
Cardiac 123I-mIBG Imaging in Heart Failure


Abstract
:
1. Introduction
2. Cardiac 123I-mIBG Imaging
2.1. Patient Preparation
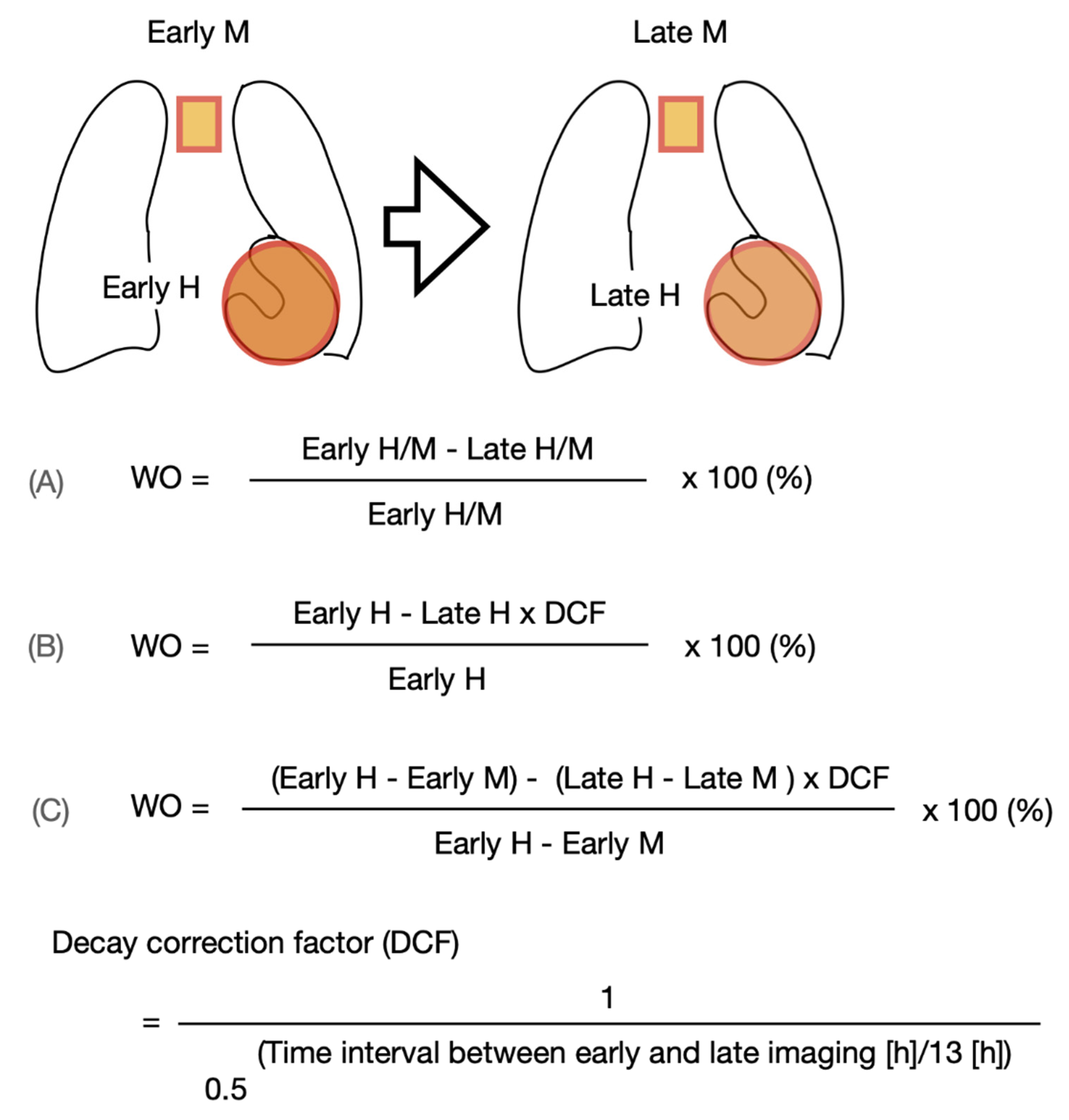
2.2. Planar 123I-mIBG Acquisition and Analysis
2.3. SPECT 123I-mIBG Acquisition and Analysis
2.4. Standardization
2.5. Challenges
3. Cardiac 123I-mIBG Imaging in CHF
3.1. Alteration of Cardiac Sympathetic Activity by Medical Heart Failure Therapy
3.2. Cardiac 123I-mIBG Imaging as a Predictor of Morbidity and Mortality in CHF
3.3. Cardiac 123I-mIBG Imaging as a Predictor for Arrhythmia and ICD Therapy in CHF
3.4. Cardiac 123I-mIBG Imaging as Predictor of CRT Response
4. Risk Stratification Using Cardiac 123I-mIBG Imaging
5. Cardiac 123I-mIBG Imaging in Takotsubo Cardiomyopathy
6. Clinical Acceptation of Cardiac 123I-mIBG Imaging
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 123I-mIBG | 123I-meta-iodobenzylguanidine |
| ACE-I | angiotensin-converting enzyme inhibitors |
| ACS | acute coronary syndrome |
| ARB | angiotensin receptor blockers |
| ARNI | angiotensin-receptor neprilysine-inhibitor |
| BNP | brain natriuretic peptide |
| β-AR | β-adrenergic receptors |
| CHF | chronic heart failure |
| CZT | Cadmium–Zinc–Telluride |
| FBBG | Flubrobenguane |
| ICD | implantable cardioverter defibrillator |
| HED | hydroxyephedrine |
| HFPEF | heart failure with preserved ejection fraction |
| HFREF | heart failure with reduced ejection fraction |
| HRV | heart rate variability |
| H/M | heart-to-mediastinum ratio |
| LBBB | left bundle branch block |
| LVEF | left ventricular ejection fraction |
| LVESV | left ventricular end systolic volume |
| MAO | monoamine oxidase |
| MPI | myocardial perfusion imaging |
| NE | norepinephrine |
| NET | norepinephrine transporter |
| NYHA | New York heart association |
| OMT | optimal medical therapy |
| ROI | region-of-interest |
| SCD | sudden cardiac death |
| SDS | summed defect score |
| SGLT2 inhibitor | sodium-glucose cotransporter-2 inhibitor |
| SPECT | single-photon emission tomography |
| TCM | takotsubo cardiomyopathy |
| WO | washout |
References
- Verschure, D.O.; van Eck-Smit, B.L.F.; Somsen, G.A.; Knol, R.J.J.; Verberne, H.J. Cardiac sympathetic activity in chronic heart failure: Cardiac 123I-mIBG scintigraphy to improve patient selection for ICD implantation. Neth. Heart J. 2016, 24, 701–708. [Google Scholar] [CrossRef] [Green Version]
- Hasking, G.J.; Esler, M.D.; Jennings, G.L.; Burton, D.; Johns, J.A.; Korner, P.I. Norepinephrine spillover to plasma in patients with congestive heart failure: Evidence of increased overall and cardiorenal sympathetic nervous activity. Circulation 1986, 73, 615–621. [Google Scholar] [CrossRef] [Green Version]
- Cohn, J.N.; Levine, T.B.; Olivari, M.T.; Garberg, V.; Lura, D.; Francis, G.S.; Simon, A.B.; Rector, T. Plasma Norepinephrine as a Guide to Prognosis in Patients with Chronic Congestive Heart Failure. N. Engl. J. Med. 1984, 311, 819–823. [Google Scholar] [CrossRef] [Green Version]
- Merlet, P.; Delforge, J.; Syrota, A.; Angevin, E.; Mazière, B.; Crouzel, C.; Valette, H.; Loisance, D.; Castaigne, A.; Randé, J.L. Positron emission tomography with 11C CGP-12177 to assess beta-adrenergic receptor concentration in idiopathic dilated cardiomyopathy. Circulation 1993, 87, 1169–1178. [Google Scholar] [CrossRef] [Green Version]
- Bristow, M.R.; Ginsburg, R.; Minobe, W.; Cubicciotti, R.S.; Sageman, W.S.; Lurie, K.; Billingham, M.E.; Harrison, D.C.; Stinson, E.B. Decreased Catecholamine Sensitivity and β-Adrenergic-Receptor Density in Failing Human Hearts. N. Engl. J. Med. 1982, 307, 205–211. [Google Scholar] [CrossRef]
- Esler, M.; Kaye, D.; Lambert, G.; Esler, D.; Jennings, G. Adrenergic Nervous System in Heart Failure. Am. J. Cardiol. 1997, 80 (Suppl. 1), 7L–14L. [Google Scholar] [CrossRef]
- Lahiri, M.K.; Kannankeril, P.J.; Goldberger, J.J. Assessment of Autonomic Function in Cardiovascular Disease: Physiological Basis and Prognostic Implications. J. Am. Coll. Cardiol. 2008, 51, 1725–1733. [Google Scholar] [CrossRef] [Green Version]
