
Reservoir-Style Polymeric Drug Delivery Systems: Empirical and Predictive Models for Implant Design

 , , ,
, , , 
Abstract
1. Introduction
2. Results and Discussion
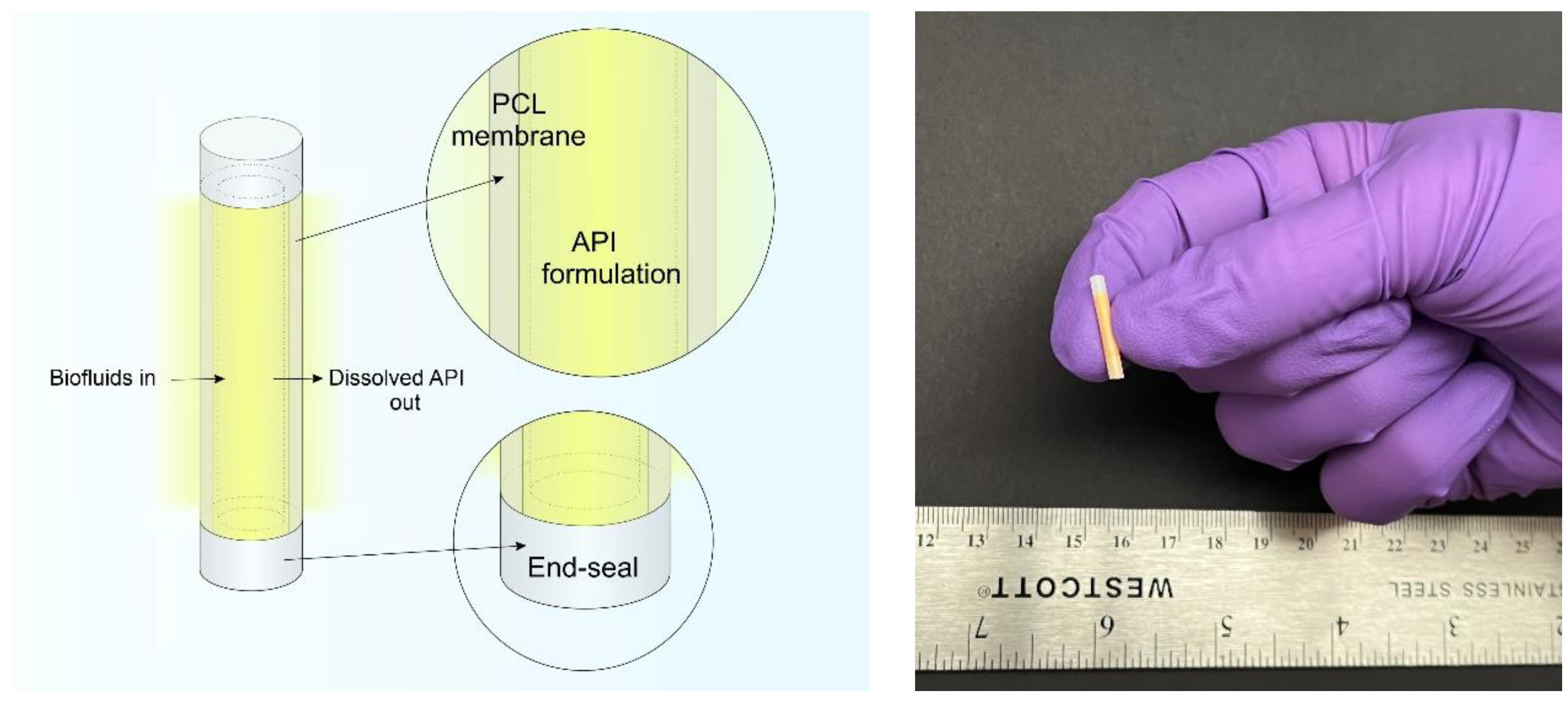
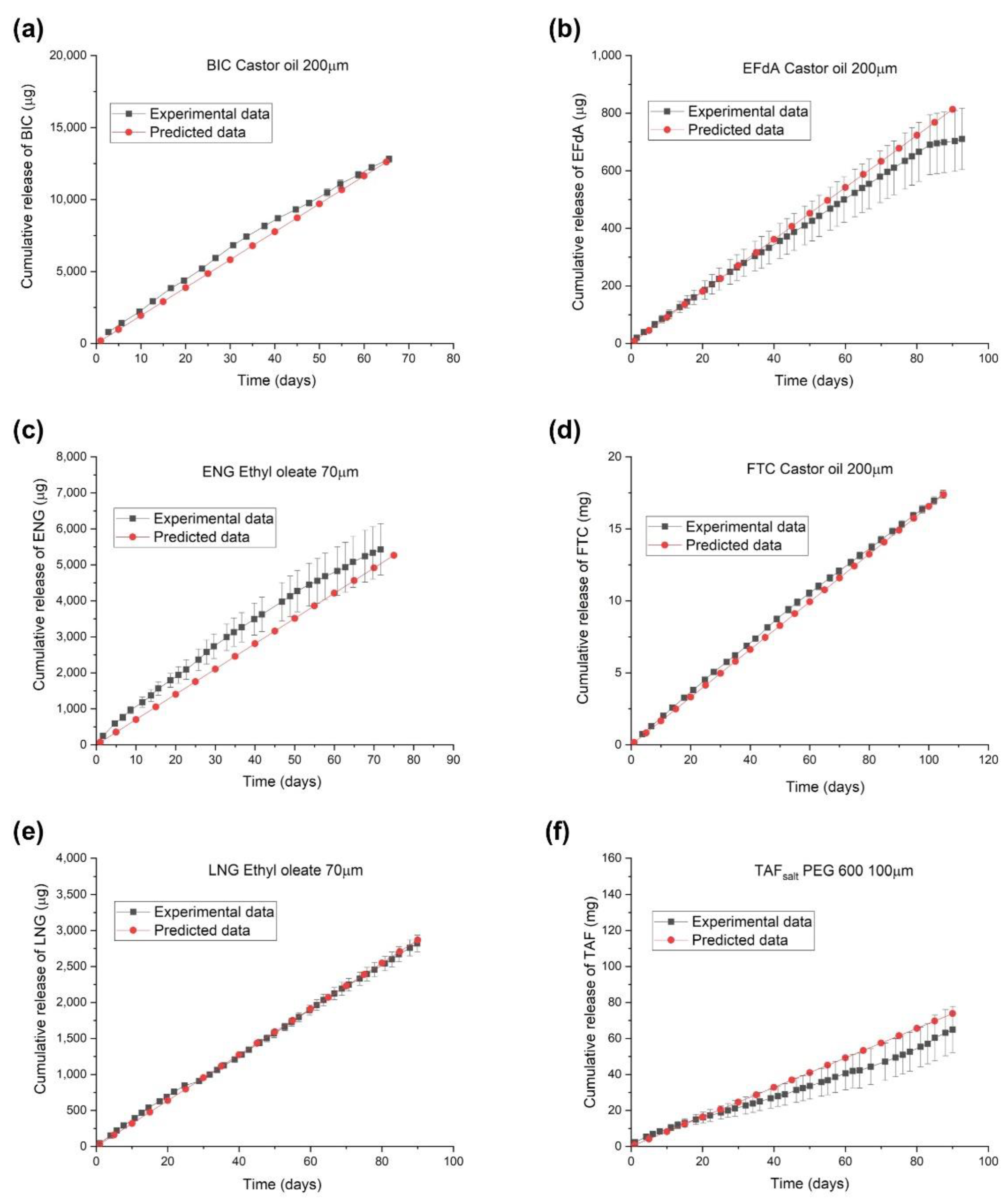
2.1. In Vitro Performance of PCL Reservoir Implants with Various API Formulations
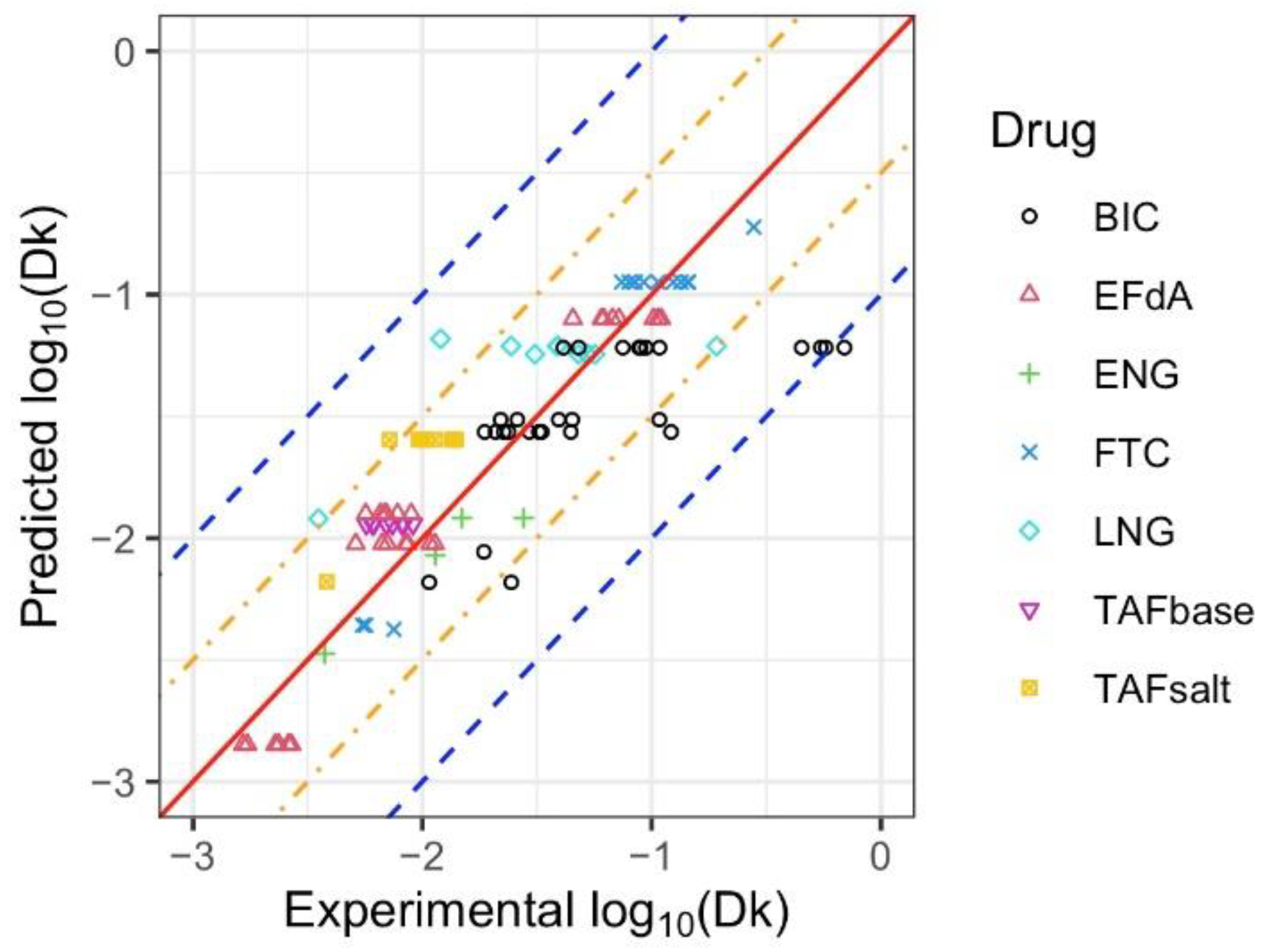
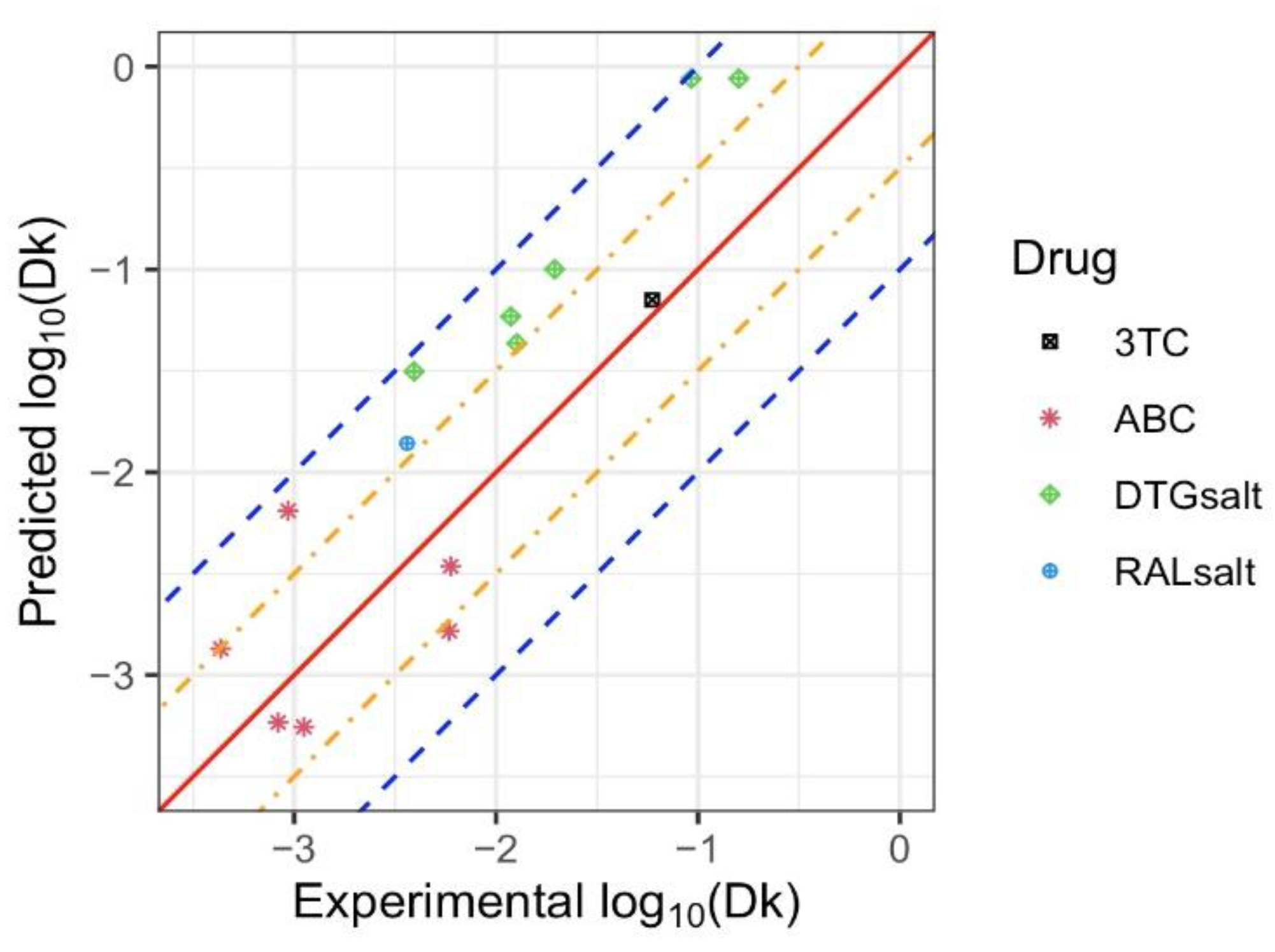
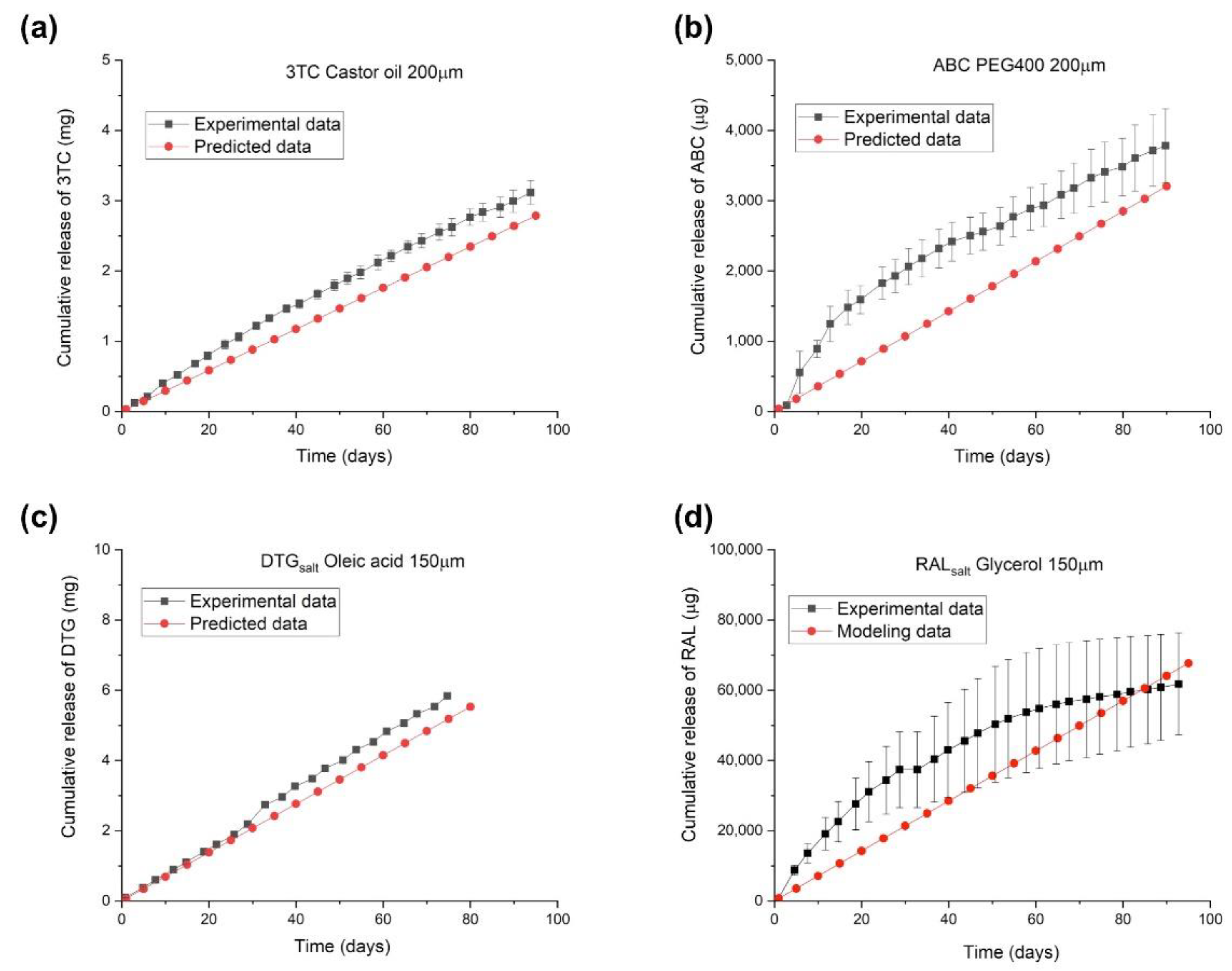
2.2. Predictive Models
2.3. Utilizing the Predictive Model
3. Materials and Methods
3.1. Solubility and Stability Analysis of the Drug Formulations
3.2. Implant Fabrication
3.3. In Vitro Drug Release Studies
3.4. Empirical Models
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaur, G.; Grewal, J.; Jyoti, K.; Jain, U.K.; Chandra, R.; Madan, J. Oral controlled and sustained drug delivery systems: Concepts, advances, preclinical, and clinical status. In Drug Targeting and Stimuli Sensitive Drug Delivery Systems; Elsevier: Amsterdam, The Netherlands, 2018; pp. 567–626. [Google Scholar]
- Sanopoulou, M.; Papadokostaki, K. Controlled Drug Release Systems: Mechanisms and Kinetics. In Biomedical Membranes and (Bio) Artificial Organs; World Scientific: Singapore, 2018; pp. 1–33. [Google Scholar]
- Huynh, C.T.; Lee, D.S. Controlled Release. In Encyclopedia of Polymeric Nanomaterials; Kobayashi, S., Müllen, K., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 439–449. [Google Scholar]
- Yang, W.W.; Pierstorff, E. Reservoir-based polymer drug delivery systems. J. Lab. Autom. 2012, 17, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Lavan, D.A.; McGuire, T.; Langer, R. Small-scale systems for in vivo drug delivery. Nat. Biotechnol. 