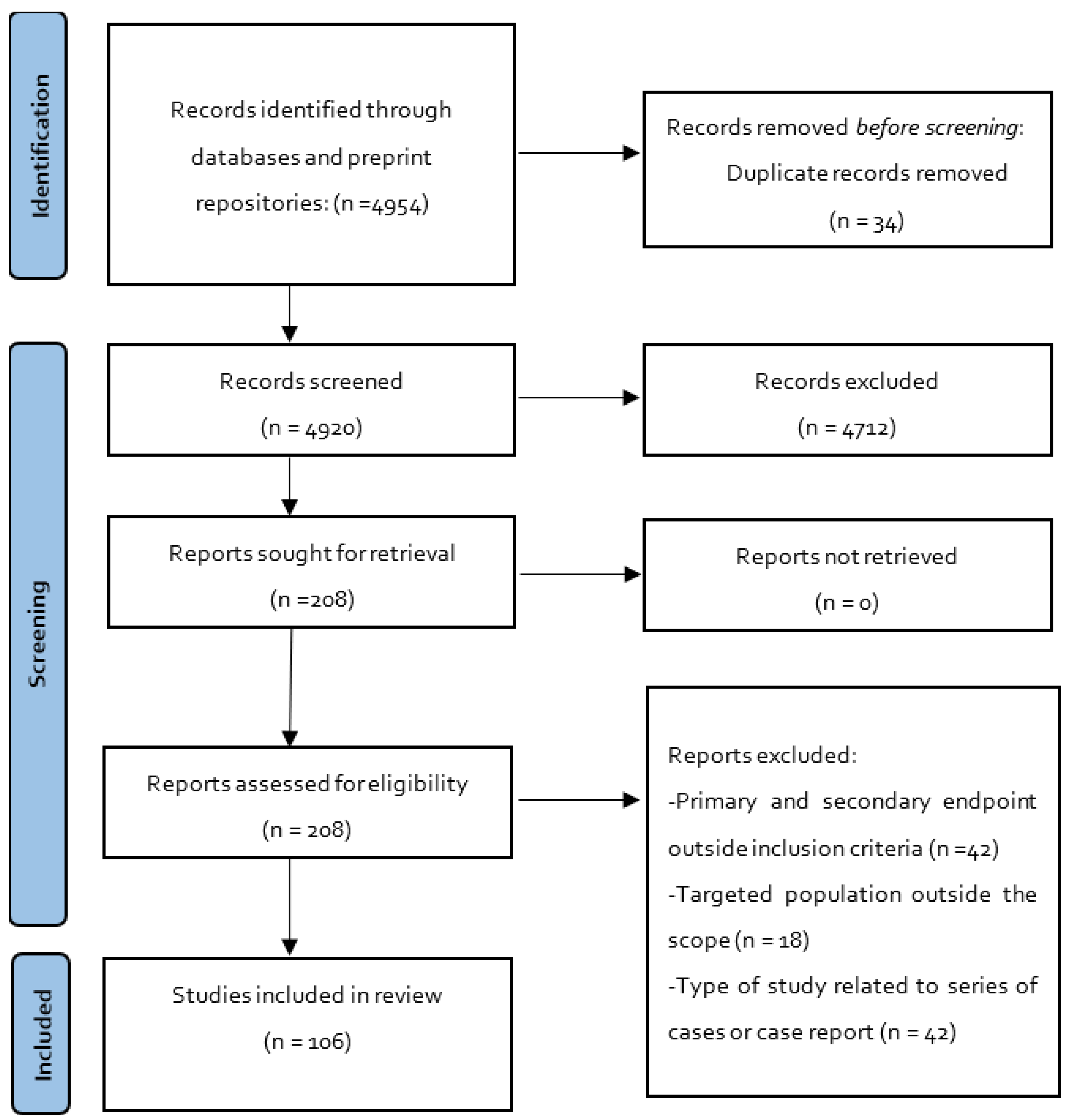
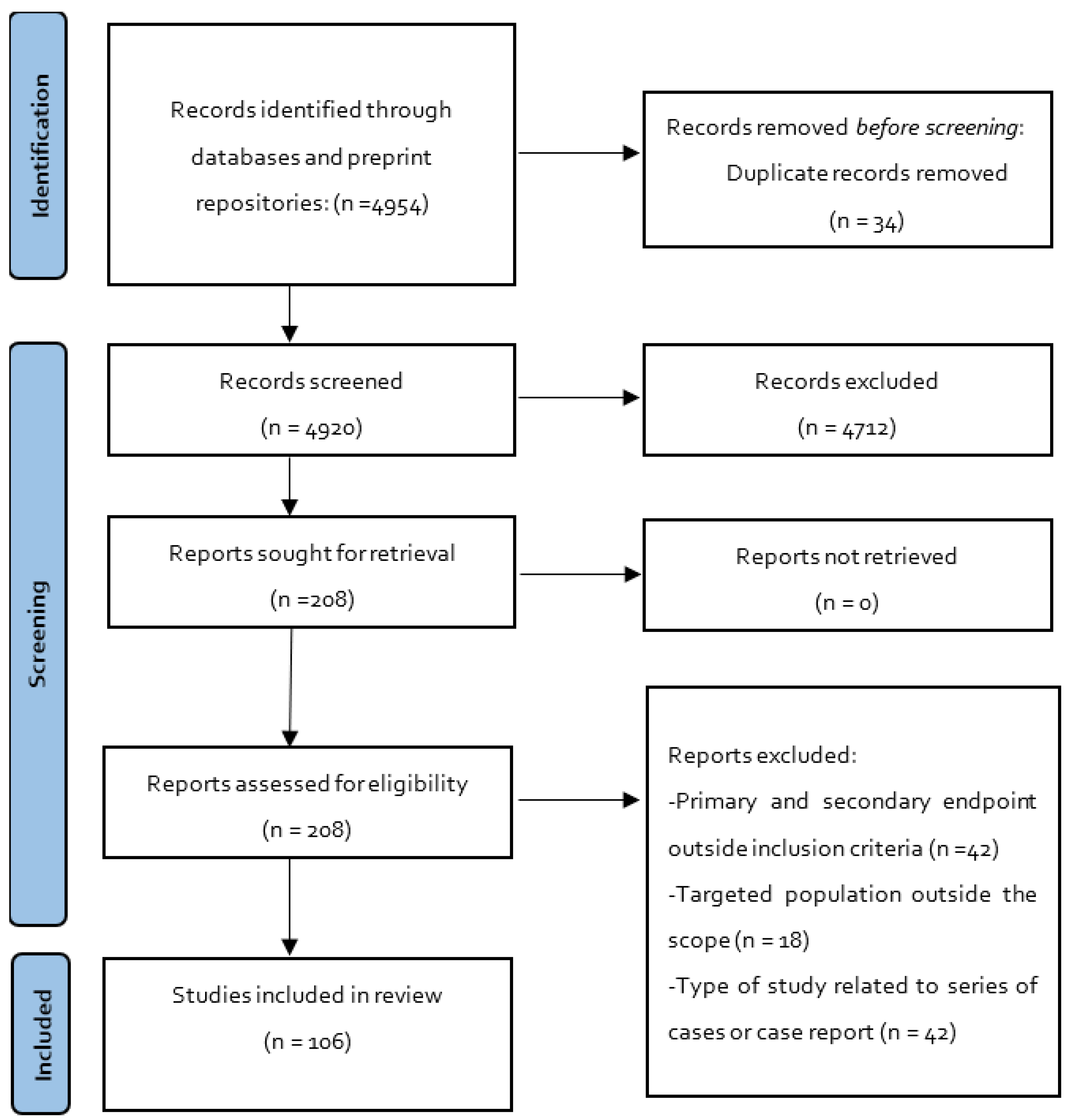
4.1. Search Eligibility Criteria and Search Strategy
4.2. Study Selection, and Data Extraction
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carlos, W.G.; Dela Cruz, C.S.; Cao, B.; Pasnick, S.; Jamil, S. Novel Wuhan (2019-nCoV) Coronavirus. Am. J. Respir. Crit. Care Med. 2020, 201, 7–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Santos, W.G. Natural history of COVID-19 and current knowledge on treatment therapeutic options. Biomed. Pharmacother. Biomed. Pharmacother. 2020, 129, 110493. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Weekly Epidemiological Update. Available online: https://www.who.int/publications/m/item/covid-19-weekly-epidemiological-update (accessed on 15 October 2021).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. Jama 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Golden, P.; Hennessey, E. Naming of Biological Products. U.S. Pharm. 2020, 45, 33–36. [Google Scholar]
- Food and Drug Administration. Definition of the Term “Biological Product”. Fed. Regist. 2020, 85, 10057–10063. [Google Scholar]
- Park, R.; Wurzburg, J.; Faccenda, M. FDA Final Rule Amends Definition of “Biological Product”. Available online: https://www.thehealthlawpulse.com/2020/03/fda-final-rule-amends-definition-of-biological-product/#:~:text=Under%20the%20final%20rule%2C%20the,are%20regulated%20as%20drugs%20or (accessed on 3 June 2022).