- Werner, R.A.; Rischpler, C.; Onthank, D.; Lapa, C.; Robinson, S.; Samnick, S.; Javadi, M.; Schwaiger, M.; Nekolla, S.G.; Higuchi, T. Retention Kinetics of the 18F-Labeled Sympathetic Nerve PET Tracer LMI1195: Comparison with 11C-Hydroxyephedrine and 123I-MIBG. J. Nucl. Med. 2015, 56, 1429–1433. [Google Scholar] [CrossRef] [Green Version]
- Thackeray, J.T.; Bengel, F.M. Assessment of cardiac autonomic neuronal function using PET imaging. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2013, 20, 150–165. [Google Scholar] [CrossRef]
- Yu, M.; Bozek, J.; Lamoy, M.; Guaraldi, M.; Silva, P.; Kagan, M.; Yalamanchili, P.; Onthank, D.; Mistry, M.; Lazewatsky, J.; et al. Evaluation of LMI1195, a novel 18F-labeled cardiac neuronal PET imaging agent, in cells and animal models. Circ. Cardiovasc. Imaging 2011, 4, 435–443. [Google Scholar] [CrossRef] [Green Version]
- Zelt, J.G.E.; Britt, D.; Mair, B.A.; Rotstein, B.H.; Quigley, S.; Walter, O.; Garrard, L.; Robinson, S.; Mielniczuk, L.M.; deKemp, R.A.; et al. Regional Distribution of Fluorine-18-Flubrobenguane and Carbon-11-Hydroxyephedrine for Cardiac PET Imaging of Sympathetic Innervation. JACC Cardiovasc. Imaging 2021, 14, 1425–1436. [Google Scholar] [CrossRef]
- Higuchi, T.; Yousefi, B.H.; Kaiser, F.; Gärtner, F.; Rischpler, C.; Reder, S.; Yu, M.; Robinson, S.; Schwaiger, M.; Nekolla, S.G. Assessment of the 18F-Labeled PET Tracer LMI1195 for Imaging Norepinephrine Handling in Rat Hearts. J. Nucl. Med. 2013, 54, 1142–1146. [Google Scholar] [CrossRef] [Green Version]
- DeGrado, T.R.; Hutchins, G.D.; Toorongian, S.A.; Wieland, D.M.; Schwaiger, M. Myocardial kinetics of carbon-11-meta-hydroxyephedrine: Retention mechanisms and effects of norepinephrine. J. Nucl. Med. 1993, 34, 1287–1293. [Google Scholar]
- Tipre, D.N.; Fox, J.J.; Holt, D.P.; Green, G.; Yu, J.; Pomper, M.; Dannals, R.F.; Bengel, F.M. In Vivo PET Imaging of Cardiac Presynaptic Sympathoneuronal Mechanisms in the Rat. J. Nucl. Med. 2008, 49, 1189–1195. [Google Scholar] [CrossRef] [Green Version]
- Mack, F.; Bönisch, H. Dissociation constants and lipophilicity of catecholamines and related compounds. Naunyn-Schmiedeberg’s Arch. Pharmacol. 1979, 310, 1–9. [Google Scholar] [CrossRef]
- Raffel, D.M.; Wieland, D.M. Assessment of cardiac sympathetic nerve integrity with positron emission tomography. Nucl. Med. Biol. 2001, 28, 541–559. [Google Scholar] [CrossRef]
- Münch, G.; Nguyen, N.T.B.; Nekolla, S.; Ziegler, S.; Muzik, O.; Chakraborty, P.; Wieland, D.M.; Schwaiger, M. Evaluation of sympathetic nerve terminals with [11C]epinephrine and [11C]hydroxyephedrine and positron emission tomography. Circulation 2000, 101, 516–523. [Google Scholar] [CrossRef] [Green Version]
- Zelt, J.G.E.; deKemp, R.A.; Rotstein, B.H.; Nair, G.M.; Narula, J.; Ahmadi, A.; Beanlands, R.S.; Mielniczuk, L.M. Nuclear Imaging of the Cardiac Sympathetic Nervous System: A Disease-Specific Interpretation in Heart Failure. JACC Cardiovasc. Imaging 2020, 13, 1036–1054. [Google Scholar] [CrossRef]
- Verschure, D.O.; Bongers, V.; Hagen, P.; Somsen, G.A.; van Eck-Smit, B.F.; Verberne, H. Impact of a predefined mediastinal ROI on inter-observer variability of planar 123I-MIBG heart-to-mediastinum ratio. J. Nucl. Cardiol. 2014, 21, 605–613. [Google Scholar] [CrossRef]
- Pellegrino, T.; Petretta, M.; De Luca, S.; Paolillo, S.; Boemio, A.; Carotenuto, R.; Petretta, M.P.; di Nuzzo, C.; Perrone-Filardi, P.; Cuocolo, A. Observer reproducibility of results from a low-dose 123I-metaiodobenzylguanidine cardiac imaging protocol in patients with heart failure. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1549–1557. [Google Scholar] [CrossRef]
- Bateman, T.M.; Ananthasubramaniam, K.; Berman, D.S.; Gerson, M.; Gropler, R.; Henzlova, M.; Mendoza, F.; Miyamoto, M.; Shah, M.; Weiland, F. Reliability of the 123I-mIBG heart/mediastinum ratio: Results of a multicenter test–retest reproducibility study. J. Nucl. Cardiol. 2019, 26, 1555–1565. [Google Scholar] [CrossRef]