2003, 21, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Freiberg, S.; Zhu, X. Polymer microspheres for controlled drug release. Int. J. Pharm. 2004, 282, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Sperry, P.; Cua, D.J.; Wetzel, S.; Moore, A.; Adler-Moore, J.P. Antimicrobial activity of AmBisome and non-liposomal amphotericin B following uptake of Candida glabrata by murine epidermal Langerhans cells. Med. Mycol. 1998, 36, 135–141. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Siena, S.; Piccart, M.J.; Holmes, F.A.; Glaspy, J.; Hackett, J.; Renwick, J.J. A combined analysis of two pivotal randomized trials of a single dose of pegfilgrastim per chemotherapy cycle and daily Filgrastim in patients with stage II-IV breast cancer. Oncol. Rep. 2003, 10, 715–724. [Google Scholar] [PubMed]
- Glue, P.; Rouzier-Panis, R.; Raffanel, C.; Sabo, R.; Gupta, S.K.; Salfi, M.; Jacobs, S.; Clement, R.P.; The Hepatitis C Intervention Therapy Group. A dose-ranging study of pegylated interferon alfa-2b and ribavirin in chronic hepatitis C. Hepatology 2000, 32, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Nabhan, C.; Tallman, M.S. Early phase I/II trials with gemtuzumab ozogamicin (Mylotarg®) in acute myeloid leukemia. Clin. Lymphoma 2002, 2, S19–S23. [Google Scholar] [CrossRef] [PubMed]
- Bory, C.; Boulieu, R.; Souillet, G.; Chantin, C.; Guibaud, P.; Hershfield, M. Effect of polyethylene glycol-modified adenosine deaminase (PEG-ADA) therapy in two ADA-deficient children: Measurement of erythrocyte deoxyadenosine triphosphate as a useful tool. In Purine and Pyrimidine Metabolism in Man VII; Springer: Berlin/Heidelberg, Germany, 1991; pp. 173–176. [Google Scholar]
- Muggia, F.; Hamilton, A. Phase III data on Caelyx® in ovarian cancer. Eur. J. Cancer 2001, 37, 15–18. [Google Scholar] [CrossRef]