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. Jama 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef]
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292.e286. [Google Scholar] [CrossRef]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Cornillez-Ty, C.T.; Liao, L.; Yates, J.R., 3rd; Kuhn, P.; Buchmeier, M.J. Severe acute respiratory syndrome coronavirus nonstructural protein 2 interacts with a host protein complex involved in mitochondrial biogenesis and intracellular signaling. J. Virol. 2009, 83, 10314–10318. [Google Scholar] [CrossRef] [Green Version]
- Cottam, E.M.; Whelband, M.C.; Wileman, T. Coronavirus NSP6 restricts autophagosome expansion. Autophagy 2014, 10, 1426–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackbart, M.; Deng, X.; Baker, S.C. Coronavirus endoribonuclease targets viral polyuridine sequences to evade activating host sensors. Proc. Natl. Acad. Sci. USA 2020, 117, 8094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Lokugamage, K.G.; Rozovics, J.M.; Narayanan, K.; Semler, B.L.; Makino, S. SARS coronavirus nsp1 protein induces template-dependent endonucleolytic cleavage of mRNAs: Viral mRNAs are resistant to nsp1-induced RNA cleavage. PLoS Pathog. 2011, 7, e1002433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivanov, K.A.; Thiel, V.; Dobbe, J.C.; van der Meer, Y.; Snijder, E.J.; Ziebuhr, J. Multiple enzymatic activities associated with severe acute respiratory syndrome coronavirus helicase. J. Virol. 2004, 78, 5619–5632. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Wu, L.; Shaw, N.; Gao, Y.; Wang, J.; Sun, Y.; Lou, Z.; Yan, L.; Zhang, R.; Rao, Z. Structural basis and functional analysis of the SARS coronavirus nsp14–nsp10 complex. Proc. Natl. Acad. Sci. USA 2015, 112, 9436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakai, Y.; Kawachi, K.; Terada, Y.; Omori, H.; Matsuura, Y.; Kamitani, W. Two-amino acids change in the nsp4 of SARS coronavirus abolishes viral replication. Virology 2017, 510, 165–174. [Google Scholar] [CrossRef]
- te Velthuis, A.J.; van den Worm, S.H.; Snijder, E.J. The SARS-coronavirus nsp7+nsp8 complex is a unique multimeric RNA polymerase capable of both de novo initiation and primer extension. Nucleic Acids Res. 2012, 40, 1737–1747. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Sun, Y.; Wu, A.; Xu, S.; Pan, R.; Zeng, C.; Jin, X.; Ge, X.; Shi, Z.; Ahola, T.; et al. Coronavirus nsp10/nsp16 Methyltransferase Can Be Targeted by nsp10-Derived Peptide In Vitro and In Vivo To Reduce Replication and Pathogenesis. J. Virol. 2015, 89, 8416–8427. [Google Scholar] [CrossRef] [Green Version]
- Fujimoto, I.; Pan, J.; Takizawa, T.; Nakanishi, Y. Virus clearance through apoptosis-dependent phagocytosis of influenza A virus-infected cells by macrophages. J. Virol. 2000, 74, 3399–3403. [Google Scholar] [CrossRef] [Green Version]
- Channappanavar, R.; Zhao, J.; Perlman, S. T cell-mediated immune response to respiratory coronaviruses. Immunol. Res. 2014, 59, 118–128. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Fu, B.; Zheng, X.; Wang, D.; Zhao, C.; Qi, Y.; Sun, R.; Tian, Z.; Xu, X.; Wei, H. Pathogenic T-cells and inflammatory monocytes incite inflammatory storms in severe COVID-19 patients. Natl. Sci. Rev. 2020, 7, 998–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients with Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Gong, E.; Zhang, B.; Zheng, J.; Gao, Z.; Zhong, Y.; Zou, W.; Zhan, J.; Wang, S.; Xie, Z.; et al. Multiple organ infection and the pathogenesis of SARS. J. Exp. Med. 2005, 202, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Capra, R.; De Rossi, N.; Mattioli, F.; Romanelli, G.; Scarpazza, C.; Sormani, M.P.; Cossi, S. Impact of low dose tocilizumab on mortality rate in patients with COVID-19 related pneumonia. Eur. J. Intern. Med. 2020, 76, 31–35. [Google Scholar] [CrossRef]
- Colaneri, M.; Bogliolo, L.; Valsecchi, P.; Sacchi, P.; Zuccaro, V.; Brandolino, F.; Montecucco, C.; Mojoli, F.; Giusti, E.M.; Bruno, R.; et al. Tocilizumab for Treatment of Severe COVID-19 Patients: Preliminary Results from SMAtteo COvid19 REgistry (SMACORE). Microorganisms 2020, 8, 695. [Google Scholar] [CrossRef]
- Klopfenstein, T.; Zayet, S.; Lohse, A.; Balblanc, J.C.; Badie, J.; Royer, P.Y.; Toko, L.; Mezher, C.; Kadiane-Oussou, N.J.; Bossert, M.; et al. Tocilizumab therapy reduced intensive care unit admissions and/or mortality in COVID-19 patients. Med. Mal. Infect. 2020, 50, 397–400. [Google Scholar] [CrossRef]
- Quartuccio, L.; Sonaglia, A.; McGonagle, D.; Fabris, M.; Peghin, M.; Pecori, D.; De Monte, A.; Bove, T.; Curcio, F.; Bassi, F.; et al. Profiling COVID-19 pneumonia progressing into the cytokine storm syndrome: Results from a single Italian Centre study on tocilizumab versus standard of care. J. Clin. Virol. 2020, 129, 104444. [Google Scholar] [CrossRef]
- Ramaswamy, M.; Mannam, P.; Comer, R.; Sinclair, E.; McQuaid, D.B.; Schmidt, M.L. Off-Label Real World Experience Using Tocilizumab for Patients Hospitalized with COVID-19 Disease in a Regional Community Health System: A Case-Control Study. medRxiv 2020. [Google Scholar] [CrossRef]
- Roumier, M.; Paule, R.; Groh, M.; Vallée, A.; Ackermann, F.; for the Foch, C.-S.G. Interleukin-6 blockade for severe COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Wadud, N.; Ahmed, N.; Shergil, M.; Khan, M.; Krishna, M.; Gilani, A.; Zarif, S.E.; Galaydick, J.; Linga, K.; Koor, S.; et al. Improved survival outcome in SARs-CoV-2 (COVID-19) Acute Respiratory Distress Syndrome patients with Tocilizumab administration. medRxiv 2020. [Google Scholar] [CrossRef]
- Alattar, R.; Ibrahim, T.B.H.; Shaar, S.H.; Abdalla, S.; Shukri, K.; Daghfal, J.N.; Khatib, M.Y.; Aboukamar, M.; Abukhattab, M.; Alsoub, H.A.; et al. Tocilizumab for the treatment of severe coronavirus disease 2019. J. Med. Virol. 2020, 92, 2042–2049. [Google Scholar] [CrossRef] [PubMed]
- Campochiaro, C.; Della-Torre, E.; Cavalli, G.; De Luca, G.; Ripa, M.; Boffini, N.; Tomelleri, A.; Baldissera, E.; Rovere-Querini, P.; Ruggeri, A.; et al. Efficacy and safety of tocilizumab in severe COVID-19 patients: A single-centre retrospective cohort study. Eur. J. Intern. Med. 2020, 76, 43–49. [Google Scholar] [CrossRef]
- Guaraldi, G.; Meschiari, M.; Cozzi-Lepri, A.; Milic, J.; Tonelli, R.; Menozzi, M.; Franceschini, E.; Cuomo, G.; Orlando, G.; Borghi, V.; et al. Tocilizumab in patients with severe COVID-19: A retrospective cohort study. Lancet Rheumatol. 2020, 2, e474–e484. [Google Scholar] [CrossRef]
- Kewan, T.; Covut, F.; Al-Jaghbeer, M.J.; Rose, L.; Gopalakrishna, K.V.; Akbik, B. Tocilizumab for treatment of patients with severe COVID-19: A retrospective cohort study. EClinicalMedicine 2020, 24, 100418. [Google Scholar] [CrossRef] [PubMed]
- Luo, P.; Liu, Y.; Qiu, L.; Liu, X.; Liu, D.; Li, J. Tocilizumab treatment in COVID-19: A single center experience. J. Med. Virol. 2020, 92, 814–818. [Google Scholar] [CrossRef] [PubMed]
- Morena, V.; Milazzo, L.; Oreni, L.; Bestetti, G.; Fossali, T.; Bassoli, C.; Torre, A.; Cossu, M.V.; Minari, C.; Ballone, E.; et al. Off-label use of tocilizumab for the treatment of SARS-CoV-2 pneumonia in Milan, Italy. Eur. J. Intern. Med. 2020, 76, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Price, C.C.; Altice, F.L.; Shyr, Y.; Koff, A.; Pischel, L.; Goshua, G.; Azar, M.M.; McManus, D.; Chen, S.C.; Gleeson, S.E.; et al. Tocilizumab Treatment for Cytokine Release Syndrome in Hospitalized Patients with Coronavirus Disease 2019: Survival and Clinical Outcomes. Chest 2020, 158, 1397–1408. [Google Scholar] [CrossRef]
- Sciascia, S.; Aprà, F.; Baffa, A.; Baldovino, S.; Boaro, D.; Boero, R.; Bonora, S.; Calcagno, A.; Cecchi, I.; Cinnirella, G.; et al. Pilot prospective open, single-arm multicentre study on off-label use of tocilizumab in patients with severe COVID-19. Clin. Exp. Rheumatol. 2020, 38, 529–532. [Google Scholar]
- Toniati, P.; Piva, S.; Cattalini, M.; Garrafa, E.; Regola, F.; Castelli, F.; Franceschini, F.; Airò, P.; Bazzani, C.; Beindorf, E.A.; et al. Tocilizumab for the treatment of severe COVID-19 pneumonia with hyperinflammatory syndrome and acute respiratory failure: A single center study of 100 patients in Brescia, Italy. Autoimmun. Rev. 2020, 19, 102568. [Google Scholar] [CrossRef]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970. [Google Scholar] [CrossRef]
- Fomina, D.S.; Lysenko, M.A.; Beloglazova, I.P.; Mutovina, Z.Y.; Poteshkina, N.G.; Samsonova, I.V.; Kruglova, T.S.; Chernov, A.A.; Karaulov, A.V. Temporal Clinical and Laboratory Response to Interleukin-6 Receptor Blockade with Tocilizumab in 89 Hospitalized Patients With COVID-19 Pneumonia. Pathog. Immun. 2020, 5, 327–341. [Google Scholar] [CrossRef] [PubMed]
- Górgolas Hernández-Mora, M.; Cabello Úbeda, A.; Prieto-Pérez, L.; Villar Álvarez, F.; Álvarez Álvarez, B.; Rodríguez Nieto, M.J.; Carrillo Acosta, I.; Fernández Ormaechea, I.; Al-Hayani, A.W.M.; Carballosa, P.; et al. Compassionate use of tocilizumab in severe SARS-CoV2 pneumonia. Int. J. Infect. Dis. 2021, 102, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Ip, A.; Berry, D.A.; Hansen, E.; Goy, A.H.; Pecora, A.L.; Sinclaire, B.A.; Bednarz, U.; Marafelias, M.; Berry, S.M.; Berry, N.S.; et al. Hydroxychloroquine and tocilizumab therapy in COVID-19 patients—An observational study. PLoS ONE 2020, 15, e0237693. [Google Scholar] [CrossRef]
- Kimmig, L.M.; Wu, D.; Gold, M.; Pettit, N.N.; Pitrak, D.; Mueller, J.; Husain, A.N.; Mutlu, E.A.; Mutlu, G.M. IL-6 Inhibition in Critically Ill COVID-19 Patients Is Associated with Increased Secondary Infections. Front. Med. 2020, 7, 583897. [Google Scholar] [CrossRef]
- Martínez-Sanz, J.; Muriel, A.; Ron, R.; Herrera, S.; Pérez-Molina, J.A.; Moreno, S.; Serrano-Villar, S. Effects of tocilizumab on mortality in hospitalized patients with COVID-19: A multicentre cohort study. Clin. Microbiol. Infect. 2021, 27, 238–243. [Google Scholar] [CrossRef]
- Moreno-García, E.; Rico, V.; Albiach, L.; Agüero, D.; Ambrosioni, J.; Bodro, M.; Cardozo, C.; Chumbita, M.; De la Mora, L.; García-Pouton, N.; et al. Tocilizumab is associated with reduced risk of ICU admission and mortality in patients with SARS-CoV-2 infection. medRxiv 2020. [Google Scholar] [CrossRef]