- Jacobson, A.F.; Senior, R.; Cerqueira, M.D.; Wong, N.D.; Thomas, G.S.; Lopez, V.A.; Agostini, D.; Weiland, F.; Chandna, H.; Narula, J. Myocardial iodine-123 meta-iodobenzylguanidine imaging and cardiac events in heart failure. Results of the prospective ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure) study. J. Am. Coll. Cardiol. 2010, 55, 2212–2221. [Google Scholar] [CrossRef] [Green Version]
- Schäfers, M.; Dutka, D.; Rhodes, C.G.; Lammertsma, A.A.; Hermansen, F.; Schober, O.; Camici, P.G. Myocardial presynaptic and postsynaptic autonomic dysfunction in hypertrophic cardiomyopathy. Circ. Res. 1998, 82, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, M.; Sugihara, N.; Kita, Y.; Shimizu, K.; Horita, Y.; Nakajima, K.; Taki, J.; Takeda, R. Long-term course and cardiac sympathetic nerve activity in patients with hypertrophic cardiomyopathy. Br. Heart J. 1992, 67, 155–160. [Google Scholar] [CrossRef]
- Nakajima, K.; Yamada, M. (123)I-Meta-iodobenzylguanidine Sympathetic Imaging: Standardization and Application to Neurological Diseases. Chonnam Med. J. 2016, 52, 145–150. [Google Scholar] [CrossRef] [Green Version]
- McKeith, I.G.; Boeve, B.F.; Dickson, D.W.; Halliday, G.; Taylor, J.P.; Weintraub, D.; Aarsland, D.; Galvin, J.; Attems, J.; Ballard, C.G.; et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology 2017, 89, 88–100. [Google Scholar] [CrossRef] [Green Version]
- Flotats, A.; Carrió, I.; Agostini, D.; Le Guludec, D.; Marcassa, C.; Schaffers, M.; Somsen, G.A.; Unlu, M.; Verberne, H. Proposal for standardization of 123I-metaiodobenzylguanidine (MIBG) cardiac sympathetic imaging by the EANM Cardiovascular Committee and the European Council of Nuclear Cardiology. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 1802–1812. [Google Scholar] [CrossRef]
- Agostini, D.; Carrio, I.; Verberne, H.J. How to use myocardial 123I-MIBG scintigraphy in chronic heart failure. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 555–559. [Google Scholar] [CrossRef] [Green Version]
- Carrió, I.; Cowie, M.R.; Yamazaki, J.; Udelson, J.; Camici, P.G. Cardiac sympathetic imaging with mIBG in heart failure. JACC Cardiovasc. Imaging 2010, 3, 92–100. [Google Scholar] [CrossRef] [Green Version]
- Friedman, N.C.; Hassan, A.; Grady, E.; Matsuoka, D.T.; Jacobson, A.F. Efficacy of thyroid blockade on thyroid radioiodine uptake in 123I-mIBG imaging. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2014, 55, 211–215. [Google Scholar] [CrossRef] [Green Version]
- Agostini, D.; Verberne, H.J.; Burchert, W.; Knuuti, J.; Povinec, P.; Sambuceti, G.; Unlu, M.; Estorch, M.; Banerjee, G.; Jacobson, A.F. I-123-mIBG myocardial imaging for assessment of risk for a major cardiac event in heart failure patients: Insights from a retrospective European multicenter study. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Garcia, E.V.; Galt, J.R.; Folks, R.D.; Carrio, I. Optimized acquisition and processing protocols for I-123 cardiac SPECT imaging. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2006, 13, 251–260. [Google Scholar] [CrossRef]
- Holly, T.A.; Abbott, B.G.; Al-Mallah, M.; Calnon, D.A.; Cohen, M.C.; DiFilippo, F.P.; Ficaro, E.P.; Freeman, M.R.; Hendel, R.C.; Jain, D.; et al. Single photon-emission computed tomography. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2010, 17, 941–973. [Google Scholar] [CrossRef] [PubMed]
- Gimelli, A.; Liga, R.; Giorgetti, A.; Genovesi, D.; Marzullo, P. Assessment of myocardial adrenergic innervation with a solid-state dedicated cardiac cadmium-zinc-telluride camera: First clinical experience. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 575–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verschure, D.O.; de Wit, T.C.; Bongers, V.; Hagen, P.J.; Sonneck-Koenne, C.; D’Aron, J.; Huber, K.; van Eck-Smit, B.L.; Knoll, P.; Somsen, G.A.; et al. ¹²³I-MIBG heart-to-mediastinum ratio is influenced by high-energy photon penetration of collimator septa from liver and lung activity. Nucl. Med. Commun. 2015, 36, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, K.; Okuda, K.; Yoshimura, M.; Matsuo, S.; Wakabayashi, H.; Imanishi, Y.; Kinuya, S. Multicenter cross-calibration of I-123 metaiodobenzylguanidine heart-to-mediastinum ratios to overcome camera-collimator variations. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2014, 21, 970–978. [Google Scholar] [CrossRef] [Green Version]