- Olsen, E.; Duvic, M.; Frankel, A.; Kim, Y.; Martin, A.; Vonderheid, E.; Jegasothy, B.; Wood, G.; Gordon, M.; Heald, P.; et al. Pivotal phase III trial of two dose levels of denileukin diftitox for the treatment of cutaneous T-cell lymphoma. J. Clin. Oncol. 2001, 19, 376–388. [Google Scholar] [CrossRef]
- Yamamoto, M.; Takahashi, Y.; Tabata, Y. Controlled release by biodegradable hydrogels enhances the ectopic bone formation of bone morphogenetic protein. Biomaterials 2003, 24, 4375–4383. [Google Scholar] [CrossRef]
- Piu, F.; Wang, X.; Fernandez, R.; Dellamary, L.; Harrop, A.; Ye, Q.; Sweet, J.; Tapp, R.; Dolan, D.F.; Altschuler, R.A.; et al. OTO-104: A sustained-release dexamethasone hydrogel for the treatment of otic disorders. Otol. Neurotol. 2011, 32, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Dellamary, L.; Fernandez, R.; Ye, Q.; LeBel, C.; Piu, F. Principles of inner ear sustained release following intratympanic administration. Laryngoscope 2011, 121, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Casadei, M.A.; Cerreto, F.; Cesa, S.; Giannuzzo, M.; Feeney, M.; Marianecci, C.; Paolicelli, P. Solid lipid nanoparticles incorporated in dextran hydrogels: A new drug delivery system for oral formulations. Int. J. Pharm. 2006, 325, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Sakamoto, T.; Hiraumi, H.; Kikkawa, Y.S.; Yamamoto, N.; Hamaguchi, K.; Ono, K.; Yamamoto, M.; Tabata, Y.; Teramukai, S.; et al. Topical insulin-like growth factor 1 treatment using gelatin hydrogels for glucocorticoid-resistant sudden sensorineural hearing loss: A prospective clinical trial. BMC Med. 2010, 8, 76. [Google Scholar] [CrossRef] [PubMed]
