

Pioglitazone Has a Null Association with Inflammatory Bowel Disease in Patients with Type 2 Diabetes Mellitus


Abstract
1. Introduction
2. Results
3. Discussion
Main Findings
- a.
- Discrepancies with preclinical studies
- b.
- Implications
- c.
- Strengths
- d.
- Limitations
4. Materials and Methods
4.1. The National Health Insurance in Taiwan
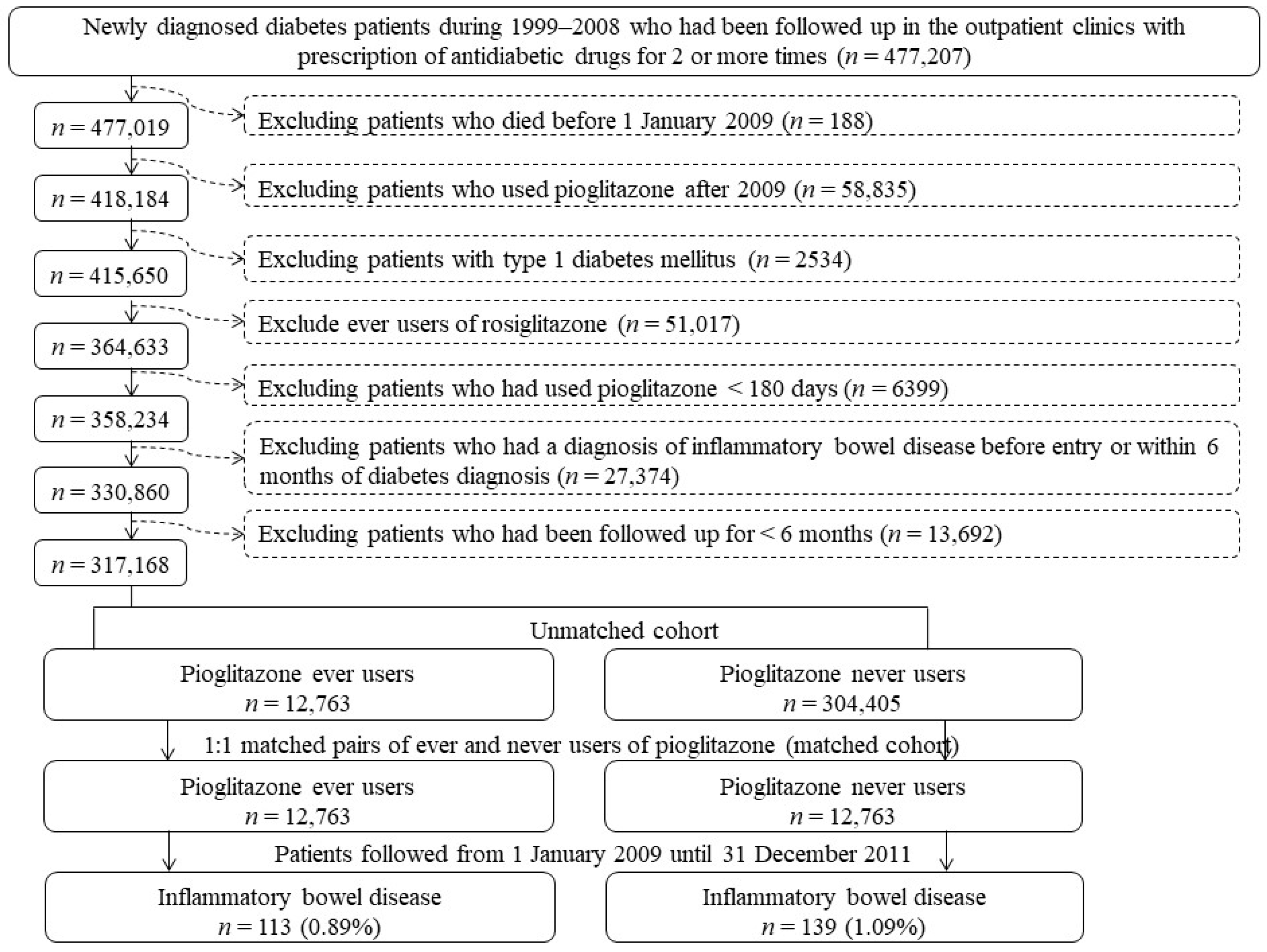
4.2. Enrollment of Study Subjects
4.3. Potential Confounders
4.4. Statistical Analyses
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flynn, S.; Eisenstein, S. Inflammatory bowel disease presentation and diagnosis. Surg. Clin. N. Am. 2019, 99, 1051–1062. [Google Scholar] [CrossRef] [PubMed]
- Decara, J.; Rivera, P.; López-Gambero, A.J.; Serrano, A.; Pavón, F.J.; Baixeras, E.; Rodríguez de Fonseca, F.; Suárez, J. Peroxisome proliferator-activated receptors: Experimental targeting for the treatment of inflammatory bowel diseases. Front. Pharmacol. 2020, 11, 730. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2018, 390, 2769–2778. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, D.C.; Carding, S.R. Inflammatory bowel disease: Cause and immunobiology. Lancet 2007, 369, 1627–1640. [Google Scholar] [CrossRef] [PubMed]
- Caioni, G.; Viscido, A.; d’Angelo, M.; Panella, G.; Castelli, V.; Merola, C.; Frieri, G.; Latella, G.; Cimini, A.; Benedetti, E. Inflammatory bowel disease: New insights into the interplay between environmental factors and PPARγ. Int. J. Mol. Sci. 2021, 22, 985. [Google Scholar] [CrossRef]
- Verdugo-Meza, A.; Ye, J.; Dadlani, H.; Ghosh, S.; Gibson, D.L. Connecting the dots between inflammatory bowel disease and metabolic syndrome: A focus on gut-derived metabolites. Nutrients 2020, 12, 1434. [Google Scholar] [CrossRef]
- Actis, G.C.; Pellicano, R.; Fagoonee, S.; Ribaldone, D.G. History of inflammatory bowel diseases. J. Clin. Med. 2019, 8, 1970. [Google Scholar] [CrossRef]
- Celiberto, L.S.; Graef, F.A.; Healey, G.R.; Bosman, E.S.; Jacobson, K.; Sly, L.M.; Vallance, B.A. Inflammatory bowel disease and immunonutrition: Novel therapeutic approaches through modulation of diet and the gut microbiome. Immunology 2018, 155, 36–52. [Google Scholar] [CrossRef]
- Lavelle, A.; Sokol, H. Gut microbiota-derived metabolites as key actors in inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 223–237. [Google Scholar] [CrossRef]
- Speca, S.; Dubuquoy, L.; Desreumaux, P. Peroxisome proliferator-activated receptor gamma in the colon: Inflammation and innate antimicrobial immunity. J. Clin. Gastroenterol. 2014, 48 (Suppl. 1), S23–S27. [Google Scholar] [CrossRef]