- Verschure, D.O.; Poel, E.; Nakajima, K.; Okuda, K.; van Eck-Smit, B.L.F.; Somsen, G.A.; Verberne, H.J. A European myocardial (123)I-mIBG cross-calibration phantom study. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2018, 25, 1191–1197. [Google Scholar] [CrossRef] [Green Version]
- Akutsu, Y.; Kaneko, K.; Kodama, Y.; Li, H.-L.; Suyama, J.; Shinozuka, A.; Gokan, T.; Hamazaki, Y.; Tanno, K.; Kobayashi, Y. Iodine-123 mIBG Imaging for Predicting the Development of Atrial Fibrillation. JACC Cardiovasc. Imaging 2011, 4, 78–86. [Google Scholar] [CrossRef]
- Hiasa, G.; Hamada, M.; Saeki, H.; Ogimoto, A.; Ohtsuka, T.; Hara, Y.; Shigematsu, Y. Cardiac sympathetic nerve activity can detect congestive heart failure sensitively in patients with hypertrophic cardiomyopathy. Chest 2004, 126, 679–686. [Google Scholar] [CrossRef]
- Dos Santos, M.J.; da Rocha, E.T.; Verberne, H.J.; da Silva, E.T.; Aragon, D.C.; Junior, J.S. Assessment of late anthracycline-induced cardiotoxicity by (123)I-mIBG cardiac scintigraphy in patients treated during childhood and adolescence. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2017, 24, 256–264. [Google Scholar] [CrossRef]
- Kasama, S.; Toyama, T.; Hatori, T.; Sumino, H.; Kumakura, H.; Takayama, Y.; Ichikawa, S.; Suzuki, T.; Kurabayashi, M. Evaluation of cardiac sympathetic nerve activity and left ventricular remodelling in patients with dilated cardiomyopathy on the treatment containing carvedilol. Eur. Heart J. 2007, 28, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Solal, A.; Rouzet, F.; Berdeaux, A.; Le Guludec, D.; Abergel, E.; Syrota, A.; Merlet, P. Effects of carvedilol on myocardial sympathetic innervation in patients with chronic heart failure. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2005, 46, 1796–1803. [Google Scholar]
- Somsen, G.A.; van Vlies, B.; de Milliano, P.A.; Borm, J.J.; van Royen, E.A.; Endert, E.; Lie, K.I. Increased myocardial [123I]-metaiodobenzylguanidine uptake after enalapril treatment in patients with chronic heart failure. Heart 1996, 76, 218–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasama, S.; Toyama, T.; Kumakura, H.; Takayama, Y.; Ichikawa, S.; Suzuki, T.; Kurabayashi, M. Effects of perindopril on cardiac sympathetic nerve activity in patients with congestive heart failure: Comparison with enalapril. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 964–971. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Merlet, P.; Valette, H.; Dubois-Randé, J.L.; Moyse, D.; Duboc, D.; Dove, P.; Bourguignon, M.H.; Benvenuti, C.; Duval, A.M.; Agostini, D.; et al. Prognostic value of cardiac metaiodobenzylguanidine imaging in patients with heart failure. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1992, 33, 471–477. [Google Scholar]
- Nakata, T.; Miyamoto, K.; Doi, A.; Sasao, H.; Wakabayashi, T.; Kobayashi, H.; Tsuchihashi, K.; Shimamoto, K. Cardiac death prediction and impaired cardiac sympathetic innervation assessed by MIBG in patients with failing and nonfailing hearts. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 1998, 5, 579–590. [Google Scholar] [CrossRef]
- Cohen-Solal, A.; Esanu, Y.; Logeart, D.; Pessione, F.; Dubois, C.; Dreyfus, G.; Gourgon, R.; Merlet, P. Cardiac metaiodobenzylguanidine uptake in patients with moderate chronic heart failure: Relationship with peak oxygen uptake and prognosis. J. Am. Coll. Cardiol. 1999, 33, 759–766. [Google Scholar] [CrossRef] [Green Version]
- Wakabayashi, T.; Nakata, T.; Hashimoto, A.; Yuda, S.; Tsuchihashi, K.; Travin, M.I.; Shimamoto, K. Assessment of underlying etiology and cardiac sympathetic innervation to identify patients at high risk of cardiac death. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2001, 42, 1757–1767. [Google Scholar]