- Pons-Faudoa, F.P.; Sizovs, A.; Shelton, K.A.; Momin, Z.; Niles, J.A.; Bushman, L.R.; Xu, J.; Chua, C.Y.X.; Nichols, J.E.; Demaria, S.; et al. Preventive Efficacy of a Tenofovir Alafenamide Fumarate Nanofluidic Implant in SHIV-Challenged Nonhuman Primates. Adv. Ther. 2021, 4, 2000163. [Google Scholar] [CrossRef] [PubMed]
- Bourges, J.; Bloquel, C.; Thomas, A.; Froussart, F.; Bochot, A.; Azan, F.; Gurny, R.; BenEzra, D.; Behar-Cohen, F. Intraocular implants for extended drug delivery: Therapeutic applications. Adv. Drug Deliv. Rev. 2006, 58, 1182–1202. [Google Scholar] [CrossRef]
- Silva, G.R.d.; Fialho, S.L.; Siqueira, R.C.; Jorge, R.; Cunha Júnior, A.D.S. Implants as drug delivery devices for the treatment of eye diseases. Braz. J. Pharm. Sci. 2010, 46, 585–595. [Google Scholar] [CrossRef]
- Salerno, A. Overview of Polycaprolactone-Based Drug Delivery Systems; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Sun, H.; Mei, L.; Song, C.; Cui, X.; Wang, P. The in vivo degradation, absorption and excretion of PCL-based implant. Biomaterials 2006, 27, 1735–1740. [Google Scholar] [CrossRef]
- Hu, X.; Liu, S.; Zhou, G.; Huang, Y.; Xie, Z.; Jing, X. Electrospinning of polymeric nanofibers for drug delivery applications. J. Control. Release 2014, 185, 12–21. [Google Scholar] [CrossRef]
- Manoukian, O.S.; Marin, C.; Ahmad, A.; James, R.; Kumbar, S.G. Biodegradable injectable implants for long-term delivery of contraceptives and other therapeutics. In Proceedings of the 2015 41st Annual Northeast Biomedical Engineering Conference (NEBEC), Troy, NY, USA, 17–19 April 2015; pp. 1–2. [Google Scholar]
- Manoukian, O.S.; Arul, M.R.; Sardashti, N.; Stedman, T.; James, R.; Rudraiah, S.; Kumbar, S.G. Biodegradable polymeric injectable implants for long-term delivery of contraceptive drugs. J. Appl. Polym. Sci. 2018, 135, 46068. [Google Scholar] [CrossRef]