- Dubuquoy, L.; Rousseaux, C.; Thuru, X.; Peyrin-Biroulet, L.; Romano, O.; Chavatte, P.; Chamaillard, M.; Desreumaux, P. PPARgamma as a new therapeutic target in inflammatory bowel diseases. Gut 2006, 55, 1341–1349. [Google Scholar] [CrossRef] [PubMed]
- Vetuschi, A.; Pompili, S.; Gaudio, E.; Latella, G.; Sferra, R. PPAR-γ with its anti-inflammatory anti-fibrotic action could be an effective therapeutic target in IBD. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 8839–8848. [Google Scholar] [PubMed]
- Venkataraman, B.; Ojha, S.; Belur, P.D.; Bhongade, B.; Raj, V.; Collin, P.D.; Adrian, T.E.; Subramanya, S.B. Phytochemical drug candidates for the modulation of peroxisome proliferator-activated receptor γ in inflammatory bowel diseases. Phytother. Res. 2020, 34, 1530–1549. [Google Scholar] [CrossRef] [PubMed]
- Celinski, K.; Dworzanski, T.; Fornal, R.; Korolczuk, A.; Madro, A.; Brzozowski, T.; Slomka, M. Comparison of anti-inflammatory properties of peroxisome proliferator-activated receptor gamma agonists rosiglitazone and troglitazone in prophylactic treatment of experimental colitis. J. Physiol. Pharmacol. 2013, 64, 587–595. [Google Scholar]
- Fang, J.; Wang, H.; Xue, Z.; Cheng, Y.; Zhang, X. PPARγ: The central mucus barrier coordinator in ulcerative colitis. Inflamm. Bowel Dis. 2021, 27, 732–741. [Google Scholar] [CrossRef]
- Luo, S.; He, J.; Huang, S.; Wang, X.; Su, Y.; Li, Y.; Chen, Y.; Yang, G.; Huang, B.; Guo, S.; et al. Emodin targeting the colonic metabolism via PPARγ alleviates UC by inhibiting facultative anaerobe. Phytomedicine 2022, 104, 154106. [Google Scholar] [CrossRef]
- da Rocha, G.H.O.; de Paula-Silva, M.; Broering, M.F.; Scharf, P.R.D.S.; Matsuyama, L.S.A.S.; Maria-Engler, S.S.; Farsky, S.H.P. Pioglitazone-mediated attenuation of experimental colitis relies on cleaving of annexin A1 released by macrophages. Front. Pharmacol. 2020, 11, 591561. [Google Scholar] [CrossRef]
- Dormandy, J.A.; Charbonnel, B.; Eckland, D.J.; Erdmann, E.; Massi-Benedetti, M.; Moules, I.K.; Skene, A.M.; Tan, M.H.; Lefèbvre, P.J.; Murray, G.D.; et al. PROactive investigators. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): A randomised controlled trial. Lancet 2005, 366, 1279–1289. [Google Scholar] [CrossRef]
- Sun, T.; Kwong, C.H.T.; Gao, C.; Wei, J.; Yue, L.; Zhang, J.; Ye, R.D.; Wang, R. Amelioration of ulcerative colitis via inflammatory regulation by macrophage-biomimetic nanomedicine. Theranostics 2020, 10, 10106–10119. [Google Scholar] [CrossRef]
- Da Silva, S.; Keita, Å.V.; Mohlin, S.; Påhlman, S.; Theodorou, V.; Påhlman, I.; Mattson, J.P.; Söderholm, J.D. A novel topical PPARγ agonist induces PPARγ activity in ulcerative colitis mucosa and prevents and reverses inflammation in induced colitis models. Inflamm. Bowel Dis. 2018, 24, 792–805. [Google Scholar] [CrossRef]