- Agostini, D.; Ananthasubramaniam, K.; Chandna, H.; Friberg, L.; Hudnut, A.; Koren, M.; Miyamoto, M.I.; Senior, R.; Shah, M.; Travin, M.I.; et al. Prognostic usefulness of planar (123)I-MIBG scintigraphic images of myocardial sympathetic innervation in congestive heart failure: Follow-Up data from ADMIRE-HF. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2021, 28, 1490–1503. [Google Scholar] [CrossRef]
- Verschure, D.O.; Veltman, C.E.; Manrique, A.; Somsen, G.A.; Koutelou, M.; Katsikis, A.; Agostini, D.; Gerson, M.C.; van Eck-Smit, B.L.; Scholte, A.J.; et al. For what endpoint does myocardial 123I-MIBG scintigraphy have the greatest prognostic value in patients with chronic heart failure? Results of a pooled individual patient data meta-analysis. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 996–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakata, T.; Nakajima, K.; Yamashina, S.; Yamada, T.; Momose, M.; Kasama, S.; Matsui, T.; Matsuo, S.; Travin, M.I.; Jacobson, A.F. A pooled analysis of multicenter cohort studies of (123)I-mIBG imaging of sympathetic innervation for assessment of long-term prognosis in heart failure. JACC Cardiovasc. Imaging 2013, 6, 772–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maggioni, A.P.; Dahlström, U.; Filippatos, G.; Chioncel, O.; Crespo Leiro, M.; Drozdz, J.; Fruhwald, F.; Gullestad, L.; Logeart, D.; Fabbri, G.; et al. EURObservational Research Programme: Regional differences and 1-year follow-up results of the Heart Failure Pilot Survey (ESC-HF Pilot). Eur. J. Heart Fail. 2013, 15, 808–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moss, A.J.; Zareba, W.; Hall, W.J.; Klein, H.; Wilber, D.J.; Cannom, D.S.; Daubert, J.P.; Higgins, S.L.; Brown, M.W.; Andrews, M.L. Prophylactic Implantation of a Defibrillator in Patients with Myocardial Infarction and Reduced Ejection Fraction. N. Engl. J. Med. 2002, 346, 877–883. [Google Scholar] [CrossRef] [Green Version]
- Connolly, S.J.; Hallstrom, A.P.; Cappato, R.; Schron, E.B.; Kuck, K.H.; Zipes, D.P.; Greene, H.L.; Boczor, S.; Domanski, M.; Follmann, D.; et al. Meta-analysis of the implantable cardioverter defibrillator secondary prevention trials. AVID, CASH and CIDS studies. Antiarrhythmics vs Implantable Defibrillator study. Cardiac Arrest Study Hamburg. Canadian Implantable Defibrillator Study. Eur. Heart J. 2000, 21, 2071–2078. [Google Scholar] [CrossRef]
- Bardy, G.H.; Lee, K.L.; Mark, D.B.; Poole, J.E.; Packer, D.L.; Boineau, R.; Domanski, M.; Troutman, C.; Anderson, J.; Johnson, G.; et al. Amiodarone or an Implantable Cardioverter–Defibrillator for Congestive Heart Failure. N. Engl. J. Med. 2005, 352, 225–237. [Google Scholar] [CrossRef]
- Moss, A.J.; Greenberg, H.; Case, R.B.; Zareba, W.; Hall, W.J.; Brown, M.W.; Daubert, J.P.; McNitt, S.; Andrews, M.L.; Elkin, A.D. Long-term clinical course of patients after termination of ventricular tachyarrhythmia by an implanted defibrillator. Circulation 2004, 110, 3760–3765. [Google Scholar] [CrossRef] [Green Version]
- Podrid, P.; Fuchs, T.; Candinas, R. Role of the sympathetic nervous system in the genesis of ventricular arrhythmia. Circulation 1990, 82 (Suppl. 2), I103–I113. [Google Scholar]
- de Bakker, J.M.; van Capelle, F.J.; Janse, M.J.; Tasseron, S.; Vermeulen, J.T.; de Jonge, N.; Lahpor, J.R. Slow conduction in the infarcted human heart. ‘Zigzag’ course of activation. Circulation 1993, 88, 915–926. [Google Scholar] [CrossRef] [Green Version]
- Zipes, D.P. Influence of myocardial ischemia and infarction on autonomic innervation of heart. Circulation 1990, 82, 1095–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, A.; Cheetham, A.; George, R.S.; Mason, M.; Kelion, A.D. Cardiac iodine-123 metaiodobenzylguanidine imaging predicts ventricular arrhythmia in heart failure patients receiving an implantable cardioverter-defibrillator for primary prevention. Heart 2012, 98, 1359–1365. [Google Scholar] [CrossRef] [PubMed]