- Holländer, J.; Genina, N.; Jukarainen, H.; Khajeheian, M.; Rosling, A.; Mäkilä, E.; Sandler, N. Three-dimensional printed PCL-based implantable prototypes of medical devices for controlled drug delivery. J. Pharm. Sci. 2016, 105, 2665–2676. [Google Scholar] [CrossRef] [PubMed]
- Barrett, S.E.; Teller, R.S.; Forster, S.P.; Li, L.; Mackey, M.A.; Skomski, D.; Yang, Z.; Fillgrove, K.L.; Doto, G.J.; Wood, S.L.; et al. Extended-duration MK-8591-eluting implant as a candidate for HIV treatment and prevention. Antimicrob. Agents Chemother. 2018, 62, e01058-18. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, M.; Sarafianos, S.G. EFdA (4′-ethynyl-2-fluoro-2′-deoxyadenosine, MK-8591): A Novel HIV-1 Reverse Transcriptase Translocation Inhibitor. Curr. Opin. HIV AIDS 2018, 13, 294. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.M.; Krovi, S.A.; Li, L.; Girouard, N.; Demkovich, Z.R.; Myers, D.; Creelman, B.; van der Straten, A. Characterization of a Reservoir-Style Implant for Sustained Release of Tenofovir Alafenamide (TAF) for HIV Pre-Exposure Prophylaxis (PrEP). Pharmaceutics 2019, 11, 315. [Google Scholar] [CrossRef]
- Li, L.; Johnson, L.M.; Krovi, S.A.; Demkovich, Z.R.; van der Straten, A. Performance and Stability of Tenofovir Alafenamide Formulations within Subcutaneous Biodegradable Implants for HIV Pre-Exposure Prophylaxis (PrEP). Pharmaceutics 2020, 12, 1057. [Google Scholar] [CrossRef]
- Li, L.; Gatto, G.J.; Brand, R.M.; Krovi, S.A.; Cottrell, M.L.; Norton, C.; van der Straten, A.; Johnson, L.M. Long-acting biodegradable implant for sustained delivery of antiretrovirals (ARVs) and hormones. J. Control. Release 2021, 340, 188–199. [Google Scholar] [CrossRef]