- Tseng, C.H.; Huang, T.S. Pioglitazone with sulfonylurea: Glycemic and lipid effects in Taiwanese diabetic patients. Diabetes Res. Clin. Pract. 2005, 70, 193–194. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Pioglitazone reduces dementia risk in patients with type 2 diabetes mellitus: A retrospective cohort analysis. J. Clin. Med. 2018, 7, 306. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Pioglitazone and risk of chronic obstructive pulmonary disease in patients with type 2 diabetes mellitus. Int J COPD. 2022, 17, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.D.; Ferrara, A.; Peng, T.; Hedderson, M.; Bilker, W.B.; Quesenberry, C.P., Jr.; Vaughn, D.J.; Nessel, L.; Selby, J.; Strom, B.L. Risk of bladder cancer among diabetic patients treated with pioglitazone: Interim report of a longitudinal cohort study. Diabetes Care 2011, 34, 916–922. [Google Scholar] [CrossRef]
- Kernan, W.N.; Viscoli, C.M.; Furie, K.L.; Young, L.H.; Inzucchi, S.E.; Gorman, M.; Guarino, P.D.; Lovejoy, A.M.; Peduzzi, P.N.; Conwit, R.; et al. IRIS Trial Investigators. Pioglitazone after ischemic stroke or transient ischemic attack. N. Engl. J. Med. 2016, 374, 1321–1331. [Google Scholar] [CrossRef]
- Al-Majed, A.; Bakheit, A.H.; Abdel Aziz, H.A.; Alharbi, H.; Al-Jenoobi, F.I. Pioglitazone. Profiles Drug Subst. Excip. Relat. Methodol. 2016, 41, 379–438. [Google Scholar]
- Pearce, N.; Checkoway, H.; Kriebel, D. Bias in occupational epidemiology studies. Occup. Environ. Med. 2007, 64, 562–568. [Google Scholar] [CrossRef]
- Kesmodel, U.S. Information bias in epidemiological studies with a special focus on obstetrics and gynecology. Acta Obstet. Gynecol. Scand. 2018, 97, 417–423. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin is associated with a lower risk of colorectal cancer in Taiwanese patients with type 2 diabetes: A retrospective cohort analysis. Diabetes Metab. 2017, 43, 438–445. [Google Scholar] [CrossRef]
- Nissen, S.E.; Wolski, K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N. Engl. J. Med. 2007, 356, 2457–2471. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin use is associated with a lower risk of inflammatory bowel disease in patients with type 2 diabetes mellitus. J. Crohn’s Colitis 2021, 15, 64–73. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Never Users | Ever Users | Standardized Difference | ||
|---|---|---|---|---|---|
| (n = 12,763) | (n = 12,763) | ||||
| n | % | n | % | ||
| Basic data | |||||
| Age * (years) | 61.01 | 12.17 | 60.95 | 11.50 | −0.68 |
| Diabetes duration * (years) | 6.51 | 2.74 | 6.50 | 2.59 | −0.40 |
| Sex (men) | 7219 | 56.56 | 7218 | 56.55 | −0.03 |
| Occupation | |||||
| I | 4966 | 38.91 | 4920 | 38.55 | |