- Boogers, M.J.; Borleffs, C.J.W.; Henneman, M.M.; van Bommel, R.J.; van Ramshorst, J.; Boersma, E.; Dibbets-Schneider, P.; Stokkel, M.P.; van der Wall, E.E.; Schalij, M.J.; et al. Cardiac Sympathetic Denervation Assessed With 123-Iodine Metaiodobenzylguanidine Imaging Predicts Ventricular Arrhythmias in Implantable Cardioverter-Defibrillator Patients. J. Am. Coll. Cardiol. 2010, 55, 2769–2777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, H.; Yamada, T.; Tamaki, S.; Morita, T.; Furukawa, Y.; Iwasaki, Y.; Kawasaki, M.; Kikuchi, A.; Kondo, T.; Ozaki, T.; et al. Prediction of sudden cardiac death in patients with chronic heart failure by regional washout rate in cardiac MIBG SPECT imaging. J. Nucl. Cardiol. 2019, 26, 109–117. [Google Scholar] [CrossRef]
- Fallavollita, J.A.; Heavey, B.M.; Luisi, A.J., Jr.; Michalek, S.M.; Baldwa, S.; Mashtare, T.L., Jr.; Hutson, A.D.; Dekemp, R.A.; Haka, M.S.; Sajjad, M.; et al. Regional myocardial sympathetic denervation predicts the risk of sudden cardiac arrest in ischemic cardiomyopathy. J. Am. Coll. Cardiol. 2014, 63, 141–149. [Google Scholar] [CrossRef] [Green Version]
- Sazonova, S.I.; Atabekov, T.A.; Batalov, R.E.; Mishkina, A.I.; Varlamova, J.V.; Zavadovsky, K.V.; Popov, S.V. Prediction of appropriate ICD therapy in patients with ischemic heart failure. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2020, 29, 680–691. [Google Scholar] [CrossRef]
- Verschure, D.O.; de Groot, J.R.; Mirzaei, S.; Gheysens, O.; Nakajima, K.; van Eck-Smit, B.L.F.; Aernout Somsen, G.; Verberne, H.J. Cardiac 123I-mIBG scintigraphy is associated with freedom of appropriate ICD therapy in stable chronic heart failure patients. Int. J. Cardiol. 2017, 248, 403–408. [Google Scholar] [CrossRef] [Green Version]
- Travin, M.I.; Henzlova, M.J.; van Eck-Smit, B.L.F.; Jain, D.; Carrio, I.; Folks, R.D.; Garcia, E.V.; Jacobson, A.F.; Verberne, H.J. Assessment of (123)I-mIBG and (99m)Tc-tetrofosmin single-photon emission computed tomographic images for the prediction of arrhythmic events in patients with ischemic heart failure: Intermediate severity innervation defects are associated with higher arrhythmic risk. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2017, 24, 377–391. [Google Scholar] [CrossRef]
- Verschure, D.O.; Poel, E.; Travin, M.I.; Henzlova, M.J.; Jain, D.; Jacobson, A.F.; Verberne, H.J. A simplified wall-based model for regional innervation/perfusion mismatch assessed by cardiac 123I-mIBG and rest 99mTc-tetrofosmin SPECT to predict arrhythmic events in ischaemic heart failure. Eur. Heart J. Cardiovasc. Imaging 2021, jeab132. [Google Scholar] [CrossRef]
- De Vincentis, G.; Frantellizzi, V.; Fedele, F.; Farcomeni, A.; Scarparo, P.; Salvi, N.; Fegatelli, D.A.; Mancone, M.; Verschure, D.O.; Verberne, H.J. Role of cardiac (123)I-mIBG imaging in predicting arrhythmic events in stable chronic heart failure patients with an ICD. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2018, 6, 1188–1196. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, K.; Nakata, T.; Doi, T.; Tada, H.; Maruyama, K. Machine learning-based risk model using (123)I-metaiodobenzylguanidine to differentially predict modes of cardiac death in heart failure. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2022, 29, 190–201. [Google Scholar] [CrossRef]
- O’Day, K.; Levy, W.C.; Johnson, M.; Jacobson, A.F. Cost-Effectiveness Analysis of Iodine-123 Meta-Iodobenzylguanidine Imaging for Screening Heart Failure Patients Eligible for an Implantable Cardioverter Defibrillator in the USA. Appl. Health Econ. Health Policy 2016, 14, 361–373. [Google Scholar] [CrossRef] [Green Version]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: Developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) With the special contribution of the European Heart Rhythm Association (EHRA). Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef]