- Li, L.; Krovi, S.; Norton, C.; Johnson, P.; Jimenez, G.; Areson, C.; Van der Straten, A.; Johnson, L. Long-Acting Coformulated Biodegradable Implant for HIV Prevention and Contraception. In Proceedings of the Conference on Retroviruses and Opportunistic Infections (CROI), Virtual, 6–10 March 2021. [Google Scholar]
- Li, L.; Areson, C.; van der Straten, A.; Johnson, L.M. Effects of Polymer Blending on the Performance of a Subcutaneous Biodegradable Implant for HIV Pre-Exposure Prophylaxis (PrEP). Int. J. Mol. Sci. 2021, 22, 6529. [Google Scholar] [CrossRef]
- Siepmann, J.; Siepmann, F. Modeling of diffusion controlled drug delivery. J. Control. Release 2012, 161, 351–362. [Google Scholar] [CrossRef]
- Lao, L.L.; Venkatraman, S.S.; Peppas, N.A. Modeling of drug release from biodegradable polymer blends. Eur. J. Pharm. Biopharm. 2008, 70, 796–803. [Google Scholar] [CrossRef]
- Manini, G.; Benali, S.; Raquez, J.-M.; Goole, J. Proof of concept of a predictive model of drug release from long-acting implants obtained by fused-deposition modeling. Int. J. Pharm. 2022, 618, 121663. [Google Scholar] [CrossRef]
- Schlesinger, E.; Ciaccio, N.; Desai, T.A. Polycaprolactone thin-film drug delivery systems: Empirical and predictive models for device design. Mater. Sci. Eng. C 2015, 57, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Pitt, C.; Chasalow, F.; Hibionada, Y.; Klimas, D.; Schindler, A. Aliphatic polyesters. I. The degradation of poly (ϵ-caprolactone) in vivo. J. Appl. Polym. Sci. 1981, 26, 3779–3787. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 13109, Levonorgestrel. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Levonorgestrel (accessed on 27 June 2022).