- Perrone, F.; Piccirillo, M.C.; Ascierto, P.A.; Salvarani, C.; Parrella, R.; Marata, A.M.; Popoli, P.; Ferraris, L.; Marrocco-Trischitta, M.M.; Ripamonti, D.; et al. Tocilizumab for patients with COVID-19 pneumonia. The single-arm TOCIVID-19 prospective trial. J. Transl. Med. 2020, 18, 405. [Google Scholar] [CrossRef]
- Petrak, R.M.; Skorodin, N.C.; Van Hise, N.W.; Fliegelman, R.M.; Pinsky, J.; Didwania, V.; Anderson, M.; Diaz, M.; Shah, K.; Chundi, V.V.; et al. Tocilizumab as a Therapeutic Agent for Critically Ill Patients Infected with SARS-CoV-2. Clin. Transl. Sci. 2021, 14, 2146–2151. [Google Scholar] [CrossRef]
- Rossi, B.; Nguyen, L.S.; Zimmermann, P.; Boucenna, F.; Dubret, L.; Baucher, L.; Guillot, H.; Bouldouyre, M.A.; Allenbach, Y.; Salem, J.E.; et al. Effect of Tocilizumab in Hospitalized Patients with Severe COVID-19 Pneumonia: A Case-Control Cohort Study. Pharmaceuticals 2020, 13, 317. [Google Scholar] [CrossRef]
- Sánchez-Montalvá, A.; Sellarés-Nadal, J.; Espinosa-Pereiro, J.; Fernández-Hidalgo, N.; Pérez-Hoyos, S.; Salvador, F.; Durà, X.; Miarons, M.; Antón, A.; Eremiev-Eremiev, S.; et al. Early outcomes of tocilizumab in adults hospitalized with severe COVID-19 - The Vall d’Hebron COVID-19 prospective cohort study. medRxiv 2020. [Google Scholar] [CrossRef]
- Somers, E.C.; Eschenauer, G.A.; Troost, J.P.; Golob, J.L.; Gandhi, T.N.; Wang, L.; Zhou, N.; Petty, L.A.; Baang, J.H.; Dillman, N.O.; et al. Tocilizumab for Treatment of Mechanically Ventilated Patients With COVID-19. Clin. Infect. Dis. 2021, 73, e445–e454. [Google Scholar] [CrossRef] [PubMed]
- Sabbatinelli, J.; Giuliani, A.; Matacchione, G.; Latini, S.; Laprovitera, N.; Pomponio, G.; Ferrarini, A.; Svegliati Baroni, S.; Pavani, M.; Moretti, M.; et al. Decreased serum levels of the inflammaging marker miR-146a are associated with clinical non-response to tocilizumab in COVID-19 patients. Mech. Ageing Dev. 2021, 193, 111413. [Google Scholar] [CrossRef] [PubMed]
- Hermine, O.; Mariette, X.; Tharaux, P.L.; Resche-Rigon, M.; Porcher, R.; Ravaud, P. Effect of Tocilizumab vs Usual Care in Adults Hospitalized with COVID-19 and Moderate or Severe Pneumonia: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Salvarani, C.; Dolci, G.; Massari, M.; Merlo, D.F.; Cavuto, S.; Savoldi, L.; Bruzzi, P.; Boni, F.; Braglia, L.; Turrà, C.; et al. Effect of Tocilizumab vs Standard Care on Clinical Worsening in Patients Hospitalized with COVID-19 Pneumonia: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 24–31. [Google Scholar] [CrossRef]
- Malekzadeh, R.; Abedini, A.; Mohsenpour, B.; Sharifipour, E.; Ghasemian, R.; Javad-Mousavi, S.A.; Khodashahi, R.; Darban, M.; Kalantari, S.; Abdollahi, N.; et al. Subcutaneous tocilizumab in adults with severe and critical COVID-19: A prospective open-label uncontrolled multicenter trial. Int. Immunopharmacol. 2020, 89, 107102. [Google Scholar] [CrossRef]
- Dastan, F.; Saffaei, A.; Haseli, S.; Marjani, M.; Moniri, A.; Abtahian, Z.; Abedini, A.; Kiani, A.; Seifi, S.; Jammati, H.; et al. Promising effects of tocilizumab in COVID-19: A non-controlled, prospective clinical trial. Int. Immunopharmacol. 2020, 88, 106869. [Google Scholar] [CrossRef]
- Rodríguez-Molinero, A.; Pérez-López, C.; Gálvez-Barrón, C.; Miñarro, A.; Macho, O.; López, G.F.; Robles, M.T.; Dapena, M.D.; Martínez, S.; Rodríguez, E.; et al. Matched cohort study on the efficacy of tocilizumab in patients with COVID-19. One Health 2021, 12, 100214. [Google Scholar] [CrossRef]
- Vela, D.; Vela-Gaxha, Z.; Rexhepi, M.; Olloni, R.; Hyseni, V.; Nallbani, R. Efficacy and safety of tocilizumab versus standard care/placebo in patients with COVID-19; a systematic review and meta-analysis of randomized clinical trials. Br. J. Clin. Pharmacol. 2022, 88, 1955–1963. [Google Scholar] [CrossRef]
- Duarte-Millán, M.A.; Mesa-Plaza, N.; Guerrero-Santillán, M.; Morales-Ortega, A.; Bernal-Bello, D.; Farfán-Sedano, A.I.; García de Viedma-García, V.; Velázquez-Ríos, L.; Frutos-Pérez, B.; De Ancos-Aracil, C.L.; et al. Prognostic factors and combined use of tocilizumab and corticosteroids in a Spanish cohort of elderly COVID-19 patients. J. Med. Virol. 2022, 94, 1540–1549. [Google Scholar] [CrossRef]
- Moosazadeh, M.; Mousavi, T. Combination therapy of tocilizumab and steroid for COVID-19 patients: A meta-analysis. J. Med. Virol. 2022, 94, 1350–1356. [Google Scholar] [CrossRef]
- Martínez-Guerra, B.A.; de-León-Cividanes, N.A.; Tamez-Torres, K.M.; Román-Montes, C.M.; Rajme-López, S.; Ortiz-Brizuela, E.; Aguilar-Salinas, C.A.; Sierra-Madero, J.; Sifuentes-Osornio, J.; Ponce-de-León, A.; et al. Effect of Tocilizumab in Mortality among Patients with Severe and Critical COVID-19: Experience in a Third-Level Medical Center. Rev. Investig. Clin. Organo Hosp. Enferm. Nutr. 2022, 74, 40–50. [Google Scholar] [CrossRef] [PubMed]
- AlQahtani, H.; AlBilal, S.; Mahmoud, E.; Aldibasi, O.; Alharbi, A.; Shamas, N.; Alsaedy, A.; Owaidah, K.; Alqahtani, F.Y.; Aleanizy, F.S.; et al. Outcomes associated with tocilizumab with or without corticosteroid versus dexamethasone for treatment of patients with severe to critical COVID-19 pneumonia. J. Infect. Public Health 2022, 15, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Mushtaq, M.Z.; Mahmood, S.B.Z.; Almas, A.; Ather Wasti, S.; Ahsan Ali, S. Tocilizumab in critically ill COVID-19 patients: An observational study. Int. Immunopharmacol. 2022, 102, 108384. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.N.; Hernández-Sánchez, J.; Nagel, S.; Feng, Y.; Cai, F.; Rabin, J.; Morse, C.G.; Nadig, N.R.; Ashraf, O.; Gotur, D.B.; et al. Safety and Efficacy of Tocilizumab 4 or 8 mg/kg in Hospitalized Patients with Moderate to Severe Coronavirus Disease 2019 Pneumonia: A Randomized Clinical Trial. Open Forum Infect. Dis. 2021, 9, ofab608. [Google Scholar] [CrossRef] [PubMed]
- Çelik Ekinci, S.; Akkaya Işık, S. A retrospective evaluation of COVID-19 patients treated with Tocilizumab: Who should be treated? J. Infect. Dev. Ctries. 2021, 15, 1825–1832. [Google Scholar] [CrossRef]
- Karampitsakos, T.; Malakounidou, E.; Papaioannou, O.; Dimakopoulou, V.; Zarkadi, E.; Katsaras, M.; Tsiri, P.; Tsirikos, G.; Georgiopoulou, V.; Oikonomou, I.; et al. Tocilizumab improves 28-day survival in hospitalized patients with severe COVID-19: An open label, prospective study. Respir. Res. 2021, 22, 317. [Google Scholar] [CrossRef]
- Naik, N.B.; Puri, G.D.; Kajal, K.; Mahajan, V.; Bhalla, A.; Kataria, S.; Singla, K.; Panigrahi, P.; Singh, A.; Lazar, M.; et al. High-Dose Dexamethasone Versus Tocilizumab in Moderate to Severe COVID-19 Pneumonia: A Randomized Controlled Trial. Cureus 2021, 13, e20353. [Google Scholar] [CrossRef]
- Abdelnaby, H.; Aboelhassan, W.; Al-Jarallah, M.; Rajan, R.; Dashti, R.; Zhanna, K.D.; Alsaber, A.R.; Abd El-Aleem, A.; Ashry, I.; Abdullah, M.; et al. Outcomes of tocilizumab therapy in severe or critical COVID-19 patients: A retrospective cohort, single-centre study. Trop. Med. Int. Health 2021, 26, 1689–1699. [Google Scholar] [CrossRef]
- Gritti, G.; Raimondi, F.; Ripamonti, D.; Riva, I.; Landi, F.; Alborghetti, L.; Frigeni, M.; Damiani, M.; Micò, C.; Fagiuoli, S.; et al. IL-6 signalling pathway inactivation with siltuximab in patients with COVID-19 respiratory failure: An observational cohort study. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Della-Torre, E.; Campochiaro, C.; Cavalli, G.; De Luca, G.; Napolitano, A.; La Marca, S.; Boffini, N.; Da Prat, V.; Di Terlizzi, G.; Lanzillotta, M.; et al. Interleukin-6 blockade with sarilumab in severe COVID-19 pneumonia with systemic hyperinflammation: An open-label cohort study. Ann. Rheum. Dis. 2020, 79, 1277–1285. [Google Scholar] [CrossRef]
- The Remap-CAP Investigators; Gordon, A.C.; Mouncey, P.R.; Al-Beidh, F.; Rowan, K.M.; Nichol, A.D.; Arabi, Y.M.; Annane, D.; Beane, A.; van Bentum-Puijk, W.; et al. Interleukin-6 Receptor Antagonists in Critically Ill Patients with COVID-19—Preliminary report. medRxiv 2021. [Google Scholar] [CrossRef]
- Gremese, E.; Cingolani, A.; Bosello, S.L.; Alivernini, S.; Tolusso, B.; Perniola, S.; Landi, F.; Pompili, M.; Murri, R.; Santoliquido, A.; et al. Sarilumab use in severe SARS-CoV-2 pneumonia. EClinicalMedicine 2020, 27, 100553. [Google Scholar] [CrossRef]
- Cauchois, R.; Koubi, M.; Delarbre, D.; Manet, C.; Carvelli, J.; Blasco, V.B.; Jean, R.; Fouche, L.; Bornet, C.; Pauly, V.; et al. Early IL-1 receptor blockade in severe inflammatory respiratory failure complicating COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 18951–18953. [Google Scholar] [CrossRef]
- Huet, T.; Beaussier, H.; Voisin, O.; Jouveshomme, S.; Dauriat, G.; Lazareth, I.; Sacco, E.; Naccache, J.M.; Bézie, Y.; Laplanche, S.; et al. Anakinra for severe forms of COVID-19: A cohort study. Lancet. Rheumatol. 2020, 2, e393–e400. [Google Scholar] [CrossRef]
- CORIMUNO-19 Collaborative Group. Effect of anakinra versus usual care in adults in hospital with COVID-19 and mild-to-moderate pneumonia (CORIMUNO-ANA-1): A randomised controlled trial. Lancet Respir. Med. 2021, 9, 295–304. [Google Scholar] [CrossRef]
- Bozzi, G.; Mangioni, D.; Minoia, F.; Aliberti, S.; Grasselli, G.; Barbetta, L.; Castelli, V.; Palomba, E.; Alagna, L.; Lombardi, A.; et al. Anakinra combined with methylprednisolone in patients with severe COVID-19 pneumonia and hyperinflammation: An observational cohort study. J. Allergy Clin. Immunol. 2021, 147, 561–566. [Google Scholar] [CrossRef]
- Cavalli, G.; Larcher, A.; Tomelleri, A.; Campochiaro, C.; Della-Torre, E.; De Luca, G.; Farina, N.; Boffini, N.; Ruggeri, A.; Poli, A.; et al. Interleukin-1 and interleukin-6 inhibition compared with standard management in patients with COVID-19 and hyperinflammation: A cohort study. Lancet Rheumatol. 2021, 3, e253–e261. [Google Scholar] [CrossRef]