- Scholtens, A.M.; Braat, A.J.; Tuinenburg, A.; Meine, M.; Verberne, H.J. Cardiac sympathetic innervation and cardiac resynchronization therapy. Heart Fail. Rev. 2014, 19, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Moreira, R.I.; Abreu, A.; Portugal, G.; Oliveira, L.; Oliveira, M.; Rodrigues, I.; Cruz, M.C.; Cunha, P.S.; Santos, V.; Clara, H.S.; et al. Prognostic effect and modulation of cardiac sympathetic function in heart failure patients treated with cardiac resynchronization therapy. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2018, 27, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Verschure, D.O.; Poel, E.; De Vincentis, G.; Frantellizzi, V.; Nakajima, K.; Gheysens, O.; de Groot, J.R.; Verberne, H.J. The relation between cardiac 123I-mIBG scintigraphy and functional response 1 year after CRT implantation. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 49–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pocock, S.J.; Ariti, C.A.; McMurray, J.J.; Maggioni, A.; Køber, L.; Squire, I.B.; Swedberg, K.; Dobson, J.; Poppe, K.K.; Whalley, G.A.; et al. Predicting survival in heart failure: A risk score based on 39 372 patients from 30 studies. Eur. Heart J. 2013, 34, 1404–1413. [Google Scholar] [CrossRef]
- Levy, W.C.; Mozaffarian, D.; Linker, D.T.; Sutradhar, S.C.; Anker, S.D.; Cropp, A.B.; Anand, I.; Maggioni, A.; Burton, P.; Sullivan, M.D.; et al. The Seattle Heart Failure Model: Prediction of survival in heart failure. Circulation 2006, 113, 1424–1433. [Google Scholar] [CrossRef]
- Sartipy, U.; Dahlström, U.; Edner, M.; Lund, L.H. Predicting survival in heart failure: Validation of the MAGGIC heart failure risk score in 51,043 patients from the Swedish heart failure registry. Eur. J. Heart Fail. 2014, 16, 173–179. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, C.M.; Whellan, D.J.; Wojdyla, D.; Leifer, E.; Clare, R.M.; Ellis, S.J.; Fine, L.J.; Fleg, J.L.; Zannad, F.; Keteyian, S.J.; et al. Factors related to morbidity and mortality in patients with chronic heart failure with systolic dysfunction: The HF-ACTION predictive risk score model. Circ. Heart Fail. 2012, 5, 63–71. [Google Scholar] [CrossRef] [Green Version]
- Tsutsui, H.; Isobe, M.; Ito, H.; Ito, H.; Okumura, K.; Ono, M.; Kitakaze, M.; Kinugawa, K.; Kihara, Y.; Goto, Y.; et al. JCS 2017/JHFS 2017 Guideline on Diagnosis and Treatment of Acute and Chronic Heart Failure—Digest Version. Circ. J. Off. J. Jpn. Circ. Soc. 2019, 83, 2084–2184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakajima, K.; Nakata, T.; Yamada, T.; Yamashina, S.; Momose, M.; Kasama, S.; Matsui, T.; Matsuo, S.; Travin, M.I.; Jacobson, A.F. A prediction model for 5-year cardiac mortality in patients with chronic heart failure using (1)(2)(3)I-metaiodobenzylguanidine imaging. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1673–1682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakajima, K.; Nakata, T.; Matsuo, S.; Jacobson, A.F. Creation of mortality risk charts using 123I meta-iodobenzylguanidine heart-to-mediastinum ratio in patients with heart failure: 2- and 5-year risk models. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1138–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bielecka-Dabrowa, A.; Mikhailidis, D.P.; Hannam, S.; Rysz, J.; Michalska, M.; Akashi, Y.J.; Banach, M. Takotsubo cardiomyopathy--the current state of knowledge. Int. J. Cardiol. 2010, 142, 120–125. [Google Scholar] [CrossRef]
- Paur, H.; Wright, P.T.; Sikkel, M.B.; Tranter, M.H.; Mansfield, C.; O’Gara, P.; Stuckey, D.J.; Nikolaev, V.O.; Diakonov, I.; Pannell, L.; et al. High levels of circulating epinephrine trigger apical cardiodepression in a β2-adrenergic receptor/Gi-dependent manner: A new model of Takotsubo cardiomyopathy. Circulation 2012, 126, 697–706. [Google Scholar] [CrossRef] [Green Version]
- Lyon, A.R.; Rees, P.S.; Prasad, S.; Poole-Wilson, P.A.; Harding, S.E. Stress (Takotsubo) cardiomyopathy--a novel pathophysiological hypothesis to explain catecholamine-induced acute myocardial stunning. Nat. Clin. Pract. Cardiovasc. Med. 2008, 5, 22–29. [Google Scholar] [CrossRef]