- Toxin and Toxin Target Database. Levonorgestrel (T3D4749). Available online: http://www.t3db.ca/toxins/T3D4749 (accessed on 28 June 2022).
- National Center for Biotechnology Information. Compound Summary for CID 6917715, Etonogestrel. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Etonogestrel (accessed on 28 June 2022).
- Toral, M.; Nacaratte, F.; Nova-Ramirez, F.; Otipka, R. Parallel determination of desogestrel and 17α-ethinylestradiol in pharmaceutical formulation by derivative spectrophotometry. J. Chil. Chem. Soc. 2013, 58, 1779–1784. [Google Scholar] [CrossRef]
- DrugBank. Tenofovir Alafenamide Fumarate. Available online: https://go.drugbank.com/salts/DBSALT002533 (accessed on 27 June 2022).
- Puri, A.; Bhattaccharjee, S.A.; Zhang, W.; Clark, M.; Singh, O.N.; Doncel, G.F.; Banga, A.K. Development of a transdermal delivery system for tenofovir alafenamide, a prodrug of tenofovir with potent antiviral activity against HIV and HBV. Pharmaceutics 2019, 11, 173. [Google Scholar] [CrossRef]
- DrugBank. Tenofovir Alafenamide. Available online: https://go.drugbank.com/drugs/DB09299 (accessed on 28 June 2022).
- Zhang, W.; Parniak, M.A.; Mitsuya, H.; Sarafianos, S.G.; Graebing, P.W.; Rohan, L.C. Preformulation studies of EFdA, a novel nucleoside reverse transcriptase inhibitor for HIV prevention. Drug Dev. Ind. Pharm. 2014, 40, 1101–1111. [Google Scholar] [CrossRef][Green Version]
- Drugbank. Islatravir. Available online: https://go.drugbank.com/drugs/DB15653 (accessed on 28 June 2022).
- ChemSpider. Bictegravir. Available online: http://www.chemspider.com/Chemical-Structure.44208822.html (accessed on 28 June 2022).
- DrugBank. Bictegravir. Available online: https://go.drugbank.com/drugs/DB11799 (accessed on 28 June 2022).
- Glilead.com. EMTRIVA® (Emtricitabine) capsule, for Oral Use. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/021500s029lbl.pdf (accessed on 28 June 2022).
- Human Metabolome Database. Lamivudine (HMDB0014847). Available online: https://hmdb.ca/metabolites/HMDB0014847 (accessed on 28 June 2022).
- Wuxi LabNetwork. [(1S,4R)-4-[2-amino-6-(cyclopropylamino)purin-9-yl]cyclopent-2-en-1-yl]methanol. Available online: https://www.labnetwork.com/frontend-app/p/#!/moleculedetails/LN01275094 (accessed on 28 June 2022).
- Drugfuture.com. Abacavir. Available online: https://www.drugfuture.com/chemdata/abacavir.html (accessed on 28 June 2022).
- Administration, T.T.G. Product Information Tivicay â (Dolutegravir) Tablets. Available online: https://www.tga.gov.au/sites/default/files/auspar-dolutegravir-140519-pi.pdf (accessed on 28 June 2022).
- DrugBank. Raltegravir. Available online: https://go.drugbank.com/drugs/DB06817 (accessed on 28 June 2022).