- Pontali, E.; Volpi, S.; Signori, A.; Antonucci, G.; Castellaneta, M.; Buzzi, D.; Montale, A.; Bustaffa, M.; Angelelli, A.; Caorsi, R.; et al. Efficacy of early anti-inflammatory treatment with high doses of intravenous anakinra with or without glucocorticoids in patients with severe COVID-19 pneumonia. J. Allergy Clin. Immunol. 2021, 147, 1217–1225. [Google Scholar] [CrossRef]
- Kooistra, E.J.; Waalders, N.J.B.; Grondman, I.; Janssen, N.A.F.; de Nooijer, A.H.; Netea, M.G.; van de Veerdonk, F.L.; Ewalds, E.; van der Hoeven, J.G.; Kox, M.; et al. Anakinra treatment in critically ill COVID-19 patients: A prospective cohort study. Crit. Care 2020, 24, 688. [Google Scholar] [CrossRef]
- Kyriazopoulou, E.; Panagopoulos, P.; Metallidis, S.; Dalekos, G.N.; Poulakou, G.; Gatselis, N.; Karakike, E.; Saridaki, M.; Loli, G.; Stefos, A.; et al. An open label trial of anakinra to prevent respiratory failure in COVID-19. eLife 2021, 10. [Google Scholar] [CrossRef]
- Balkhair, A.; Al-Zakwani, I.; Al Busaidi, M.; Al-Khirbash, A.; Al Mubaihsi, S.; BaTaher, H.; Al Aghbari, J.; Al Busaidi, I.; Al Kindi, M.; Baawain, S.; et al. Anakinra in hospitalized patients with severe COVID-19 pneumonia requiring oxygen therapy: Results of a prospective, open-label, interventional study. Int. J. Infect. Dis. 2021, 103, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Langer-Gould, A.; Smith, J.B.; Gonzales, E.G.; Castillo, R.D.; Figueroa, J.G.; Ramanathan, A.; Li, B.H.; Gould, M.K. Early identification of COVID-19 cytokine storm and treatment with anakinra or tocilizumab. Int. J. Infect. Dis. 2020, 99, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Iglesias-Julián, E.; López-Veloso, M.; de-la-Torre-Ferrera, N.; Barraza-Vengoechea, J.C.; Delgado-López, P.D.; Colazo-Burlato, M.; Ubeira-Iglesias, M.; Montero-Baladía, M.; Lorenzo-Martín, A.; Minguito-de-la-Iglesia, J.; et al. High dose subcutaneous Anakinra to treat acute respiratory distress syndrome secondary to cytokine storm syndrome among severely ill COVID-19 patients. J. Autoimmun. 2020, 115, 102537. [Google Scholar] [CrossRef] [PubMed]
- Borie, R.; Savale, L.; Dossier, A.; Ghosn, J.; Taillé, C.; Visseaux, B.; Jebreen, K.; Diallo, A.; Tesmoingt, C.; Morer, L.; et al. Glucocorticoids with low-dose anti-IL1 anakinra rescue in severe non-ICU COVID-19 infection: A cohort study. PLoS ONE 2020, 15, e0243961. [Google Scholar] [CrossRef] [PubMed]
- Kyriazopoulou, E.; Poulakou, G.; Milionis, H.; Metallidis, S.; Adamis, G.; Tsiakos, K.; Fragkou, A.; Rapti, A.; Damoulari, C.; Fantoni, M.; et al. Early treatment of COVID-19 with anakinra guided by soluble urokinase plasminogen receptor plasma levels: A double-blind, randomized controlled phase 3 trial. Nat. Med. 2021, 27, 1752–1760. [Google Scholar] [CrossRef]
- Franzetti, M.; Forastieri, A.; Borsa, N.; Pandolfo, A.; Molteni, C.; Borghesi, L.; Pontiggia, S.; Evasi, G.; Guiotto, L.; Erba, M.; et al. IL-1 Receptor Antagonist Anakinra in the Treatment of COVID-19 Acute Respiratory Distress Syndrome: A Retrospective, Observational Study. J. Immunol. 2021, 206, 1569. [Google Scholar] [CrossRef]
- Kharazmi, A.B.; Moradi, O.; Haghighi, M.; Kouchek, M.; Manafi-Rasi, A.; Raoufi, M.; Shoaei, S.D.; Hadavand, F.; Nabavi, M.; Miri, M.M.; et al. A randomized controlled clinical trial on efficacy and safety of anakinra in patients with severe COVID-19. Immun. Inflamm. Dis. 2022, 10, 201–208. [Google Scholar] [CrossRef]
- Landi, L.; Ravaglia, C.; Russo, E.; Cataleta, P.; Fusari, M.; Boschi, A.; Giannarelli, D.; Facondini, F.; Valentini, I.; Panzini, I.; et al. Blockage of interleukin-1β with canakinumab in patients with COVID-19. Sci. Rep. 2020, 10, 21775. [Google Scholar] [CrossRef]
- Katia, F.; Myriam, D.P.; Ucciferri, C.; Auricchio, A.; Di Nicola, M.; Marchioni, M.; Eleonora, C.; Emanuela, S.; Cipollone, F.; Vecchiet, J. Efficacy of canakinumab in mild or severe COVID-19 pneumonia. Immun. Inflamm. Dis. 2021, 9, 399–405. [Google Scholar] [CrossRef]
- Caricchio, R.; Abbate, A.; Gordeev, I.; Meng, J.; Hsue, P.Y.; Neogi, T.; Arduino, R.; Fomina, D.; Bogdanov, R.; Stepanenko, T.; et al. Effect of Canakinumab vs Placebo on Survival without Invasive Mechanical Ventilation in Patients Hospitalized with Severe COVID-19: A Randomized Clinical Trial. Jama 2021, 326, 230–239. [Google Scholar] [CrossRef]
- Generali, D.; Bosio, G.; Malberti, F.; Cuzzoli, A.; Testa, S.; Romanini, L.; Fioravanti, A.; Morandini, A.; Pianta, L.; Giannotti, G.; et al. Canakinumab as treatment for COVID-19-related pneumonia: A prospective case-control study. Int. J. Infect. Dis. 2021, 104, 433–440. [Google Scholar] [CrossRef]
- Davoudi-Monfared, E.; Rahmani, H.; Khalili, H.; Hajiabdolbaghi, M.; Salehi, M.; Abbasian, L.; Kazemzadeh, H.; Yekaninejad, M.S. A Randomized Clinical Trial of the Efficacy and Safety of Interferon β-1a in Treatment of Severe COVID-19. Antimicrob. Agents Chemother. 2020, 64, e01061-20. [Google Scholar] [CrossRef] [PubMed]
- Estébanez, M.; Ramírez-Olivencia, G.; Mata, T.; Martí, D.; Gutierrez, C.; de Dios, B.; Herrero, M.D.; Roel, A.; Martínez, Y.; Aguirre, A.; et al. Clinical evaluation of IFN beta1b in COVID-19 pneumonia: A retrospective study. medRxiv 2020. [Google Scholar] [CrossRef]
- Hung, I.F.; Lung, K.C.; Tso, E.Y.; Liu, R.; Chung, T.W.; Chu, M.Y.; Ng, Y.Y.; Lo, J.; Chan, J.; Tam, A.R.; et al. Triple combination of interferon beta-1b, lopinavir-ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: An open-label, randomised, phase 2 trial. Lancet 2020, 395, 1695–1704. [Google Scholar] [CrossRef]
- Pereda, R.; González, D.; Rivero, H.B.; Rivero, J.C.; Pérez, A.; López, L.D.R.; Mezquia, N.; Venegas, R.; Betancourt, J.R.; Domínguez, R.E. Therapeutic Effectiveness of Interferon-α2b Against COVID-19: The Cuban Experience. J. Interferon Cytokine Res. 2020, 40, 438–442. [Google Scholar] [CrossRef]
- Wang, N.; Zhan, Y.; Zhu, L.; Hou, Z.; Liu, F.; Song, P.; Qiu, F.; Wang, X.; Zou, X.; Wan, D.; et al. Retrospective Multicenter Cohort Study Shows Early Interferon Therapy Is Associated with Favorable Clinical Responses in COVID-19 Patients. Cell Host Microbe 2020, 28, 455–464.e452. [Google Scholar] [CrossRef]
- Zhou, Q.; Chen, V.; Shannon, C.P.; Wei, X.-S.; Xiang, X.; Wang, X.; Wang, Z.-H.; Tebbutt, S.J.; Kollmann, T.R.; Fish, E.N. Interferon-α2b Treatment for COVID-19. Front. Immunol. 2020, 11, 1061. [Google Scholar] [CrossRef]
- Rahmani, H.; Davoudi-Monfared, E.; Nourian, A.; Khalili, H.; Hajizadeh, N.; Jalalabadi, N.Z.; Fazeli, M.R.; Ghazaeian, M.; Yekaninejad, M.S. Interferon β-1b in treatment of severe COVID-19: A randomized clinical trial. Int. Immunopharmacol. 2020, 88, 106903. [Google Scholar] [CrossRef]
- Feld, J.J.; Kandel, C.; Biondi, M.J.; Kozak, R.A.; Zahoor, M.A.; Lemieux, C.; Borgia, S.M.; Boggild, A.K.; Powis, J.; McCready, J.; et al. Peginterferon lambda for the treatment of outpatients with COVID-19: A phase 2, placebo-controlled randomised trial. Lancet Respir. Med. 2021, 9, 498–510. [Google Scholar] [CrossRef]
- Qu, W.; Wang, Z.; Hare, J.M.; Bu, G.; Mallea, J.M.; Pascual, J.M.; Caplan, A.I.; Kurtzberg, J.; Zubair, A.C.; Kubrova, E.; et al. Cell-based therapy to reduce mortality from COVID-19: Systematic review and meta-analysis of human studies on acute respiratory distress syndrome. Stem Cells Transl. Med. 2020, 9, 1007–1022. [Google Scholar] [CrossRef]
- Leng, Z.; Zhu, R.; Hou, W.; Feng, Y.; Yang, Y.; Han, Q.; Shan, G.; Meng, F.; Du, D.; Wang, S.; et al. Transplantation of ACE2(-) Mesenchymal Stem Cells Improves the Outcome of Patients with COVID-19 Pneumonia. Aging Dis. 2020, 11, 216–228. [Google Scholar] [CrossRef] [Green Version]
- Shu, L.; Niu, C.; Li, R.; Huang, T.; Wang, Y.; Huang, M.; Ji, N.; Zheng, Y.; Chen, X.; Shi, L.; et al. Treatment of severe COVID-19 with human umbilical cord mesenchymal stem cells. Stem Cell Res. Ther. 2020, 11, 361. [Google Scholar] [CrossRef] [PubMed]
- Meng, F.; Xu, R.; Wang, S.; Xu, Z.; Zhang, C.; Li, Y.; Yang, T.; Shi, L.; Fu, J.; Jiang, T.; et al. Human umbilical cord-derived mesenchymal stem cell therapy in patients with COVID-19: A phase 1 clinical trial. Signal Transduct. Target. Ther. 2020, 5, 172. [Google Scholar] [CrossRef]
- Armitage, J.; Tan, D.B.A.; Troedson, R.; Young, P.; Lam, K.-v.; Shaw, K.; Sturm, M.; Weiss, D.J.; Moodley, Y.P. Mesenchymal stromal cell infusion modulates systemic immunological responses in stable COPD patients: A phase I pilot study. Eur. Respir. J. 2018, 51, 1702369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, L.; Huang, H.; Lu, X.; Yan, X.; Jiang, X.; Xu, R.; Wang, S.; Zhang, C.; Yuan, X.; Xu, Z.; et al. Effect of human umbilical cord-derived mesenchymal stem cells on lung damage in severe COVID-19 patients: A randomized, double-blind, placebo-controlled phase 2 trial. Signal Transduct. Target. Ther. 2021, 6, 58. [Google Scholar] [CrossRef]
- Sengupta, V.; Sengupta, S.; Lazo, A.; Woods, P.; Nolan, A.; Bremer, N. Exosomes Derived from Bone Marrow Mesenchymal Stem Cells as Treatment for Severe COVID-19. Stem Cells Dev. 2020, 29, 747–754. [Google Scholar] [CrossRef]
- Chen, P.; Nirula, A.; Heller, B.; Gottlieb, R.L.; Boscia, J.; Morris, J.; Huhn, G.; Cardona, J.; Mocherla, B.; Stosor, V.; et al. SARS-CoV-2 Neutralizing Antibody LY-CoV555 in Outpatients with COVID-19. N. Engl. J. Med. 2021, 384, 229–237. [Google Scholar] [CrossRef]
- Dougan, M.; Nirula, A.; Azizad, M.; Mocherla, B.; Gottlieb, R.L.; Chen, P.; Hebert, C.; Perry, R.; Boscia, J.; Heller, B.; et al. Bamlanivimab plus Etesevimab in Mild or Moderate COVID-19. N. Engl. J. Med. 2021, 385, 1382–1392. [Google Scholar] [CrossRef]
- Xiang, H.R.; He, B.; Li, Y.; Cheng, X.; Zhang, Q.Z.; Peng, W.X. Bamlanivimab plus etesevimab treatment have a better outcome against COVID-19: A meta-analysis. J. Med. Virol. 2022, 94, 1893–1905. [Google Scholar] [CrossRef]
- Murchu, E.; Spillane, S.; Byrne, P.; O’Neill, M.; Harrington, P.; Ryan, M. Interventions in an Ambulatory Setting to Prevent Progression to Severe Disease in Patients with COVID-19: A Systematic Review. Ann. Pharmacother. 2022, 56, 309–318. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. Randomised Evaluation of COVID-19 Therapy (RECOVERY). Available online: https://clinicaltrials.gov/ct2/show/record/NCT04381936 (accessed on 11 January 2022).