- Verberne, H.J.; van der Heijden, D.J.; van Eck-Smit, B.L.; Somsen, G.A. Persisting myocardial sympathetic dysfunction in takotsubo cardiomyopathy. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2009, 16, 321–324. [Google Scholar] [CrossRef] [Green Version]
- Akashi, Y.J.; Takano, M.; Miyake, F. Scintigraphic imaging in Tako-Tsubo cardiomyopathy. Herz 2010, 35, 231–238. [Google Scholar] [CrossRef]
- Iversen, L.L. The uptake of catechol amines at high perfusion concentrations in the rat isolated heart: A novel catechol amine uptake process. Br. J. Pharmacol. Chemother. 1965, 25, 18–33. [Google Scholar] [CrossRef]
- Matsuura, T.; Ueno, M.; Iwanaga, Y.; Miyazaki, S. Importance of sympathetic nervous system activity during left ventricular functional recovery and its association with in-hospital complications in Takotsubo syndrome. Heart Vessels 2019, 34, 1317–1324. [Google Scholar] [CrossRef]
- Akashi, Y.J.; Nakazawa, K.; Sakakibara, M.; Miyake, F.; Musha, H.; Sasaka, K. 123I-MIBG myocardial scintigraphy in patients with “takotsubo” cardiomyopathy. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2004, 45, 1121–1127. [Google Scholar]
- Owa, M.; Aizawa, K.; Urasawa, N.; Ichinose, H.; Yamamoto, K.; Karasawa, K.; Kagoshima, M.; Koyama, J.; Ikeda, S. Emotional stress-induced ‘ampulla cardiomyopathy’: Discrepancy between the metabolic and sympathetic innervation imaging performed during the recovery course. Jpn. Circ. J. 2001, 65, 349–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verschure, D.O.; Somsen, G.A.; van Eck-Smit, B.L.; Knol, R.J.; Booij, J.; Verberne, H.J. Tako-tsubo cardiomyopathy: How to understand possible pathophysiological mechanism and the role of (123)I-MIBG imaging. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2014, 21, 730–738. [Google Scholar] [CrossRef] [PubMed]
- Narula, J.; Gerson, M.; Thomas, G.S.; Cerqueira, M.D.; Jacobson, A.F. (1)(2)(3)I-MIBG Imaging for Prediction of Mortality and Potentially Fatal Events in Heart Failure: The ADMIRE-HFX Study. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2015, 56, 1011–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tracer | Imaging | Affinity for NET | Vesicular Storage | Vesicular Leakage | Sensitivity to MAO/COMT | Neuronal Membrane Leakage | Cause of Imaging Defect/Uptake reduction |
|---|---|---|---|---|---|---|---|
| 123I-mIBG | Planar and SPECT | +++ | ++ | + | Minimal | + | ↓ Nerve density ↓ NET ↑ Sympathetic activity ↑ NE (competitive inhibiton for NET) |
| 11C-EPI | PET | ++ | +++ | Minimal | + | Minimal | ↓ Nerve density ↓ NET ↑ Sympathetic activity ↑ NE (competitive inhibiton for NET) ↑ MAO activity ↓ VMAT2 ↓ Vesicular storage |
| 11C-PHEN | PET | + | + | ++ | ++ | ++ | ↓ Nerve density ↓ NET ↑ Sympathetic activity ↑ NE (competitive inhibiton for NET) ↑ MAO activity ↓ VMAT2 ↓ Vesicular storage |
| 18F-Flubrobenguane | PET | +++ | ++ | + | Minimal | + | ↓ Nerve density ↓ NET ↑ Sympathetic activity ↑ NE (competitive inhibiton for NET) |
| Cardiac 123I-mIBG imaging | |
|---|---|
| Administration dosis of 123I-mIBG | 111–370 MBq * |
| Timing of acquisition p.i. | 15–30 min (early) |
| 3–4 h (late) | |
| Planar imaging | 128 × 128 of 256 × 256 matrix |
| 5–10 min | |
| LE of ME collimators (standarization recommended) | |
| SPECT imaging | 64 × 64 matrix |
| 3–6 degree step, 30 s per projection ** | |
| 180 or 360 degree rotation | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verschure, D.O.; Nakajima, K.; Verberne, H.J. Cardiac 123I-mIBG Imaging in Heart Failure. Pharmaceuticals 2022, 15, 656. https://doi.org/10.3390/ph15060656
Verschure DO, Nakajima K, Verberne HJ. Cardiac 123I-mIBG Imaging in Heart Failure. Pharmaceuticals. 2022; 15(6):656. https://doi.org/10.3390/ph15060656
Chicago/Turabian StyleVerschure, Derk O., Kenichi Nakajima, and Hein J. Verberne. 2022. "Cardiac 123I-mIBG Imaging in Heart Failure" Pharmaceuticals 15, no. 6: 656. https://doi.org/10.3390/ph15060656
APA StyleVerschure, D. O., Nakajima, K., & Verberne, H. J. (2022). Cardiac 123I-mIBG Imaging in Heart Failure. Pharmaceuticals, 15(6), 656. https://doi.org/10.3390/ph15060656