| II | 2814 | 22.05 | 2800 | 21.94 | −0.25 |
| III | 2505 | 19.63 | 2533 | 19.85 | 0.50 |
| IV | 2478 | 19.42 | 2510 | 19.67 | 0.68 |
| Living region | |||||
| Taipei | 5068 | 39.71 | 5097 | 39.94 | |
| Northern | 1326 | 10.39 | 1327 | 10.40 | 0.10 |
| Central | 2044 | 16.02 | 15.69 | −0.84 | |
| Southern | 1574 | 12.33 | 1609 | 12.61 | 0.78 |
| Kao-Ping and Eastern | 2751 | 21.55 | 2727 | 21.37 | −0.48 |
| Major comorbidities associated with diabetes mellitus | |||||
| Hypertension | 10,370 | 81.25 | 10,422 | 81.66 | 0.97 |
| Dyslipidemia | 10,915 | 85.52 | 10,907 | 85.46 | −0.17 |
| Obesity | 715 | 5.60 | 785 | 6.15 | 2.32 |
| Diabetes-related complications | |||||
| Nephropathy | 3290 | 25.78 | 3245 | 25.43 | −0.91 |
| Eye disease | 4302 | 33.71 | 4352 | 34.10 | 0.85 |
| Diabetic polyneuropathy | 3610 | 28.28 | 3617 | 28.34 | 0.08 |
| Stroke | 3113 | 24.39 | 3175 | 24.88 | 1.02 |
| Ischemic heart disease | 5419 | 42.46 | 5479 | 42.93 | 0.84 |
| Peripheral arterial disease | 3116 | 24.41 | 3090 | 24.21 | −0.49 |
| Factors that might affect exposure/outcome | |||||
| Head injury | 436 | 3.42 | 440 | 3.45 | 0.12 |
| Parkinson’s disease | 286 | 2.24 | 272 | 2.13 | −0.81 |
| Hypoglycemia | 473 | 3.71 | 496 | 3.89 | 0.85 |
| Chronic obstructive pulmonary disease | 5759 | 45.12 | 5812 | 45.54 | 0.76 |
| Tobacco abuse | 486 | 3.81 | 504 | 3.95 | 0.65 |
| Alcohol-related diagnoses | 702 | 5.50 | 698 | 5.47 | 0.02 |
| Heart failure | 1932 | 15.14 | 1948 | 15.26 | 0.25 |
| Gingival and periodontal diseases | 11,232 | 88.00 | 11,181 | 87.60 | −1.16 |
| Pneumonia | 1576 | 12.35 | 1595 | 12.50 | 0.29 |
| Pulmonary tuberculosis | 388 | 3.04 | 444 | 3.48 | 2.40 |
| Osteoporosis | 2108 | 16.52 | 2195 | 17.20 | 1.74 |
| Human immunodeficiency virus infection | 12 | 0.09 | 8 | 0.06 | −1.31 |
| Cancer | 1579 | 12.37 | 1657 | 12.98 | 1.80 |
| Dementia | 677 | 5.30 | 653 | 5.12 | −0.99 |
| Valvular heart disease | 1025 | 8.03 | 1043 | 8.17 | 0.51 |
| Arthropathies | 9628 | 75.44 | 9685 | 75.88 | 1.02 |
| Psoriasis | 419 | 3.28 | 374 | 2.93 | −2.19 |
| Dorsopathies | 9777 | 76.60 | 9792 | 76.72 | 0.25 |
| Liver cirrhosis | 360 | 2.82 | 352 | 2.76 | −0.45 |
| Other chronic non-alcoholic liver diseases | 1171 | 9.17 | 1210 | 9.48 | 0.99 |
| Hepatitis B virus infection | 452 | 3.54 | 465 | 3.64 | 0.52 |
| Hepatitis C virus infection | 419 | 3.28 | 451 | 3.53 | 1.32 |
| Organ transplantation | 33 | 0.26 | 24 | 0.19 | −1.57 |
| Antidiabetic drugs and drugs that are commonly prescribed to diabetes patients or drugs that might affect exposure/outcome | |||||
| Insulin | 380 | 2.98 | 388 | 3.04 | 0.43 |
| Sulfonylureas | 8849 | 69.33 | 8894 | 69.69 | 0.58 |
| Metformin | 9381 | 73.50 | 9389 | 73.56 | 0.15 |