- ClinicalTrials.gov. COVID-19 Study Assessing the Efficacy and Safety of Anti-Spike SARS CoV-2 Monoclonal Antibodies for Prevention of SARS CoV-2 Infection Asymptomatic in Healthy Adults and Adolescents Who Are Household Contacts to an Individual with a Positive SARS-CoV-2 RT-PCR Assay. Available online: https://clinicaltrials.gov/ct2/show/NCT04452318 (accessed on 4 November 2021).
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; Musser, B.J.; Soo, Y.; Rofail, D.; Im, J.; et al. REGN-COV2, a Neutralizing Antibody Cocktail, in Outpatients with COVID-19. N. Engl. J. Med. 2021, 384, 238–251. [Google Scholar] [CrossRef]
- O’Brien, M.P.; Forleo-Neto, E.; Musser, B.J.; Isa, F.; Chan, K.C.; Sarkar, N.; Bar, K.J.; Barnabas, R.V.; Barouch, D.H.; Cohen, M.S.; et al. Subcutaneous REGEN-COV Antibody Combination to Prevent COVID-19. N. Engl. J. Med. 2021, 385, 1184–1195. [Google Scholar] [CrossRef]
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; Xiao, J.; Hooper, A.T.; Hamilton, J.D.; Musser, B.J.; et al. REGEN-COV Antibody Combination and Outcomes in Outpatients with COVID-19. N. Engl. J. Med. 2021, 385, e81. [Google Scholar] [CrossRef]
- Ganesh, R.; Philpot, L.M.; Bierle, D.M.; Anderson, R.J.; Arndt, L.L.; Arndt, R.F.; Culbertson, T.L.; Destro Borgen, M.J.; Hanson, S.N.; Kennedy, B.D.; et al. Real-World Clinical Outcomes of Bamlanivimab and Casirivimab-Imdevimab Among High-Risk Patients With Mild to Moderate Coronavirus Disease 2019. J. Infect. Dis. 2021, 224, 1278–1286. [Google Scholar] [CrossRef] [PubMed]
- Du, L.; Yang, Y.; Zhang, X. Neutralizing antibodies for the prevention and treatment of COVID-19. Cell Mol. Immunol. 2021, 18, 2293–2306. [Google Scholar] [CrossRef] [PubMed]
- Cardwell, K.; O Murchu, E.; Byrne, P.; Broderick, N.; Walsh, K.A.; O’Neill, S.M.; Smith, S.M.; Harrington, P.; Ryan, M.; O’Neill, M. Pharmacological interventions to prevent COVID-19 disease: A rapid review. Rev. Med. Virol. 2022, 32, e2299. [Google Scholar] [CrossRef]
- Verderese, J.P.; Stepanova, M.; Lam, B.; Racila, A.; Kolacevski, A.; Allen, D.; Hodson, E.; Aslani-Amoli, B.; Homeyer, M.; Stanmyre, S.; et al. Neutralizing Monoclonal Antibody Treatment Reduces Hospitalization for Mild and Moderate Coronavirus Disease 2019 (COVID-19): A Real-World Experience. Clin. Infect. Dis. 2022, 74, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.J.; Banu, S.; Sasikala, M.; Parsa, K.V.L.; Sowpati, D.T.; Yadav, R.; Tallapaka, K.B.; Siva, A.B.; Vishnubhotla, R.; Rao, G.V.; et al. Effectiveness of REGEN-COV antibody cocktail against the B.1.617.2 (delta) variant of SARS-CoV-2: A cohort study. J. Intern. Med. 2022, 291, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Mutoh, Y.; Umemura, T.; Ota, A.; Okuda, K.; Moriya, R.; Tago, M.; Soejima, K.; Noguchi, Y.; Bando, T.; Ota, S.; et al. Effectiveness of monoclonal antibody therapy for COVID-19 patients using a risk scoring system. J. Infect. Chemother. 2022, 28, 352–355. [Google Scholar] [CrossRef]
- Sakurai, A.; Marshall, S.; Ogasawara, T.; Ogasawara, T.; Aoka, Y.; Sakura, H.; Uchigata, Y.; Ogawa, T. REGN-COV2 antibody cocktail in patients with SARS-CoV-2: Observational study from a single institution in Japan. J. Infect. Chemother. 2022, 28, 943–947. [Google Scholar] [CrossRef]
- Falcone, M.; Tiseo, G.; Valoriani, B.; Barbieri, C.; Occhineri, S.; Mazzetti, P.; Vatteroni, M.L.; Suardi, L.R.; Riccardi, N.; Pistello, M.; et al. Efficacy of Bamlanivimab/Etesevimab and Casirivimab/Imdevimab in Preventing Progression to Severe COVID-19 and Role of Variants of Concern. Infect. Dis. Ther. 2021, 10, 2479–2488. [Google Scholar] [CrossRef]
- Razonable, R.R.; Pawlowski, C.; O’Horo, J.C.; Arndt, L.L.; Arndt, R.; Bierle, D.M.; Borgen, M.D.; Hanson, S.N.; Hedin, M.C.; Lenehan, P.; et al. Casirivimab-Imdevimab treatment is associated with reduced rates of hospitalization among high-risk patients with mild to moderate coronavirus disease-19. EClinicalMedicine 2021, 40, 101102. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gonzalez-Rojas, Y.; Juarez, E.; Crespo Casal, M.; Moya, J.; Falci, D.R.; Sarkis, E.; Solis, J.; Zheng, H.; Scott, N.; et al. Early Treatment for COVID-19 with SARS-CoV-2 Neutralizing Antibody Sotrovimab. N. Engl. J. Med. 2021, 385, 1941–1950. [Google Scholar] [CrossRef] [PubMed]
- Kreuzberger, N.; Hirsch, C.; Chai, K.L.; Tomlinson, E.; Khosravi, Z.; Popp, M.; Neidhardt, M.; Piechotta, V.; Salomon, S.; Valk, S.J.; et al. SARS-CoV-2-neutralising monoclonal antibodies for treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 9, CD013825. [Google Scholar] [CrossRef] [PubMed]
- ACTIV-3/Therapeutics for Inpatients with COVID-19 (TICO) Study Group. Efficacy and safety of two neutralising monoclonal antibody therapies, sotrovimab and BRII-196 plus BRII-198, for adults hospitalised with COVID-19 (TICO): A randomised controlled trial. Lancet Infect. Dis. 2022, 22, 622–635. [Google Scholar] [CrossRef]
- Siemieniuk, R.A.; Bartoszko, J.J.; Diaz Martinez, J.P.; Kum, E.; Qasim, A.; Zeraatkar, D.; Izcovich, A.; Mangala, S.; Ge, L.; Han, M.A.; et al. Antibody and cellular therapies for treatment of covid-19: A living systematic review and network meta-analysis. BMJ 2021, 374, n2231. [Google Scholar] [CrossRef]
- Aggarwal, N.R.; Beaty, L.E.; Bennett, T.D.; Carlson, N.E.; Davis, C.B.; Kwan, B.M.; Mayer, D.A.; Ong, T.C.; Russell, S.; Steele, J.; et al. Real World Evidence of the Neutralizing Monoclonal Antibody Sotrovimab for Preventing Hospitalization and Mortality in COVID-19 Outpatients. medRxiv 2022. [Google Scholar] [CrossRef]
- Chen, X.; Zhao, B.; Qu, Y.; Chen, Y.; Xiong, J.; Feng, Y.; Men, D.; Huang, Q.; Liu, Y.; Yang, B.; et al. Detectable Serum Severe Acute Respiratory Syndrome Coronavirus 2 Viral Load (RNAemia) Is Closely Correlated with Drastically Elevated Interleukin 6 Level in Critically Ill Patients with Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 1937–1942. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Lan, S.H.; Lai, C.C.; Huang, H.T.; Chang, S.P.; Lu, L.C.; Hsueh, P.R. Tocilizumab for severe COVID-19: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2020, 56, 106103. [Google Scholar] [CrossRef]
- Cortegiani, A.; Ippolito, M.; Greco, M.; Granone, V.; Protti, A.; Gregoretti, C.; Giarratano, A.; Einav, S.; Cecconi, M. Rationale and evidence on the use of tocilizumab in COVID-19: A systematic review. Pulmonology 2021, 27, 52–66. [Google Scholar] [CrossRef]
- Rimland, C.A.; Morgan, C.E.; Bell, G.J.; Kim, M.K.; Hedrick, T.; Marx, A.; Bramson, B.; Swygard, H.; Napravnik, S.; Schmitz, J.L.; et al. Clinical characteristics and early outcomes in patients with COVID-19 treated with tocilizumab at a United States academic center. medRxiv 2020. [Google Scholar] [CrossRef]
- Khan, F.A.; Stewart, I.; Fabbri, L.; Moss, S.; Robinson, K.; Smyth, A.R.; Jenkins, G. Systematic review and meta-analysis of anakinra, sarilumab, siltuximab and tocilizumab for COVID-19. Thorax 2021, 76, 907–919. [Google Scholar] [CrossRef] [PubMed]
- Shakoory, B.; Carcillo, J.A.; Chatham, W.W.; Amdur, R.L.; Zhao, H.; Dinarello, C.A.; Cron, R.Q.; Opal, S.M. Interleukin-1 Receptor Blockade Is Associated with Reduced Mortality in Sepsis Patients with Features of Macrophage Activation Syndrome: Reanalysis of a Prior Phase III Trial. Crit. Care Med. 2016, 44, 275–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyriazopoulou, E.; Huet, T.; Cavalli, G.; Gori, A.; Kyprianou, M.; Pickkers, P.; Eugen-Olsen, J.; Clerici, M.; Veas, F.; Chatellier, G.; et al. Effect of anakinra on mortality in patients with COVID-19: A systematic review and patient-level meta-analysis. Lancet Rheumatol. 2021, 3, e690–e697. [Google Scholar] [CrossRef]
- Ivashkiv, L.B.; Donlin, L.T. Regulation of type I interferon responses. Nat. Rev. Immunol. 2014, 14, 36–49. [Google Scholar] [CrossRef] [Green Version]
- MacMicking, J.D. Interferon-inducible effector mechanisms in cell-autonomous immunity. Nat. Rev. Immunol. 2012, 12, 367–382. [Google Scholar] [CrossRef]
- Walz, L.; Cohen, A.J.; Rebaza, A.P.; Vanchieri, J.; Slade, M.D.; Dela Cruz, C.S.; Sharma, L. JAK-inhibitor and type I interferon ability to produce favorable clinical outcomes in COVID-19 patients: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 47. [Google Scholar] [CrossRef]
- Hunt, C.L.; Her, Y.F.; Law, L.A.; Bydon, M.; Nassr, A.; Smith, J.; Mauck, W.D.; Eldrige, J.S.; Malanga, G.A.; Qu, W. Five generations of cell preparation: A translational framework for categorizing regenerative stem cell therapies. J. Am. Acad. Regen. Med. 2017, 1, 1. [Google Scholar] [CrossRef]
- Loy, H.; Kuok, D.I.T.; Hui, K.P.Y.; Choi, M.H.L.; Yuen, W.; Nicholls, J.M.; Peiris, J.S.M.; Chan, M.C.W. Therapeutic Implications of Human Umbilical Cord Mesenchymal Stromal Cells in Attenuating Influenza A(H5N1) Virus-Associated Acute Lung Injury. J. Infect. Dis. 2019, 219, 186–196. [Google Scholar] [CrossRef]
- Miguez-Rey, E.; Choi, D.; Kim, S.; Yoon, S.; Sandulescu, O. Monoclonal antibody therapies in the management of SARS-CoV-2 infection. Expert Opin. Investig. Drugs 2022, 31, 41–58. [Google Scholar] [CrossRef]
- Taylor, P.C.; Adams, A.C.; Hufford, M.M.; de la Torre, I.; Winthrop, K.; Gottlieb, R.L. Neutralizing monoclonal antibodies for treatment of COVID-19. Nat. Rev. Immunol. 2021, 21, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Drug | Therapeutic Target | n | Study Type | Dose | Clinical Outcome | Ref. |
|---|---|---|---|---|---|---|
| Tocilizumab | Il 6 | 85 | Retrospective observational study | 400 mg i.v. once (n = 33), 324 mg s.c. once (n = 27), 800 mg i.v. (n = 2) | Survival rate increase favoring tocilizumab hazard ratio for death: 0.035; 95% confidence interval [CI], 0.004 to 0.347; p = 0.004 | [26] |
| Tocilizumab | Il 6 | 112 | Retrospective observational study | 8 mg/kg i.v. and repeated after 12 h (n = 21) | ICU admission and mortality favors tocilizumab OR 0.78; 95% CI between 0.06 and 9.34; p = 0.84 | [27] |