- Fick, A. Ueber Diffusion. Annalen Physik 1855, 170, 59–86. [Google Scholar] [CrossRef]
- Crank, J. The Mathematics of Diffusion, 2nd ed.; Clarendon Press: Oxford, UK, 1975; p. 421. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| API | Suppliers | logP | Molecular Weight (MW) (Da) | Solubility in PBS (CsP) (mg/mL) | pKa |
|---|---|---|---|---|---|
| LNG | Selleck | 3.8 [40] | 312.5 | 0.0071 | 17.9 [41] |
| ENG | AdooQ | 3.3 [42] | 324.6 | 0.0093 | 10.4 [43] |
| TAFsalt | Gilead | 1.49 [44] | 534.5 | 11.59 | 11.36 [44] |
| TAFbase | Gilead | 1.8 [45] | 476.5 | 4.98 | 3.96 [46] |
| EFdA | Wuxi/Pharm | −1.19 [47] | 293.2 | 1.05 | 13.32 [48] |
| BIC | AstaTech | 1.71 [49] | 449.4 | 0.17 | 9.81 [50] |
| FTC | BOC Sciences | −0.43 [51] | 247.2 | 165.6 | 2.65 [51] |
| Excipient | BIC Solubility (mg/mL) | Wuxi EFdA Solubility (mg/mL) | Pharm EFdA Solubility (mg/mL) | ENG Solubility (mg/mL) | FTC Solubility (mg/mL) | LNG solubility (mg/mL) | TAFbase Solubility (mg/mL) | TAFsalt Solubility (mg/mL) |
|---|---|---|---|---|---|---|---|---|
| Castor Oil | 4.35 ± 1.58 | 1.81 ± 0.10 | 2.50 ± 0.18 | 16.20 ± 0.76 | 0.906 ± 0.14 | 1.24 ± 0.21 | 16.75 ± 0.23 | 12.4 ± 0.01 |
| Cottonseed Oil | 2.19 ± 1.13 | 0.04 ± 0.01 | 0.057 ± 0.002 | 3.98 ± 0.07 | 0.011 ± 0.002 | 0.51 ± 0.07 | 0.19 ± 0.18 | 0.168 ± 0.004 |
| Ethyl Oleate | 0.62 ± 0.24 | 0.04 ± 0.01 | 0.05 ± 0.001 | 5.60 ± 0.05 | 0.015 ± 0.002 | 0.59 ± 0.03 | 0.21 ± 0.15 | 0.11 ± 0.01 |
| Glycerol | 3.81 ± 1.21 | 21.9 ± 0.22 | 11.5 ± 0.14 | 2.02 ± 1.20 | 36.9 ± 1.69 | 0.55 ± 0.23 | 29.19 ± 2.73 | 41.8 ± 0.55 |
| Oleic Acid | 15.9 ± 0.29 | 0.71 ± 0.23 | 0.054 ± 0.001 | 4.73 ± 0.37 | 0.5 ± 0.01 | 0.50 ± 0.14 | 52.96 ± 2.08 | 59.9 ± 0.71 |
| PEG300 | 24.8 ± 1.42 | 69.89 ± 0.86 | 11.4 ± 0.16 | 32.95 ± 0.93 | 37.0 ± 3.71 | 3.68 ± 0.33 | 66.93 ± 3.79 | 65.2 ± 0.36 |
| PEG400 | 24.8 ± 5.83 | 68.37 ± 3.52 | 14.2 ± 0.13 | 32.82 ± 1.13 | 37.2 ± 1.76 | 3.83 ± 0.23 | 67.05 ± 2.96 | 39.9 ± 0.18 |
| PEG600 | 25.4 ± 1.83 | 62.87 ± 0.52 | 14.2 ± 0.13 | 31.10 ± 1.26 | 39.0 ± 0.82 | 3.81 ± 0.07 | 59.60 ± 3.22 | 57.6 ± 0.44 |
| PEG40 Castor Oil | 22.1 ± 3.00 | 37.54 ± 0.60 | 22.2 ± 0.21 | 28.02 ± 1.71 | 21.2 ± 0.21 | 4.13 ± 0.46 | 18.37 ± 1.46 | 28.4 ± 0.22 |
| Polysorbate 80 | 24.1 ± 0.72 | 35.02 ± 1.00 | 16.9 ± 0.047 | 25.44 ± 1.55 | 14.8 ± 0.17 | 3.49± 0.54 | 19.06 ± 3.12 | 28.5 ± 0.85 |
| Propylene Glycol | 24.2 ± 4.09 | 41.45 ± 1.22 | 16.9 ± 0.05 | 18.66 ± 1.28 | 38.6 ± 0.49 | 3.49 ± 0.54 | 63.59 ± 4.15 | 75.8 ± 0.86 |
| Sesame Oil | 1.75 ± 1.02 | 0.03 ± 0.01 | 0.22 ± 0.01 | 3.74 ± 0.06 | 0.020 ± 0.006 | 0.54 ± 0.04 | 0.06 ± 0.004 | 0.34 ± 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, L.; Lee, C.; Cruz, D.F.; Krovi, S.A.; Hudgens, M.G.; Cottrell, M.L.; Johnson, L.M. Reservoir-Style Polymeric Drug Delivery Systems: Empirical and Predictive Models for Implant Design. Pharmaceuticals 2022, 15, 1226. https://doi.org/10.3390/ph15101226
Li L, Lee C, Cruz DF, Krovi SA, Hudgens MG, Cottrell ML, Johnson LM. Reservoir-Style Polymeric Drug Delivery Systems: Empirical and Predictive Models for Implant Design. Pharmaceuticals. 2022; 15(10):1226. https://doi.org/10.3390/ph15101226
Chicago/Turabian StyleLi, Linying, Chanhwa Lee, Daniela F. Cruz, Sai Archana Krovi, Michael G. Hudgens, Mackenzie L. Cottrell, and Leah M. Johnson. 2022. "Reservoir-Style Polymeric Drug Delivery Systems: Empirical and Predictive Models for Implant Design" Pharmaceuticals 15, no. 10: 1226. https://doi.org/10.3390/ph15101226
APA StyleLi, L., Lee, C., Cruz, D. F., Krovi, S. A., Hudgens, M. G., Cottrell, M. L., & Johnson, L. M. (2022). Reservoir-Style Polymeric Drug Delivery Systems: Empirical and Predictive Models for Implant Design. Pharmaceuticals, 15(10), 1226. https://doi.org/10.3390/ph15101226