| Meglitinide | 905 | 7.09 | 879 | 6.89 | −1.00 |
| Acarbose | 1702 | 13.34 | 1742 | 13.65 | 0.89 |
| Angiotensin converting enzyme inhibitors/Angiotensin receptor blockers | 9404 | 73.68 | 9487 | 74.33 | 1.38 |
| Calcium channel blockers | 7273 | 56.99 | 7358 | 57.65 | 1.27 |
| Statins | 9457 | 74.10 | 9505 | 74.47 | 0.91 |
| Fibrates | 5736 | 44.94 | 5728 | 44.88 | −0.15 |
| Aspirin | 7594 | 59.50 | 7587 | 59.45 | −0.21 |
| Corticosteroids | 359 | 2.81 | 331 | 2.59 | −1.48 |
| Pioglitazone Use | Incident Case Number | Cases Followed | Person-Years | Incidence Rate (per 100,000 Person-Years) | Hazard Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|---|---|---|---|
| Never users | 139 | 12,763 | 33,988.31 | 408.96 | 1.000 | ||
| Ever users | 113 | 12,763 | 34,154.60 | 330.85 | 0.809 | (0.631–1.037) | 0.0937 |
| Tertiles of cumulative duration of pioglitazone therapy (months) | |||||||
| Never users | 139 | 12,763 | 33,988.31 | 408.96 | 1.000 | ||
| <11.0 | 32 | 4147 | 10,833.86 | 295.37 | 0.727 | (0.495–1.068) | 0.1044 |
| 11.0–19.7 | 35 | 4282 | 11,466.87 | 305.23 | 0.745 | (0.514–1.079) | 0.1191 |
| >19.7 | 46 | 4334 | 11,853.86 | 388.06 | 0.942 | (0.675–1.315) | 0.7253 |
| Tertiles of cumulative dose of pioglitazone therapy (mg) | |||||||
| Never users | 139 | 12,763 | 33,988.31 | 408.96 | 1.000 | ||
| <7980 | 31 | 4155 | 10,897.90 | 284.46 | 0.700 | (0.474–1.033) | 0.0726 |
| 7980–14,940 | 37 | 4266 | 11,435.47 | 323.55 | 0.790 | (0.550–1.135) | 0.2018 |
| >14,940 | 45 | 4342 | 11,821.23 | 380.67 | 0.925 | (0.661–1.294) | 0.6478 |
| Risk Factor/Pioglitazone Use | Incident Case Number | Cases Followed | Person-Years | Incidence Rate (per 100,000 Person-Years) | Hazard Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|---|---|---|---|
| Psoriasis (+)/Pioglitazone (−) | 3 | 419 | 1124.62 | 266.76 | 1.000 | ||
| Psoriasis (+)/Pioglitazone (+) | 6 | 374 | 994.22 | 603.49 | 2.329 | (0.581–9.332) | 0.2325 |
| Psoriasis (−)/Pioglitazone (−) | 136 | 12,344 | 32,863.69 | 413.83 | 1.602 | (0.509–5.043) | 0.4206 |
| Psoriasis (−)/Pioglitazone (+) | 107 | 12,389 | 33,160.38 | 322.67 | 1.250 | (0.396–3.947) | 0.7042 |
| P-interaction | 0.1286 | ||||||
| Arthropathies (+)/Pioglitazone (−) | 117 | 9628 | 25,741.21 | 454.52 | 1.000 | ||
| Arthropathies (+)/Pioglitazone (+) | 90 | 9685 | 25,978.83 | 346.44 | 0.763 | (0.580–1.005) | 0.0546 |
| Arthropathies (−)/Pioglitazone (−) | 22 | 3135 | 8247.10 | 266.76 | 0.687 | (0.427–1.107) | 0.1228 |
| Arthropathies (−)/Pioglitazone (+) | 23 | 3078 | 8175.77 | 281.32 | 0.731 | (0.457–1.169) | 0.1906 |
| P-interaction | 0.3149 | ||||||
| Dorsopathies (+)/Pioglitazone (−) | 113 | 9777 | 26,118.94 | 432.64 | 1.000 | ||