| Tocilizumab | Il 6 | 45 | Retrospective case–control study | 1 or 2 doses (n = 20) | Combined primary endpoint (death and/or ICU admission) was higher in the control group than in the Tocilizumab group (72% vs. 25%, p = 0.002) | [28] |
| Tocilizumab | Il 6 | 111 | Retrospective observational study | 8 mg/kg i.v. once (n = 42) | Fatality rate and levels of inflammatory markers increase in tocilizumab group 4 of 42 cases died with no fatalities in standard care group | [29] |
| Tocilizumab | Il 6 | 86 | Retrospective case–control study | 400 mg fixed dose or 8 mg/kg (n = 21) once or twice | Death rates decrease in tocilizumab group RR 0.472; 95% CI 0.449–0.497 | [30] |
| Tocilizumab | Il 6 | 59 | Retrospective case–control study | 8 mg/kg at discretion of the treating physicians, | Death, invasive ventilation reduction in tocilizumab group OR: 0.25 95%CI [0.05–0.95], p = 0.04 | [31] |
| Tocilizumab | Il 6 | 94 | Retrospective case–control study | N/A (n = 44) | Survival rate in tocilizumab group 61.36% versus 48% in the control group, p < 0.00001 | [32] |
| Tocilizumab | Il 6 | 25 | Retrospective observational study | Median total dose 5.7 mg/kg | 36% of patients were discharged alive from ICU by day 14 with no comparator | [33] |
| Tocilizumab | Il 6 | 65 | Prospective observational study | 400 mg fixed dose and 24-h 400 mg depending on clinical deterioration | At day 28 (16%) of the tocilizumab group died, compared to 33% of standard treatment group (p = 0.150). | [34] |
| Tocilizumab | Il 6 | 544 | Multicentered retrospective observational study | Tocilizumab 8 mg/kg (up to 800 mg) twice | Hazard ratio of death/mechanical ventilation favors tocilizumab adjusted (hazard ratio 0.61, 95% CI 0.40–0.92; p = 0.020) | [35] |
| Tocilizumab | Il 6 | 51 | Retrospective observational study | Tocilizumab 8 mg/kg and received (up to 400 mg) | Death/clinical improvement at 21 days in treated vs. Control favors control 76.5% (95% CI: 57.3–95.6) vs. 79.4% (95% CI: 56.0–100) | [36] |
| Tocilizumab | Il 6 | 15 | Retrospective observational study | 80−600 mg per time according to clinical worsening | Laboratory data and clinical course with no comparator; 20% of the patients died | [37] |
| Tocilizumab | Il 6 | 51 | Prospective nonrandomized study | Fixed first dose of 400 mg followed by 400 mg after 12 h | Mortality and clinical course with no comparator 30 day mortality: 27%. | [38] |
| Tocilizumab | Il 6 | 153 | Prospective observational study | Tocilizumab 8 mg/kg i.v. (up to 800 mg); second dose if elevated body mass | 87% survival at day 14 with no comparator | [39] |
| Tocilizumab | Il 6 | 63 | Prospective observational study | Tocilizumab i.v. 8 mg/kg | 11% Mortality at day 14 no comparator | [40] |
| Tocilizumab | Il 6 | 100 | Prospective observational study | Tocilizumab 8 mg/kg (up to 800 mg) twice | Clinical outcome at day 10: 77% improved or stabilized and 23% worsened no comparator | [41] |
| Tocilizumab | Il 6 | 21 | Retrospective observational study | Tocilizumab 4–8 mg/kg (up to 800 mg) twice | Mean discharge day 15.1 without comparator | [42] |
| Tocilizumab | Il 6 | 89 | Retrospective observational study | Tocilizumab 400 mg single dose | Descriptive deaths, mechanical ventilation and discharged with no comparator; 63/72 not mechanically ventilated patients were discharged | [43] |
| Tocilizumab | Il 6 | 186 | Retrospective observational study | Tocilizumab single dose of 400−600 mg | 51 patients were intubated or dead at day 15 with no comparator. | [44] |
| Tocilizumab | Il 6 | 547 | Retrospective observational study | Tocilizumab: 400 mg some with a second dose of 800 mg | The unadjusted 30 day mortality favored tocilizumab (HR, 0.76, 95% CI, 0.57−1.00) | [45] |
| Tocilizumab | Il 6 | 60 | Nonrandomized prospective observational study | Tocilizumab 400 mg single dose according to clinical response redosing possibility | Bacterial and fungal infections | [46] |
| Tocilizumab | Il 6 | 1229 | Multicentered retrospective observational study | Tocilizumab median dose 600 mg, second dosing according to clinical response | Tocilizumab associated with higher risk of death (HR 1.53,95% CI 1.20–1.96, p = 0.001) | [47] |
| Tocilizumab | Il 6 | 171 | Retrospective observational study | Tocilizumab 400 mg/24 for patients with ≤75 kg and 600 mg/24 for patients with >75 kg with second and third dosing according to clinical response | Description of frequency for composite ICU admission or death favoring Tocilizumab (10.3% vs. 195 27.6%, p = 0.005) | [48] |
| Tocilizumab | Il 6 | 1221 | Multicentered phase 2 clinical trial | Tocilizumab 8 mg/kg and second dose according to clinical response | Lower lethality rates at 14 and 30 days (15.6% and 20.0%) among the treated with tocilizumab | [49] |
| Tocilizumab | Il 6 | 145 | Multicentered retrospective observational study | Tocilizumab 400–800 mg single dose | Descriptive study of mortality with no comparator 43.8% of the population discharged and 29.3% died | [50] |
| Tocilizumab | Il 6 | 246 | Retrospective observational study | Tocilizumab 400 mg single dose | Composite of all-cause mortality and invasive mechanical ventilation favoring tocilizumab (HR = 0.49 (95% CI 0.3−0.81), p = 0.005) | [51] |
| Tocilizumab | Il 6 | 82 | Prospective and retrospective observational | Tocilizumab 400 mg single dose with second dose according to clinical response; 600 mg if >75 kg | Mortality at 7 days of tocilizumab start; 26.8% of all patients died (no comparator) | [52] |
| Tocilizumab | Il 6 | 154 | Single center retrospective observational | Tocilizumab 8 mg/kg single dose | Survival probability post intubation favoring tocilizumab in 3 models: model A HR 0.54 (95% CI 0.29, 1.00) | [53] |
| Tocilizumab | Il 6 | 29 | Single center prospective clinical trial | Tocilizumab 8 mg/kg single dose | Classified as responders or non-responders (secondary analysis described correlation with miR-146a marker) 55.17% of patients where responders | [54] |
| Tocilizumab | Il 6 | 130 | Prospective multicenter randomized clinical trial | Tocilizumab 8 mg/kg two doses | Risk of mechanical ventilation or death at day 28 favored tocilizumab HR 0.58 (90% CrI, 0.30 to 1.09). | [55] |
| Tocilizumab | Il 6 | 126 | Prospective randomized clinical trial | Tocilizumab 8 mg/kg up to a maximum of 800 mg | Clinical worsening ratio showed worst outcome in tocilizumab group (risk ratio, 1.05; 95%CI, 0.59–1.86). | [56] |
| Tocilizumab | Il 6 | 126 | Prospective nonrandomized clinical trial | Tocilizumab 324–486 mg according to body weight single dose | Mortality rates with no comparator: by day 14 of the study, 4.65% (4/86) of severe patients and 50.00% (20/40) of critical patients died. | [57] |
| Tocilizumab | Il 6 | 42 | Prospective nonrandomized clinical trial | Tocilizumab 400 mg single dose | Mortality rates with no comparator: 35 patients (83.33%) showed clinical improvement by day 28 | [58] |
| Tocilizumab | Il 6 | 418 | Matched cohort study | Tocilizumab up to 3 doses ranging from 400 mg to 600 mg according to clinical evaluation | Inspired oxygen fraction/saturation 48 h post treatment showed no difference, logistic regression didnot show an effect of tocilizumab on mortality (OR 0.99; p = 0.990). | [59] |
| Tocilizumab | IL 6 | 6837 | Meta Analysis | Single IV dose of 8 mg/kg (maximum 800 mg) initially according to clinical evaluation | Reduce in risk of mechanical ventilation at 28–30 days (0.79) and lowers risk of mortality | [60] |
| Tocilizumab | IL 6 | 163 | Observational cohort study | 2 doses of 600 mg on consecutive days | Benefit in the combined treatment with TCZ and CS may have a potential role in reducing mortality | [61] |
| Tocilizumab | IL 6 | 567 | Meta Analysis | 400 mg single dose | Risk of mortality similar in treatment with TCZ alone and comined therapy 0.74 (95% CI: 0.36–1.50) | [62] |
| Tocilizumab | IL 6 | 99 | Prospective cohort study | 400 mg single dose | There were no significant differences in mortality compared to the control group (34% vs. 34%, p = 0,98) | [63] |
| Tocilizumab | IL6 | 135 | Prospective nonrandomized clinical trial | 625 mg (mean dose) on 9 consecutive days | No additional survival benefit with TCZ 29% vs. 35% with RR = 0.79 and 95% CI: 0.70–0.89, p = 0.01 | [64] |
| Tocilizumab | IL 6 | 514 | Observational retrospective study | 400 mg single dose | Significant difference in length of stay of patients with invasive mechanical ventilation (73.1%) | [65] |
| Tocilizumab | IL 6 | 100 | Phase 2, open-label, randomized study | 4 mg/Kg and 8 mg/kg | There was no clear difference between 2 treatment groups in the odds ratio for mortality at day 28 | [66] |
| Tocilizumab | IL 6 | 23 | Retrospective, observational study | 400 mg single dose | Rapid clinical improvement with TCZ treatment in the severely ill COVID-19 patients, as opposed to the case in the critically ill patients | [67] |
| Tocilizumab | IL 6 | 114 | Prospective study | 6 mg/kg | At the time point that PaO2/FiO2 < 200 was observed, improved survival (16.1%) than in the usual care group (32.8% | [68] |
| Tocilizumab | IL 6 | 87 | Randomised, controlled | 6 mg/kg | TCZ associated with a decrease mortality (9.52%) and reduce the invasive mechanical ventilator | [69] |
| Tocilizumab | IL 6 | 129 | Retrospective cohort study | 4–8 mg/kg | In patients with severe or critical COVID-19 was significantly associated with better survival compare with control group (21.6% vs. 42.3% respectively; p = 0.015) | [70] |
| Siltuximab | IL 6 | 218 | Observational cohort study | Siltuximab 2 doses 11 mg/kg | 30 day mortality rate favors Siltuximab (HR 0.462, 95% CI 0.221–0.965); p = 0.0399). | [71] |
| Sarilumab | Il 6 | 28 | Observational cohort study | Sarilumab 400 mg single dose | Clinical improvement and lethality rate showed no differences; 61% of patients treated with sarilumab experienced clinical improvement and 7% died | [72] |
| Sarilumab | Il 6 | 803 | Prospective nonrandomized clinical trial | Sarilumab 400 mg single dose | Descriptive Hospital mortality: 28.0% (98/350) for tocilizumab, 22.2% (10/45) for sarilumab and 35.8% (142/397) for control. | [73] |
| Sarilumab | Il 6 | 53 | Prospective nonrandomized clinical trial | Sarilumab 400 mg two doses | Descriptive with Sarilumab no comparator; global resolution rate of 83.0% (89.7% in medical wards and 64.3% in ICU) and an overall mortality rate of 5.7%. | [74] |
| Anakinra | IL 1 | 22 | Observational cohort study | Anakinra 300 mg for two 5 days tapered to 200 mg for 2 days | Descriptive outcomes regarding mechanical ventilation, death, and mean days to discharge (mean days in control group 9.5 and 5 days in Anakinra group) | [75] |
| Anakinra | IL 1 | 96 | Observational cohort study with historical controls | Anakinra 100 mg twice a day for 72 h, then 100 mg daily for 7 days | Composite endpoint of admission to the ICU for invasive mechanical ventilation or death (HR 0.22 [95% CI 0.10–0.49]; p = 0.0002) | [76] |
| Anakinra | IL 1 | 153 | Randomized control trial | Anakinra 400 mg/day on days 1–3 then 200 mg on day 4, and 100 mg once on day 5 | Patient death or need of mechanical ventilation HR 0.97; 90% CrI 0.62 to 1.52 | [77] |
| Anakinra | IL 1 | 120 | Observational cohort study | High dose anakinra non specified | Adjusted risk of death comparing anakinra group with control HR, 0.18, 95% CI, 0.07–0.50, p = 0.001, | [78] |
| Anakinra | IL 1 | 392 | Observational cohort study with historical controls | Anakinra 10 mg/kg/day until clinical benefit | Anakinra group with reduced mortality risk (hazard ratio [HR] 0.450, 95% CI 0.204–0.990, p = 0.047) | [79] |
| Anakinra | IL 1 | 128 | Observational cohort study | Anakinra 100 mg every 8 h for 3 days, with tapering | Mortality reduction favoring anakinra adjusted [HR] = 0.26; p < 0.001 | [80] |
| Anakinra | IL 1 | 21 | Observational prospective cohort | Anakinra 300 mg initial dose following 100 mg every 6 h | In the anakinra group, 28 day mortality was 19% vs. 18% in the control group (p = 0.87). | [81] |
| Anakinra | IL 1 | 130 | Observational prospective cohort | Anakinra 100 mg once daily for 10 days | Reduction in 30 day mortality with anakinra (hazard ratio 0.49; 95% CI 0.25–0.97) | [82] |
| Anakinra | IL 1 | 69 | Observational cohort study with historical controls | Anakinra 100 mg twice daily for 3 days, followed by 100 mg daily for a maximum of 7 days | Hospital death occurred in 13 (29%) of the anakinra-treated group and 11 (46%) of the historical cohort (p = 0.082). | [83] |
| Anakinra | IL 1 | 93 | Observational retrospective Cohort studies | Anakinra minimum use of 100 mg every 12 h (depending on clinical condition and comorbidities) | Survival rate of anakinra vs Tocilizumab: HR 0.46, 95% confidence interval 0.18–1.20 | [84] |
| Anakinra | IL 1 | 27 | Observational retrospective Cohort studies | Anakinra 100 mg every 6 h for at least 3 days, tapering until 7 days | Descriptive of only 9 treated patients with matched cohort of tocilizumab treated patients (9 survivals) | [85] |
| Anakinra | IL 1 | 120 | Prospective nonrandomized clinical trial | 100 mg anakinra daily for 5 days | Patient mortality without significant difference OR of 0.9 (95%CI [0.80–1.01], p = 0.067) | [86] |
| Anakinra | IL 1 | 606 | Multicentered, double blind, randomized, clinical trial | 100 mg anakinra daily for 7–10 days | Risk of death at day 28 hazard ratio = 0.45, 95% CI 0.21–0.98, p = 0.045 | [87] |
| Anakinra | IL 1 | 112 | Observational cohort study with matched controls | 100 mg four times a day, if managed in a regular ward, or 200 mg three times daily if managed in the intensive care unit | Anakinra as a survival predictor at day 28 odds ratio: 3.2; 95% confidence interval, 1.47–7.17 | [88] |
| Anakinra | IL 1 | 30 | Randomized clinical trial | 100 mg daily for a median 5 (3–9) days | A significant reduction of 50% in length of hospital stay compared with control (9.50 ± 4.45 vs. 19.00 ± 12.04, p = 0.043). A significant reduction in mortality (odds ratio [OR] = 0.32 [95% confidence interval, CI: 0.20–0.51] | [89] |
| Canakinumab | IL 1 | 88 | Observational prospective cohort | Canakinumab 300 mg single dose | Descriptive outcome with no comparator, overall survival at 1 month was 79.5% (95% CI 68.7–90.3) | [90] |
| Canakinumab | IL 1 | 34 | Observational prospective cohort | Canakinumab 300 mg single dose | Descriptive oxygen support requirement at 3 time points: reduction in oxygen flow in patients treated with canakinumab (−28.6% at T1 vs. T0 and −40.0% at T2 vs. T1). | [91] |
| Canakinumab | IL 1 | 454 | Randomized Clinical trial | Canakinumab 450–750 mg single dose | Non-significant mortality risk reduction with Canakinumab odds ratio of 0.67 (95%CI, 0.30 to 1.50) | [92] |
| Canakinumab | IL 1 | 48 | Prospective case control | Canakinumab 150 mg at day 1 and day 7 | Descriptive outcome, survival at 60 days was 90.0% (95% CI 71.9–96.7) in patients treated with canakinumab and 73.3% (95% CI 43.6–89.1) | [93] |
| Interferon β-1a | interferon β-1a | 81 | Randomized Clinical trial | 12 million IU/mL three times a week for two weeks | Mortality reduction in interferon group at day 28 (OR, 6.65; 95% CI, 1.67 to 26.45) adjusted for confounders. | [94] |
| Interferon β-1b | interferon β-1b | 256 | Retrospective cohort | 250 mcg on alternate days | Descriptive outcome mortality rate was 24.6% (63/256). 22 patients (20.8%) in the interferon group and 41 (27.3%) in the control group (p = 0.229) | [95] |
| Interferon β-1b | interferon β-1b | 127 | Randomized Clinical trial | Three doses of 8 million IU on alternate days | Combination group of interferon was independent risk factor for nasopharyngeal swaps negativization HR 4.27 [95% CI 1.82–10.02], p = 0.0010; no deaths in either group | [96] |
| Interferon α-2b | interferon α-2b | 814 | Multicenter prospective observational study | 3 million IU 3 times per week, for 2 weeks | Descriptive outcome: The overall case fatality rate was 2.95% of the infected population. The case fatality rate for patients treated with IFN-a2b was 0.92 (p < 0.01) | [97] |
| Interferon α-2b | interferon α-2b | 446 | Retrospective multicenter cohort study | Different regimes in each center (non-specified) | IFN therapy is univariably associated with lower mortality (odds ratio [OR] = 0.18, p = 0.029) | [98] |
| Interferon α-2b | interferon α-2b | 77 | Prospective observational study | 5 mIU in inhaled aerosol each day | Accelerated viral clearance from the upper respiratory tract in patients who received IFN-a2b treatment (20.4 days, p = 0.002) mean difference of 7 days with control group | [99] |
| Interferon β-1b | interferon β-1b | 80 | Randomized clinical trial | 250 µg on alternate days | All-cause 28 day mortality was 6.06% and 18.18% in the IFN and control groups, respectively (p = 0.12) | [100] |
| Peginterferon lambda | interferon lambda | 60 | Randomized Clinical trial | 180 mcg single dose | Favors faster viral clearance with pegylated interferon 2.42 log copies per mL at day 7 (p =0.0041) | [101] |
| Mesenchymal stem cells | Mesenchymal stem cells | 200 | Meta analysis | Variable according to study and type of mesenchymal stem cells | Favor treatment with mesenchymal cells without achieving significance: OR 0.63, 95% confidence interval 0.21–1.93 | [102] |
| Mesenchymal stem cells | Mesenchymal stem cells | 10 | Nonrandomized pilot clinical trial | 1 × 106 cells per kilogram of weight single transplantation | Descriptive outcome favoring treatment group: none of the patients in the mesenchymal stem cell group died | [103] |
| Mesenchymal stem cells (umbilical cord) | Mesenchymal stem cells | 41 | Randomized clinical trial | 2 × 106 cells per kilogram of weight single transplantation | Descriptive outcome favoring treatment group: none of the patients in the mesenchymal stem cell group died | [104] |
| Mesenchymal stem cells (umbilical cord) | Mesenchymal stem cells | 18 | Nonrandomized clinical trial | Three transplantations of 3 × 107 cells per infusion | Descriptive outcome: mechanical ventilation was required in one patient in the treatment group compared with four in the control group | [105] |
| Mesenchymal stem cells | Mesenchymal stem cells | 25 | Retrospective observational study | 1 × 106 mononuclear cells per kilogram of weight per infusion every 5 days | No differences comparing Mesenchymal cell treatment and placebo group (inflammatory markers surrogate did not show any differences either) | [106] |
| Mesenchymal stem cells | Mesenchymal stem cells | 100 | Randomized double blind clinical trial | Three transplantations of 4 × 107 cells per infusion | Lung function in 6 min walking test at day 28 favors mesenchymal cell treatment median 420 m vs. 403 m in control group p = 0.057 | [107] |
| Exosomes Derived from Bone Marrow Mesenchymal Stem Cells | Mesenchymal stem cells | 27 | Prospective nonrandomized cohort study | 15 mL intravenous dose of ExoFlo single dose | Descriptive outcome with no comparator with overall survival rate in the study of 83%. | [108] |
| Bamlanivimab | Spike protein | 467 | Randomized, double-blind, placebo-controlled, single-dose trial | 700 mg (101 patients), 2800 mg (107 patients), or 7000 mg (101 patients) | Descriptive outcome: At day 29, the percentage of patients who were hospitalized with COVID-19 was 1.6% (5 of 309 patients) in the LY-CoV555 group and 6.3% (9 of 143 patients) in the placebo group | [109] |
| Bamlanivimab plus Etesevimab | Spike protein | 452 | Randomized, double blinded clin-ical tria | Bamlanivimab and etesevimab, 2800 mg of each given intravenously | Descriptive outcome: By day 29, a total of 11 of 518 patients (2.1%) in the bamlanivimab–etesevimab group had a COVID-19-related hospitalization or death from any cause, as compared with 36 of 517 patients (7.0%) in the placebo group (absolute risk difference, −4.8 percentage points; 95% confidence interval [CI], −7.4 to −2.3; relative risk difference, 70%; p < 0.001) | [110] |