| Dorsopathies (+)/Pioglitazone (+) | 93 | 9792 | 26,258.73 | 354.17 | 0.820 | (0.623–1.079) | 0.1558 |
| Dorsopathies (−)/Pioglitazone (−) | 26 | 2986 | 7869.37 | 330.39 | 0.942 | (0.603–1.471) | 0.7920 |
| Dorsopathies (−)/Pioglitazone (+) | 20 | 2971 | 7895.87 | 253.30 | 0.726 | (0.444–1.188) | 0.2026 |
| P-interaction | 0.8522 | ||||||
| COPD/Tobacco abuse (+)/Pioglitazone (−) | 72 | 5960 | 15,908.15 | 452.60 | 1.000 | ||
| COPD/Tobacco abuse (+)/Pioglitazone (+) | 56 | 6038 | 16,163.84 | 346.45 | 0.760 | (0.536–1.079) | 0.1252 |
| COPD/Tobacco abuse (−)/Pioglitazone (−) | 67 | 6803 | 18,080.16 | 370.57 | 0.860 | (0.609–1.215) | 0.3932 |
| COPD/Tobacco abuse (−)/Pioglitazone (+) | 57 | 6725 | 17,990.76 | 316.83 | 0.744 | (0.520–1.066) | 0.1074 |
| P-interaction | 0.9709 | ||||||
| Any of the four (+)/Pioglitazone (−) | 130 | 11,333 | 30,243.27 | 429.85 | 1.000 | ||
| Any of the four (+)/Pioglitazone (+) | 104 | 11,370 | 30,483.71 | 341.17 | 0.797 | (0.615–1.031) | 0.0843 |
| All of the four (−)/Pioglitazone (−) | 9 | 1430 | 3745.04 | 240.32 | 0.660 | (0.332–1.310) | 0.2347 |
| All of the four (−)/Pioglitazone (+) | 9 | 1393 | 3670.88 | 245.17 | 0.668 | (0.336–1.327) | 0.2492 |
| P-interaction | 0.6240 |
| Metformin/Pioglitazone Use | Incident Case Number | Cases Followed | Person-Years | Incidence Rate (per 100,000 Person-Years) | Hazard Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|---|---|---|---|
| Metformin (−)/Pioglitazone (−) | 33 | 3382 | 8911.51 | 370.31 | 1.000 | ||
| Metformin (−)/Pioglitazone (+) | 27 | 3374 | 8986.75 | 300.44 | 0.840 | (0.503–1.402) | 0.5043 |
| Metformin (+)/Pioglitazone (−) | 106 | 9381 | 25,076.80 | 422.70 | 1.186 | (0.793–1.771) | 0.4061 |
| Metformin (+)/Pioglitazone (+) | 86 | 9389 | 25,167.85 | 341.71 | 0.950 | (0.630–1.433) | 0.8074 |
| P-interaction | 0.6002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseng, C.-H. Pioglitazone Has a Null Association with Inflammatory Bowel Disease in Patients with Type 2 Diabetes Mellitus. Pharmaceuticals 2022, 15, 1538. https://doi.org/10.3390/ph15121538
Tseng C-H. Pioglitazone Has a Null Association with Inflammatory Bowel Disease in Patients with Type 2 Diabetes Mellitus. Pharmaceuticals. 2022; 15(12):1538. https://doi.org/10.3390/ph15121538
Chicago/Turabian StyleTseng, Chin-Hsiao. 2022. "Pioglitazone Has a Null Association with Inflammatory Bowel Disease in Patients with Type 2 Diabetes Mellitus" Pharmaceuticals 15, no. 12: 1538. https://doi.org/10.3390/ph15121538
APA StyleTseng, C.-H. (2022). Pioglitazone Has a Null Association with Inflammatory Bowel Disease in Patients with Type 2 Diabetes Mellitus. Pharmaceuticals, 15(12), 1538. https://doi.org/10.3390/ph15121538