| Bamlanivimab plus Etesevimab | Spike protein | 14,461 | Meta analysis | Variable according to study | Favor treatment with Bamlanivimab plus Etesevimab; Bmlanivimab may help outpatients to prevent hospitalizationor emergency department visits (RR 0.41, 95%CI 0.29−0.58), reduce ICU admission (RR 0.47, 95%CI 0.23−0.92), and mortality (RR 0.32, 95%CI 0.13−0.77)from the disease. The combination of bamlanivimab and etesevimab may have agreater potential for positive treatment outcomes. | [111] |
| Bamlanivimab plus Etesevimab | Spike protein | 577 | Systematic review | 2800 mg IV | Bamlanivimab 2800 mg plus etesevimab 2800 mg: significant difference in hospitalizations/emergency department visit versus placebo; absolute risk difference was −4.9% (95% CI: −8.9% to −0.8%; p = 0.049) | [112] |
| Casirivimab/imdevimab | Spike protein | 9785 | Randomized, double-blind, placebo-controlled clinical trial | 8000 mg IV infusion | Favor treatment casirivimab/imdevimab in addition to usual care with 20% reduction in all-cause mortality (rate ratio 0.80; 95% CI 0.70–0.91; p = 0.001); 17% lower relative risk of progressing to invasive mechanical ventilation or death (composite endpoint) with casirivimab/imdevimab plus usual care than with usual care alone among seronegative patients not on such ventilation at baseline (30% vs. 37% of patients; relative risk ratio 0.83; 95% CI 0.75–0.92); | [113] |
| Casirivimab/ imdevimab | Spike protein | 2067 | Randomized, double-blind, placebo-controlled, phase 3 trial | Subcutaneous dose of 1200 mg | Casirivimab/imdevimab was effective in preventing symptomatic and asymptomatic SARS-CoV-2 infection, a relative risk reduction of 81.4% (odds ratio [OR] 0.17; 95% CI 0.09–0.33; p < 0.001). | [114] |
| Casirivimab/ imdevimab | Spike protein | 275 | Double-blind, phase 1–3 trial | 2.4 g of REGN-COV2, or 8.0 g of REGN-COV2 | The REGN-COV2 antibody cocktail reduced viral load, with a greater effect in patients whose immune response had not yet been initiated or who had a high viral load at baseline. | [115] |
| Casirivimab/ imdevimab | Spike protein | 1505 | Randomized, double-blind, placebo-controlled, phase 3 trial | 1200 mg of REGEN-COV | Subcutaneous REGEN-COV prevented symptomatic COVID-19 and asymptomatic SARS-CoV-2 infection in previously uninfected household contacts of infected persons. Among the participants who became infected, REGEN-COV reduced the duration of symptomatic disease and the duration of a high viral load. | [116] |
| Casirivimab/ imdevimab | Spike protein | 2696 | Adaptive trial | 2 groups: 2400-mg group and 1200-mg group | EGEN-COV reduced the risk of COVID-19-related hospitalization or death from any cause, and it resolved symptoms and reduced the SARS-CoV-2 viral load more rapidly than placebo | [117] |
| Casirivimab/ imdevimab | Spike protein | 3596 | Observational study | N.S. | Descriptive outcome: no significant difference in all-cause and COVID-19-related hospitalization rates between bamlanivimab and casirivimab-imdevimab (adjusted hazard ratios [95% confidence interval], 1.4 [0.9–2.2] and 1.6 [0.8–2.7], respectively). | [118] |
| Casirivimab/ imdevimab | Spike protein | Systematic review | N.S. | Prevention of COVID-19 progression from asymptomatic to symptomatic disease in early SARS-CoV-2 infection; patients with mild-to-moderate COVID-19 exhibited reduced hospital utilization after receiving REGN-COV2 treatment within a few days of symptom onset, and a low-dose REGN-COV2 infusion has been shown to improve COVID-19 symptoms; Subcutaneously injected REGN-COV2 prevented SARS-CoV-2 infection and the presence of COVID-19 symptoms in high-risk individuals who had close contact with SARS-CoV-2-infected persons. | [119] | |
| Casirivimab/ imdevimab | Spike protein | 2067 | Review | Subcutaneous injection of 1200 mg REGEN-COV | The combination of monoclonal antibodies significantly reduced the incidence of symptomatic and asymptomatic SARS-CoV-2 infection, viral load, duration of symptomatic disease and the duration of a high viral load | [120] |
| Bamlanivimab or Casirivimab/ imdevimab | Spike protein | 707 | Observational study | N.S. | Patients receiving NmAb infusion had significantly lower hospitalization rates (5.8% vs. 11.4%, p < 0.0001), shorter length of stay if hospitalized (mean, 5.2 vs. 7.4 days; p = 0.02), and fewer ED visits within 30 days post-index (8.1% vs. 12.3%, p = 0.003) than controls. Hospitalization-free survival was significantly longer in NmAb patients compared with controls (p < 0.0001). There was a trend towards a lower hospitalization rate among patients who received NmAbs within 2–4 days after symptom onset. | [121] |
| Bamlanivimab or Casirivimab/ | Spike protein | 285 | Single-center prospective observational cohort study | N.S. | Favoring cocktail group: Assessing all the symptoms, the number of symptomatic individuals on Day 7 was significantly lower in the cocktail group than in the SOC group (23/108 [21.30%] vs. 39/78 [50.0%]; p = 0.0001) while the remaining patients in each of the groups recovered completely. (cocktail group: casirivimab/imdevimab; SOC: standard-of-care) | [122] |
| imdevimab | Spike protein | 115 | Obervational study | N.S. | Administering monoclonal antibody therapy for high-risk patients with COVID-19 using a regional severity prediction scoring system notably reduced the number of hospitalisations and severe cases | [123] |
| Casirivimab/ imdevimab | Spike protein | 108 | Retrospective cohort study | 120 mg casirivimab and 120 mg imdevimab | Descriptive outcome: After the treatment, the number of patients with COVID-19-related hospitalization, due to decreased SpO2, was 12, accounting for 11% of the enrolled patients who received REGN-COV2. | [124] |
| Casirivimab/ imdevimab | Spike protein | 165 | Observational prospective study | Bamlanivimab (700 mg) com-bined with etesevimab (1400 mg) or casirivimab (1200 mg)combined with imdevimab (1200 mg). | In the Gamma viral strain group, a higher proportion of patients treated with bamlanivimab/etesevimab met the primary endpoint (a composite of hospitalization or death within 30 days from mAbs infusion) compared to those receiving casirivimab/imdevimab (55% vs. 17.4%, p = 0.013). | [125] |
| Casirivimab/ imdevimab | Spike protein | 696 | Retrospective cohort | One hour infusion of casirivimab (1200-mg dose) and imdevimab (1200-mg dose) | Patients who received casirivimab–imdevimab had significantly lower all-cause hospitalization rates at day 14 (1.3% vs. 3.3%; Absolute Difference: 2.0%; 95% confidence interval (CI): 0.5–3.7%), day 21 (1.3% vs. 4.2%; Absolute Difference: 2.9%; 95% CI: 1.2–4.7%), and day 28 (1.6% vs. 4.8%; Absolute Difference: 3.2%; 95% CI: 1.4–5.1%) | [126] |
| Sotrovimab | Spike protein | 583 | Ongoing, multicenter, double-blind, trial | 500 mg | A total of (1%) in the sotrovimab group, as compared with 21 patients (7%) in the placebo group, had disease progression leading to hospitalization or death (relative risk reduction, 85%; 97.24% confidence interval, 44 to 96; p = 0.002). The clinical progression of COVID-19 at Day 29 in recipients of sotrovimab was reduced by 85% compared with the placebo group (p = 0.002) | [127] |
| Sotrovimab | Spike protein | n/a | Systematic review | N.S. | Treatment with sotrovimab may reduce the number of participants with oxygen requirement (RR 0.11, 95% CI 0.02 to 0.45), hospital admission or death by day 30 (RR 0.14, 95% CI 0.04 to 0.48), grades 3–4 AEs (RR 0.26, 95% CI 0.12 to 0.60), SAEs (RR 0.27, 95% CI 0.12 to 0.63) and may have little or no effect on any grade AEs (RR 0.87, 95% CI 0.66 to 1.16). | [128] |
| Sotrovimab | Spike protein | 546 | Multinational, double-blind, randomised, placebo-controlled, clinical trial | 500 mg | Neither sotrovimab nor BRII-196 plus BRII-198 showed efficacy for improving clinical outcomes among adults hospitalised with COVID-19. At day 5, neither the sotrovimab group nor the BRII-196 plus BRII-198 group had significantly higher odds of more favourable outcomes than the placebo group on either the pulmonary scale (adjusted odds ratio sotrovimab 1.07 [95% CI 0.74-1.56]; BRII-196 plus BRII-198 0.98 [95% CI 0.67–1.43]) or the pulmonary-plus complications scale (sotrovimab 1.08 [0.74–1.58]; BRII-196 plus BRII-198 1.00 [0.68–1.46]) | [129] |
| Sotrovimab | Spike protein | n/a | Systematic review and network meta-analysis | NS | Patients with non-severe disease randomised to antiviral monoclonal antibodies had lower risk of hospitalisation than those who received placebo: sotrovimab (OR 0.17 (0.04 to 0.57); RD −4.8%; low certainty). They did not have an important impact on any other outcome. | [130] |
| Sotrovimab | Spike protein | 10,036 | Observational cohort study | NS | Sotrovimab treatment was associated with a 63% decrease in the odds of all-cause hospitalization (raw rate 2.1% versus 5.7%; adjusted OR 0.37, 95% CI 0.19–0.66) and an 89% decrease in the odds of all-cause 28 day mortality (raw rate 0% versus 1.0%; adjustced OR 0.11, 95% CI 0.0–0.79), and may reduce respiratory disease severity among those hospitalized. | [131] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arias, M.; Oliveros, H.; Lechtig, S.; Bustos, R.-H. Biologics in COVID-19 So Far: Systematic Review. Pharmaceuticals 2022, 15, 783. https://doi.org/10.3390/ph15070783
Arias M, Oliveros H, Lechtig S, Bustos R-H. Biologics in COVID-19 So Far: Systematic Review. Pharmaceuticals. 2022; 15(7):783. https://doi.org/10.3390/ph15070783
Chicago/Turabian StyleArias, Milton, Henry Oliveros, Sharon Lechtig, and Rosa-Helena Bustos. 2022. "Biologics in COVID-19 So Far: Systematic Review" Pharmaceuticals 15, no. 7: 783. https://doi.org/10.3390/ph15070783
APA StyleArias, M., Oliveros, H., Lechtig, S., & Bustos, R.-H. (2022). Biologics in COVID-19 So Far: Systematic Review. Pharmaceuticals, 15(7), 783. https://doi.org/10.3390/ph15070783